
Mothers with Cancer: An Intersectional Mixed-Methods Study Investigating Role Demands and Perceived Coping Abilities



Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Role Strain due to Cancer-Related Disability
1.2. The Importance of Occupying Multiple Social Roles
1.3. Applying an Intersectional Framework
1.4. Primary Study Aims
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measures
2.3.1. Questionnaire Battery
2.3.2. Semi-Structured Interviews and Focus Groups
2.4. Data Analysis
2.4.1. Questionnaire Battery
2.4.2. Semi-Structured Interviews and Focus Groups
3. Results
3.1. Questionnaire Battery
3.1.1. Demographic, Clinical, and Health Characteristics
3.1.2. Psychological and Role Functioning Compared with General Population
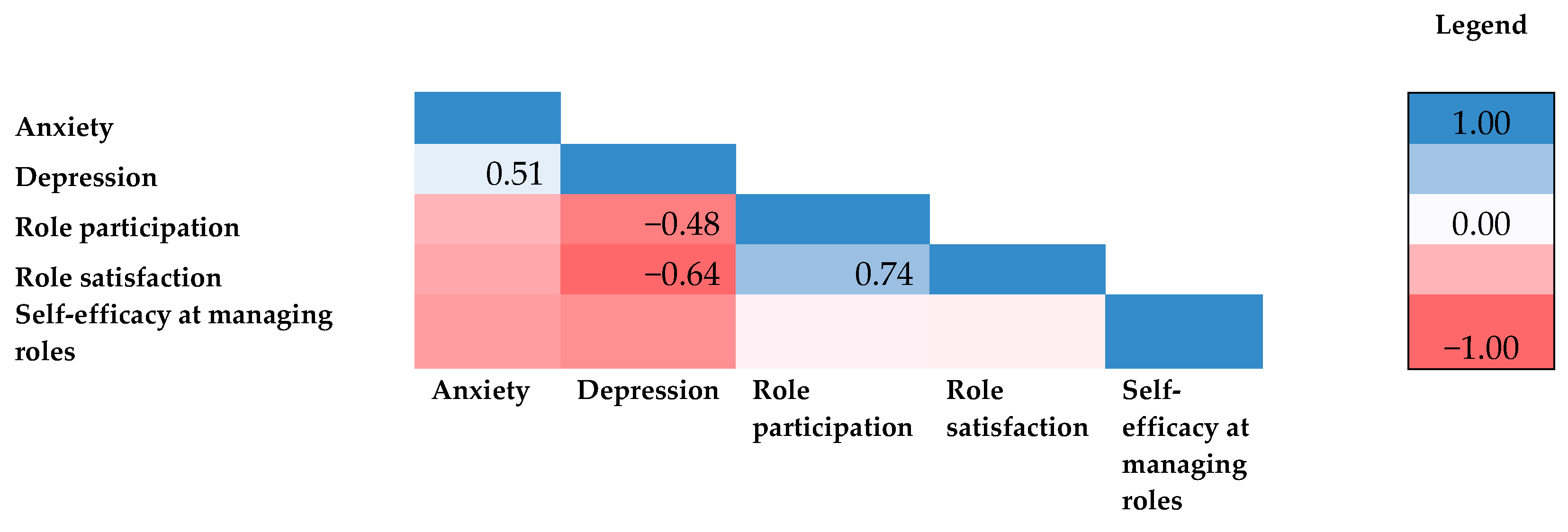
3.1.3. Associations between Psychological and Role Functioning
3.2. Semi-Structured Interviews
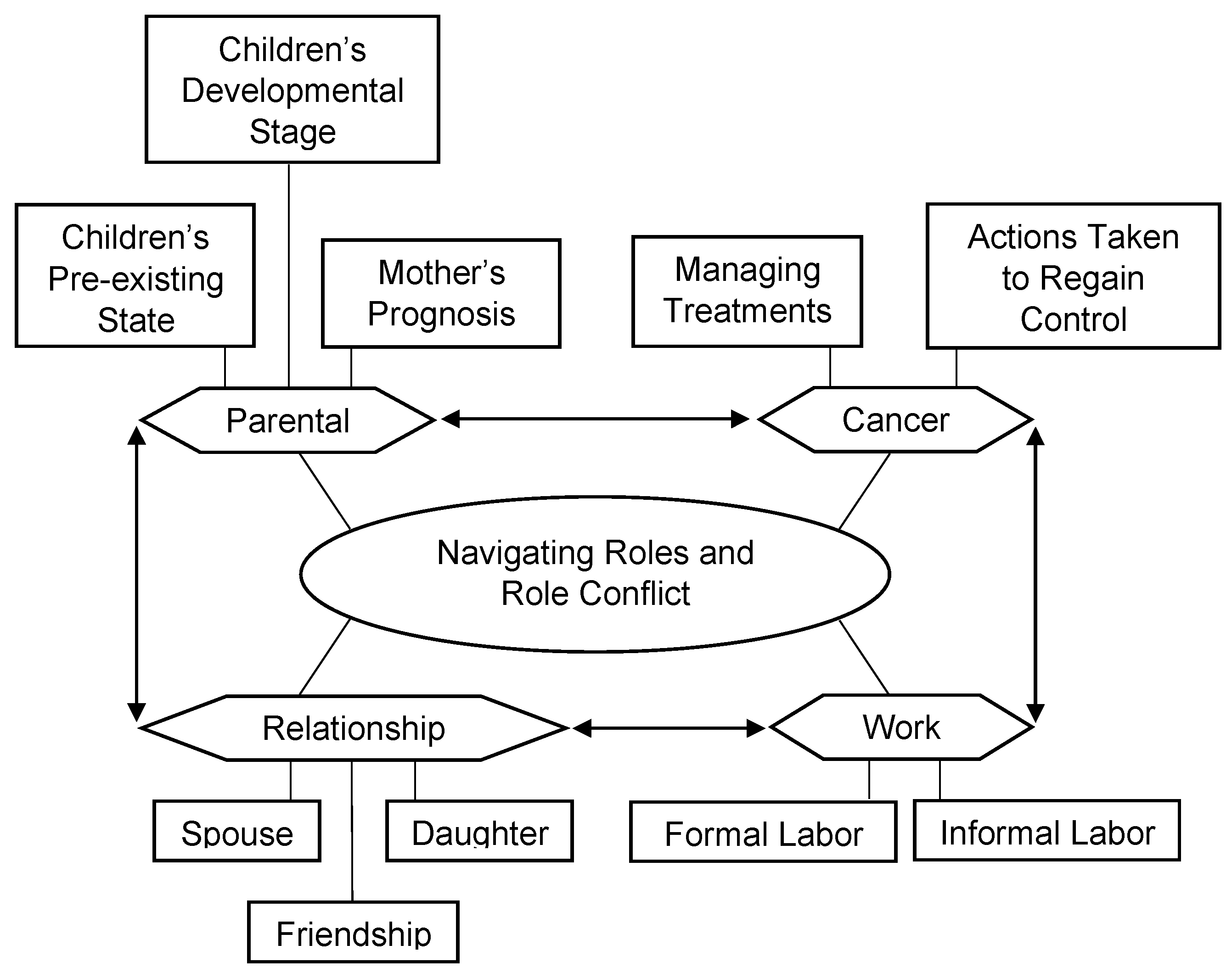
3.2.1. Theme 1: Navigating Roles and Role Conflict
“I’m a mom, I’m a girlfriend, sister, friend, an employee, the housewife, I clean, I cook, and above all the things, an independent woman.”(Melanie)
“She was just like a happy and joyful little [toddler] and I think we all, like all of us, her brothers, my husband, and grandparents and all that like really got in escape like in playing with her joyfulness.”(Kristina)
“Even at [older-elementary age] developmentally they’re starting to understand a few more things about the world.—And mortality, right. She had a fish that died. She understands that there’s other people—even in COVID that there’s other people that, do you know what I mean? Mortality is a bit of a real thing and I think that there’s been, she’s starting to kind of get a little bit of grasp with that, and so there are certain levels of anxiety that come out just from the sheer understanding that there’s a big universe out there and that people are mortal.”(Lauren)
“He is going through the teenage crazies basically. I don’t even know. He is smoking weed; he is sneaking out. Like all the f **** things. I never would have suspected he would be a kid like that, but that is what is happening and it’s just like all happening around the same time as this cancer stuff, which is honestly a million times more stressful.”(Alex)
“You start thinking about your own mortality and you imagine that how much time might I have. I think a lot about how that’s going to impact my son’s life, my ability to be a participant in his life, how long am I going to be alive for him. That was the biggest difficulty. I know my husband would struggle, but he’d move on, but I always think about the impact on my son.”(Gabriella)
“When you go through chemos everything in your body is changing hormones, you’re exhausted. There was zero intimacy. I don’t think my husband and I did more than a kiss for probably a year.”(Nicole)
“I just feel like I don’t have enough time to input into all these relationships that I need to. So, they’re always at odds with each other, my daughter and my boyfriend who don’t get along.”(Lynn)
“I think that there was an expectation that mom would look after the food and mom would look after cleaning and mom would—so mom would take care of the home.”(Gabriella)
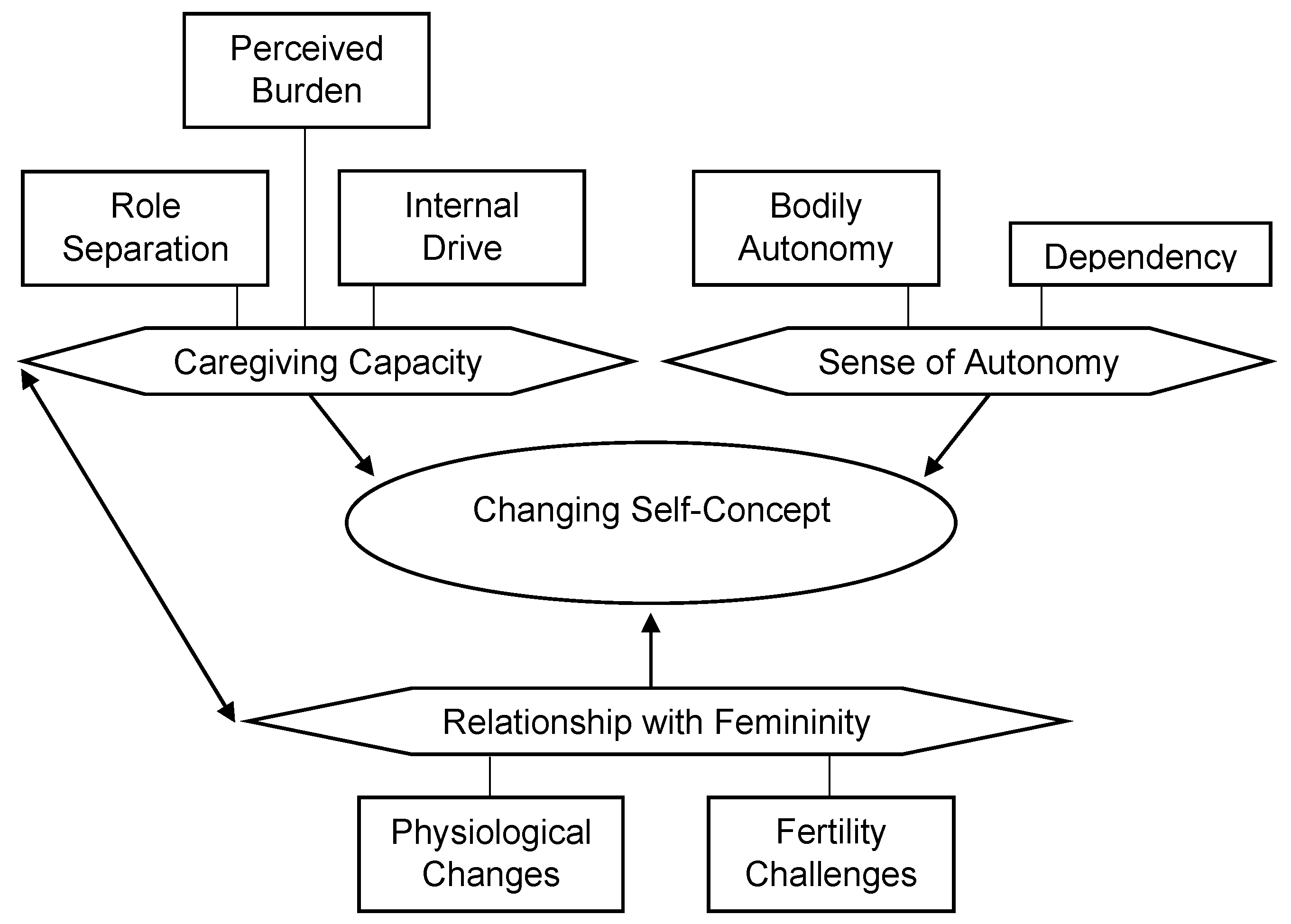
3.2.2. Theme 2: Changing Self-Concept
“I feel pretty guilty because I’ve always prided myself on being really reliable and dependable, and I’m not that way anymore.”(Monica)
“It’s very frustrating for me not to be able to do things on my own, especially after my surgery—it’s detrimental to my mental health not to be able to be independent and I liked that, I liked that part of my identity. I think I worked really hard to get there and to be self-sufficient and learning skills to be able to do things on my own and to lose that ability has been very difficult.”(Lynn)
“She told me that because I asked about the pregnancy and she said because I was so early in my pregnancy if I did the chemo with the pregnancy it would cause the baby harm and pain and they would be deformed.—So, I had to decide if I was going to delay treatment and then hope and pray that my cancer—to give the baby a fighting chance or if I just didn’t have any treatment at all I deliver that baby to term and then that was the end of me or if I had to end the pregnancy that week to then start the chemotherapy.”(Nicole)
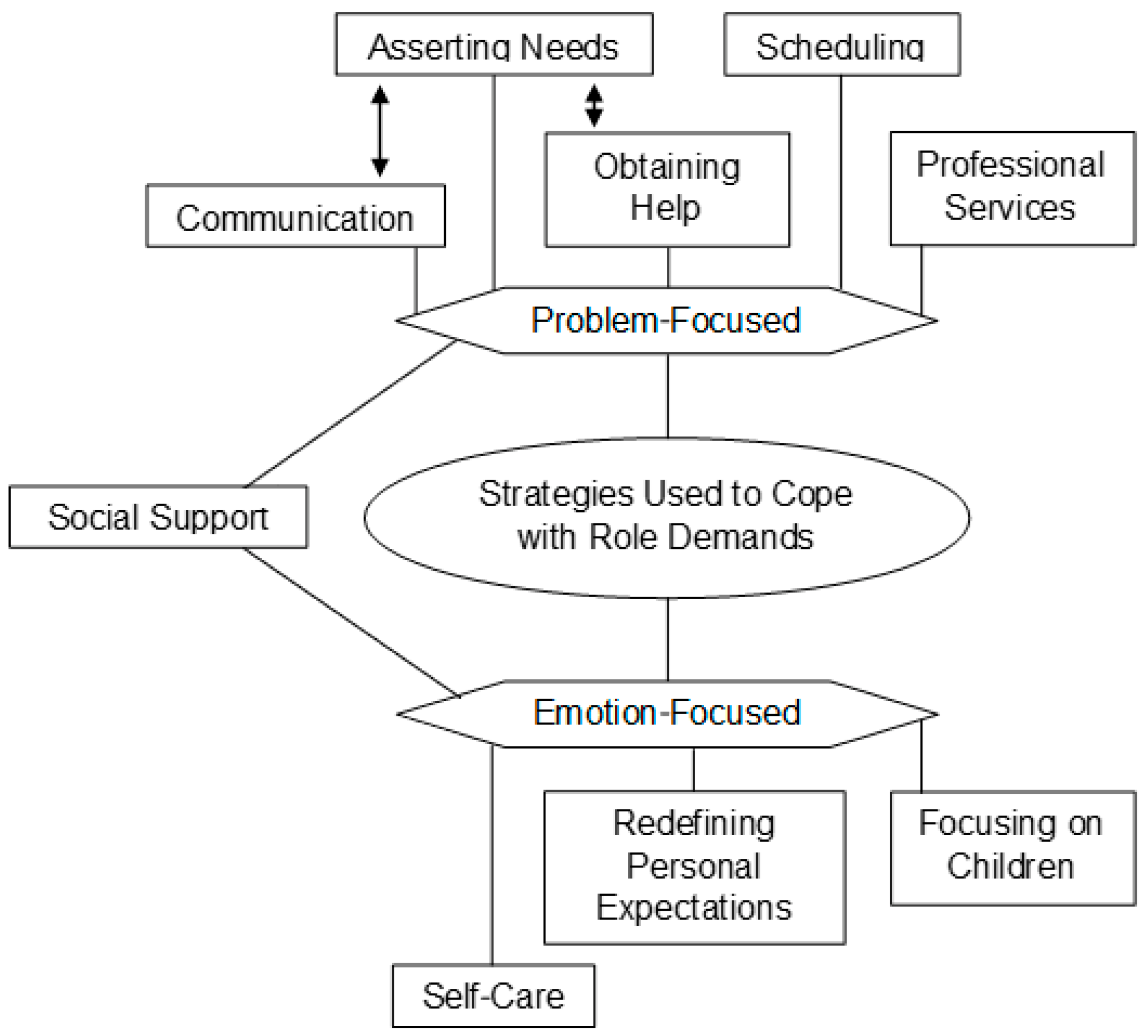
3.2.3. Theme 3: Strategies Used to Cope with Role Demands
“I like to be surrounded by lots of people and I’ve actually made great new friends because of cancer for me and that’s like the best thing ever when I can expand my community.”(Lana)
“Either meditate or take a nap and, and that’s what, that’s what my body needs in order to have the mental energy to, to think more clearly when I have more energy.”(Anna)
“It takes like extra, extra communication to be constantly talking about how our roles are going to change I guess on a daily basis even. What needs to be done and who can do what.”(Kristina)
“It happened to be a time where my husband’s work was really busy, so he couldn’t really take more time off to do those things.”(Irene)
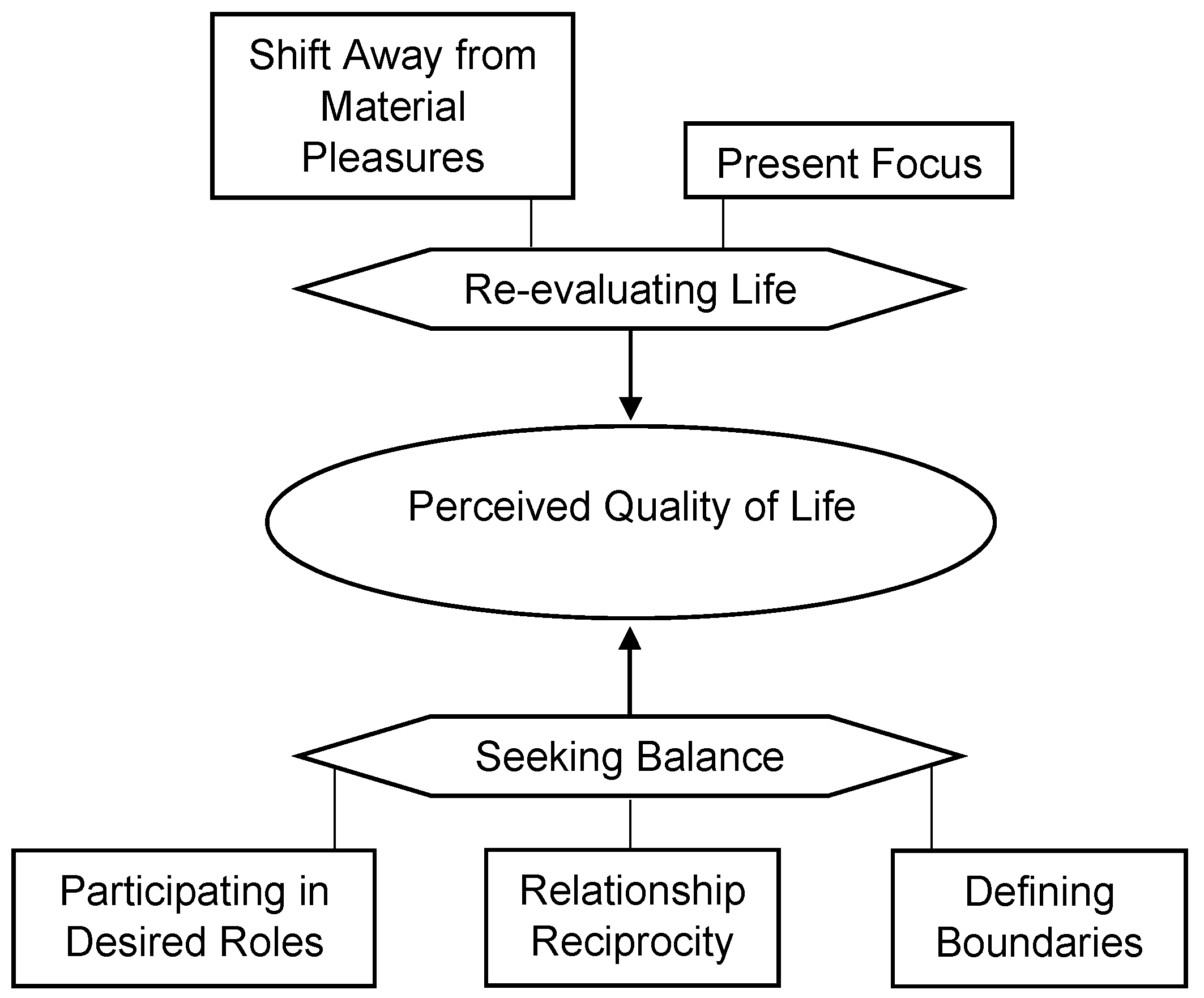
3.2.4. Theme 4: Perceived QoL
“I think the less you try to live by someone else’s standards and you really just try to be comfortable with your life,—everything you hear and see and what your girlfriends are telling you and what they post on Facebook it’s all noise and that you just have to find your rhythm. And the moment you can find your rhythm that’s where you find that peace.”(Annette)
“I think women have been given so many false representations of what balance looks like that’s not achievable.”(Annette)
“My friend got pregnant, she didn’t want to tell me because I wanted to have another baby and I might be infertile. And so they, but she didn’t want to tell me, right? So I feel like they’re scared to tell me their things, so I can’t even be [there] to support them with their stuff. So that’s really crappy, for sure.”(Tracy)
“My work has been really good with letting me work two days a week. I find it gives me purpose, gets me out of bed, makes me feel normal to be honest with you, and that’s what I appreciate.”(Bridgette)
“We needed to have that discussion. If this is still what should be done at home, then I am not going to work, because I can’t do it all.”(Olivia)
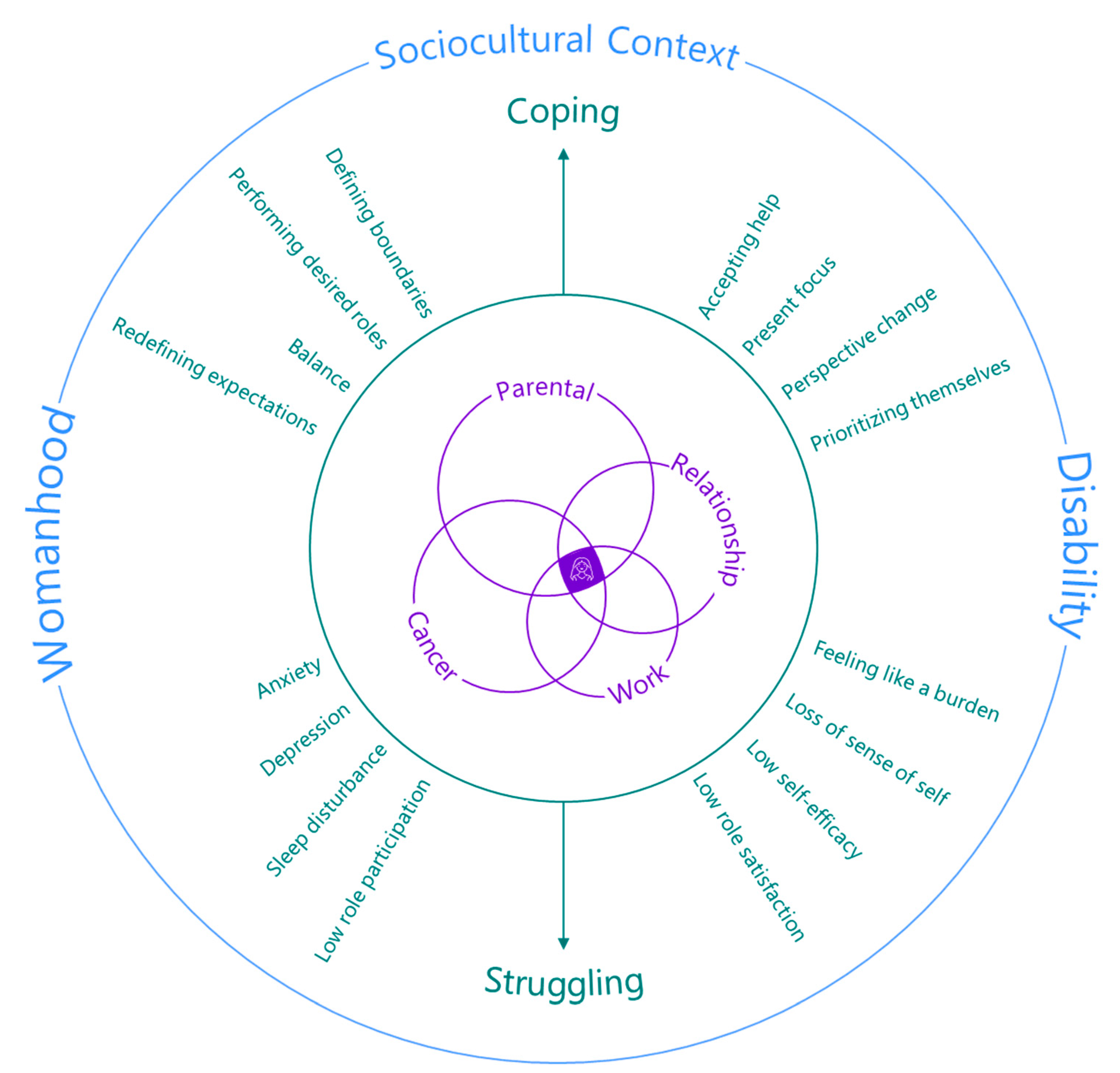
3.2.5. Proposing a New Model: Role Coping as a Mother with Cancer (RCMC)
3.3. Focus Groups
4. Discussion
4.1. The Roles Mothers with Cancer Assume and the Impact of Cancer
4.2. Consequences of Maintaining Multiple Roles and how Mothers with Cancer Cope
4.3. Sociocultural Context Surrounding the Relationship between Mothers’ Roles and Cancer
4.4. Implications and Future Directions
5. Conclusions
“I think what’s so great about just seeing this [the RCMC model] and it is that, to be able to be shown this as a discussion point on the start of this cancer journey, is it just helps you kind of prepare for it a little bit. I think that that’s why there’s like symbolic representation of all this, the study, and the contributions, and the thesis, and when you can distill it down into this, yes, it’s simplified, but to be able to look at this at the outset and think, well, these are all the things I’m actually going to have to think about. I think this is really powerful.”(Lana)
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Families, Living Arrangements, and Unpaid Work. Available online: https://www150.statcan.gc.ca/n1/pub/89-503-x/2010001/article/11546-eng.htm (accessed on 1 April 2021).
- Coverman, S. Role overload, role conflict, and stress: Addressing consequences of multiple role demands. Soc. Forces 1989, 67, 965. [Google Scholar] [CrossRef]
- Dicker, D.; Pain, A.; Moradi-Lakeh, M.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; Hamadeh, R.R.; Werdecker, A.; Gessner, B.D.; et al. The global burden of cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef]
- Journal of Oncology. Physical/psychological disability common in cancer patients. JONS J. Oncol. Navig. Surviv. 2017, 7, 10. Available online: https://www.jons-online.com/issues/2017/october-2017-vol-8-no-10/1703-physicalpsychological-disability (accessed on 1 April 2021).
- Ancoli-Israel, S.; Moore, P.; Jones, V. The relationship between fatigue and sleep in cancer patients: A review. Eur. J. Cancer Care 2001, 10, 245–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roscoe, J.A.; Kaufman, M.E.; Matteson-Rusby, S.E.; Palesh, O.G.; Ryan, J.L.; Kohli, S.; Perlis, M.L.; Morrow, G.R. Cancer-related fatigue and sleep disorders. Oncology 2007, 12, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Zengin, L.; Aylaz, R. The effects of sleep hygiene education and reflexology on sleep quality and fatigue in patients receiving chemotherapy. Eur. J. Cancer Care 2019, 28. [Google Scholar] [CrossRef]
- Asher, A. Cognitive dysfunction among cancer survivors. Am. J. Phys. Med. Rehabil. 2011, 90, 16–26. [Google Scholar] [CrossRef]
- Binarelli, G.; Lange, M.; Dos Santos, M.; Grellard, J.-M.; Lelaidier, A.; Tron, L.; Lefevre, S.; Clarisse, B.; Joly, F. Multimodal web-based intervention for cancer-related cognitive impairment in breast cancer patients: Cog-stim feasibility study protocol. Cancers 2021, 13, 4868. [Google Scholar] [CrossRef]
- Lindner, O.C.; Phillips, B.; McCabe, M.G.; Mayes, A.; Wearden, A.; Varese, F.; Talmi, D.B.; Gregory, G. A meta-analysis of cognitive impairment following adult cancer chemotherapy. Neuropsychology 2014, 28, 726–740. [Google Scholar] [CrossRef] [Green Version]
- Boykoff, N.; Moieni, M.; Subramanian, S.K. Confronting chemo brain: An in-depth look at survivors’ reports of impact on work, social networks, and health care response. J. Cancer Surviv. 2009, 3, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Billhult, A.; Segesten, K. Strength of motherhood: Nonrecurrent breast cancer as experienced by mothers with dependent children. Scand. J. Caring Sci. 2003, 17, 122–128. [Google Scholar] [CrossRef]
- Elmberger, E.; Bolund, C.; Lützén, K. Transition in the experience of moral responsibility of being a parent with cancer by redefining mothering. Nurs. Ethics 2005, 12, 253–262. [Google Scholar] [CrossRef]
- Elmberger, E.; Bolund, C.; Magnusson, A.; Lützén, K.; Andershed, B. Being a mother with cancer: Achieving a sense of balance in the transition process. Cancer Nurs. 2008, 31, 58–66. [Google Scholar] [CrossRef]
- Henderson, A.; Harmon, S.; Newman, H.; Allen, K.R.; Jaramillo-Sierra, A.L. The price mothers pay, even when they are not buying it: Mental health consequences of idealized motherhood. Sex Roles 2015, 74, 512–526. [Google Scholar] [CrossRef]
- Park, E.M.; Check, D.K.; Song, M.-K.; Reeder-Hayes, K.E.; Hanson, L.C.; Yopp, J.M.; Rosenstein, D.L.; Mayer, D.K. Parenting while living with advanced cancer: A qualitative study. Palliat. Med. 2017, 31, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Baird, C.L.; Burge, S.W. Family-friendly benefits and full-time working mothers’ labor force persistence. Community Work Fam. 2018, 21, 168–192. [Google Scholar] [CrossRef]
- Kim, Y.; Hong, S. Profiles of working moms’ daily time use: Exploring their impact on leisure. Int. J. Environ. Res. Public Health 2021, 18, 2305. [Google Scholar] [CrossRef]
- Dorfman, C.S.; Arthur, S.S.; Kimmick, G.; Westbrook, K.W.; Marcom, P.K.; Corbett, C.; Edmond, S.N.; Shelby, R.A. Partner status moderates the relationships between sexual problems and self-efficacy for managing sexual problems and psychosocial quality-of-life for postmenopausal breast cancer survivors taking adjuvant endocrine therapy. Menopause 2019, 26, 823–832. [Google Scholar] [CrossRef] [Green Version]
- Pepin, J.R.; Sayer, L.C.; Casper, L.M. Marital status and mothers’ time use: Childcare, housework, leisure, and sleep. Demography 2018, 55, 107–133. [Google Scholar] [CrossRef]
- Preston, K.; MacDonald, M.; Giuliani, M.E.; Melosky, B.L.; Leung, B.; Ingledew, P-A. Propping up the parents: An environmental scan of childcare programs available to cancer patients in North America. J. Clin. Oncol. 2021, 39, 18805. [Google Scholar] [CrossRef]
- Inhestern, L.; Bergelt, C. When a mother has cancer: Strains and resources of affected families from the mother’s and father’s perspective—a qualitative study. BMC Women’s Health 2018, 18, 72. [Google Scholar] [CrossRef] [PubMed]
- Barnett, R.C.; Hyde, J.S. Women, men, work, and family: An expansionist theory. Am. Psychol. 2001, 56, 781–796. [Google Scholar] [CrossRef] [PubMed]
- Nordenmark, M. Multiple social roles and well-being: A longitudinal test of the role stress theory and the role expansion theory. Acta Sociol. 2004, 47, 115–126. [Google Scholar] [CrossRef]
- Paquette, M.-C.; Raine, K. Sociocultural context of women’s body image. Soc. Sci. Med. 2004, 59, 1047–1058. [Google Scholar] [CrossRef]
- Straiton, M.L.; Ledesma, H.M.L.; Donnelly, T.T. A qualitative study of Filipina immigrants’ stress, distress and coping: The impact of their multiple, transnational roles as women. BMC Women’s Health 2017, 17, 72. [Google Scholar] [CrossRef]
- Baker, J.P.; Berenbaum, H. Emotional approach and problem-focused coping: A comparison of potentially adaptive strategies. Cogn. Emot. 2007, 21, 95–118. [Google Scholar] [CrossRef]
- Folkman, S.; Moskowitz, J.T. Coping: Pitfalls and promise. Annu. Rev. Psychol. 2004, 55, 745–774. [Google Scholar] [CrossRef]
- Samuels, G.M.; Ross-Sheriff, F. Identity, oppression, and power: Feminisms and intersectionality theory. Affilia 2008, 23, 5–9. [Google Scholar] [CrossRef] [Green Version]
- Chrisler, J.C.; Barney, A.; Palatino, B. Ageism can be hazardous to women’s health: Ageism, sexism, and stereotypes of older women in the healthcare system. J. Soc. Issues 2016, 72, 86–104. [Google Scholar] [CrossRef]
- Travis, C.B.; Howerton, D.M.; Szymanski, D.M. Risk, uncertainty, and gender stereotypes in healthcare decisions. Women Ther. 2012, 35, 207–220. [Google Scholar] [CrossRef]
- Gordon, L. Socialist feminism: The legacy of the “second wave”. New Labor Forum 2013, 22, 20–28. [Google Scholar] [CrossRef]
- Gordon, L. ‘Intersectionality’, socialist feminism and contemporary activism: Musings by a second-wave socialist feminist. Gend. Hist. 2016, 28, 340–357. [Google Scholar] [CrossRef]
- Wen, K.Y.; Fang, C.Y.; Ma, G.X. Breast cancer experience and survivorship among Asian Americans: A systematic review. J. Cancer Surviv. 2013, 8, 94–107. [Google Scholar] [CrossRef] [Green Version]
- Goodley, D.; Liddiard, K.; Runswick-Cole, K. Feeling disability: Theories of affect and critical disability studies. Disabil. Soc. 2018, 33, 197–217. [Google Scholar] [CrossRef] [Green Version]
- Silva, C.F.; Howe, P.D. The (in)validity of supercrip representation of paralympian athletes. J. Sport Soc. Issues 2012, 36, 174–194. [Google Scholar] [CrossRef]
- Leech, N.L.; Onwuegbuzie, A.J. A typology of mixed methods research designs. Qual. Quant. 2007, 43, 265–275. [Google Scholar] [CrossRef]
- Cameron, H.M. Methods that Matter: Integrating Mixed Methods for More Effective Social Science Research; University of Chicago Press: Chicago, IL, USA, 2016. [Google Scholar]
- Health Measures PROMIS. Available online: https://www.healthmeasures.net/index.php?option=com_content&view=category&layout=blog&id=147&Itemid=806 (accessed on 20 June 2021).
- Canadian Community Health Survey (CCHS). Available online: https://www23.statcan.gc.ca/imdb-bmdi/pub/document/3226_D71_T9_V1-eng.pdf (accessed on 2 August 2021).
- QSR International Pty Ltd. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 12 November 2021).
- Guest, G.; Namey, E.; Chen, M. A simple method to assess and report thematic saturation in qualitative research. PLOS ONE 2020, 15, e0232076. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Cella, D.; Choi, S.; Garcia, S.; Cook, K.F.; Rosenbloom, S.; Lai, J.-S.; Tatum, D.S.; Gershon, R. Setting standards for severity of common symptoms in oncology using the PROMIS item banks and expert judgment. Qual Life Res. 2014, 23, 2651–2661. [Google Scholar] [CrossRef] [Green Version]
- Mesly, O. Creating Models in Psychological Research; Springer Briefs in Psychology; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1–24. [Google Scholar] [CrossRef]
- Hammersen, F.; Pursche, T.; Fischer, D.; Katalinic, A.; Waldmann, A. Psychosocial and family-centered support among breast cancer patients with dependent children. Psycho-Oncology 2021, 30, 361–368. [Google Scholar] [CrossRef]
- Blackwood, J.; Karczewski, H.; Huang, M.H.; Pfalzer, L. Katz activities of daily living disability in older cancer survivors by age, stage, and cancer type. J. Cancer Surviv. 2020, 14, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Aulibrk, J.; Delia, M.; Mitrovia, S.; Aulibrk, D. Job satisfaction, organizational commitment and job involvement: The mediating role of job involvement. Front. Psychol. 2018, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Fang, C.Y.; Daly, M.B.; Miller, S.M.; Zerr, T.; Malick, J.; Engstrom, P. Coping with ovarian cancer risk: The moderating effects of perceived control on coping and adjustment. Br. J. Health Psychol. 2006, 11, 561–580. [Google Scholar] [CrossRef] [PubMed]
- Rottenberg, C. Happiness and the liberal imagination: How superwoman became balanced. Fem. Stud. 2014, 40, 144–168. [Google Scholar] [CrossRef]
- Warmoth, K.; Cheung, B.; You, J.; Yeung, N.C.Y.; Lu, Q. Exploring the social needs and challenges of Chinese American immigrant breast cancer survivors: A qualitative study using an expressive writing approach. Int. J. Behav. Med. 2017, 24, 827–835. [Google Scholar] [CrossRef]
- Veenstra, C.M.; Regenbogen, S.E.; Hawley, S.T.; Banerjee, M.; Kato, I.; Ward, K.C.; Morris, A.M. The impact of chemotherapy use on financial strain among stage III colorectal cancer patients: A population-based survey. J. Clin. Oncol. 2014, 32, 505. [Google Scholar] [CrossRef]
- Longo, C.J.; Fitch, M.I.; Loree, J.M.; Carlson, L.E.; Turner, D.; Cheung, W.Y.; Gopaul, D.; Ellis, J.; Ringash, J.; Mathews, M. Patient and family financial burden associated with cancer treatment in Canada: A national study. Support Care Cancer 2021, 29, 3377–3386. [Google Scholar] [CrossRef]
- Jahani Sayad Noveiri, M.; Khodaveisi, M.; Shamsaei, F.; Vanaki, Z.; Tapak, L. Identifying Important challenges of coping with female breast cancer among Iranian spouses: A qualitative study. Iran. J. Psychiatry 2022, 17, 379–387. [Google Scholar] [CrossRef]
- Shands, L.F.M.; Sinsheimer, J.; Cochrane, B.B. Core concerns of couples living with early stage breast cancer. Psycho-Oncology 2006, 15, 1055–1064. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase | Coding Method | Performed By |
|---|---|---|
| A.S., volunteer 1, volunteer 2 | |
| Inductive approach | A.S., volunteer 1, volunteer 2 |
| Iterative process | Consensus-based codebook | A.S., volunteer 1, volunteer 2 |
| Review | Consensus-based codebook | A.S., volunteer 1, volunteer 2, J.D. |
| Data saturation | Final codebook | A.S., volunteer 1, volunteer 2 |
| Consensus approach based on emergent themes | A.S., volunteer 1, volunteer 2 |
| Consensus approach based on literature | A.S., volunteer 1, volunteer 2 |
| Consensus approach based on emergent themes and literature | A.S., volunteer 1, volunteer 2, J.D., |
| A.S., volunteer 1, volunteer 2, J.D. |
| n | % | |
|---|---|---|
| Gender | ||
| Female | 18 | 100 |
| Ethnicity * | ||
| European | 17 | 94 |
| Central and South America | 1 | 6 |
| Japanese | 1 | 6 |
| Housing | ||
| Urban | 16 | 89 |
| Rural | 2 | 11 |
| Highest level of education | ||
| Community college | 2 | 11 |
| University (undergraduate) | 11 | 61 |
| University (professional/post-graduate) | 5 | 28 |
| Annual household income (CAD) | ||
| From 51,000 to 80,000 | 3 | 17 |
| From 81,000 to 120,000 | 1 | 6 |
| >120,000 | 10 | 56 |
| Prefer not to say | 4 | 22 |
| Primary source of income * | ||
| Employment/business/investment | 14 | 78 |
| Pension/retirement | 1 | 6 |
| Social assistance | 3 | 17 |
| Family support | 4 | 22 |
| Employment status | ||
| Full time | 6 | 33 |
| Part time | 7 | 39 |
| Full-time homemaker | 4 | 22 |
| Marital status | ||
| Single | 1 | 6 |
| Married | 12 | 67 |
| Common-law | 4 | 22 |
| Separated | 1 | 6 |
| No. of dependent children | ||
| One | 9 | 50 |
| Two | 6 | 33 |
| Three | 3 | 17 |
| Cancer type | ||
| Breast | 13 | 72 |
| Hodgkin’s lymphoma | 1 | 6 |
| Non-Hodgkin’s lymphoma | 2 | 11 |
| Colorectal | 1 | 6 |
| Lung | 1 | 6 |
| Stage | ||
| One | 1 | 6 |
| Two | 6 | 33 |
| Three | 4 | 22 |
| Four | 5 | 28 |
| Unsure | 2 | 11 |
| Treatments received * | ||
| Chemotherapy | 12 | 67 |
| Radiation | 11 | 61 |
| Surgery | 11 | 61 |
| Hormone therapy | 9 | 50 |
| Immunotherapy | 1 | 6 |
| Targeted therapy | 1 | 6 |
| Stem-cell transplant | 1 | 6 |
| Prescription drug use | ||
| Never | 10 | 56 |
| Rarely | 6 | 53 |
| Sometimes | 1 | 6 |
| Often | 1 | 6 |
| Marijuana use | ||
| Never | 14 | 78 |
| Rarely | 3 | 17 |
| Often | 1 | 6 |
| Cigarette or tobacco use | ||
| Never | 17 | 94 |
| Rarely | 2 | 11 |
| Alcohol use | ||
| Never | 8 | 44 |
| Rarely | 2 | 11 |
| Sometimes | 7 | 39 |
| Often | 1 | 6 |
| Overindulging in foods | ||
| Never | 1 | 6 |
| Rarely | 9 | 50 |
| Sometimes | 4 | 22 |
| Often | 4 | 22 |
| Weekly exercise | ||
| <2 h | 4 | 22 |
| From 2 to 5 h | 11 | 61 |
| From 6 to 9 h | 1 | 6 |
| >9 h | 2 | 11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spiropoulos, A.; Deleemans, J.; Beattie, S.; Carlson, L.E. Mothers with Cancer: An Intersectional Mixed-Methods Study Investigating Role Demands and Perceived Coping Abilities. Cancers 2023, 15, 1915. https://doi.org/10.3390/cancers15061915
Spiropoulos A, Deleemans J, Beattie S, Carlson LE. Mothers with Cancer: An Intersectional Mixed-Methods Study Investigating Role Demands and Perceived Coping Abilities. Cancers. 2023; 15(6):1915. https://doi.org/10.3390/cancers15061915
Chicago/Turabian StyleSpiropoulos, Athina, Julie Deleemans, Sara Beattie, and Linda E. Carlson. 2023. "Mothers with Cancer: An Intersectional Mixed-Methods Study Investigating Role Demands and Perceived Coping Abilities" Cancers 15, no. 6: 1915. https://doi.org/10.3390/cancers15061915