
Multidisciplinary Approach to Spinal Metastases and Metastatic Spinal Cord Compression—A New Integrative Flowchart for Patient Management
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Background
1.1. General Pathophysiological Mechanisms of Bone Metastases
1.2. Specific Pathophysiological Framework of Spinal Metastases and Metastatic Spinal Cord Compression
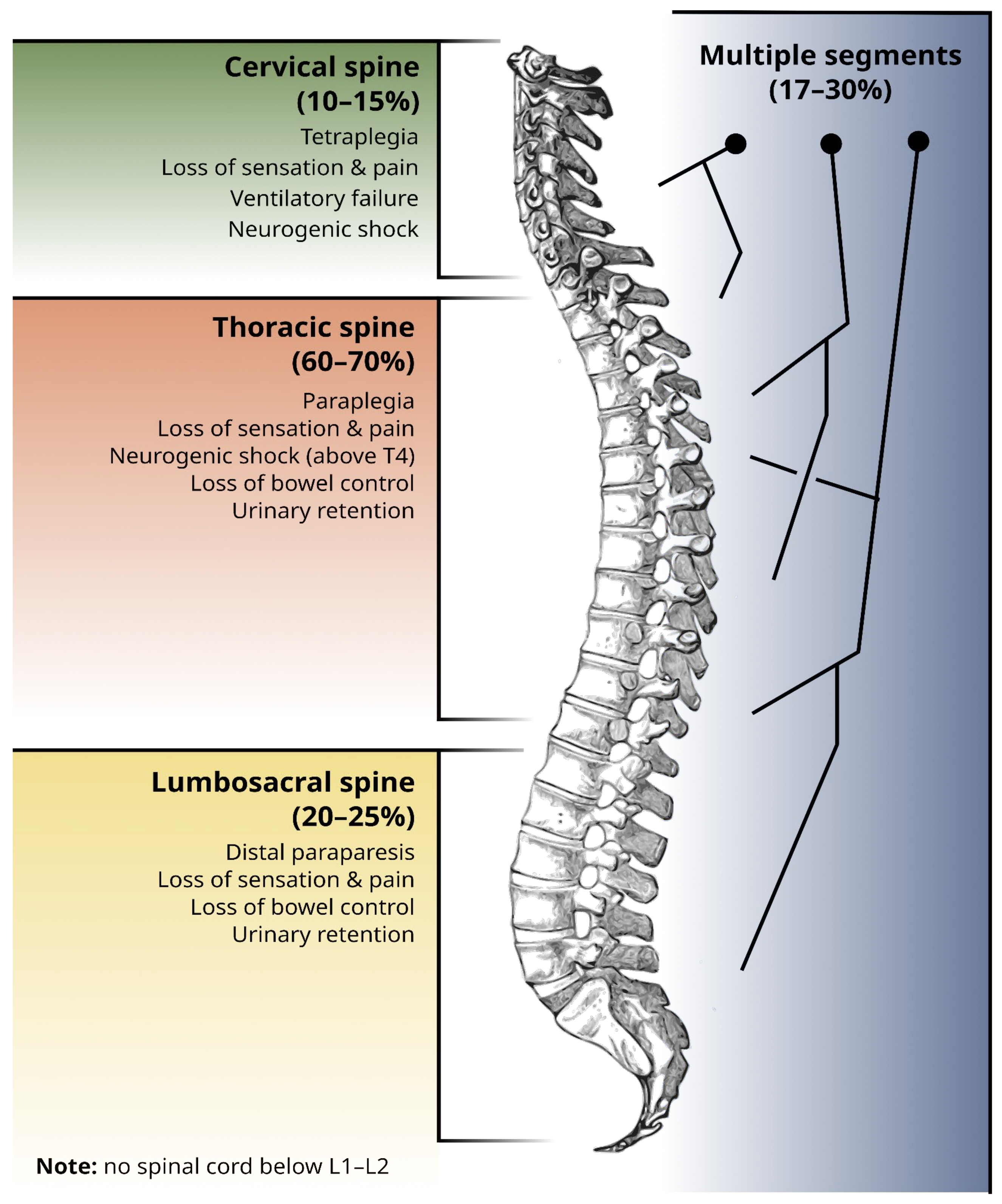
1.3. Topographical Distribution of Spinal Metastases
1.4. Anatomical Classification of Spinal Metastases
2. Relevance of Spinal Metastatic Disease, Importance of Its Multidisciplinary Management, and Motivation for the Development of the Algorithms
- Before spinal cord compression, radiooncologists and medical oncologists cooperate to achieve control of the primary tumor and metastases (including the use of bone targeted agents, as mentioned in Section 1.1), in order to prevent complications. Spinal surgeons can stabilize the relevant spinal segments preemptively;
- During acute spinal cord compression or after an unstable vertebral fracture, there is a short time window in which surgical decompression and stabilization can restore a degree of functionality. In this case, an optimized referral pathway and well-established lines of communication between professionals (emergency physician, medical oncologist, radio-oncologist, and spinal surgeon) are essential;
- In the post-acute phase, after an established neurological deficit, surgical decompression, and stabilization (if not performed before) may still play a role. Radiation therapy is almost universally recommended, and systemic treatment is often indicated. Because permanent neurological sequelae are expected, other professionals, such as palliative care physicians and formal or informal caregivers, will play a role in trying to avoid further loss of quality of life. Rehabilitation plays an important role, as function recovery after metastatic spinal cord compression is similar to the one observed in traumatic spinal injury [31].
3. The Art of Prognostication, Clinical Judgment, and Decision
3.1. Ingredients for an Appropriate Decision: Spinal Stability Status, the Concept of Tumor Radiosensitivity, Clinical Criteria, and Expected Treatment Complications
3.2. Evaluating the Spinal Stability Status: The Spinal Instability Neoplastic Score (SINS)
3.3. Tumor Radiosensitivity
3.4. Clinical Criteria and Its Validation
3.5. The Complexity of Management: Concrete Examples

{kind=link}
{kind=link}
{kind=link}
| Tumor Type | First-Line Treatment | Treatment Efficacy |
|---|---|---|
| Hormonal receptor-positive breast cancer | Combination of hormone-therapy and cyclin-dependent kinase 4/6 inhibitors (palbociclib, ribociclib, and abemaciclib) | Median overall survival (OS) is 63.9 months for ribociclib [76] |
| HER2-positive breast cancer | Combination of taxane-based chemotherapy and dual HER-2 blockade | Median OS is 56.5 months [77] |
| Castration-sensitive prostate cancer | Androgen deprivation therapy plus hormonal therapy | Median OS > 52 months (median overall survival not yet reached) [78] |
| Renal cell carcinoma | Combination of a tyrosine-kinase inhibitor (axitinib) and immunotherapy (pembrolizumab) or double immunotherapy (ipilimumab + nivolumab) | Median OS is 45.7 months [79] |
| Multiple myeloma | Bortezomib (proteasome inhibitor), lenalidomide, and dexamethasone (corticosteroid) | Median OS is 60 months [80] |
| Testicular germ cell tumors | Platinum-based chemotherapy (e.g., bleomycin + cisplatin + etoposide−good performance status only) | Good-risk disease: 90% cure rate; intermediate-risk disease: 80% cure rate; high-risk disease: 50% cure rate [83] |
3.6. Objective Metrics to Appropriately Prognosticate, Judge, and Decide
3.7. Prognostication
3.7.1. Tomita Score
3.7.2. Tokuhashi Score
3.7.3. Skeletal Oncology Research Group (SORG) Nomogram
3.7.4. New England Spinal Metastasis Score (NESMS)
3.8. Clinical Judgment and Decision
3.8.1. Neurologic, Oncologic, Mechanical, and Systemic Status (NOMS) Framework
3.8.2. Location, Mechanical Instability, Neurology, Oncology, and Patient’s Features (LMNOP) System
3.8.3. Metastatic Spine Disease Multidisciplinary Working Group Algorithms (MSDA)
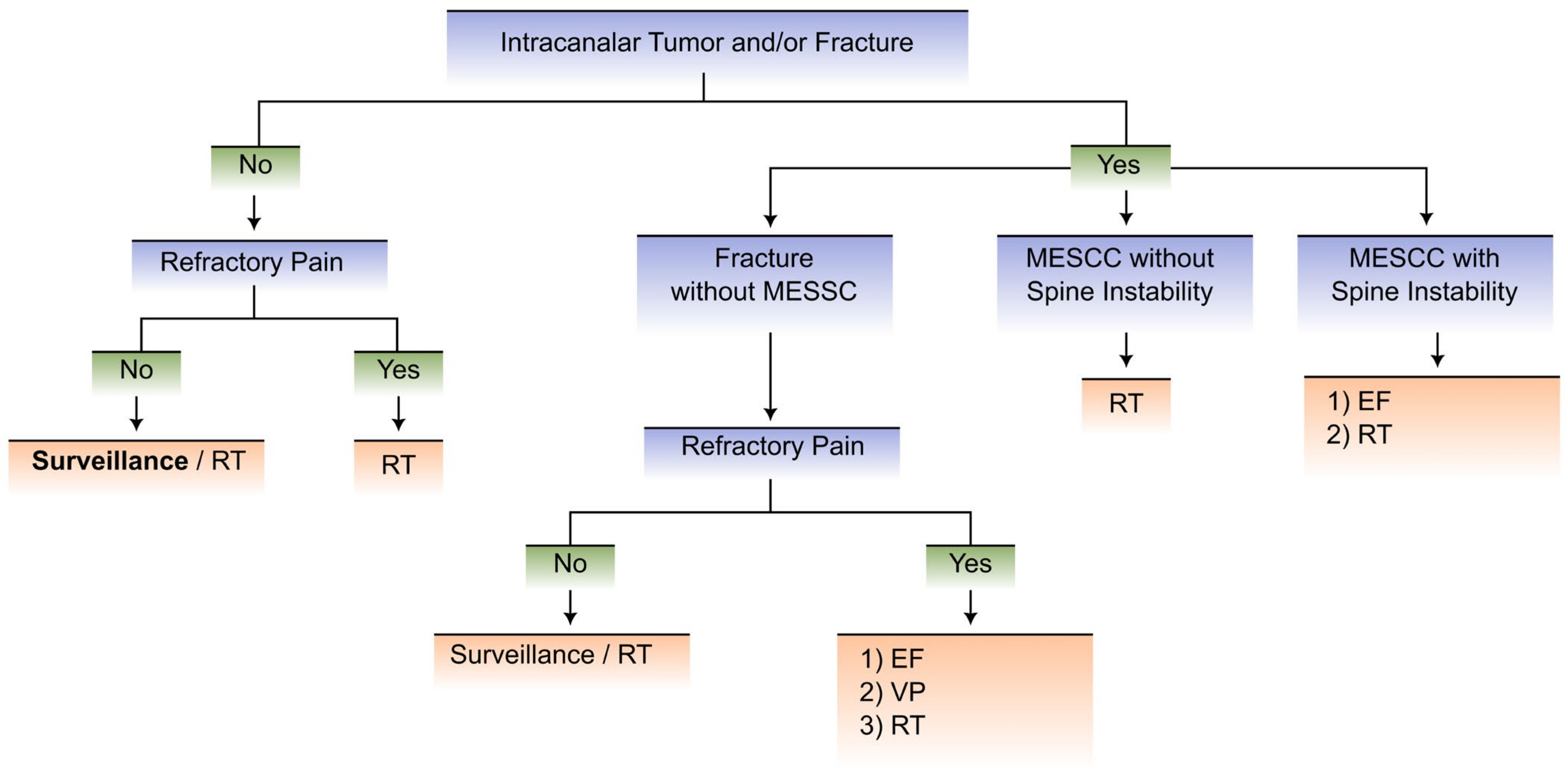
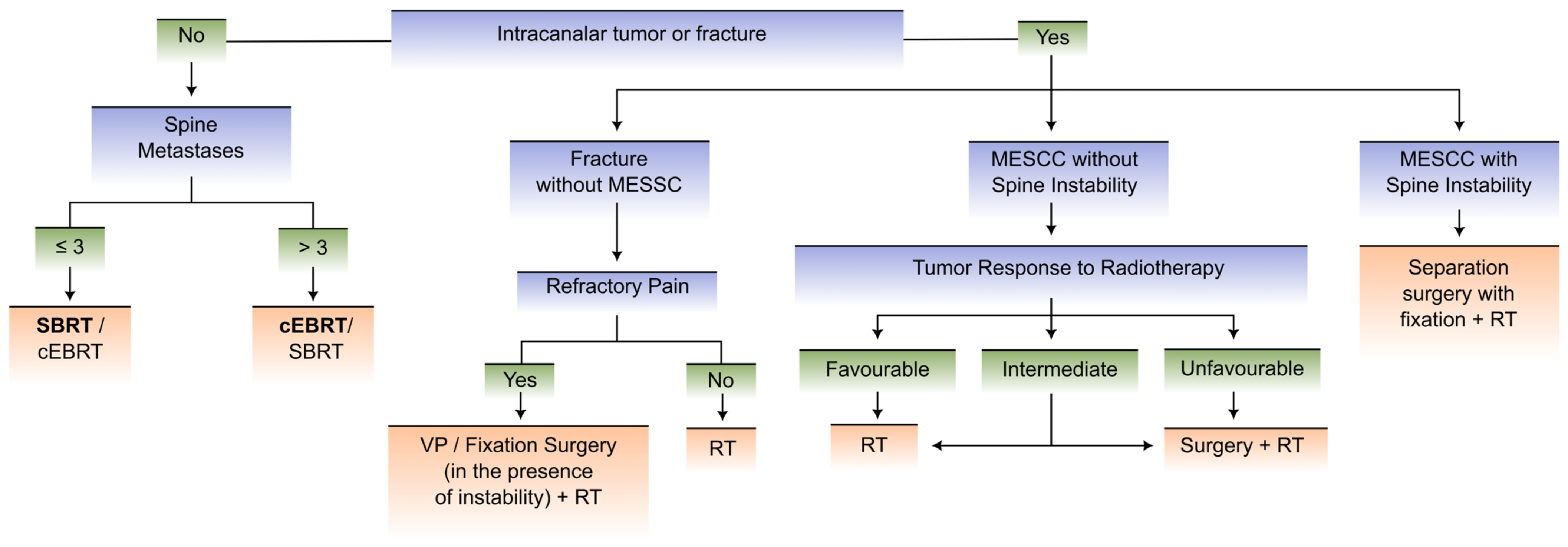
4. A New Integrative Flowchart Proposal
4.1. Goals of the Flowchart Development
4.2. Clinical Scenarios and Proposed Flowcharts
- Scenario 1 comprises patients with KPS ≤ 40% and/or expected 6-month survival < 50% and/or oncologic disease with multisystemic and progressive involvement and a lack of therapeutic options (as assessed by the medical oncologist).
- Scenario 2 includes patients with KPS > 40% and expected 6-month survival ≥ 50% and oncologic disease with stable/limited involvement or multisystemic involvement with available therapeutic options (as assessed by the medical oncologist).
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rothberg, B.E.G.; Quest, T.E.; Yeung, S.J.; Pelosof, L.C.; Gerber, D.E.; Seltzer, J.A.; Bischof, J.J.; Thomas, C.R.; Akhter, N.; Mamtani, M.; et al. Oncologic emergencies and urgencies: A comprehensive review. CA Cancer J. Clin. 2022, 72, 570–593. [Google Scholar] [CrossRef] [PubMed]
- Spring, J.; Munshi, L. Oncologic emergencies: Traditional and contemporary. Crit. Care Clin. 2021, 37, 85–103. [Google Scholar] [CrossRef] [PubMed]
- von Moos, R.; Costa, L.; Ripamonti, C.I.; Niepel, D.; Santini, D. Improving quality of life in patients with advanced cancer: Targeting metastatic bone pain. Eur. J. Cancer 2017, 71, 80–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versteeg, A.L.; Sahgal, A.; Rhines, L.D.; Sciubba, D.M.; Schuster, J.M.; Weber, M.H.; Lazary, A.; Boriani, S.; Bettegowda, C.; Fehlings, M.G.; et al. Health related quality of life outcomes following surgery and/or radiation for patients with potentially unstable spinal metastases. Spine J. 2021, 21, 492–499. [Google Scholar] [CrossRef]
- Van den Brande, R.; Cornips, E.M.; Peeters, M.; Ost, P.; Billiet, C.; Van de Kelft, E. Epidemiology of spinal metastases, metastatic epidural spinal cord compression and pathologic vertebral compression fractures in patients with solid tumors: A systematic review. J. Bone Oncol. 2022, 35, 100446. [Google Scholar] [CrossRef]
- da Silva, G.T.; Bergmann, A.; Thuler, L.C.S. Impact of Symptomatic Metastatic Spinal Cord Compression on Survival of Patients with Non-Small-Cell Lung Cancer. World Neurosurg. 2017, 108, 698–704. [Google Scholar] [CrossRef]
- He, S.; Wei, H.; Ma, Y.; Zhao, J.; Xu, W.; Xiao, J. Outcomes of metastatic spinal cord compression secondary to primary hepatocellular carcinoma with multidisciplinary treatments. Oncotarget 2017, 8, 43439–43449. [Google Scholar] [CrossRef] [Green Version]
- Ju, D.G.; Zadnik, P.L.; Groves, M.L.; Hwang, L.; Kaloostian, P.E.; Wolinksy, J.-P.; Witham, T.F.; Bydon, A.; Gokaslan, Z.L.; Sciubba, D.M. Factors associated with improved outcomes following decompressive surgery for prostate cancer metastatic to the spine. Neurosurgery 2013, 73, 657–666, discussion 666. [Google Scholar] [CrossRef]
- Douglas, S.; Huttenlocher, S.; Bajrovic, A.; Rudat, V.; Schild, S.E.; Rades, D. Prognostic factors for different outcomes in patients with metastatic spinal cord compression from cancer of unknown primary. BMC Cancer 2012, 12, 261. [Google Scholar] [CrossRef] [Green Version]
- Douglas, S.; Schild, S.E.; Rades, D. A new score predicting the survival of patients with spinal cord compression from myeloma. BMC Cancer 2012, 12, 425. [Google Scholar] [CrossRef] [Green Version]
- Rades, D.; Dunst, J.; Schild, S.E. The first score predicting overall survival in patients with metastatic spinal cord compression. Cancer 2008, 112, 157–161. [Google Scholar] [CrossRef]
- Nenclares, P.; Guardado, S.; Asiáin, L.; Pérez-Escutia, M.Á.; Peña, M.C.; Bartolomé, A.; Ruíz, A.; Cabeza, M.Á.; Colmenero, M.; Gascón, N.; et al. A new and simple scoring system to predict overall survival after irradiation for metastatic spinal cord compression. Clin. Transl. Oncol. 2020, 22, 440–444. [Google Scholar] [CrossRef]
- Coleman, R.E.; Croucher, P.I.; Padhani, A.R.; Clézardin, P.; Chow, E.; Fallon, M.; Guise, T.; Colangeli, S.; Capanna, R.; Costa, L. Bone metastases. Nat. Rev. Dis. Primers 2020, 6, 83. [Google Scholar] [CrossRef]
- Nowak, H.; Szwacka, D.M.; Pater, M.; Mrugalski, W.K.; Milczarek, M.G.; Staniszewska, M.; Jankowski, R.; Barciszewska, A.-M. Holistic Approach to the Diagnosis and Treatment of Patients with Tumor Metastases to the Spine. Cancers 2022, 14, 3480. [Google Scholar] [CrossRef]
- Coleman, R.; Hadji, P.; Body, J.J.; Santini, D.; Chow, E.; Terpos, E.; Oudard, S.; Bruland, Ø.; Flamen, P.; Kurth, A.; et al. Bone health in cancer: ESMO Clinical Practice Guidelines. Ann. Oncol. 2020, 31, 1650–1663. [Google Scholar] [CrossRef]
- Singleton, J.M.; Hefner, M. Spinal Cord Compression. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Zhang, Y.; Al Mamun, A.; Yuan, Y.; Lu, Q.; Xiong, J.; Yang, S.; Wu, C.; Wu, Y.; Wang, J. Acute spinal cord injury: Pathophysiology and pharmacological intervention (Review). Mol. Med. Rep. 2021, 23, 417. [Google Scholar] [CrossRef]
- Anjum, A.; Yazid, M.D.; Fauzi Daud, M.; Idris, J.; Ng, A.M.H.; Selvi Naicker, A.; Ismail, O.H.R.; Athi Kumar, R.K.; Lokanathan, Y. Spinal cord injury: Pathophysiology, multimolecular interactions, and underlying recovery mechanisms. Int. J. Mol. Sci. 2020, 21, 7533. [Google Scholar] [CrossRef]
- Tsukamoto, S.; Kido, A.; Tanaka, Y.; Facchini, G.; Peta, G.; Rossi, G.; Mavrogenis, A.F. Current overview of treatment for metastatic bone disease. Curr. Oncol. 2021, 28, 3347–3372. [Google Scholar] [CrossRef]
- Gray, H.; Ukray, M. Gray’s Anatomy: Illustrated With 1247 Coloured Well Drawing Engrawings (Volume 1), 20th ed.; CreateSpace Independent Publishing Platform: Scotts Valley, CA, USA, 2016; p. 828. ISBN 1537434438. [Google Scholar]
- Ziu, E.; Viswanathan, V.K.; Mesfin, F.B. Spinal Metastasis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Batson, O.V. The function of the vertebral veins and their role in the spread of metastases. Ann. Surg. 1940, 112, 138–149. [Google Scholar] [CrossRef]
- Coman, D.R.; Delong, R.P. The role of the vertebral venous system in the metastasis of cancer to the spinal column. Experiments with tumor-cell suspensions in rats and rabbits. Cancer 1951, 4, 610–618. [Google Scholar] [CrossRef]
- Maccauro, G.; Spinelli, M.S.; Mauro, S.; Perisano, C.; Graci, C.; Rosa, M.A. Physiopathology of spine metastasis. Int. J. Surg. Oncol. 2011, 2011, 107969. [Google Scholar] [CrossRef] [PubMed]
- Yuh, W.T.; Quets, J.P.; Lee, H.J.; Simonson, T.M.; Michalson, L.S.; Nguyen, P.T.; Sato, Y.; Mayr, N.A.; Berbaum, K.S. Anatomic distribution of metastases in the vertebral body and modes of hematogenous spread. Spine 1996, 21, 2243–2250. [Google Scholar] [CrossRef] [PubMed]
- Amelot, A.; Terrier, L.-M.; Cristini, J.; LeNail, L.-R.; Buffenoir, K.; Pascal-Moussellard, H.; Bonaccorsi, R.; Mathon, B. Approaching spinal metastases spread profile. Surg. Oncol. 2019, 31, 61–66. [Google Scholar] [CrossRef]
- Li, J.; Wei, W.; Xu, F.; Wang, Y.; Liu, Y.; Fu, C. Clinical therapy of metastatic spinal tumors. Front. Surg. 2021, 8, 626873. [Google Scholar] [CrossRef] [PubMed]
- Bhowmik, D.; Song, X.; Intorcia, M.; Gray, S.; Shi, N. Examination of burden of skeletal-related events in patients naive to denosumab and intravenous bisphosphonate therapy in bone metastases from solid tumors population. Curr. Med. Res. Opin. 2019, 35, 513–523. [Google Scholar] [CrossRef]
- Patnaik, S.; Turner, J.; Inaparthy, P.; Kieffer, W.K. Metastatic spinal cord compression. Br. J. Hosp. Med. 2020, 81, 1–10. [Google Scholar] [CrossRef]
- Al-Qurainy, R.; Collis, E. Metastatic spinal cord compression: Diagnosis and management. BMJ 2016, 353, i2539. [Google Scholar] [CrossRef] [Green Version]
- Newman, W.C.; Patel, A.; Goldberg, J.L.; Bilsky, M.H. The importance of multidisciplinary care for spine metastases: Initial tumor management. Neurooncol Pract. 2020, 7, i25–i32. [Google Scholar] [CrossRef]
- Wallace, A.N.; Robinson, C.G.; Meyer, J.; Tran, N.D.; Gangi, A.; Callstrom, M.R.; Chao, S.T.; Van Tine, B.A.; Morris, J.M.; Bruel, B.M.; et al. The metastatic spine disease multidisciplinary working group algorithms. Oncologist 2015, 20, 1205–1215, Erratum in Oncologist 2019, 24, 424. [Google Scholar] [CrossRef] [Green Version]
- ATLS Subcommittee; American College of Surgeons’ Committee on Trauma; International ATLS working group. Advanced trauma life support (ATLS®): The ninth edition. J. Trauma Acute Care Surg. 2013, 74, 1363–1366. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Jauch, E.C.; Saver, J.L.; Adams, H.P., Jr.; Bruno, A.; Connors, J.J.B.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W., Jr.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef]
- De la Garza Ramos, R.; Benton, J.A.; Gelfand, Y.; Echt, M.; Flores Rodriguez, J.V.; Yanamadala, V.; Yassari, R. Racial disparities in clinical presentation, type of intervention, and in-hospital outcomes of patients with metastatic spine disease: An analysis of 145,809 admissions in the United States. Cancer Epidemiol. 2020, 68, 101792. [Google Scholar] [CrossRef] [PubMed]
- Oldenburger, E.; Brown, S.; Willmann, J.; van der Velden, J.M.; Spałek, M.; van der Linden, Y.M.; Kazmierska, J.; Menten, J.; Andratschke, N.; Hoskin, P. ESTRO ACROP guidelines for external beam radiotherapy of patients with complicated bone metastases. Radiother. Oncol. 2022, 173, 240–253. [Google Scholar] [CrossRef]
- Patchell, R.A.; Tibbs, P.A.; Regine, W.F.; Payne, R.; Saris, S.; Kryscio, R.J.; Mohiuddin, M.; Young, B. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: A randomised trial. Lancet 2005, 366, 643–648. [Google Scholar] [CrossRef] [Green Version]
- Itshayek, E.; Yamada, J.; Bilsky, M.; Schmidt, M.; Shaffrey, C.; Gerszten, P.; Polly, D.; Gokaslan, Z.; Varga, P.P.; Fisher, C.G. Timing of surgery and radiotherapy in the management of metastatic spine disease: A systematic review. Int. J. Oncol. 2010, 36, 533–544. [Google Scholar] [CrossRef] [Green Version]
- Abu-Hegazy, M.; Wahba, H.A. Single-versus multi-fraction radiation treatment for metastatic spinal cord compression: Functional outcome study. Chin. Ger. J. Clin. Oncol. 2011, 10, 535–540. [Google Scholar] [CrossRef]
- Maranzano, E.; Trippa, F.; Casale, M.; Costantini, S.; Lupattelli, M.; Bellavita, R.; Marafioti, L.; Pergolizzi, S.; Santacaterina, A.; Mignogna, M.; et al. 8Gy single-dose radiotherapy is effective in metastatic spinal cord compression: Results of a phase III randomized multicentre Italian trial. Radiother. Oncol. 2009, 93, 174–179. [Google Scholar] [CrossRef]
- Hoskin, P.J.; Hopkins, K.; Misra, V.; Holt, T.; McMenemin, R.; Dubois, D.; McKinna, F.; Foran, B.; Madhavan, K.; MacGregor, C.; et al. Effect of Single-Fraction vs Multifraction Radiotherapy on Ambulatory Status Among Patients with Spinal Canal Compression From Metastatic Cancer: The SCORAD Randomized Clinical Trial. JAMA 2019, 322, 2084–2094. [Google Scholar] [CrossRef]
- Lee, K.A.; Dunne, M.; Small, C.; Kelly, P.J.; McArdle, O.; O’Sullivan, J.; Hacking, D.; Pomeroy, M.; Armstrong, J.; Moriarty, M.; et al. (ICORG 05-03): Prospective randomized non-inferiority phase III trial comparing two radiation schedules in malignant spinal cord compression (not proceeding with surgical decompression); the quality of life analysis. Acta Oncol. 2018, 57, 965–972. [Google Scholar] [CrossRef]
- Donovan, E.K.; Sienna, J.; Mitera, G.; Kumar-Tyagi, N.; Parpia, S.; Swaminath, A. Single versus multifraction radiotherapy for spinal cord compression: A systematic review and meta-analysis. Radiother. Oncol. 2019, 134, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Kirshblum, S.C.; Burns, S.P.; Biering-Sorensen, F.; Donovan, W.; Graves, D.E.; Jha, A.; Johansen, M.; Jones, L.; Krassioukov, A.; Mulcahey, M.J.; et al. International standards for neurological classification of spinal cord injury (revised 2011). J. Spinal Cord Med. 2011, 34, 535–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilsky, M.H.; Laufer, I.; Fourney, D.R.; Groff, M.; Schmidt, M.H.; Varga, P.P.; Vrionis, F.D.; Yamada, Y.; Gerszten, P.C.; Kuklo, T.R. Reliability analysis of the epidural spinal cord compression scale. J. Neurosurg. Spine 2010, 13, 324–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koswig, S.; Budach, V. Remineralization and pain relief in bone metastases after after different radiotherapy fractions (10 times 3 Gy vs. 1 time 8 Gy). A prospective study. Strahlenther. Onkol. 1999, 175, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Hakim, S.G.; Bajrovic, A.; Karstens, J.H.; Veninga, T.; Rudat, V.; Schild, S.E. Impact of zoledronic acid on control of metastatic spinal cord compression. Strahlenther. Onkol. 2012, 188, 910–916. [Google Scholar] [CrossRef]
- Guerin, P.; El Fegoun, A.B.; Obeid, I.; Gille, O.; Lelong, L.; Luc, S.; Bourghli, A.; Cursolle, J.C.; Pointillart, V.; Vital, J.-M. Incidental durotomy during spine surgery: Incidence, management and complications. A retrospective review. Injury 2012, 43, 397–401. [Google Scholar] [CrossRef]
- Swann, M.C.; Hoes, K.S.; Aoun, S.G.; McDonagh, D.L. Postoperative complications of spine surgery. Best Pract. Res. Clin. Anaesthesiol. 2016, 30, 103–120. [Google Scholar] [CrossRef]
- Tarawneh, A.M.; Pasku, D.; Quraishi, N.A. Surgical complications and re-operation rates in spinal metastases surgery: A systematic review. Eur. Spine J. 2021, 30, 2791–2799. [Google Scholar] [CrossRef]
- Marks, L.B.; Yorke, E.D.; Jackson, A.; Ten Haken, R.K.; Constine, L.S.; Eisbruch, A.; Bentzen, S.M.; Nam, J.; Deasy, J.O. Use of normal tissue complication probability models in the clinic. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S10–S19. [Google Scholar] [CrossRef] [Green Version]
- Sahgal, A.; Chang, J.H.; Ma, L.; Marks, L.B.; Milano, M.T.; Medin, P.; Niemierko, A.; Soltys, S.G.; Tomé, W.A.; Wong, C.S.; et al. Spinal cord dose tolerance to stereotactic body radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 124–136. [Google Scholar] [CrossRef] [Green Version]
- Boussios, S.; Cooke, D.; Hayward, C.; Kanellos, F.S.; Tsiouris, A.K.; Chatziantoniou, A.A.; Zakynthinakis-Kyriakou, N.; Karathanasi, A. Metastatic spinal cord compression: Unraveling the diagnostic and therapeutic challenges. Anticancer Res. 2018, 38, 4987–4997. [Google Scholar] [CrossRef] [Green Version]
- Fisher, C.G.; DiPaola, C.P.; Ryken, T.C.; Bilsky, M.H.; Shaffrey, C.I.; Berven, S.H.; Harrop, J.S.; Fehlings, M.G.; Boriani, S.; Chou, D.; et al. A novel classification system for spinal instability in neoplastic disease: An evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 2010, 35, E1221–E1229. [Google Scholar] [CrossRef] [Green Version]
- Serratrice, N.; Faddoul, J.; Tarabay, B.; Attieh, C.; Chalah, M.A.; Ayache, S.S.; Abi Lahoud, G.N. Ten years after SINS: Role of surgery and radiotherapy in the management of patients with vertebral metastases. Front. Oncol. 2022, 12, 802595. [Google Scholar] [CrossRef]
- Bentzen, S.M.; Joiner, M.C. The Linear-Quadratic Approach in Clinical Practice. In Basic Clinical Radiobiology, 5th ed.; Joiner, M.C., van der Kogel, A.J., Eds.; CRC Press: Boca Raton, FL, USA; Taylor & Francis Group: Abingdon, UK, 2018; pp. 112–124. ISBN 9780429490606. [Google Scholar]
- Vogelius, I.R.; Bentzen, S.M. Meta-analysis of the alpha/beta ratio for prostate cancer in the presence of an overall time factor: Bad news, good news, or no news? Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Barendsen, G.W. Dose fractionation, dose rate and iso-effect relationships for normal tissue responses. Int. J. Radiat. Oncol. Biol. Phys. 1982, 8, 1981–1997. [Google Scholar] [CrossRef]
- Qi, X.S.; White, J.; Li, X.A. Is α/β for breast cancer really low? Radiother. Oncol. 2011, 100, 282–288. [Google Scholar] [CrossRef]
- van Leeuwen, C.M.; Oei, A.L.; Crezee, J.; Bel, A.; Franken, N.A.P.; Stalpers, L.J.A.; Kok, H.P. The alfa and beta of tumours: A review of parameters of the linear-quadratic model, derived from clinical radiotherapy studies. Radiat. Oncol. 2018, 13, 96. [Google Scholar] [CrossRef]
- Thames, H.D.; Withers, H.R.; Peters, L.J.; Fletcher, G.H. Changes in early and late radiation responses with altered dose fractionation: Implications for dose-survival relationships. Int. J. Radiat. Oncol. Biol. Phys. 1982, 8, 219–226. [Google Scholar] [CrossRef]
- Gerszten, P.C.; Mendel, E.; Yamada, Y. Radiotherapy and radiosurgery for metastatic spine disease: What are the options, indications, and outcomes? Spine 2009, 34, S78–S92. [Google Scholar] [CrossRef]
- Rades, D.; Cacicedo, J.; Conde-Moreno, A.J.; Segedin, B.; But-Hadzic, J.; Groselj, B.; Kevlishvili, G.; Lomidze, D.; Ciervide-Jurio, R.; Rubio, C.; et al. Precision Radiation Therapy for Metastatic Spinal Cord Compression: Final Results of the PRE-MODE Trial. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 780–789. [Google Scholar] [CrossRef]
- Sprave, T.; Verma, V.; Förster, R.; Schlampp, I.; Bruckner, T.; Bostel, T.; Welte, S.E.; Tonndorf-Martini, E.; Nicolay, N.H.; Debus, J.; et al. Randomized phase II trial evaluating pain response in patients with spinal metastases following stereotactic body radiotherapy versus three-dimensional conformal radiotherapy. Radiother. Oncol. 2018, 128, 274–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahgal, A.; Myrehaug, S.D.; Siva, S.; Masucci, G.L.; Maralani, P.J.; Brundage, M.; Butler, J.; Chow, E.; Fehlings, M.G.; Foote, M.; et al. Stereotactic body radiotherapy versus conventional external beam radiotherapy in patients with painful spinal metastases: An open-label, multicentre, randomised, controlled, phase 2/3 trial. Lancet Oncol. 2021, 22, 1023–1033. [Google Scholar] [CrossRef] [PubMed]
- Pielkenrood, B.J.; van der Velden, J.M.; van der Linden, Y.M.; Bartels, M.M.T.; Kasperts, N.; Verhoeff, J.J.C.; Eppinga, W.S.C.; Gal, R.; Verlaan, J.J.; Verkooijen, H.M.L. Pain Response After Stereotactic Body Radiation Therapy Versus Conventional Radiation Therapy in Patients With Bone Metastases—A Phase 2 Randomized Controlled Trial Within a Prospective Cohort. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Q.-N.; Chun, S.G.; Chow, E.; Komaki, R.; Liao, Z.; Zacharia, R.; Szeto, B.K.; Welsh, J.W.; Hahn, S.M.; Fuller, C.D.; et al. Single-Fraction Stereotactic vs Conventional Multifraction Radiotherapy for Pain Relief in Patients With Predominantly Nonspine Bone Metastases: A Randomized Phase 2 Trial. JAMA Oncol. 2019, 5, 872–878. [Google Scholar] [CrossRef] [Green Version]
- Berwouts, D.; De Wolf, K.; Lambert, B.; Bultijnck, R.; De Neve, W.; De Lobel, L.; Jans, L.; Goetghebeur, E.; Speleers, B.; Olteanu, L.A.M.; et al. Biological 18[F]-FDG-PET image-guided dose painting by numbers for painful uncomplicated bone metastases: A 3-arm randomized phase II trial. Radiother. Oncol. 2015, 115, 272–278. [Google Scholar] [CrossRef]
- Sahgal, A.; Whyne, C.M.; Ma, L.; Larson, D.A.; Fehlings, M.G. Vertebral compression fracture after stereotactic body radiotherapy for spinal metastases. Lancet Oncol. 2013, 14, e310–e320. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef]
- Rades, D.; Rudat, V.; Veninga, T.; Stalpers, L.J.A.; Basic, H.; Karstens, J.H.; Hoskin, P.J.; Schild, S.E. A score predicting posttreatment ambulatory status in patients irradiated for metastatic spinal cord compression. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 905–908. [Google Scholar] [CrossRef]
- Rades, D.; Douglas, S.; Huttenlocher, S.; Rudat, V.; Veninga, T.; Stalpers, L.J.A.; Basic, H.; Karstens, J.H.; Hoskin, P.J.; Adamietz, I.A.; et al. Validation of a score predicting post-treatment ambulatory status after radiotherapy for metastatic spinal cord compression. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1503–1506. [Google Scholar] [CrossRef]
- Rades, D.; Al-Salool, A.; Staackmann, C.; Cremers, F.; Cacicedo, J.; Lomidze, D.; Segedin, B.; Groselj, B.; Jankarashvili, N.; Conde-Moreno, A.J.; et al. A New Clinical Instrument for Estimating the Ambulatory Status after Irradiation for Malignant Spinal Cord Compression. Cancers 2022, 14, 3827. [Google Scholar] [CrossRef]
- Rispoli, R.; Reverberi, C.; Targato, G.; D’Agostini, S.; Fasola, G.; Trovò, M.; Calci, M.; Fanin, R.; Cappelletto, B. Multidisciplinary approach to patients with metastatic spinal cord compression: A diagnostic therapeutic algorithm to improve the neurological outcome. Front. Oncol. 2022, 12, 902928. [Google Scholar] [CrossRef] [PubMed]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.-S.; Sonke, G.S.; Hart, L.; Campone, M.; Petrakova, K.; Winer, E.P.; Janni, W.; et al. Overall Survival with Ribociclib plus Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2022, 386, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Swain, S.M.; Miles, D.; Kim, S.-B.; Im, Y.-H.; Im, S.-A.; Semiglazov, V.; Ciruelos, E.; Schneeweiss, A.; Loi, S.; Monturus, E.; et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): End-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2020, 21, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Chi, K.N.; Chowdhury, S.; Bjartell, A.; Chung, B.H.; de Santana Gomes, A.J.P.; Given, R.; Juárez, A.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide in Patients With Metastatic Castration-Sensitive Prostate Cancer: Final Survival Analysis of the Randomized, Double-Blind, Phase III TITAN Study. J. Clin. Oncol. 2021, 39, 2294–2303. [Google Scholar] [CrossRef]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Waddell, T.; Gafanov, R.; Pouliot, F.; Nosov, D.; Melichar, B.; Soulieres, D.; Borchiellini, D.; et al. Pembrolizumab (pembro) plus axitinib (axi) versus sunitinib as first-line therapy for advanced clear cell renal cell carcinoma (ccRCC): Results from 42-month follow-up of KEYNOTE-426. J. Clin. Oncol. 2021, 39, 4500. [Google Scholar] [CrossRef]
- Braunlin, M.; Belani, R.; Buchanan, J.; Wheeling, T.; Kim, C. Trends in the multiple myeloma treatment landscape and survival: A U.S. analysis using 2011-2019 oncology clinic electronic health record data. Leuk. Lymphoma 2021, 62, 377–386. [Google Scholar] [CrossRef]
- Godby, R.C.; Johnson, D.B.; Williams, G.R. Immunotherapy in Older Adults with Cancer. Curr. Oncol. Rep. 2019, 21, 56. [Google Scholar] [CrossRef]
- Kanesvaran, R.; Cordoba, R.; Maggiore, R. Immunotherapy in Older Adults With Advanced Cancers: Implications for Clinical Decision-Making and Future Research. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 400–414. [Google Scholar] [CrossRef]
- Wilkinson, P.M.; Read, G. International Germ Cell Consensus Classification: A prognostic factor-based staging system for metastatic germ cell cancers. International Germ Cell Cancer Collaborative Group. J. Clin. Oncol. 1997, 15, 594–603. [Google Scholar] [CrossRef]
- Gridelli, C.; Rossi, A.; Carbone, D.P.; Guarize, J.; Karachaliou, N.; Mok, T.; Petrella, F.; Spaggiari, L.; Rosell, R. Non-small-cell lung cancer. Nat. Rev. Dis. Primers 2015, 1, 15009. [Google Scholar] [CrossRef]
- Tomita, K.; Kawahara, N.; Kobayashi, T.; Yoshida, A.; Murakami, H.; Akamaru, T. Surgical strategy for spinal metastases. Spine 2001, 26, 298–306. [Google Scholar] [CrossRef]
- Tokuhashi, Y.; Matsuzaki, H.; Toriyama, S.; Kawano, H.; Ohsaka, S. Scoring system for the preoperative evaluation of metastatic spine tumor prognosis. Spine 1990, 15, 1110–1113. [Google Scholar] [CrossRef]
- Tokuhashi, Y.; Matsuzaki, H.; Oda, H.; Oshima, M.; Ryu, J. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine 2005, 30, 2186–2191. [Google Scholar] [CrossRef]
- Candido, P.B.M.; Perria, F.M.; Costa, H.R.D.; Defino, H.L.A. A comparison of the tomita and tokuhashi scores in spinal metastasis. Coluna/Columna 2020, 19, 297–301. [Google Scholar] [CrossRef]
- Aoude, A.; Amiot, L.-P. A comparison of the modified Tokuhashi and Tomita scores in determining prognosis for patients afflicted with spinal metastasis. Can. J. Surg. 2014, 57, 188–193. [Google Scholar] [CrossRef] [Green Version]
- Pereira, N.R.P.; Janssen, S.J.; van Dijk, E.; Harris, M.B.; Hornicek, F.J.; Ferrone, M.L.; Schwab, J.H. Development of a Prognostic Survival Algorithm for Patients with Metastatic Spine Disease. J. Bone Joint Surg. Am. 2016, 98, 1767–1776. [Google Scholar] [CrossRef]
- Zegarek, G.; Tessitore, E.; Chaboudez, E.; Nouri, A.; Schaller, K.; Gondar, R. SORG algorithm to predict 3- and 12-month survival in metastatic spinal disease: A cross-sectional population-based retrospective study. Acta Neurochir. 2022, 164, 2627–2635. [Google Scholar] [CrossRef]
- Tseng, T.-E.; Lee, C.-C.; Yen, H.-K.; Groot, O.Q.; Hou, C.-H.; Lin, S.-Y.; Bongers, M.E.R.; Hu, M.-H.; Karhade, A.V.; Ko, J.-C.; et al. International Validation of the SORG Machine-learning Algorithm for Predicting the Survival of Patients with Extremity Metastases Undergoing Surgical Treatment. Clin. Orthop. Relat. Res. 2022, 480, 367–378. [Google Scholar] [CrossRef]
- Zhong, G.; Cheng, S.; Zhou, M.; Xie, J.; Xu, Z.; Lai, H.; Yan, Y.; Xie, Z.; Zhou, J.; Xie, X.; et al. External validation of the SORG machine learning algorithms for predicting 90-day and 1-year survival of patients with lung cancer-derived spine metastases—A recent bi-center cohort from China. Spine J. 2023. [Google Scholar] [CrossRef]
- Li, Z.; Guo, L.; Guo, B.; Zhang, P.; Wang, J.; Wang, X.; Yao, W. Evaluation of different scoring systems for spinal metastases based on a Chinese cohort. Cancer Med. 2022. [Google Scholar] [CrossRef]
- Ghori, A.K.; Leonard, D.A.; Schoenfeld, A.J.; Saadat, E.; Scott, N.; Ferrone, M.L.; Pearson, A.M.; Harris, M.B. Modeling 1-year survival after surgery on the metastatic spine. Spine J. 2015, 15, 2345–2350. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, A.J.; Le, H.V.; Marjoua, Y.; Leonard, D.A.; Belmont, P.J.; Bono, C.M.; Harris, M.B. Assessing the utility of a clinical prediction score regarding 30-day morbidity and mortality following metastatic spinal surgery: The New England Spinal Metastasis Score (NESMS). Spine J. 2016, 16, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, A.J.; Ferrone, M.L.; Schwab, J.H.; Blucher, J.A.; Barton, L.B.; Tobert, D.G.; Chi, J.H.; Shin, J.H.; Kang, J.D.; Harris, M.B. Prospective validation of a clinical prediction score for survival in patients with spinal metastases: The New England Spinal Metastasis Score. Spine J. 2021, 21, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Laufer, I.; Rubin, D.G.; Lis, E.; Cox, B.W.; Stubblefield, M.D.; Yamada, Y.; Bilsky, M.H. The NOMS framework: Approach to the treatment of spinal metastatic tumors. Oncologist 2013, 18, 744–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, Y.; Lei, M.; Pan, Y.; Lin, Y.; Shi, X. Scoring algorithms for predicting survival prognosis in patients with metastatic spinal disease: The current status and future directions. Clin. Spine Surg. 2020, 33, 296–306. [Google Scholar] [CrossRef]
- Paton, G.R.; Frangou, E.; Fourney, D.R. Contemporary treatment strategy for spinal metastasis: The “LMNOP” system. Can. J. Neurol. Sci. 2011, 38, 396–403. [Google Scholar] [CrossRef] [Green Version]
- Pennington, Z.; Ahmed, A.K.; Westbroek, E.M.; Cottrill, E.; Lubelski, D.; Goodwin, M.L.; Sciubba, D.M. SINS score and stability: Evaluating the need for stabilization within the uncertain category. World Neurosurg. 2019, 128, e1034–e1047. [Google Scholar] [CrossRef]
- Ivanishvili, Z.; Fourney, D.R. Incorporating the Spine Instability Neoplastic Score into a Treatment Strategy for Spinal Metastasis: LMNOP. Global Spine J. 2014, 4, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Spratt, D.E.; Beeler, W.H.; de Moraes, F.Y.; Rhines, L.D.; Gemmete, J.J.; Chaudhary, N.; Shultz, D.B.; Smith, S.R.; Berlin, A.; Dahele, M.; et al. An integrated multidisciplinary algorithm for the management of spinal metastases: An International Spine Oncology Consortium report. Lancet Oncol. 2017, 18, e720–e730. [Google Scholar] [CrossRef]
- Giammalva, G.R.; Ferini, G.; Torregrossa, F.; Brunasso, L.; Musso, S.; Benigno, U.E.; Gerardi, R.M.; Bonosi, L.; Costanzo, R.; Paolini, F.; et al. The palliative care in the metastatic spinal tumors. A systematic review on the radiotherapy and surgical per-spective. Life 2022, 12, 571. [Google Scholar] [CrossRef]



| Professional | Roles | |
|---|---|---|
| Before spinal cord compression | Medical oncologist | Prognostication of the disease and definition of systemic treatment of both tumors and metastases (refer to the discussion of bone-targeted agents, as mentioned in Section 1.1); patient care coordination |
| Radiation oncologist | Local treatment of symptomatic metastatic disease (and possibly the primary tumor, when indicated) | |
| Spinal ourgeon | Assessment of the risk of spinal cord compression; preemptive decompression or stabilization | |
| Radiologist | Assessment of the risk of spinal cord compression; diagnosis of the likely primary tumor; image-directed biopsy of the primary tumor or metastasis | |
| Pathologist | Histological diagnosis from tissue samples of the primary tumor or metastasis (essential for prognostication and systemic treatment) | |
| Palliative care specialist | Assessment and treatment of physical, emotional, and spiritual distress | |
| Acute spinal cord compression | Assisting doctor in the emergency department | Often the first to encounter the patient, especially if the cancer is not yet known Diagnosis/suspicion of spinal cord compression and activation of the proper care pathways Organ support in the perioperative period (neurogenic shock and ventilatory failure) |
| Medical oncologist | Prognostication of the disease (there is a very limited role for cancer-directed systemic therapy at this stage) | |
| Radiation oncologist | Metastases-directed treatment, with or without surgery | |
| Spinal surgeon | Spinal cord decompression, stabilization, and/or resection of the neoplastic lesion Can obtain specimen for histological diagnosis | |
| Radiologist | Differential diagnosis of the neurological syndrome | |
| After spinal cord compression (established neurological deficit and permanent disability) | Medical oncologist | Treatment of the systemic disease to prevent further deterioration and increase survival and quality of life |
| Radiation oncologist | Treatment directed to metastases or primary tumor (if indicated) | |
| Spinal surgeon | Decompression and stabilization to prevent deterioration, treat pain and allow for early mobilization Can obtain specimen for histological diagnosis if there is no diagnosis at this stage | |
| Rehabilitation specialist | Optimization of the remaining neurological function to increase patient autonomy and preserve quality of life Assistive devices to improve patient autonomy and safety | |
| Palliative care specialist | Assessment and treatment of physical, emotional, and spiritual distress related to the systemic disease and neurological complications |
| Responsive to Radiation | Resistant to Radiation |
|---|---|
| Lymphomas (high α/β) * | Malignant melanoma (low α/β) |
| Multiple myeloma (high α/β) * | Renal cell cancer (low α/β) |
| Small cell lung cancer (high α/β) | Non-small cell lung cancer (low α/β) |
| Germ cell tumors (high α/β) * | Gastrointestinal cancers (low α/β) |
| Prostate cancer (low α/β) | Sarcomas (low α/β **) |
| Breast cancer (low α/β) |
| Variable | Post-RT Ambulatory Rate, Percent | Score |
|---|---|---|
| Type of primary tumor | ||
| Breast cancer | 81 | 8 |
| Prostate cancer | 68 | 7 |
| Myeloma/lymphoma | 89 | 9 |
| Non-small cell lung cancer | 54 | 5 |
| Small cell lung cancer | 64 | 6 |
| Cancer of unknown primary | 45 | 5 |
| Renal cell carcinoma | 62 | 6 |
| Colorectal cancer | 64 | 6 |
| Other tumors | 59 | 6 |
| Interval from tumor diagnosis to MSCC | ||
| ≤15 months | 58 | 6 |
| >15 months | 78 | 8 |
| Motor function before RT | ||
| Ambulatory without aid | 98 | 10 |
| Ambulatory with aid | 89 | 9 |
| Not ambulatory | 28 | 3 |
| Paraplegic | 7 | 1 |
| Time of developing motor deficits before RT | ||
| 1–7 days | 37 | 4 |
| 8–14 days | 69 | 7 |
| >14 days | 88 | 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esperança-Martins, M.; Roque, D.; Barroso, T.; Abrunhosa-Branquinho, A.; Belo, D.; Simas, N.; Costa, L. Multidisciplinary Approach to Spinal Metastases and Metastatic Spinal Cord Compression—A New Integrative Flowchart for Patient Management. Cancers 2023, 15, 1796. https://doi.org/10.3390/cancers15061796
Esperança-Martins M, Roque D, Barroso T, Abrunhosa-Branquinho A, Belo D, Simas N, Costa L. Multidisciplinary Approach to Spinal Metastases and Metastatic Spinal Cord Compression—A New Integrative Flowchart for Patient Management. Cancers. 2023; 15(6):1796. https://doi.org/10.3390/cancers15061796
Chicago/Turabian StyleEsperança-Martins, Miguel, Diogo Roque, Tiago Barroso, André Abrunhosa-Branquinho, Diogo Belo, Nuno Simas, and Luis Costa. 2023. "Multidisciplinary Approach to Spinal Metastases and Metastatic Spinal Cord Compression—A New Integrative Flowchart for Patient Management" Cancers 15, no. 6: 1796. https://doi.org/10.3390/cancers15061796