
Is It Time to Integrate Frailty Assessment in Onconephrology?

Abstract
:Simple Summary
Abstract
1. Introduction
2. Definition and Operationalization of Frailty
2.1. Kidney Disease
2.2. Oncology
2.3. Cognitive Frailty
2.4. Geriatric Assessment
2.5. Assessing Frailty Using a Virtual Approach
3. Clinical Significance of Frailty Assessment in Onconephrology
3.1. Renal Cell Carcinoma
3.2. Concurrent Cancer and Kidney Disease
4. Current Approaches to Frailty Assessment in Onconephrology
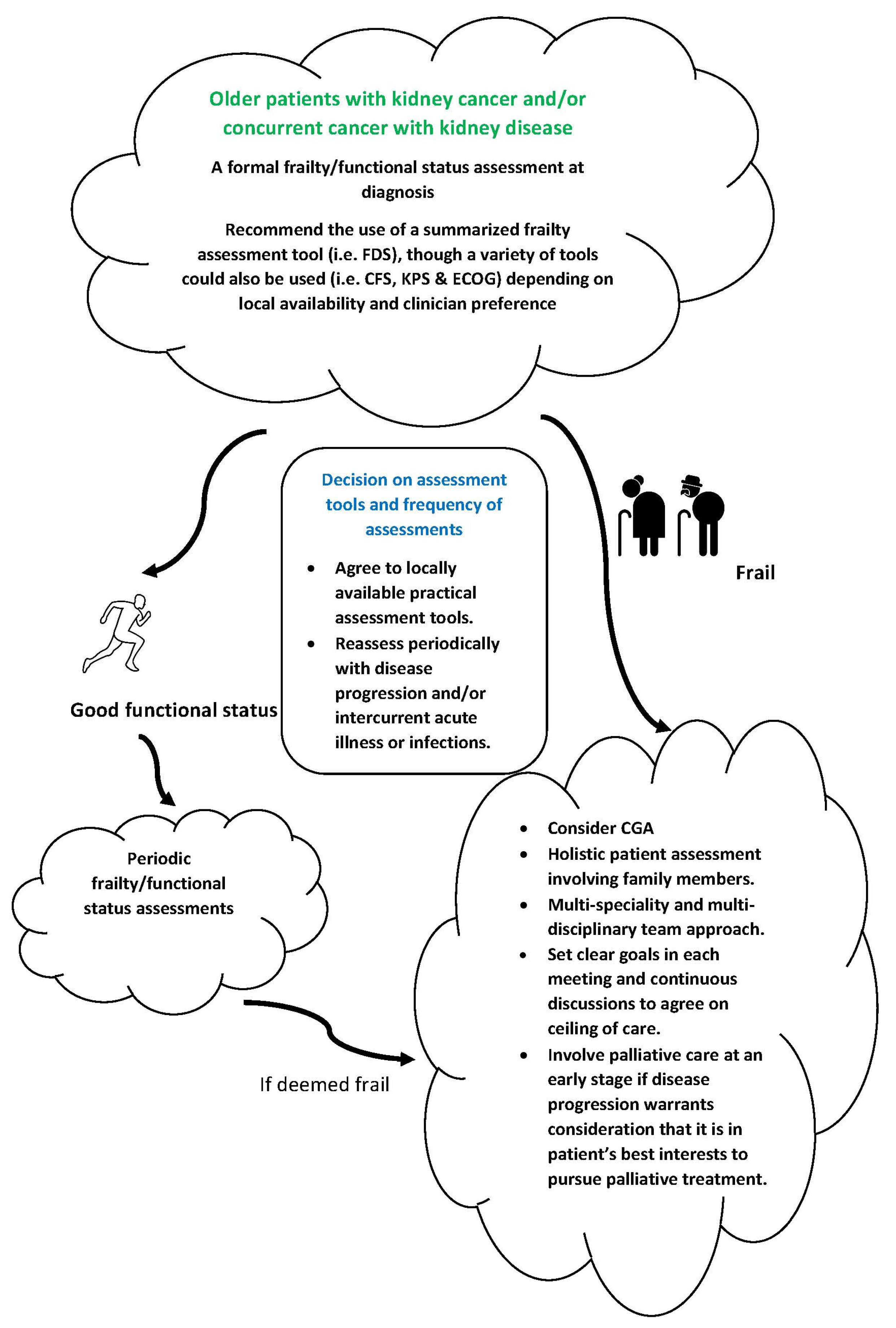
5. Recommendations for a Summarized Frailty Assessment Tool in Onconephrology
6. Summary and Future Areas of Development for Frailty Assessment in Onconephrology
Author Contributions
Funding
Conflicts of Interest
References
- Rosner, M.H.; Jhaveri, K.D.; McMahon, B.A.; Perazella, M.A. Onconephrology: The intersections between the kidney and cancer. CA A Cancer J. Clin. 2021, 71, 47–77. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallenberg, M.H.; Kleinveld, H.A.; Dekker, F.W.; van Munster, B.C.; Rabelink, T.J.; van Buren, M.; Mooijaart, S.P. Functional and cognitive impairment, frailty, and adverse health outcomes in older patients reaching ESRD—A systematic review. Clin. J. Am. Soc. Nephrol. 2016, 11, 1624–1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, S.R.; Gill, K.; Macdonald, K.; Komenda, P.; Rigatto, C.; Sood, M.M.; Bohm, C.J.; Storsley, L.J.; Tangri, N. Association of frailty and physical function in patients with non-dialysis CKD: A systematic review. BMC Nephrol. 2013, 14, 228. [Google Scholar] [CrossRef] [Green Version]
- McAdams-DeMarco, M.A.; Law, A.; Salter, M.L.; Boyarsky, B.; Gimenez, L.; Jaar, B.G.; Walston, J.D.; Segev, D.L. Frailty as a novel predictor of mortality and hospitalization in individuals of all ages undergoing hemodialysis. J. Am. Geriatr. Soc. 2013, 61, 896–901. [Google Scholar] [CrossRef] [Green Version]
- Walston, J.; Hadley, E.C.; Ferrucci, L.; Guralnik, J.M.; Newman, A.B.; Studenski, S.A.; Ershler, W.B.; Harris, T.; Fried, L.P. Research agenda for frailty in older adults: Toward a better understanding of physiology and etiology: Summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J. Am. Geriatr. Soc. 2006, 54, 991–1001. [Google Scholar] [CrossRef]
- Cheng, X.S.; Lentine, K.L.; Koraishy, F.M.; Myers, J.; Tan, J.C. Implications of frailty for peritransplant outcomes in kidney transplant recipients. Curr. Transplant. Rep. 2019, 6, 16–25. [Google Scholar] [CrossRef] [Green Version]
- McAdams-DeMarco, M.A.; Chu, N.M.; Segev, D.L. Frailty and long-term post-kidney transplant outcomes. Curr. Transplant. Rep. 2019, 6, 45–51. [Google Scholar] [CrossRef]
- Morton, S.; Isted, A.; Avery, P.; Wang, J. Is frailty a predictor of outcomes in elderly inpatients with acute kidney injury? A prospective cohort study. Am. J. Med. 2018, 131, 1251–1256. [Google Scholar] [CrossRef]
- Jiesisibieke, Z.L.; Tung, T.H.; Xu, Q.Y.; Chen, P.E.; Hsu, S.Y.; Liu, Y.; Chien, C.W. Association of acute kidney injury with frailty in elderly population: A systematic review and meta-analysis. Ren. Fail. 2019, 41, 1021–1027. [Google Scholar] [CrossRef]
- Bao, Y.; Dalrymple, L.; Chertow, G.M.; Kaysen, G.A.; Johansen, K.L. Frailty, dialysis initiation, and mortality in end-stage renal disease. Arch. Intern. Med. 2012, 172, 1071–1077. [Google Scholar] [CrossRef]
- Nixon, A.C.; Bampouras, T.M.; Pendleton, N.; Woywodt, A.; Mitra, S.; Dhaygude, A. Frailty and chronic kidney disease: Current evidence and continuing uncertainties. Clin. Kidney J. 2018, 11, 236–245. [Google Scholar] [CrossRef] [Green Version]
- Carrero, J.J.; Stenvinkel, P.; Cuppari, L.; Ikizler, T.A.; Kalantar-Zadeh, K.; Kaysen, G.; Mitch, W.E.; Price, S.R.; Wanner, C.; Wang, A.Y.; et al. Etiology of the protein-energy wasting syndrome in chronic kidney disease: A consensus statement from the International Society of Renal Nutrition and Metabolism (ISRNM). J. Ren. Nutr. 2013, 23, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.C.; Kalantar-Zadeh, K.; Kopple, J.D. Frailty and protein-energy wasting in elderly patients with end stage kidney disease. J. Am. Soc. Nephrol. 2013, 24, 337–351. [Google Scholar] [CrossRef] [Green Version]
- Beddhu, S.; Baird, B.C.; Zitterkoph, J.; Neilson, J.; Greene, T. Physical activity and mortality in chronic kidney disease (NHANES III). Clin. J. Am. Soc. Nephrol. 2009, 4, 1901–1906. [Google Scholar] [CrossRef] [Green Version]
- Górriz, J.L.; Molina, P.; Bover, J.; Barril, G.; Martín-de Francisco, Á.L.; Caravaca, F.; Hervás, J.; Piñera, C.; Escudero, V.; Molinero, L.M. Characteristics of bone mineral metabolism in patients with stage 3-5 chronic kidney disease not on dialysis: Results of the OSERCE study. Nephrology 2013, 33, 46–60. [Google Scholar]
- Handforth, C.; Clegg, A.; Young, C.; Simpkins, S.; Seymour, M.T.; Selby, P.J.; Young, J. The prevalence and outcomes of frailty in older cancer patients: A systematic review. Ann. Oncol. 2015, 26, 1091–1101. [Google Scholar] [CrossRef]
- Ethun, C.G.; Bilen, M.A.; Jani, A.B.; Maithel, S.K.; Ogan, K.; Master, V.A. Frailty and cancer: Implications for oncology surgery, medical oncology, and radiation oncology. CA A Cancer J. Clin. 2017, 67, 362–377. [Google Scholar] [CrossRef] [Green Version]
- Nishijima, T.F.; Deal, A.M.; Williams, G.R.; Guerard, E.J.; Nyrop, K.A.; Muss, H.B. Frailty and inflammatory markers in older adults with cancer. Aging 2017, 9, 650–661. [Google Scholar] [CrossRef] [Green Version]
- Bruijnen, C.P.; Koldenhof, J.J.; Verheijden, R.J.; van den Bos, F.; Emmelot-Vonk, M.H.; Witteveen, P.O.; Suijkerbuijk, K.P. Frailty and checkpoint inhibitor toxicity in older patients with melanoma. Cancer 2022, 128, 2746–2752. [Google Scholar] [CrossRef]
- Chappidi, M.R.; Kates, M.; Patel, H.D.; Tosoian, J.J.; Kaye, D.R.; Sopko, N.A.; Lascano, D.; Liu, J.J.; McKiernan, J.; Bivalacqua, T.J. Frailty as a marker of adverse outcomes in patients with bladder cancer undergoing radical cystectomy. Urol. Oncol. 2016, 34, 256.e1–256.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boenink, R.; Astley, M.E.; Huijben, J.A.; Stel, V.S.; Kerschbaum, J.; Ots-Rosenberg, M.; Asberg, A.A.; Lopot, F.; Golan, E.; Castro de la Nuez, P.; et al. The ERA Registry Annual Report 2019, summary and age comparisons. Clin. Kidney J. 2022, 15, 452–472. [Google Scholar] [CrossRef] [PubMed]
- Bowling, C.B.; Sharma, P.; Fox, C.S.; O’Hare, A.M.; Muntner, P. Prevalence of reduced estimated glomerular filtration rate among the oldest old from 1988–1994 through 2005–2010. JAMA 2013, 310, 1284–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilleron, S.; Sarfati, D.; Janssen-Heijnen, M.; Vignat, J.; Ferlay, J.; Bray, F.; Soerjomataram, I. Global cancer incidence in older adults, 2012 and 2035, A population-based study. Int. J. Cancer 2019, 144, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Quinn, R.R.; Lam, N.N.; Al-Wahsh, H.; Sood, M.M.; Tangri, N.; Tonelli, M.; Ravani, P. Progression and Regression of Chronic Kidney Disease by Age Among Adults in a Population-Based Cohort in Alberta, Canada. JAMA Netw. Open 2021, 4, e2112828. [Google Scholar] [CrossRef]
- Hamczyk, M.R.; Nevado, R.M.; Barettino, A.; Fuster, V.; Andres, V. Biological Versus Chronological Aging: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 75, 919–930. [Google Scholar] [CrossRef]
- Ortiz, A.; Mattace-Raso, F.; Soler, M.J.; Fouque, D. Ageing meets kidney disease. Clin. Kidney J. 2022, 15, 1793–1796. [Google Scholar] [CrossRef]
- Rodriguez-Manas, L.; Feart, C.; Mann, G.; Vina, J.; Chatterji, S.; Chodzko-Zajko, W.; Gonzalez-Colaco Harmand, M.; Bergman, H.; Carcaillon, L.; Nicholson, C.; et al. Searching for an operational definition of frailty: A Delphi method based consensus statement: The frailty operative definition-consensus conference project. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2013, 68, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Brar, R.; Whitlock, R.; Komenda, P.; Lerner, B.; Prasad, B.; Bohm, C.; Thorsteinsdottir, B.; Rigatto, C.; Tangri, N. The Impact of Frailty on Technique Failure and Mortality in Patients on Home Dialysis. Perit. Dial. Int. 2019, 39, 532–538. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; King, E.A.; Luo, X.; Haugen, C.; DiBrito, S.; Shaffer, A.; Kucirka, L.M.; Desai, N.M.; Dagher, N.N.; Lonze, B.E.; et al. Frailty, Length of Stay, and Mortality in Kidney Transplant Recipients: A National Registry and Prospective Cohort Study. Ann. Surg. 2017, 266, 1084–1090. [Google Scholar] [CrossRef] [Green Version]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef] [Green Version]
- Hall, R.K.; Morton, S.; Wilson, J.; Kim, D.H.; Colon-Emeric, C.; Scialla, J.J.; Platt, A.; Ephraim, P.L.; Boulware, L.E.; Pendergast, J. Development of an Administrative Data-Based Frailty Index for Older Adults Receiving Dialysis. Kidney360 2022, 3, 1566–1577. [Google Scholar] [CrossRef]
- Worthen, G.; Vinson, A.; Cardinal, H.; Doucette, S.; Gogan, N.; Gunaratnam, L.; Keough-Ryan, T.; Kiberd, B.A.; Prasad, B.; Rockwood, K.; et al. Prevalence of Frailty in Patients Referred to the Kidney Transplant Waitlist. Kidney360 2021, 2, 1287–1295. [Google Scholar] [CrossRef]
- Alfaadhel, T.A.; Soroka, S.D.; Kiberd, B.A.; Landry, D.; Moorhouse, P.; Tennankore, K.K. Frailty and mortality in dialysis: Evaluation of a clinical frailty scale. Clin. J. Am. Soc. Nephrol. 2015, 10, 832–840. [Google Scholar] [CrossRef] [Green Version]
- Clark, D.; Matheson, K.; Miller, A.J.; Kiberd, B.; Tennankore, K. Frailty and Hospitalization in Dialysis: Evaluation of the Clinical Frailty Scale. In Proceedings of the Canadian Society of Nephrology Annual Meeting, Vancouver, BC, Canada, 4–5 May 2018. [Google Scholar]
- Oki, R.; Hamasaki, Y.; Tsuji, S.; Suzuki, K.; Tsuneishi, S.; Imafuku, M.; Komaru, Y.; Miyamoto, Y.; Matsuura, R.; Doi, K.; et al. Clinical frailty assessment might be associated with mortality in incident dialysis patients. Sci. Rep. 2022, 12, 17651. [Google Scholar] [CrossRef]
- Brar, R.S.; Whitlock, R.H.; Komenda, P.V.J.; Rigatto, C.; Prasad, B.; Bohm, C.; Tangri, N. Provider Perception of Frailty Is Associated with Dialysis Decision Making in Patients with Advanced CKD. Clin. J. Am. Soc. Nephrol. 2021, 16, 552–559. [Google Scholar] [CrossRef]
- Clark, D.A.; Khan, U.; Kiberd, B.A.; Turner, C.C.; Dixon, A.; Landry, D.; Moffatt, H.C.; Moorhouse, P.A.; Tennankore, K.K. Frailty in end-stage renal disease: Comparing patient, caregiver, and clinician perspectives. BMC Nephrol. 2017, 18, 148. [Google Scholar] [CrossRef] [Green Version]
- Belkin, M.D.; Doerfler, R.M.; Wagner, L.A.; Zhan, M.; Fink, J.C. Associations of Performance-Based Functional Assessments and Adverse Outcomes in CKD. Kidney360 2021, 2, 629–638. [Google Scholar] [CrossRef]
- Cheng, X.S.; Myers, J.; Han, J.; Stedman, M.R.; Watford, D.J.; Lee, J.; Discipulo, K.V.; Chan, K.N.; Chertow, G.M.; Tan, J.C. Physical Performance Testing in Kidney Transplant Candidates at the Top of the Waitlist. Am. J. Kidney Dis. 2020, 76, 815–825. [Google Scholar] [CrossRef]
- Chowdhury, R.; Peel, N.M.; Krosch, M.; Hubbard, R.E. Frailty and chronic kidney disease: A systematic review. Arch. Gerontol. Geriatr. 2017, 68, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Abel, G.A.; Klepin, H.D. Frailty and the management of hematologic malignancies. Blood 2018, 131, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Azam, F.; Latif, M.F.; Farooq, A.; Tirmazy, S.H.; AlShahrani, S.; Bashir, S.; Bukhari, N. Performance Status Assessment by Using ECOG (Eastern Cooperative Oncology Group) Score for Cancer Patients by Oncology Healthcare Professionals. Case Rep. Oncol. 2019, 12, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, M.; Kasinath, P.; High, R.; Yu, F.; Teply, B.A. Impact of Performance Status on Response and Survival Among Patients Receiving Checkpoint Inhibitors for Advanced Solid Tumors. JCO Oncol. Pract. 2022, 18, e175–e182. [Google Scholar] [CrossRef] [PubMed]
- Schag, C.C.; Heinrich, R.L.; Ganz, P.A. Karnofsky performance status revisited: Reliability, validity, and guidelines. J. Clin. Oncol. 1984, 2, 187–193. [Google Scholar] [CrossRef]
- Chow, R.; Bruera, E.; Temel, J.S.; Krishnan, M.; Im, J.; Lock, M. Inter-rater reliability in performance status assessment among healthcare professionals: An updated systematic review and meta-analysis. Support. Care Cancer 2020, 28, 2071–2078. [Google Scholar] [CrossRef]
- Chow, R.; Zimmermann, C.; Bruera, E.; Temel, J.; Im, J.; Lock, M. Inter-rater reliability in performance status assessment between clinicians and patients: A systematic review and meta-analysis. BMJ Support. Palliat. Care 2020, 10, 129–135. [Google Scholar] [CrossRef]
- Scott, J.M.; Stene, G.; Edvardsen, E.; Jones, L.W. Performance Status in Cancer: Not Broken, But Time for an Upgrade? J. Clin. Oncol. 2020, 38, 2824–2829. [Google Scholar] [CrossRef]
- Sugimoto, T.; Arai, H.; Sakurai, T. An update on cognitive frailty: Its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatr. Gerontol. Int. 2022, 22, 99–109. [Google Scholar] [CrossRef]
- Rockwood, K.; Silvius, J.L.; Fox, R.A. Comprehensive geriatric assessment. Helping your elderly patients maintain functional well-being. Postgrad. Med. 1998, 103, 247–249. [Google Scholar] [CrossRef]
- Brown, E.A.; Farrington, K. Geriatric Assessment in Advanced Kidney Disease. Clin. J. Am. Soc. Nephrol. 2019, 14, 1091–1093. [Google Scholar] [CrossRef] [Green Version]
- Mohile, S.G.; Magnuson, A. Comprehensive geriatric assessment in oncology. Cancer Aging 2013, 38, 85–103. [Google Scholar]
- Novais, T.; Pongan, E.; Gervais, F.; Coste, M.H.; Morelon, E.; Krolak-Salmon, P.; Vernaudon, J. Pretransplant Comprehensive Geriatric Assessment in Older Patients with Advanced Chronic Kidney Disease. Nephron 2021, 145, 692–701. [Google Scholar] [CrossRef]
- de Paula Ferreira, M.; Chowdhury, N.; Wickerson, L.; Ross, H.; Selzner, N.; Kim, S.J.; Singer, L.G.; Mathur, S. Feasibility of Virtual Assessment of Physical Frailty in Solid Organ Transplant Recipients: A Single Center, Observational Study. Int. J. Telerehabil. 2022, 14, e6447. [Google Scholar]
- DuMontier, C.; Jaung, T.; Bahl, N.E.; Manor, B.; Testa, M.; Dieli-Conwright, C.M.; Kim, D.; Hshieh, T.; Driver, J.A.; Abel, G.A. Virtual frailty assessment for older adults with hematologic malignancies. Blood Adv. 2022, 6, 5360–5363. [Google Scholar] [CrossRef]
- Kanesvaran, R.; Le Saux, O.; Motzer, R.; Choueiri, T.K.; Scotté, F.; Bellmunt, J.; Launay-Vacher, V. Elderly patients with metastatic renal cell carcinoma: Position paper from the International Society of Geriatric Oncology. Lancet Oncol. 2018, 19, e317–e326. [Google Scholar] [CrossRef]
- Hahn, A.W.; Esther, J.; Haaland, B.; Swami, U.; Dizman, N.; Rathi, N.; Maughan, B.L.; Pal, S.K.; Agarwal, N. Patterns of treatment in metastatic renal cell carcinoma for older versus younger patients. J. Geriatr. Oncol. 2020, 11, 724–726. [Google Scholar] [CrossRef]
- Rajasekaran, T.; Chowdhury, A.R.; Kanesvaran, R. Renal Cell Carcinoma in Older Adults with Frailty. In Frailty in Older Adults with Cancer; Springer: Cham, Switzerland, 2022; pp. 371–381. [Google Scholar]
- Fenton, A.; Montgomery, E.; Nightingale, P.; Peters, A.M.; Sheerin, N.; Wroe, A.C.; Lipkin, G.W. Glomerular filtration rate: New age-and gender-specific reference ranges and thresholds for living kidney donation. BMC Nephrol. 2018, 19, 336. [Google Scholar] [CrossRef] [Green Version]
- Janssen-Heijnen, M.L.; Houterman, S.; Lemmens, V.E.; Louwman, M.W.; Maas, H.A.; Coebergh, J.W. Prognostic impact of increasing age and co-morbidity in cancer patients: A population-based approach. Crit. Rev. Oncol. Hematol. 2005, 55, 231–240. [Google Scholar] [CrossRef]
- Liu, L.; Zhu, M.; Meng, Q.; Wang, Y.; Zhao, Y.; Xie, D.; Zhang, L.; Zhao, M.H. Association between kidney function and the risk of cancer: Results from the China Health and Retirement longitudinal study (CHARLS). J. Cancer 2020, 11, 6429–6436. [Google Scholar] [CrossRef]
- Wong, G.; Hayen, A.; Chapman, J.R.; Webster, A.C.; Wang, J.J.; Mitchell, P.; Craig, J.C. Association of CKD and cancer risk in older people. J. Am. Soc. Nephrol. 2009, 20, 1341–1350. [Google Scholar] [CrossRef] [Green Version]
- Maisonneuve, P.; Agodoa, L.; Gellert, R.; Stewart, J.H.; Buccianti, G.; Lowenfels, A.B.; Wolf, R.A.; Jones, E.; Dsiney, A.P.; Briggs, D.; et al. Cancer in patients on dialysis for end-stage renal disease: An international collaborative study. Lancet 1999, 354, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.H.; Lee, S.W.; Kim, S.W.; Ahn, S.Y.; Yu, M.Y.; Kim, K.I.; Chin, H.J.; Na, K.Y.; Chae, D.W.; Kim, S. Frailty as a predictor of acute kidney injury in hospitalized elderly patients: A single center, retrospective cohort study. PLoS ONE 2016, 11, e0156444. [Google Scholar] [CrossRef] [PubMed]
- Rainfray, M.; Mertens, C.; Duc, S. Renal Function in Elderly and in Relationship with Management of Genitourinary Tumors. In Management of Urological Cancers in Older People; Springer: London, UK, 2013; pp. 51–62. [Google Scholar]
- Docherty, N.G.; Delles, C.; D’Haese, P.; Layton, A.T.; Martínez-Salgado, C.; Vervaet, B.A.; López-Hernández, F.J. Haemodynamic frailty–A risk factor for acute kidney injury in the elderly. Ageing Res. Rev. 2021, 70, 101408. [Google Scholar] [CrossRef] [PubMed]
- Coll, P.P.; Korc-Grodzicki, B.; Ristau, B.T.; Shahrokni, A.; Koshy, A.; Filippova, O.T.; Ali, I. Cancer prevention and screening for older adults: Part 1. Lung, colorectal, bladder, and kidney cancer. J. Am. Geriatr. Soc. 2020, 68, 2399–2406. [Google Scholar] [CrossRef]
- Launay-Vacher, V.; Chatelut, E.; Lichtman, S.M.; Wildiers, H.; Steer, C.; Aapro, M. Renal insufficiency in elderly cancer patients: International Society of Geriatric Oncology clinical practice recommendations. Ann. Oncol. 2007, 18, 1314–1321. [Google Scholar] [CrossRef]
- Pal, S.K.; Vanderwalde, A.; Hurria, A.; Figlin, R.A. Systemic therapies for metastatic renal cell carcinoma in older adults. Drugs Aging 2011, 28, 635–649. [Google Scholar] [CrossRef] [Green Version]
- Pierantoni, F.; Basso, U.; Maruzzo, M.; Lamberti, E.; Bimbatti, D.; Tierno, G.; Bergo, E.; Brunello, A.; Zagonel, V. Comprehensive geriatric assessment is an independent prognostic factor in older patients with metastatic renal cell cancer treated with first-line Sunitinib or Pazopanib: A single center experience. J. Geriatr. Oncol. 2021, 12, 290–297. [Google Scholar] [CrossRef]
- Ommundsen, N.; Wyller, T.B.; Nesbakken, A.; Bakka, A.O.; Jordhøy, M.S.; Skovlund, E.; Rostoft, S. Preoperative geriatric assessment and tailored interventions in frail older patients with colorectal cancer: A randomized controlled trial. Colorectal. Dis. 2018, 20, 16–25. [Google Scholar] [CrossRef]
- Hatakeyama, S.; Narita, S.; Okita, K.; Narita, T.; Iwamura, H.; Fujita, N.; Inokuchi, J.; Matsui, Y.; Kitamura, H.; Ohyama, C. Management of bladder cancer in older patients. Jpn. J. Clin. Oncol. 2022, 52, 203–213. [Google Scholar] [CrossRef]
- Iannuzzella, D.F.; Maiorana, M. Challenges of Chronic Kidney Disease on Frail Patients: Two Projects Addressing the Impact of Aging and Cancer. Ph.D. Thesis, University of Modena and Reggio Emilia, Modena, Italy, 2022; pp. 1–82. [Google Scholar]
- Gontero, P.; Mari, A.; Marra, G.; Nazzani, S.; Allasia, M.; Antonelli, A.; Barale, M.; Brunocilla, E.; Capitanio, U.; Di Maida, F.; et al. Is partial nephrectomy safe and effective in the setting of frail comorbid patients affected by renal cell carcinoma? Insights from the RECORD 2 multicentre prospective study. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 78.e17–78.e26. [Google Scholar] [CrossRef]
- Miller, C.; Raza, S.J.; Davaro, F.; May, A.; Siddiqui, S.; Hamilton, Z.A. Trends in the treatment of clinical T1 renal cell carcinoma for octogenarians: Analysis of the National Cancer Database. J. Geriatr. Oncol. 2019, 10, 285–291. [Google Scholar] [CrossRef]
- Walach, M.T.; Wunderle, M.F.; Haertel, N.; Mühlbauer, J.K.; Kowalewski, K.F.; Wagener, N.; Rathmann, N.; Kriegmair, M.C. Frailty predicts outcome of partial nephrectomy and guides treatment decision towards active surveillance and tumor ablation. World J. Urol. 2021, 39, 2843–2851. [Google Scholar] [CrossRef]
- Chow, W.B.; Rosenthal, R.A.; Merkow, R.P.; Ko, C.Y.; Esnaola, N.F. Optimal preoperative assessment of the geriatric surgical patient: A best practices guideline from the American College of Surgeons National Surgical Quality Improvement Program and the American Geriatrics Society. J. Am. Coll. Surg. 2012, 215, 453–466. [Google Scholar] [CrossRef]
- Klatte, T.; Grubmüller, B.; Waldert, M.; Weibl, P.; Remzi, M. Laparoscopic cryoablation versus partial nephrectomy for the treatment of small renal masses: Systematic review and cumulative analysis of observational studies. Eur. Urol. 2011, 60, 435–443. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Frontera, O.A.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef]
- Araujo, D.V.; Wells, J.C.; Hansen, A.R.; Dizman, N.; Pal, S.K.; Beuselinck, B.; Donskov, F.; Gan, C.L.; Yan, F.; Tran, B.; et al. Efficacy of immune-checkpoint inhibitors (ICI) in the treatment of older adults with metastatic renal cell carcinoma (mRCC)–an International mRCC Database Consortium (IMDC) analysis. J. Geriatr. Oncol. 2021, 12, 820–826. [Google Scholar] [CrossRef]
- Hale, P.; Hahn, A.W.; Rathi, N.; Pal, S.K.; Haaland, B.; Agarwal, N. Treatment of metastatic renal cell carcinoma in older patients: A network meta-analysis. J. Geriatr. Oncol. 2019, 10, 149–154. [Google Scholar] [CrossRef]
- Lee, J.L.; Ziobro, M.; Gafanov, R.; Matveev, V.B.; Suarez, C.; Donskov, F.; Pouliot, F.; Alekseev, B.Y.; Wiechno, P.J.; Tomczak, P.; et al. KEYNOTE-427 cohort B: First-line pembrolizumab (pembro) monotherapy for advanced non‒clear cell renal cell carcinoma (NCC-RCC). J. Clin. Oncol. 2019, 37, 4569. [Google Scholar] [CrossRef]
- Schmidinger, M.; Porta, C.; Oudard, S.; Dénéchère, G.; Brault, Y.; Serfass, L.; Costa, N.M.; Larkin, J.M. Real-world experience with sunitinib treatment in patients with metastatic renal cell carcinoma: Clinical outcome according to risk score. Clin. Genitourin. Cancer 2020, 18, e588–e597. [Google Scholar] [CrossRef] [Green Version]
- Kader, A.K.; Tamboli, P.; Luongo, T.; Matin, S.F.; Bell, K.; Jonasch, E.; Swanson, D.A.; Wood, C.G. Cytoreductive nephrectomy in the elderly patient: The MD Anderson Cancer Center experience. J. Urol. 2007, 177, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Kirkhus, L.; Šaltytė Benth, J.; Grønberg, B.H.; Hjermstad, M.J.; Rostoft, S.; Harneshaug, M.; Selbæk, G.; Wyller, T.B.; Jordhøy, M.S. Frailty identified by geriatric assessment is associated with poor functioning, high symptom burden and increased risk of physical decline in older cancer patients: Prospective observational study. Palliat. Med. 2019, 33, 312–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farcet, A.; De Decker, L.; Pauly, V.; Rousseau, F.; Bergman, H.; Molines, C.; Retornaz, F. Frailty markers and treatment decisions in patients seen in oncogeriatric clinics: Results from the ASRO pilot study. PLoS ONE 2016, 11, e0149732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, N.; Momota, M.; Hatakeyama, S.; Ito, H.; Yoneyama, T.; Hashimoto, Y.; Yoshikawa, K.; Ohyama, C. Impact of neoadjuvant chemotherapy–induced acute kidney injury on oncological outcomes in patients who underwent radical cystectomy: A multicenter retrospective study. J. Clin. Oncol. 2023, 41, 573. [Google Scholar]
- Courcier, J.; De La Taille, A.; Lassau, N.; Ingels, A. Comorbidity and frailty assessment in renal cell carcinoma patients. World J. Urol. 2021, 39, 2831–2841. [Google Scholar] [CrossRef]
- ASA Physical Status Classification System. 2020. Available online: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (accessed on 3 November 2022).
- Lakomkin, N.; Zuckerman, S.L.; Stannard, B.; Montejo, J.; Sussman, E.S.; Virojanapa, J.; Kuzmik, G.; Goz, V.; Hadjipanayis, C.G.; Cheng, J.S. Preoperative risk stratification in spine tumor surgery: A comparison of the modified charlson index, frailty index, and ASA score. Spine 2019, 44, E782–E787. [Google Scholar] [CrossRef]
- Pitts, K.D.; Arteaga, A.A.; Stevens, B.P.; White, W.C.; Su, D.; Spankovich, C.; Jefferson, G.D.; Jackson, L.L. Frailty as a predictor of postoperative outcomes among patients with head and neck cancer. Otolaryngol. Head Neck Surg. 2019, 160, 664–671. [Google Scholar] [CrossRef]
- Bellera, C.A.; Rainfray, M.; Mathoulin-Pélissier, S.; Mertens, C.; Delva, F.; Fonck, M.; Soubeyran, P.L. Screening older cancer patients: First evaluation of the G-8 geriatric screening tool. Ann. Oncol. 2012, 23, 2166–2172. [Google Scholar] [CrossRef]
- Kenis, C.; Decoster, L.; Van Puyvelde, K.; De Greve, J.; Conings, G.; Milisen, K.; Flamaing, J.; Lobelle, J.P.; Wildiers, H. Performance of two geriatric screening tools in older patients with cancer. J. Clin. Oncol. 2014, 32, 19–26. [Google Scholar] [CrossRef]
- Soubeyran, P.; Bellera, C.; Goyard, J.; Heitz, D.; Curé, H.; Rousselot, H.; Albrand, G.; Servent, V.; Jean, O.S.; van Praagh, I.; et al. Screening for vulnerability in older cancer patients: The ONCODAGE Prospective Multicenter Cohort Study. PLoS ONE 2014, 9, e115060. [Google Scholar] [CrossRef]
- Pamoukdjian, F.; Laurent, M.; Martinez-Tapia, C.; Rolland, Y.; Paillaud, E.; Canoui-Poitrine, F. Frailty parameters, morbidity and mortality in older adults with cancer: A structural equation modelling approach based on the fried phenotype. J. Clin. Med. 2020, 9, 1826. [Google Scholar] [CrossRef]
- Dos Reis, P.F.; de França, P.S.; Dos Santos, M.P.; Martucci, R.B. Influence of nutritional status and frailty phenotype on health-related quality of life of patients with bladder or kidney cancer. Support. Care Cancer 2021, 29, 5139–5150. [Google Scholar] [CrossRef]
- Escudier, B.; Porta, C.; Schmidinger, M.; Rioux-Leclercq, N.; Bex, A.; Khoo, V.; Grünwald, V.; Gillessen, S.; Horwich, A. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 706–720. [Google Scholar] [CrossRef] [Green Version]
- Motzer, R.J.; Bacik, J.; Murphy, B.A.; Russo, P.; Mazumdar, M. Interferon-alfa as a comparative treatment for clinical trials of new therapies against advanced renal cell carcinoma. J. Clin. Oncol. 2002, 20, 289–296. [Google Scholar] [CrossRef]
- Motzer, R.J.; Mazumdar, M.; Bacik, J.; Berg, W.; Amsterdam, A.; Ferrara, J. Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. J. Clin. Oncol. 1999, 17, 2530–2540. [Google Scholar] [CrossRef] [Green Version]
- Heng, D.Y.; Xie, W.; Regan, M.M.; Warren, M.A.; Golshayan, A.R.; Sahi, C.; Eigl, B.J.; Ruether, J.D.; Cheng, T.; North, S.; et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor–targeted agents: Results from a large, multicenter study. J. Clin. Oncol. 2009, 27, 5794–5799. [Google Scholar] [CrossRef]
- Heng, D.Y.; Xie, W.; Regan, M.M.; Harshman, L.C.; Bjarnason, G.A.; Vaishampayan, U.N.; Mackenzie, M.; Wood, L.; Donskov, F.; Tan, M.H.; et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: A population-based study. Lancet Oncol. 2013, 14, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Kwon, W.A.; Cho, I.C.; Yu, A.; Nam, B.H.; Joung, J.Y.; Seo, H.K.; Lee, K.H.; Chung, J. Validation of the MSKCC and Heng risk criteria models for predicting survival in patients with metastatic renal cell carcinoma treated with sunitinib. Ann. Surg. Oncol. 2013, 20, 4397–4404. [Google Scholar] [CrossRef]
- Fiala, O.; Finek, J.; Poprach, A.; Melichar, B.; Kopecký, J.; Zemanova, M.; Kopeckova, K.; Mlcoch, T.; Dolezal, T.; Capkova, L.; et al. Outcomes according to MSKCC risk score with focus on the intermediate-risk group in metastatic renal cell carcinoma patients treated with first-line sunitinib: A retrospective analysis of 2390 patients. Cancers 2020, 12, 808. [Google Scholar] [CrossRef] [Green Version]
- Yip, S.; Wells, C.; Moreira, R.B.; Wong, A.; Srinivas, S.; Beuselinck, B.; Porta, C.; Sim, H.W.; Ernst, D.S.; Rini, B.I.; et al. Real world experience of immuno-oncology agents in metastatic renal cell carcinoma: Results from the IMDC. J. Clin. Oncol. 2017, 35, 492. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European association of urology guidelines on renal cell carcinoma: The 2019 update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.W.; Kim, S.M.; Kim, W.T.; Yun, S.J.; Lee, S.C.; Kim, W.J.; Hwang, E.C.; Kang, S.H.; Hong, S.H.; Chung, J.; et al. The age-adjusted Charlson comorbidity index as a predictor of overall survival of surgically treated non-metastatic clear cell renal cell carcinoma. J. Cancer Res. Clin. Oncol. 2020, 146, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Hamaker, M.E.; Jonker, J.M.; de Rooij, S.E.; Vos, A.G.; Smorenburg, C.H.; van Munster, B.C. Frailty screening methods for predicting outcome of a comprehensive geriatric assessment in elderly patients with cancer: A systematic review. Lancet Oncol. 2012, 13, e437–e444. [Google Scholar] [CrossRef] [PubMed]
- Togashi, K.; Hatakeyama, S.; Soma, O.; Okita, K.; Fujita, N.; Tanaka, T.; Noro, D.; Horiguchi, H.; Uemura, N.; Iwane, T.; et al. Utility of the Age Discrepancy between Frailty-Based Biological Age and Expected Life Age in Patients with Urological Cancers. Cancers 2022, 14, 6229. [Google Scholar] [CrossRef]
- Soma, O.; Hatakeyama, S.; Okamoto, T.; Fujita, N.; Matsumoto, T.; Tobisawa, Y.; Yoneyama, T.; Yamamoto, H.; Yoneyama, T.; Hashimoto, Y.; et al. Clinical implication of a quantitative frailty assessment tool for prognosis in patients with urological cancers. Oncotarget 2018, 9, 17396–17405. [Google Scholar] [CrossRef] [Green Version]
- Hwang, A.C.; Lee, W.J.; Huang, N.; Chen, L.Y.; Peng, L.N.; Lin, M.H.; Chou, Y.J.; Chen, L.K. Longitudinal changes of frailty in 8 years: Comparisons between physical frailty and frailty index. BMC Geriatr. 2021, 21, 726. [Google Scholar] [CrossRef]


{kind=link}
| Factor | Fried Frailty Phenotype | Frailty Index | Tool Based on Clinical Impression (i.e., Karnofsky Performance Index, Eastern Cooperative Oncology Group Performance Status, and Clinical Frailty Scale Score | Objective Measurement Tool (i.e., Short Physical Performance Battery) |
|---|---|---|---|---|
| Type of Measure | Binary (frail or not) | Continuous | Ordinal | Binary or Ordinal |
| Data Source | Physical exam/questionnaire | Multiple including administrative data | Clinical judgment (provider or patient) | Physical examination |
| Ease of Capture | Mixed, depending on the traditional or modified version | Mixed, depending on the availability of information sources or the need for primary capture | Very easy/point of care | Mixed (may require face-to-face assessment and equipment) |
| Ease of Understanding (Patients and Providers) | Very easy | Potentially difficult | Very easy | Very easy |
| Construct Validity | Low | High | Moderate | Mixed (depending on how used) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, H.H.L.; Chinnadurai, R.; Walker, R.J.; Tennankore, K.K. Is It Time to Integrate Frailty Assessment in Onconephrology? Cancers 2023, 15, 1674. https://doi.org/10.3390/cancers15061674
Wu HHL, Chinnadurai R, Walker RJ, Tennankore KK. Is It Time to Integrate Frailty Assessment in Onconephrology? Cancers. 2023; 15(6):1674. https://doi.org/10.3390/cancers15061674
Chicago/Turabian StyleWu, Henry H. L., Rajkumar Chinnadurai, Robert J. Walker, and Karthik K. Tennankore. 2023. "Is It Time to Integrate Frailty Assessment in Onconephrology?" Cancers 15, no. 6: 1674. https://doi.org/10.3390/cancers15061674