
Translational Potential of Fluorescence Polarization for Breast Cancer Cytopathology
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Acquisition and Handling
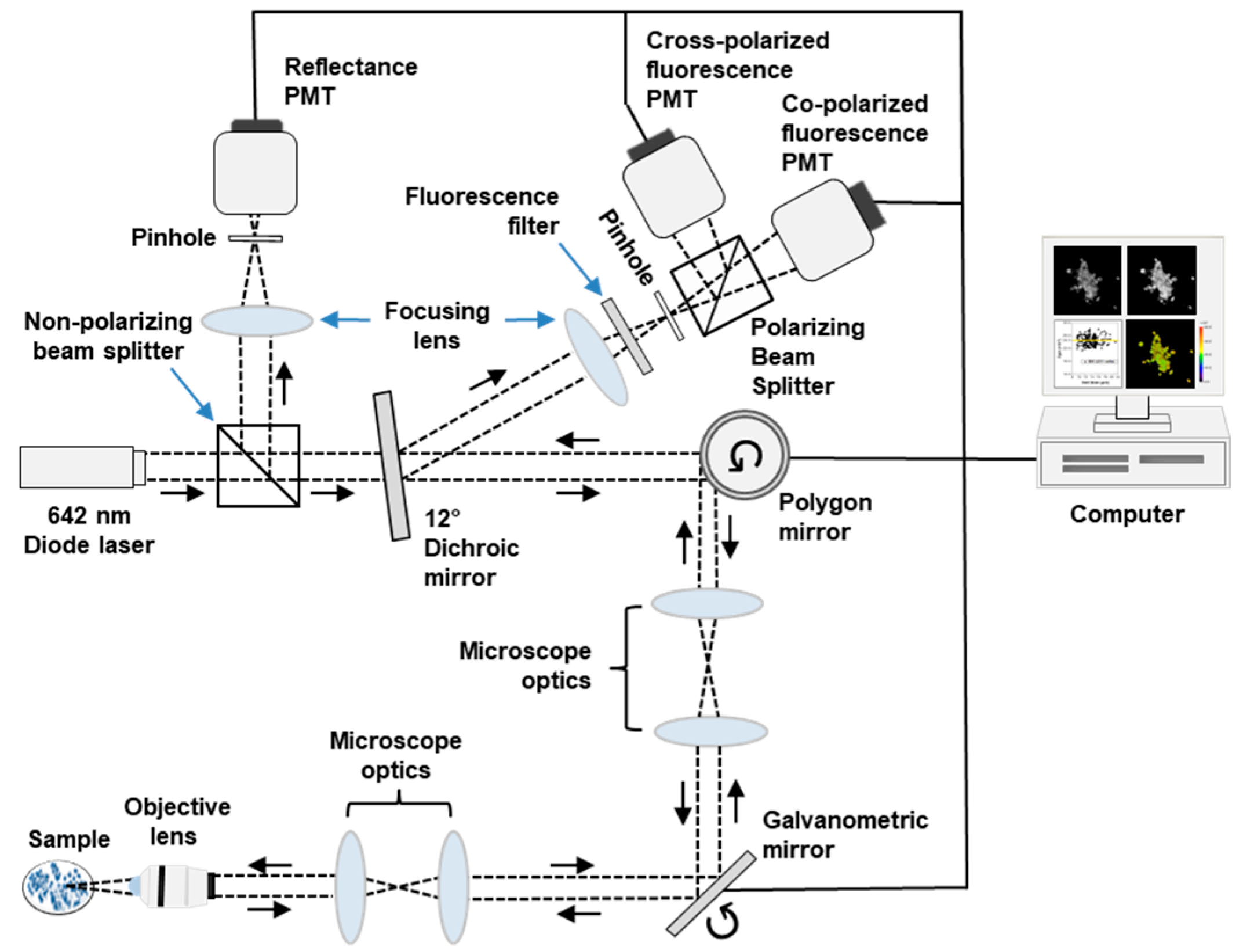
2.3. Confocal Imaging
2.4. System Calibration
2.5. Image Processing
2.6. Statistical Analysis
2.7. Cytopathology and Histopathology
3. Results
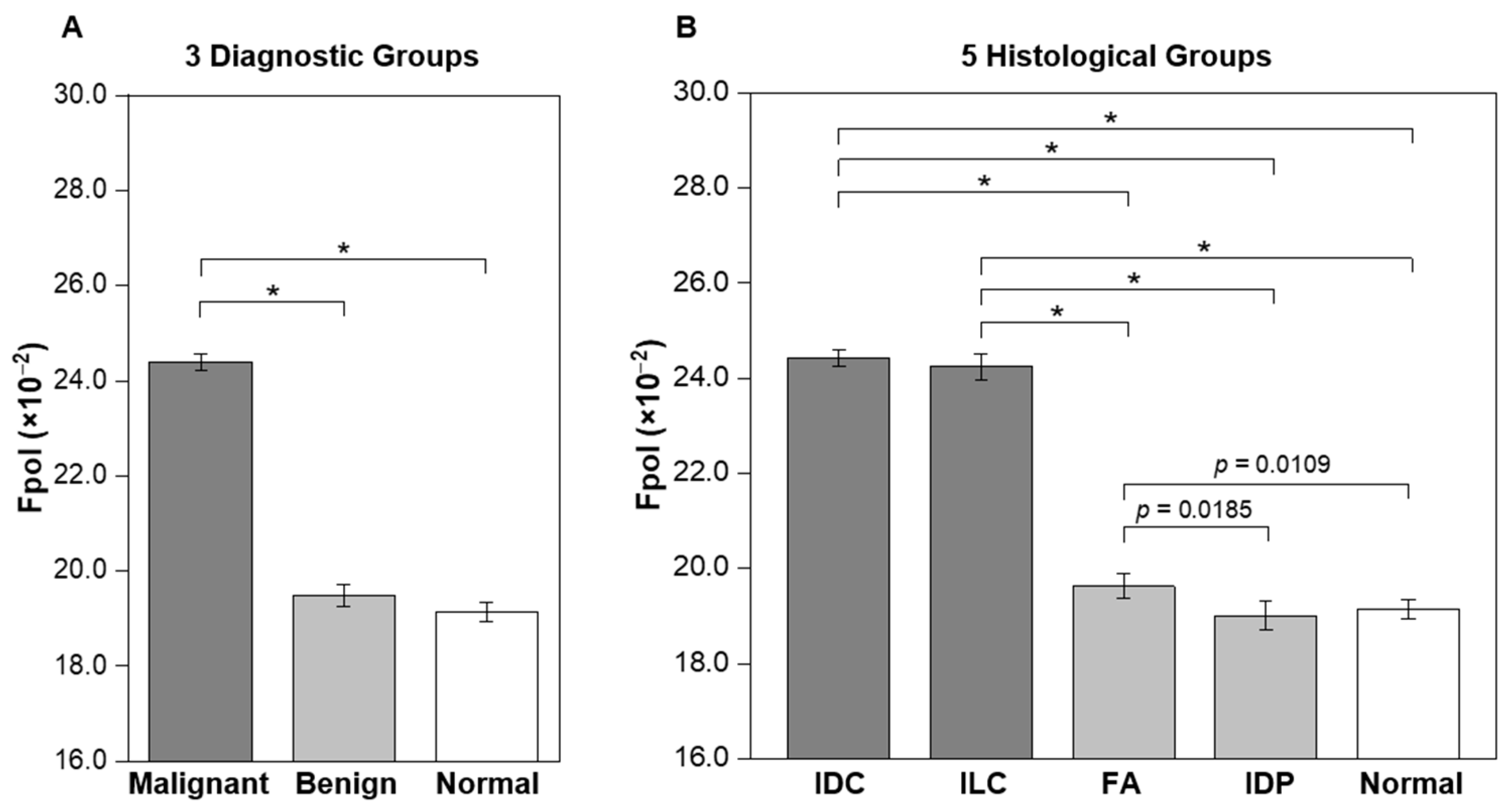
3.1. Increased MB Fpol in Cancerous Breast FNAs
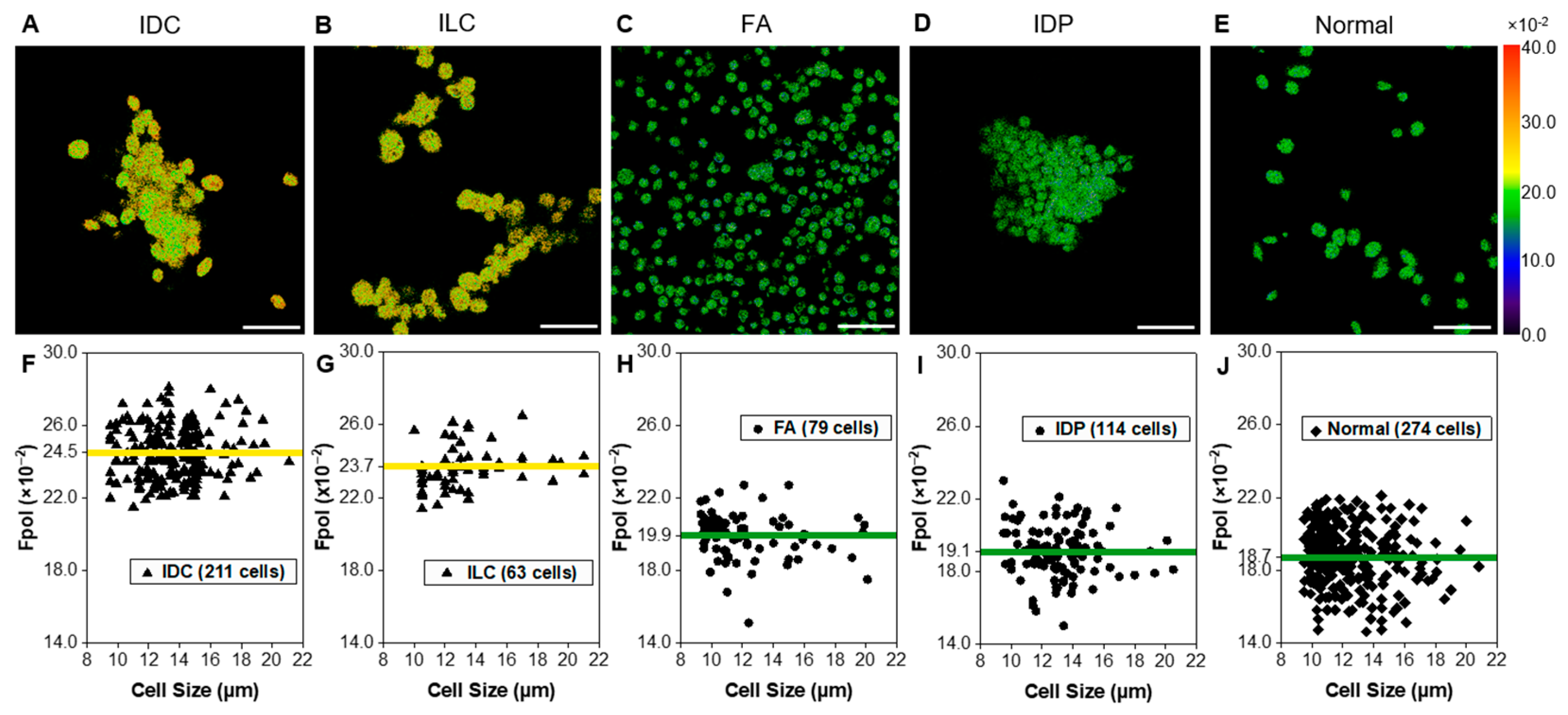
3.2. Quantitative Fpol Imaging of Breast FNA Specimens
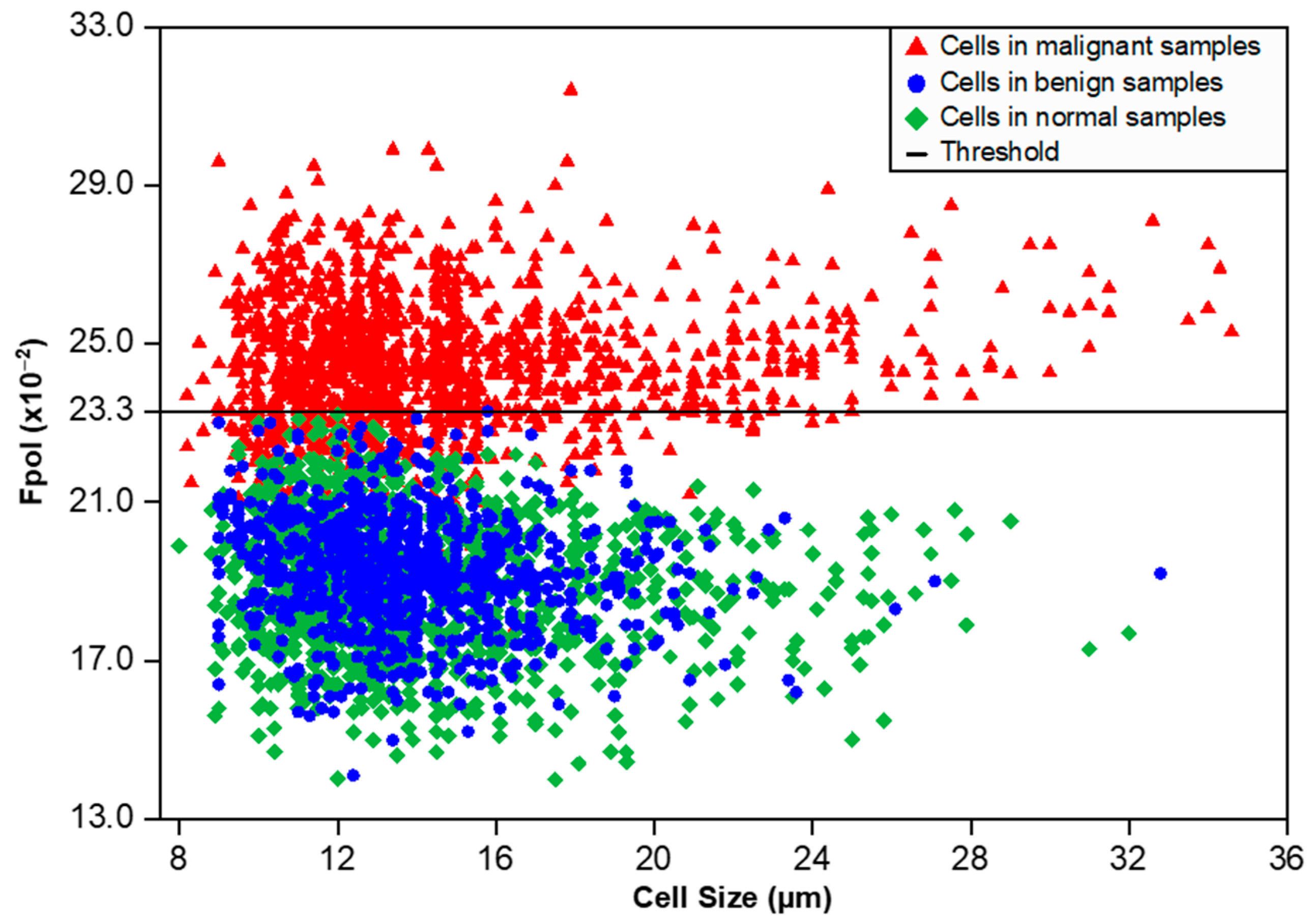
3.3. MB Fpol Scatter Plot of All Imaged Cells
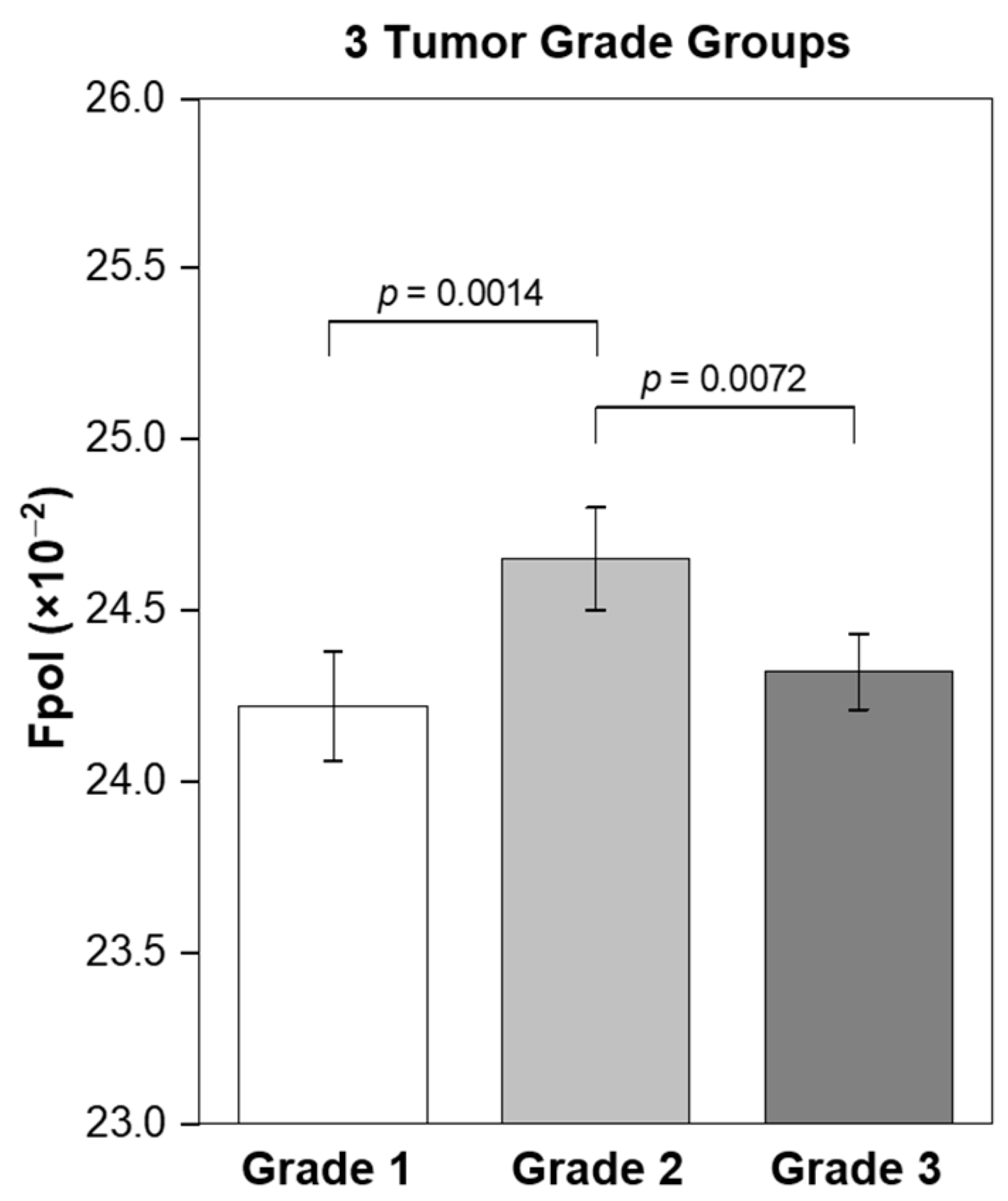
3.4. MB Fpol Correlation with the Tumor Grade
3.5. MB Fluorescence Emission Images Display Cytomorphology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Breast Cancer Facts & Figures 2022–2024. American Cancer Society, Atlanta. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/2022-2024-breast-cancer-fact-figures-acs.pdf (accessed on 14 January 2023).
- Harding, C.; Pompei, F.; Burmistrov, D.; Welch, H.G.; Abebe, R.; Wilson, R. Breast cancer screening, incidence, and mortality across US counties. JAMA Intern Med. 2015, 175, 1483–1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elmore, J.G.; Longton, G.M.; Carney, P.A.; Geller, B.M.; Onega, T.; Tosteson, A.N.; Nelson, H.D.; Pepe, M.S.; Allison, K.H.; Schnitt, S.J.; et al. Diagnostic concordance among pathologists interpreting breast biopsy specimens. JAMA 2015, 313, 1122–1132. [Google Scholar] [CrossRef] [Green Version]
- Schnitt, S.J. Problematic issues in breast core needle biopsies. Mod. Pathol. 2019, 32 (Suppl. S1), 71–76. [Google Scholar] [CrossRef] [PubMed]
- Sidransky, D. Emerging molecular markers of cancer. Nat. Rev. Cancer 2002, 2, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Li, A.; Abreo, F.; Turbat-Herrera, E.; Grafton, W.D. Comparison of fine-needle aspiration cytology and core biopsy for diagnosis of breast cancer. Diagn. Cytopathol. 2001, 24, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Goossens, N.; Nakagawa, S.; Sun, X.; Hoshida, Y. Cancer biomarker discovery and validation. Transl. Cancer Res. 2015, 4, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Guan, X.; Fan, Z.; Ching, L.M.; Li, Y.; Wang, X.; Cao, W.M.; Liu, D.X. Non-invasive biomarkers for early detection of breast cancer. Cancers 2020, 12, 2767. [Google Scholar] [CrossRef]
- Carver, G.E.; Locknar, S.A.; Weaver, D.L.; Stein, J.L.; Stein, G.S. Real-time detection of breast cancer at the cellular level. J. Cell Physiol. 2019, 234, 5413–5419. [Google Scholar] [CrossRef]
- Weber, J.; Bollepalli, L.; Belenguer, A.M.; Antonio, M.D.; De Mitri, N.; Joseph, J.; Balasubramanian, S.; Hunter, C.A.; Bohndiek, S.E. An activatable cancer-targeted hydrogen peroxide probe for photoacoustic and fluorescence imaging. Cancer Res. 2019, 79, 5407–5417. [Google Scholar] [CrossRef] [Green Version]
- Phipps, J.E.; Gorpas, D.; Unger, J.; Darrow, M.; Bold, R.J.; Marcu, L. Automated detection of breast cancer in resected specimens with fluorescence lifetime imaging. Phys. Med. Biol. 2017, 63, 015003. [Google Scholar] [CrossRef] [Green Version]
- Streeter, S.S.; Hunt, B.; Zuurbier, R.A.; Wells, W.A.; Paulsen, K.D.; Pogue, B.W. Developing diagnostic assessment of breast lumpectomy tissues using radiomic and optical signatures. Sci. Rep. 2021, 11, 21832. [Google Scholar] [CrossRef]
- Streeter, S.S.; Maloney, B.W.; Zuurbier, R.A.; Wells, W.A.; Barth, R.J.; Paulsen, K.D.; Pogue, B.W. Optical scatter imaging of resected breast tumor structures matches the patterns of micro-computed tomography. Phys. Med. Biol. 2021, 66, 115021. [Google Scholar] [CrossRef]
- Vanna, R.; Morasso, C.; Marcinnò, B.; Piccotti, F.; Torti, E.; Altamura, D.; Albasini, S.; Agozzino, M.; Villani, L.; Sorrentino, L.; et al. Raman spectroscopy reveals that biochemical composition of breast microcalcifications correlates with histopathologic features. Cancer Res. 2020, 80, 1762–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, G.; Nguyen, T.Q.; Pence, I.J.; Caldwell, B.; O’Connor, M.E.; Giltnane, J.; Sanders, M.E.; Grau, A.; Meszoely, I.; Hooks, M.; et al. Evaluating feasibility of an automated 3-dimensional scanner using Raman spectroscopy for intraoperative breast margin assessment. Sci. Rep. 2017, 7, 13548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, B.F.; McLaughlin, R.A.; Kennedy, K.M.; Chin, L.; Wijesinghe, P.; Curatolo, A.; Tien, A.; Ronald, M.; Latham, B.; Saunders, C.M.; et al. Investigation of optical coherence microelastography as a method to visualize cancers in human breast tissue. Cancer Res. 2015, 75, 3236–3245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, X.; Gan, Y.; Chang, E.; Hibshoosh, H.; Feldman, S.; Hendon, C. Visualization and tissue classification of human breast cancer images using ultrahigh-resolution, O.C.T. Lasers Surg. Med. 2017, 49, 258–269. [Google Scholar] [CrossRef] [Green Version]
- Yaroslavsky, A.N.; Feng, X.; Muzikansky, A.; Hamblin, M.R. Fluorescence polarization of methylene blue as a quantitative marker of breast cancer at the cellular level. Sci. Rep. 2019, 9, 940. [Google Scholar] [CrossRef] [Green Version]
- Feng, X.; Muzikansky, A.; Ross, A.H.; Hamblin, M.R.; Jermain, P.R.; Yaroslavsky, A.N. Multimodal quantitative imaging of brain cancer in cultured cells. Biomed. Opt. Express 2019, 10, 4237–4248. [Google Scholar] [CrossRef] [Green Version]
- Malik, S.; Jermain, P.R.; Feng, X.; Yaroslavsky, A.N. Multimodal optical imaging of renal cells. Opt. Eng. 2019, 58, 082415. [Google Scholar] [CrossRef]
- Jermain, P.R.; Fischer, A.H.; Joseph, L.; Muzikansky, A.; Yaroslavsky, A.N. Fluorescence polarization imaging of methylene blue facilitates quantitative detection of thyroid cancer in single cells. Cancers 2022, 14, 1339. [Google Scholar] [CrossRef]
- Simmons, R.; Thevarajah, S.; Brennan, M.B.; Christos, P.; Osborne, M. Methylene blue dye as an alternative to isosulfan blue dye for sentinel lymph node localization. Ann. Surg. Oncol. 2003, 10, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Nour, A. Efficacy of methylene blue dye in localization of sentinel lymph node in breast cancer patients. Breast J. 2004, 10, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Varghese, P.; Abdel-Rahman, A.T.; Akberali, S.; Mostafa, A.; Gattuso, J.M.; Carpenter, R. Methylene blue dye--a safe and effective alternative for sentinel lymph node localization. Breast J. 2008, 14, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Blessing, W.D.; Stolier, A.J.; Teng, S.C.; Bolton, J.S.; Fuhrman, G.M. A comparison of methylene blue and lymphazurin in breast cancer sentinel node mapping. Am. J. Surg. 2002, 184, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Yaroslavsky, A.N.; Feng, X.; Neel, V.A. Optical mapping of nonmelanoma skin cancers-A pilot clinical study. Lasers Surg. Med. 2017, 49, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Lakowicz, J.R. Principles of Fluorescence Spectroscopy, 3rd ed.; Springer: New York, NY, USA, 2006; pp. 353–382. [Google Scholar]
- Jameson, D.M.; Ross, J.A. Fluorescence polarization/anisotropy in diagnostics and imaging. Chem. Rev. 2010, 110, 2685–2708. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Wu, Q.; Berezin, M.Y. Fluorescence anisotropy (polarization): From drug screening to precision medicine. Expert. Opin. Drug. Discov. 2015, 10, 1145–1161. [Google Scholar] [CrossRef] [Green Version]
- Patel, R.; Khan, A.; Quinlan, R.; Yaroslavsky, A.N. Polarization-sensitive multimodal imaging for detecting breast cancer. Cancer Res. 2014, 74, 4685–4693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, J.; Suhling, K.; Lévêque-Fort, S.; Webb, S.E.D.; Davis, D.M.; Phillips, D.; Sabharwal, Y.; French, P.M.W. Wide-field time-resolved fluorescence anisotropy imaging (TR-FAIM): Imaging the rotational mobility of a fluorophore. Rev. Sci. Instrum. 2003, 74, 182–192. [Google Scholar] [CrossRef] [Green Version]
- Demidenko, E. Mixed Models: Theory and Applications with R, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2013; pp. 1–713. [Google Scholar]
- Vajpeyi, R. WHO classification of tumours: Pathology and genetics of tumours of the breast and female genital organs. J. Clin. Pathol. 2005, 58, 671–672. [Google Scholar]
- Summerhayes, I.C.; Lampidis, T.J.; Bernal, S.D.; Nadakavukaren, J.J.; Nadakavukaren, K.K.; Shepherd, E.L.; Chen, L.B. Unusual retention of rhodamine 123 by mitochondria in muscle and carcinoma cells. Proc. Natl. Acad. Sci. USA 1982, 79, 5292–5296. [Google Scholar] [CrossRef] [Green Version]
- Lampidis, T.J.; Bernal, S.D.; Summerhayes, I.C.; Chen, L.B. Selective toxicity of rhodamine 123 in carcinoma cells in vitro. Cancer Res. 1983, 43, 716–720. [Google Scholar] [PubMed]
- Chen, L.B. Mitochondrial membrane potential in living cells. Annu. Rev. Cell Biol. 1988, 4, 155–181. [Google Scholar] [CrossRef] [PubMed]
- Avagliano, A.; Ruocco, M.R.; Aliotta, F.; Belviso, I.; Accurso, A.; Masone, S.; Montagnani, S.; Arcucci, A. Mitochondrial Flexibility of Breast Cancers: A Growth Advantage and a Therapeutic Opportunity. Cells 2019, 8, 401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Liu, H.; Liu, Z.; Ding, Y.; Ledoux, S.P.; Wilson, G.L.; Voellmy, R.; Lin, Y.; Lin, W.; Nahta, R.; et al. Overcoming trastuzumab resistance in breast cancer by targeting dysregulated glucose metabolism. Cancer Res. 2011, 71, 4585–4597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magometschnigg, H.; Pinker, K.; Helbich, T.; Brandstetter, A.; Rudas, M.; Nakuz, T.; Baltzer, P.; Wadsak, W.; Hacker, M.; Weber, M.; et al. PIK3CA Mutational Status Is Associated with High Glycolytic Activity in ER+/HER2- Early Invasive Breast Cancer: A Molecular Imaging Study Using [18F]FDG PET/CT. Mol. Imaging Biol. 2019, 21, 991–1002. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histological Classification | No. of Samples (%) | No. of Cells (%) | Mean Fpol, No. ± SE (×10−2) |
|---|---|---|---|
| Malignant | 19 (43) | 1577 (41) | 24.40 ± 0.17 |
| IDC | 15 (34) | 1335 (35) | 24.42 ± 0.17 |
| ILC | 4 (9) | 242 (6) | 24.24 ± 0.27 |
| Benign | 10 (23) | 910 (24) | 19.49 ± 0.23 |
| FA | 6 (14) | 632 (17) | 19.63 ± 0.25 |
| IDP | 4 (9) | 278 (7) | 19.00 ± 0.30 |
| Normal | 15 (34) | 1321 (35) | 19.14 ± 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jermain, P.R.; Kandil, D.H.; Muzikansky, A.; Khan, A.; Yaroslavsky, A.N. Translational Potential of Fluorescence Polarization for Breast Cancer Cytopathology. Cancers 2023, 15, 1501. https://doi.org/10.3390/cancers15051501
Jermain PR, Kandil DH, Muzikansky A, Khan A, Yaroslavsky AN. Translational Potential of Fluorescence Polarization for Breast Cancer Cytopathology. Cancers. 2023; 15(5):1501. https://doi.org/10.3390/cancers15051501
Chicago/Turabian StyleJermain, Peter R., Dina H. Kandil, Alona Muzikansky, Ashraf Khan, and Anna N. Yaroslavsky. 2023. "Translational Potential of Fluorescence Polarization for Breast Cancer Cytopathology" Cancers 15, no. 5: 1501. https://doi.org/10.3390/cancers15051501