

Thyroid Profile in the First Three Months after Starting Treatment in Children with Newly Diagnosed Cancer
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods and Patients
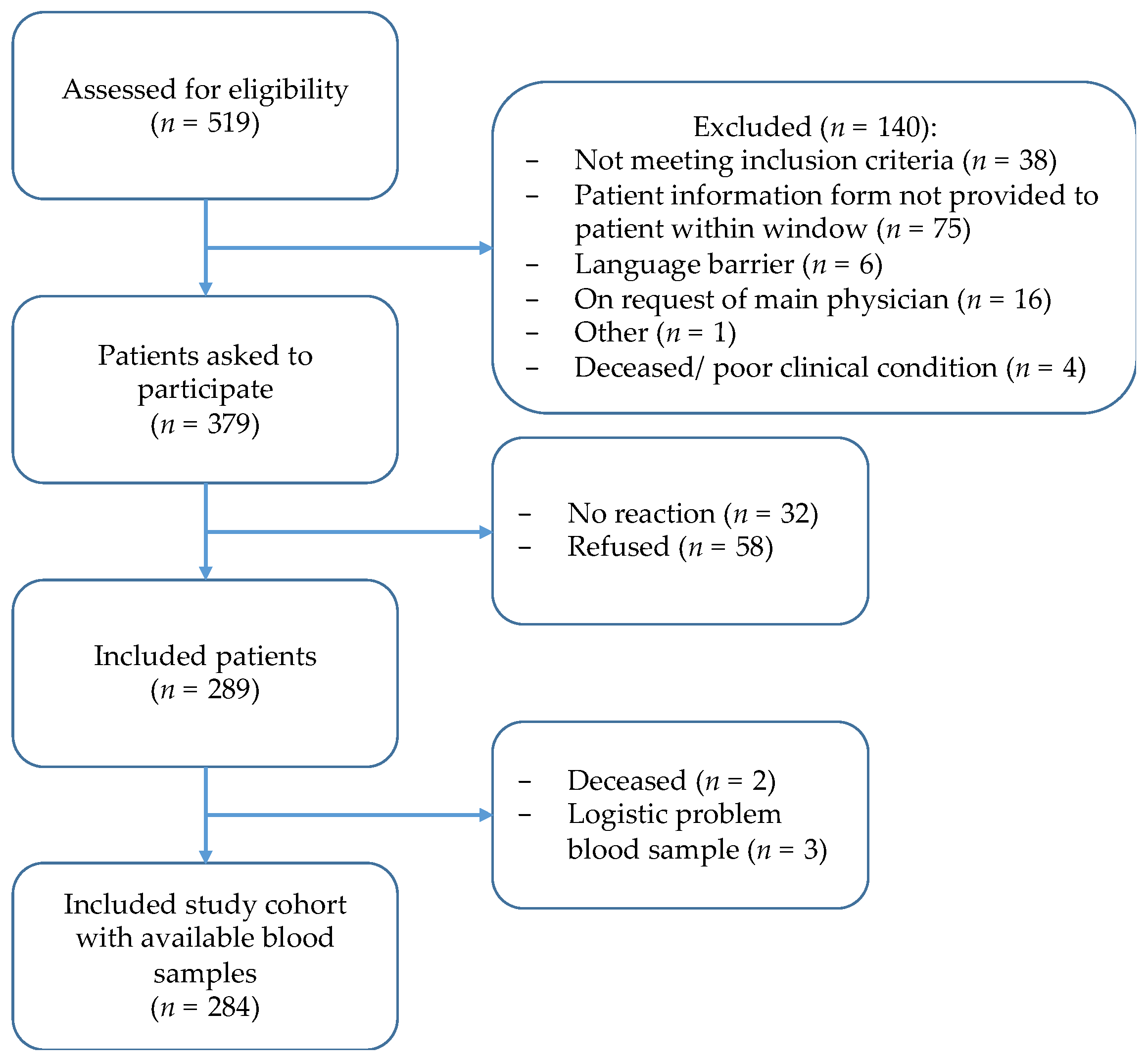
2.1. Patients
2.2. Data Collection
2.3. Laboratory Assays
2.4. Definitions
2.5. Statistics
2.6. Ethics
3. Results
3.1. General Patient Characteristics
3.2. Thyroid Profile
3.2.1. (Subclinical) Hypo- and Hyperthyroidism
3.2.2. ESS
3.2.3. Central Hypothyroidism
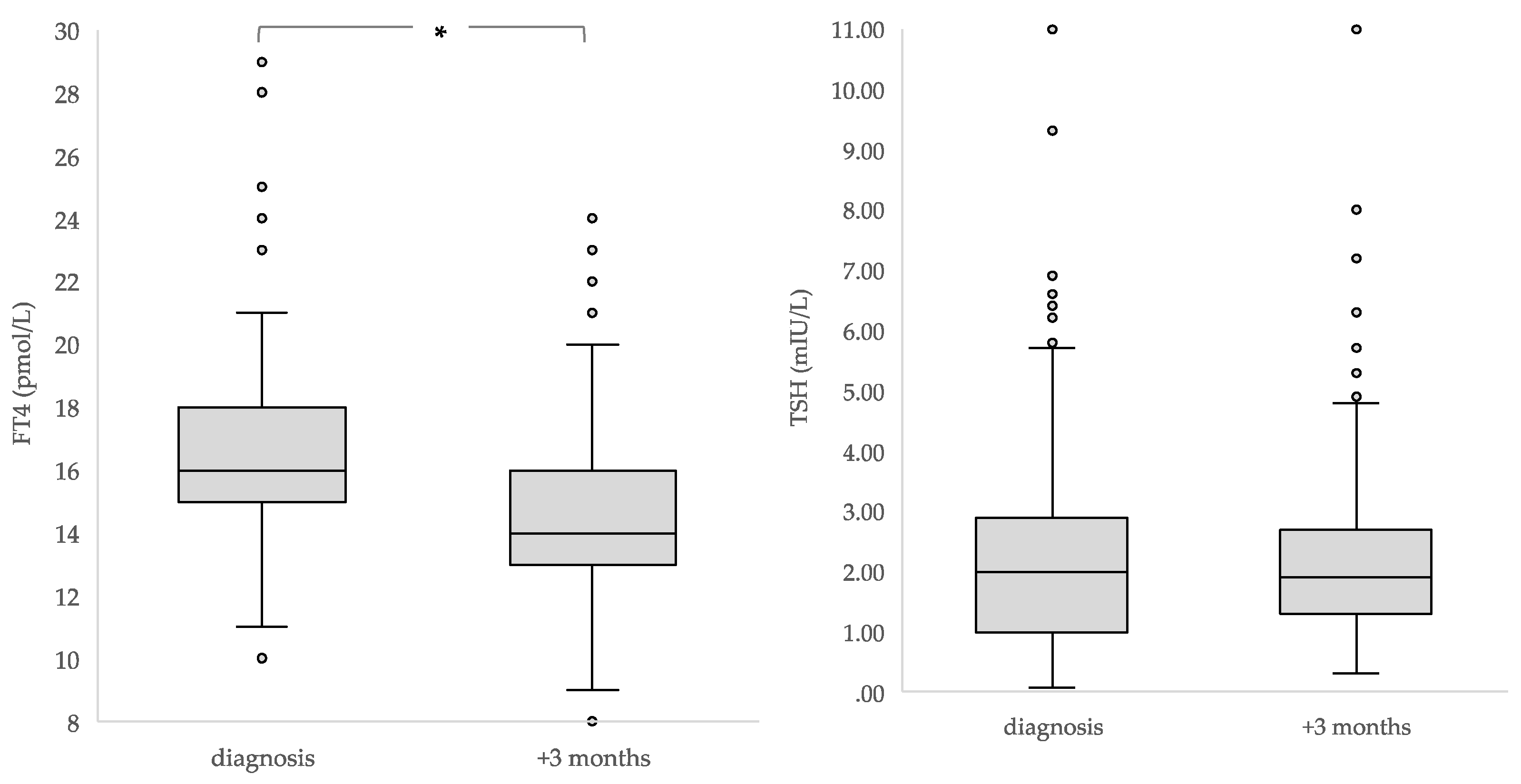
3.3. Decline in FT4 over Time
3.4. Radiotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheng, S.Y.; Leonard, J.L.; Davis, P.J. Molecular aspects of thyroid hormone actions. Endocr. Rev. 2010, 31, 139–170. [Google Scholar] [CrossRef] [Green Version]
- Williams, G.R. Neurodevelopmental and neurophysiological actions of thyroid hormone. J. Neuroendocrinol. 2008, 20, 784–794. [Google Scholar] [CrossRef] [PubMed]
- Lebbink, C.A.; Waguespack, S.G.; van Santen, H.M. Thyroid Dysfunction and Thyroid Cancer in Childhood Cancer Survivors: Prevalence, Surveillance and Management. Front. Horm. Res. 2021, 54, 140–153. [Google Scholar]
- Chao, M.M.; Schwartz, J.L.; Wechsler, D.S.; Thornburg, C.D.; Griffith, K.A.; Williams, J.A. High-risk surgically resected pediatric melanoma and adjuvant interferon therapy. Pediatr. Blood Cancer 2005, 44, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narayanan, K.R.; Bansal, D.; Walia, R.; Sachdeva, N.; Bhansali, A.; Varma, N.; Marwaha, R. Growth failure in children with chronic myeloid leukemia receiving imatinib is due to disruption of GH/IGF-1 axis. Pediatr. Blood Cancer 2013, 60, 1148–1153. [Google Scholar] [CrossRef]
- Walia, R.; Aggarwal, A.; Bhansali, A.; Aggarwal, A.; Varma, N.; Sachdeva, N.; Khandelwal, N.; Bansal, D. Acquired neuro-secretory defect in growth hormone secretion due to Imatinib mesylate and the efficacy of growth hormone therapy in children with chronic myeloid leukemia. Pediatr. Hematol. Oncol. 2020, 37, 99–108. [Google Scholar] [CrossRef]
- Heidemann, P.H.; Stubbe, P.; Beck, W. Transient secondary hypothyroidism and thyroxine binding globulin deficiency in leukemic children during polychemotherapy: An effect of L-asparaginase. Eur. J. Pediatr. 1981, 136, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Ferster, A.; Glinoer, D.; Vliet, G.V.; Otten, J. Thyroid function during l-asparaginase therapy in children with acute lymphoblastic leukemia: Difference between induction and late intensification. J. Pediatr. Hematol. Oncol. 1992, 14, 192–196. [Google Scholar] [CrossRef] [PubMed]
- van Santen, H.M.; Thonissen, N.M.; de Krakert, J.; Vulsma, T. Changes in thyroid hormone state in children receiving chemotherapy. Clin. Endocrinol. 2005, 62, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Chopra, I.J. Euthyroid sick syndrome: Is it a misnomer? J. Clin. Endocrinol. Metab. 1997, 82, 329–334. [Google Scholar] [CrossRef]
- Fliers, E.; Boelen, A. An update on non-thyroidal illness syndrome. J. Endocrinol. Investig. 2021, 44, 1597–1607. [Google Scholar] [CrossRef]
- Jacobs, A.; Derese, I.; vander Perre, S.; Van Puffelen, E.; Verstraete, S.; Pauwels, L.; Verbruggen, S.; Wouters, P.; Langouche, L.; Guerra, G.G.; et al. Non-Thyroidal Illness Syndrome in Critically Ill Children: Prognostic Value and Impact of Nutritional Management. Thyroid 2019, 29, 480–492. [Google Scholar] [CrossRef] [PubMed]
- van den Berghe, G. Euthyroid sick syndrome. Curr. Opin. Anesthesiol. 2000, 13, 89–91. [Google Scholar] [CrossRef] [PubMed]
- van Iersel, L.; Xu, J.; Potter, B.S.; Conklin, H.M.; Zhang, H.; Chemaitilly, W.; Van Santen, H.M.; Merchant, T.E. Clinical Importance of Free Thyroxine Concentration Decline after Radiotherapy for Pediatric and Adolescent Brain Tumors. J. Clin. Endocrinol. Metab. 2019, 104, 4998–5007. [Google Scholar] [CrossRef]
- Xiu, S.; Mu, Z.; Zhao, L.; Sun, L. Low free triiodothyronine levels are associated with risk of frailty in older adults with type 2 diabetes mellitus. Exp. Gerontol. 2020, 138, 111013. [Google Scholar] [CrossRef]
- Weise, K.; Zaritsky, A. Endocrine manifestations of critical illness in the child. Pediatr. Clin. N. Am. 1987, 34, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Brierre, S.; Kumari, R.; Deboisblanc, B.P. The endocrine system during sepsis. Am. J. Med. Sci. 2004, 328, 238–247. [Google Scholar] [CrossRef]
- Re, R.N.; Kourides, I.A.; Ridgway, E.C.; Weintraub, B.D.; Maloof, F. The Effect of Glucocorticoid Administration on Human Pituitary Secretion of Thyrotropin and Prolactin. J. Clin. Endocrinol. Metab. 1976, 43, 338–346. [Google Scholar] [CrossRef]
- Mebis, L.; van den Berghe, G. Thyroid axis function and dysfunction in critical illness. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 745–757. [Google Scholar] [CrossRef]
- van Iersel, L.; van Santen, H.M.; Potter, B.; Li, Z.; Conklin, H.M.; Zhang, H.; Chemaitilly, W.; Merchant, T.E. Clinical impact of hypothalamic-pituitary disorders after conformal radiation therapy for pediatric low-grade glioma or ependymoma. Pediatr. Blood Cancer 2020, 67, e28723. [Google Scholar] [CrossRef]
- Ness, K.K.; Armstrong, G.T.; Kundu, M.; Wilson, C.L.; Tchkonia, T.; Kirkland, J.L. Frailty in childhood cancer survivors. Cancer 2015, 121, 1540–1547. [Google Scholar] [CrossRef] [Green Version]
- Kaltsas, G.; Vgontzas, A.; Chrousos, G. Fatigue, Endocrinopathies, and Metabolic Disorders. PM&R 2010, 2, 393–398. [Google Scholar]
- Susperreguy, S.; Muñoz, L.; Tkalenko, N.Y.; Mascanfroni, I.D.; Alamino, V.A.; Montesinos, M.M.; Masini-Repiso, A.M.; Miras, M.B.; Pellizas, C.G. Growth hormone treatment in children with idiopathic short stature: Correlation of growth response with peripheral thyroid hormone action. Clin. Endocrinol. 2011, 74, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Rodig, N.M.; McDermott, K.C.; Schneider, M.F.; Hotchkiss, H.M.; Yadin, O.; Seikaly, M.G.; Furth, S.L.; Warady, B.A. Growth in children with chronic kidney disease: A report from the Chronic Kidney Disease in Children Study. Pediatr. Nephrol. 2014, 29, 1987–1995. [Google Scholar] [CrossRef] [Green Version]
- Arrigo, T.; Rulli, I.; Sferlazzas, C.; de Luca, F. Pubertal development in cystic fibrosis: An Overview. J. Pediatr. Endocrinol. Metab. 2003, 16 (Suppl. S2), 267–270. [Google Scholar] [PubMed]
- Hokken-Koelega, A.C.S.; Saenger, P.; Cappa, M.; Greggio, N. Unresolved problems concerning optimal therapy of puberty in children with chronic renal diseases. J. Pediatr. Endocrinol. Metab. 2001, 14 (Suppl. 2), 945–952. [Google Scholar] [CrossRef] [PubMed]
- Reiter, E.O.; Lee, P.A. Delayed puberty. Adolesc. Med. Clin. 2002, 13, 101. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Age at diagnosis (yrs) (median, range) | 9.4 (0.0–19.7) |
| No. of females (%) | 127/284 (45%) |
| Diagnosis (number (% of entire cohort)) | |
| Leukemia | 141 (50%) |
| ALL | 118 (42%) |
| AML | 20 (7.0%) |
| CML | 2 (0.7%) |
| Other | 1 (0.4%) |
| Lymphoma | 74 (26%) |
| Hodgkin lymphoma | 35 (12%) |
| B-NHL/B-ALL | 25 (8.8%) |
| Non-B NHL | 12 (4.2%) |
| ALCL | 2 (0.7%) |
| Sarcoma | 38 (13%) |
| Bone tumor (osteosarcoma/Ewing sarcoma) | 22 (7.7%) |
| Rhabdomyosarcoma | 11 (3.9%) |
| Non-rhabdomyosarcoma | 4 (1.4%) |
| Other | 1 (0.4%) |
| Brain tumor | 31 (11%) |
| ATRT | 1 (0.4%) |
| Ependymoma | 5 (1.8%) |
| Low-grade glioma | 3 (1.0%) |
| High-grade glioma | 10 (3.5%) |
| Germ-cell tumor | 2 (0.7%) |
| Medulloblastoma | 9 (3.2%) |
| Optic glioma | 1 (0.4%) |
| Physical condition * | |
| At diagnosis | |
| Good | 76 (38%) |
| Medium | 112 (57%) |
| Poor | 10 (5.1%) |
| Unknown | 22 |
| After three months | |
| Good | 186 (69%) |
| Medium | 74 (28%) |
| Poor | 8 (3.0%) |
| Unknown | 8 |
| All Children (n = 284) | Analysis of Children Who Had Not Received Corticosteroids or Chemotherapy before First Measurement Only (n = 202) | |||||
|---|---|---|---|---|---|---|
| Thyroid Hormone Determinant | Median Concentration at Diagnosis, mIU/L (Range) (No. of Samples) | Median Concentration Three Months after Diagnosis, mIU/L (Range) (No. of Samples) | p-Value | Median Concentration at Diagnosis before Start of Chemotherapy or Corticosteroids, mIU/L (Range) (No. of Samples) | Median Concentration Three Months after Diagnosis, mIU/L (Range) (No. of Samples) | p-Value |
| TSH (0.30–5.00 mIU/L) | 2.00 (0.07–11.0) (n = 222) | 1.90 (0.31–8.00) (n = 276) | 0.334 | 2.30 (0.34–9.40) (n = 141) | 1.90 (0.31–11.00) (n = 199) | <0.001 |
| FT4 (10–22 pmol/L) * | 16 (10–29) (n = 220) | 14 (8–23) (n = 276) | <0.001 | 16 (10–29) (n = 139) | 14 (8–24) (n = 199) | <0.001 |
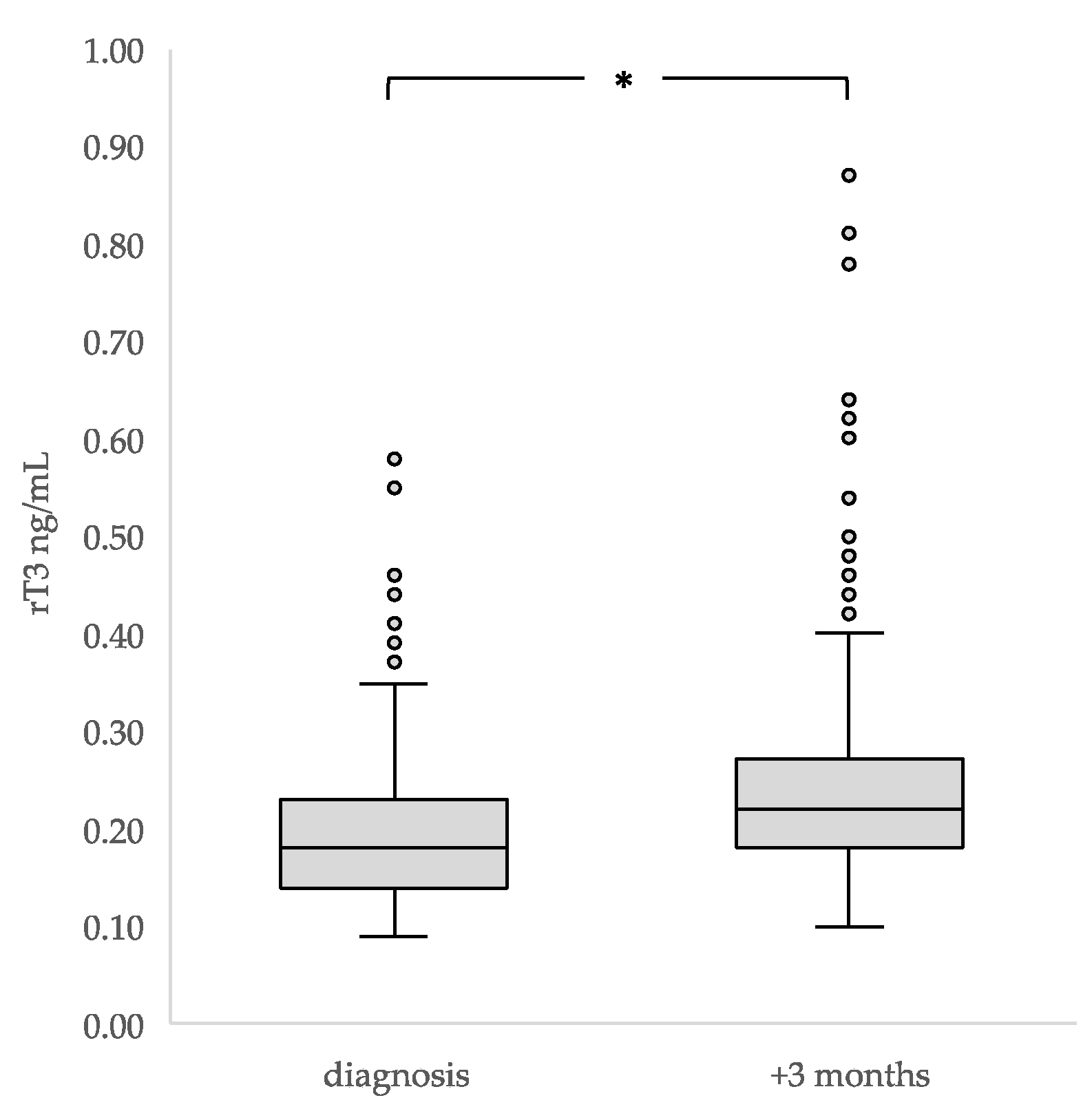
| rT3 (0.098–0.218 ng/mL) | 0.18 (0.09–0.58) (n = 148) | 0.22 (0.10–2.36) (n = 265) | <0.001 | 0.16 (0.09–0.58) (n = 90) | 0.22 (0.10–2.26) (n = 191) | <0.001 |
| A. Risk Factors Associated with ≥20% FT4 Decline | ||
| Covariate/Category | ≥20% FT4 Decline | |
| Univariable OR (95% CI) | Multivariable OR (95% CI) | |
| Age at diagnosis, years | 0.95 (0.89 to 1.02) | 0.97 (0.90 to 1.04) |
| Administration of antimetabolites | 2.59 (0.98 to 6.81) | 2.37 (0.78 to 7.18) |
| Use of corticosteroids <48 h before thyroid hormone measurement after three months | 1.11 (0.27 to 4.55) | 1.55 (0.35 to 6.97) |
| Radiotherapy before thyroid hormone measurement after three months | 0.54 (0.11 to 2.67) | 0.93 (0.15 to 5.65) |
| B. Risk factors associated with elevated rT3 concentration | ||
| Covariate/Category | Elevated rT3 Concentration | |
| Univariable OR (95% CI) | Multivariable OR (95% CI) | |
| Age at diagnosis, years | 0.96 (0.92 to 1.00) | 0.97 (0.92 to 1.01) |
| Brain tumor vs. others a | 3.16 (1.29 to 7.76) | 3.17 (1.19 to 8.41) b |
| Physical condition three months after diagnosis Medium/poor vs. good | 1.54 (0.90 to 2.64) | 1.42 (0.80 to 2.53) |
| Use of corticosteroids <48 h before thyroid hormone measurement | 1.68 (0.67 to 4.20) | 1.72 (0.67 to 4.43) |
| Underweight (<−2 SDS) | 0.51 (0.12 to 2.08) | 0.57 (0.13 to 2.45) |
| NOTE. 3A. Multivariable logistic regression for risk factors of children with a ≥20% FT4 decline from diagnosis to three months after diagnosis (n = 38) compared with children without ≥20% FT4 decline from diagnosis to three months after diagnosis (n = 98). NOTE. 3B. Multivariable logistic regression for risk factors of children with elevated rT3 concentrations three months after diagnosis (n = 133) compared with children without elevated rT3 concentrations three months after diagnosis (n = 132). | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lebbink, C.A.; van den Bos, C.; Dierselhuis, M.P.; Fiocco, M.; Verrijn Stuart, A.A.; Lentjes, E.G.W.M.; Plasschaert, S.L.A.; Tissing, W.J.E.; van Santen, H.M. Thyroid Profile in the First Three Months after Starting Treatment in Children with Newly Diagnosed Cancer. Cancers 2023, 15, 1500. https://doi.org/10.3390/cancers15051500
Lebbink CA, van den Bos C, Dierselhuis MP, Fiocco M, Verrijn Stuart AA, Lentjes EGWM, Plasschaert SLA, Tissing WJE, van Santen HM. Thyroid Profile in the First Three Months after Starting Treatment in Children with Newly Diagnosed Cancer. Cancers. 2023; 15(5):1500. https://doi.org/10.3390/cancers15051500
Chicago/Turabian StyleLebbink, Chantal A., Cor van den Bos, Miranda P. Dierselhuis, Marta Fiocco, Annemarie A. Verrijn Stuart, Eef G. W. M. Lentjes, Sabine L. A. Plasschaert, Wim J. E. Tissing, and Hanneke M. van Santen. 2023. "Thyroid Profile in the First Three Months after Starting Treatment in Children with Newly Diagnosed Cancer" Cancers 15, no. 5: 1500. https://doi.org/10.3390/cancers15051500