
COVID-19 Severity and Survival over Time in Patients with Hematologic Malignancies: A Population-Based Registry Study

 , , , , , , , , , , , , , ,
, , , , , , , , , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
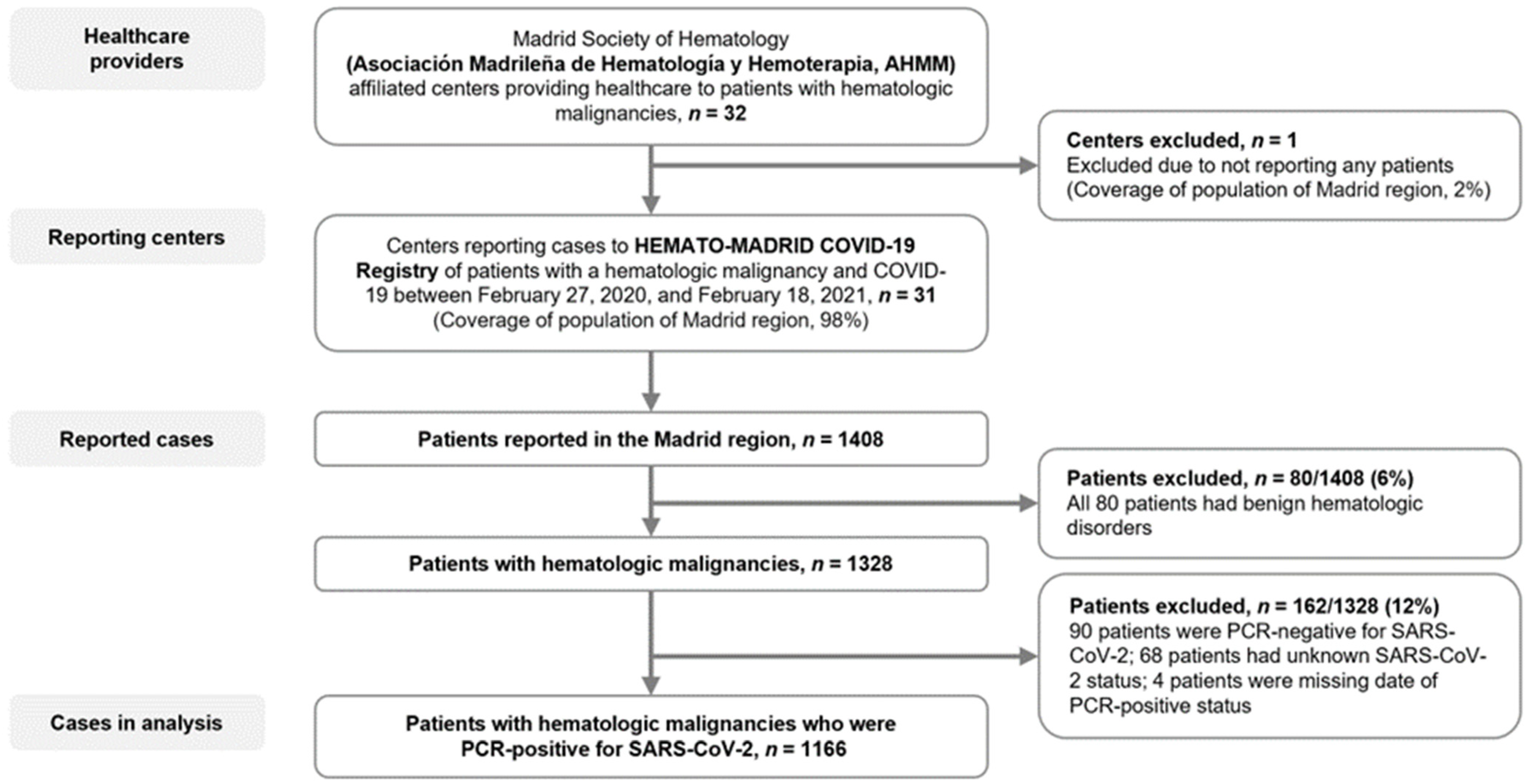
2.1. Study Design and Participants
2.2. Data Collection and End Points
2.3. Statistical Analyses
3. Results
3.1. Patients
3.2. COVID-19 Diagnosis and Treatment
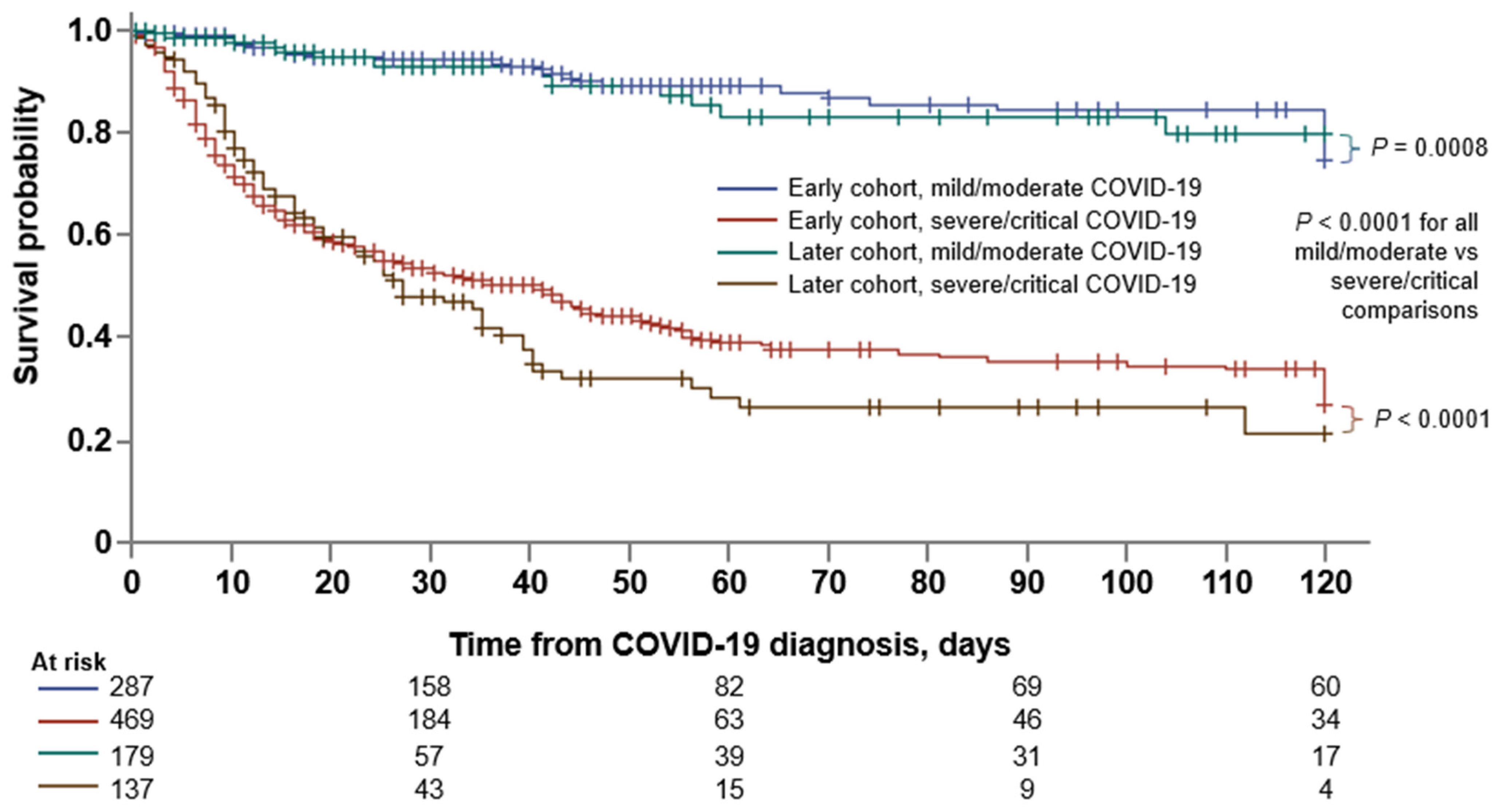
3.3. Comparison between the Early and Later Cohorts
3.4. Factors Associated with COVID-19 Severity
3.5. Factors Associated with Mortality
3.6. Comparison between HM and Non-Cancer Inpatients with COVID-19
3.7. Post COVID-19 Condition
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 7 September 2022).
- Spanish Ministry of Health Social Services and Equality. Madrid—The Evolution of the Coronavirus by Region. Available online: https://www.epdata.es/datos/evolucion-coronavirus-cada-comunidad/518/madrid/304 (accessed on 6 September 2022).
- Statistical Information for the Analysis of the Impact of the COVID-19 Crisis. Available online: https://www.ine.es/en/covid/covid_inicio_en.htm (accessed on 6 September 2022).
- Dennis, J.M.; McGovern, A.P.; Vollmer, S.J.; Mateen, B.A. Improving survival of critical care patients with coronavirus disease 2019 in England: A national cohort study, March to June. Crit. Care Med. 2020, 49, 209. [Google Scholar] [CrossRef] [PubMed]
- Gray, W.K.; Navaratnam, A.V.; Day, J.; Wendon, J.; Briggs, T.W. Changes in COVID-19 in-hospital mortality in hospitalised adults in England over the first seven months of the pandemic: An observational study using administrative data. Lancet Reg. Health Eur. 2021, 5, 100104. [Google Scholar] [CrossRef] [PubMed]
- I Horwitz, L.; A Jones, S.; Cerfolio, R.J.; Francois, F.; Greco, J.; Rudy, B.; Petrilli, C.M. Trends in COVID-19 Risk-Adjusted Mortality Rates. J. Hosp. Med. 2020, 16, 90–92. [Google Scholar] [CrossRef]
- The Royal Society. Available online: https://royalsociety.org/-/media/policy/projects/set-c/set-c-long-covid.pdf (accessed on 6 September 2022).
- Asch, D.A.; Sheils, N.E.; Islam, M.N.; Chen, Y.; Werner, R.M.; Buresh, J.; Doshi, J.A. Variation in US Hospital Mortality Rates for Patients Admitted With COVID-19 During the First 6 Months of the Pandemic. JAMA Intern. Med. 2021, 181, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Galloway, S.E.; Paul, P.; MacCannell, D.R.; Johansson, M.A.; Brooks, J.T.; MacNeil, A.; Slayton, R.B.; Tong, S.; Silk, B.J.; Armstrong, G.L.; et al. Emergence of SARS-CoV-2 B.1.1.7 Lineage - United States, December 29, 2020-January 12, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 95–99. [Google Scholar] [CrossRef]
- Booth, S.; Curley, H.M.; Varnai, C.; Arnold, R.; Lee, L.Y.W.; Campton, N.A.; Cook, G.; Purshouse, K.; Aries, J.; Innes, A.; et al. Key findings from the UKCCMP cohort of 877 patients with haematological malignancy and COVID-19: Disease control as an important factor relative to recent chemotherapy or anti-CD20 therapy. Br. J. Haematol. 2022, 196, 892–901. [Google Scholar] [CrossRef]
- García-Suárez, J.; de la Cruz, J.; De La Cruz, J.; Cedillo, Á.; Llamas, P.; Duarte, R.; Jiménez-Yuste, V.; Hernández-Rivas, J.Á.; Gil-Manso, R.; Kwon, M.; et al. Impact of hematologic malignancy and type of cancer therapy on COVID-19 severity and mortality: Lessons from a large population-based registry study. J. Hematol. Oncol. 2020, 13, 133. [Google Scholar] [CrossRef]
- Passamonti, F.; Cattaneo, C.; Arcaini, L.; Bruna, R.; Cavo, M.; Merli, F.; Angelucci, E.; Krampera, M.; Cairoli, R.; Della Porta, M.G.; et al. Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: A retrospective, multicentre, cohort study. Lancet Haematol. 2020, 7, e737–e745. [Google Scholar] [CrossRef]
- Piñana, J.L.; Martino, R.; García-García, I.; Parody, R.; Morales, M.D.; Benzo, G.; Gómez-Catalan, I.; Coll, R.; Fuente, I.D.L.; Luna, A.; et al. Risk factors and outcome of COVID-19 in patients with hematological malignancies. Exp. Hematol. Oncol. 2020, 9, 21. [Google Scholar] [CrossRef]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martín-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of patients with hematologic malignancies and COVID-19: A systematic review and meta-analysis of 3377 patients. Blood 2020, 136, 2881–2892. [Google Scholar] [CrossRef]
- Johns Hopkins University of Medicine—Coronavirus Resource Center. Mortality Analyses. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 6 September 2022).
- Lee, L.Y.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef] [PubMed]
- Pagano, L.; Salmanton-García, J.; Marchesi, F.; Busca, A.; Corradini, P.; Hoenigl, M.; Klimko, N.; Koehler, P.; Pagliuca, A.; Passamonti, F.; et al. COVID-19 infection in adult patients with hematological malignancies: A European Hematology Association Survey (EPICOVIDEHA). J. Hematol. Oncol. 2021, 14, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Roeker, L.E.; Eyre, T.A.; Thompson, M.C.; Lamanna, N.; Coltoff, A.R.; Davids, M.S.; Baker, P.O.; Leslie, L.A.; Rogers, K.A.; Allan, J.N.; et al. COVID-19 in patients with CLL: Improved survival outcomes and update on management strategies. Blood 2021, 138, 1768–1773. [Google Scholar] [CrossRef] [PubMed]
- Wood, W.A.; Neuberg, D.S.; Thompson, J.C.; Tallman, M.S.; Sekeres, M.A.; Sehn, L.H.; Anderson, K.; Goldberg, A.D.; Pennell, N.A.; Niemeyer, C.M.; et al. Outcomes of Patients with Hematologic Malignancies and COVID-19 Infection: A Report from the ASH Research Collaborative Data Hub. Blood 2020, 136, 7–8. [Google Scholar] [CrossRef]
- Wood, W.A.; Neuberg, D.S.; Thompson, J.C.; Tallman, M.S.; Sekeres, M.A.; Sehn, L.H.; Anderson, K.C.; Goldberg, A.D.; Pennell, N.A.; Niemeyer, C.M.; et al. Outcomes of patients with hematologic malignancies and COVID-19: A report from the ASH Research Collaborative Data Hub. Blood Adv. 2020, 4, 5966–5975. [Google Scholar] [CrossRef] [PubMed]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 6 October 2021).
- Pinato, D.J.; Tabernero, J.; Bower, M.; Scotti, L.; Patel, M.; Colomba, E.; Dolly, S.; Loizidou, A.; Chester, J.; Mukherjee, U.; et al. Prevalence and impact of COVID-19 sequelae on treatment and survival of patients with cancer who recovered from SARS-CoV-2 infection: Evidence from the OnCovid retrospective, multicentre registry study. Lancet Oncol. 2021, 22, 1669–1680. [Google Scholar] [CrossRef]
- Tang, Y.W.; Schmitz, J.E.; Persing, D.H.; Stratton, C.W. Laboratory Diagnosis of COVID-19: Current Issues and Challenges. J. Clin. Microbiol. 2020, 58, e00512–e00520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO COVID-19: Case Definitions, Updated in Public Health Surveillance for COVID-19. Available online: https://apps.who.int/iris/bitstream/handle/10665/333912/WHO-2019-nCoV-Surveillance_Case_Definition-2020.1-eng.pdf (accessed on 7 August 2020).
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection when Novel Coronavirus (nCoV) Infection is Suspected. Available online: https://www.who.int/publications/i/item/10665-332299 (accessed on 12 January 2020).
- Casas-Rojo, J.; Antón-Santos, J.; Millán-Núñez-Cortés, J.; Lumbreras-Bermejo, C.; Ramos-Rincón, J.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.; Vargas-Núñez, J.; et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Registry. Rev. Clín. Esp. 2020, 220, 480–494. [Google Scholar] [CrossRef]
- Chavez-MacGregor, M.; Lei, X.; Zhao, H.; Scheet, P.; Giordano, S.H. Evaluation of COVID-19 Mortality and Adverse Outcomes in US Patients with or Without Cancer. JAMA Oncol. 2022, 8, 69. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.-Y.; Desai, A.; de Lima Lopes, G., Jr.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet. 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Shah, V.; Ko Ko, T.; Zuckerman, M.; Vidler, J.; Sharif, S.; Mehra, V.; Gandhi, S.; Kuhnl, A.; Yallop, D.; Avenoso, D.; et al. Poor outcome and prolonged persistence of SARS-CoV-2 RNA in COVID-19 patients with haematological malignancies; King’s College Hospital experience. Br. J. Haematol. 2020, 190, e279–e282. [Google Scholar] [CrossRef] [PubMed]
- Recovery Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Westblade, L.F.; Brar, G.; Pinheiro, L.C.; Paidoussis, D.; Rajan, M.; Martin, P.; Goyal, P.; Sepulveda, J.L.; Zhang, L.; George, G.; et al. SARS-CoV-2 Viral Load Predicts Mortality in Patients with and without Cancer Who Are Hospitalized with COVID-19. Cancer Cell 2020, 38, 661–671.e2. [Google Scholar] [CrossRef]
- Barbui, T.; Iurlo, A.; Masciulli, A.; Carobbio, A.; Ghirardi, A.; Rossi, G.; Harrison, C.; Alvarez-Larran, A.; Elli, E.M.; Kiladjian, J.-J.; et al. Long-term follow-up of recovered MPN patients with COVID-19. Blood Cancer J. 2021, 11, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Yan, D.; Zhang, X.; Chen, C.; Jiang, D.; Liu, X.; Zhou, Y.; Huang, C.; Zhou, Y.; Guan, Z.; Ding, C.; et al. Characteristics of Viral Shedding Time in SARS-CoV-2 Infections: A Systematic Review and Meta-Analysis. Front Public Health 2021, 9, 652842. [Google Scholar] [CrossRef]
- Tejerina, F.; Catalan, P.; Rodriguez-Grande, C.; Adan, J.; Rodriguez-Gonzalez, C.; Muñoz, P.; Aldamiz, T.; Diez, C.; Perez, L.; Fanciulli, C.; et al. Post-COVID-19 syndrome. SARS-CoV-2 RNA detection in plasma, stool, and urine in patients with persistent symptoms after COVID-19. BMC Infect. Dis. 2022, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients with Hematologic Malignancies, N = 1166 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | Lymphoid Malignancies | Myeloid Malignancies | ||||||||
| NHL | MM | CLL | HL | ALL | MDS | AML | CML | Ph-MPN | ||
| Patients, n (%) | 1166 (100) | 325 (27.9) | 263 (22.6) | 175 (15.0) | 50 (4.3) | 26 (2.2) | 115 (9.9) | 92 (7.9) | 33 (2.8) | 87 (7.5) |
| Age, y | N = 1147 | n = 322 | n = 253 | n = 174 | n = 49 | n = 26 | n = 113 | n = 91 | n = 32 | n = 87 |
| Median (IQR) | 71 (59–79) | 69 (57–76) | 72 (63–79) | 74 (63–82) | 57 (42–71) | 47 (33–59) | 79 (71–84) | 65 (50–75) | 64 (54–84) | 72 (65–82) |
| Sex, n (%) | N = 1152 | n = 321 | n = 261 | n = 175 | n = 49 | n = 26 | n = 113 | n = 91 | n = 33 | n = 83 |
| Female | 464 (40.3) | 136 (42.4) | 108 (41.4) | 61 (34.9) | 18 (36.7) | 8 (30.8) | 41 (36.3) | 46 (50.5) | 8 (24.2) | 28 (34) |
| Male | 688 (59.7) | 185 (57.6) | 153 (58.6) | 114 (65.1) | 31 (63.3) | 18 (69.2) | 72 (63.7) | 45 (49.5) | 25 (75.8) | 55 (66) |
| Comorbidity count | N = 1166 | n = 325 | n = 263 | n = 175 | n = 50 | n = 26 | n = 115 | n = 92 | n = 33 | n = 87 |
| 0 | 314 (26.9) | 96 (29.4) | 62 (23.6) | 44 (25.1) | 13 (26.0) | 15 (57.7) | 22 (19.1) | 33 (35.9) | 11 (33.3) | 18 (20.7) |
| 1 | 484 (41.5) | 140 (43.1) | 102 (38.8) | 77 (44.0) | 18 (36.0) | 8 (30.8) | 50 (43.5) | 40 (43.5) | 9 (27.3) | 40 (46.0) |
| ≥2 | 368 (31.6) | 89 (27.4) | 99 (37.6) | 54 (30.9) | 19 (38) | 3 (11.6) | 43 (37.4) | 19 (20.7) | 13 (39.4) | 29 (33.3) |
| Stem cell transplantation, * n (%) | N = 1127 | n = 312 | n = 259 | n = 168 | n = 47 | n = 24 | n = 112 | n = 92 | n = 32 | n = 81 |
| Autologous | 100 (8.9) | 23 (7.4) | 66 (25.5) | 0 | 7 (14.9) | 1 (4.2) | 1 (0.9) | 2 (2.2) | 0 | 0 |
| Allogeneic | 56 (5.0) | 5 (1.6) | 3 (1.2) | 1 (0.6) | 4 (8.5) | 9 (37.5) | 9 (8.0) | 25 (27.2) | 0 | 0 |
| No | 971 (86.2) | 284 (91.0) | 190 (73.4) | 167 (99.4) | 36 (76.6) | 14 (58.3) | 102 (91.1) | 65 (70.7) | 32 (100) | 81 (100) |
| Cancer therapy, within 30 d, † n (%) | N = 1162 | n = 325 | n = 260 | n = 175 | n = 50 | n = 26 | n = 115 | n = 92 | n = 33 | n = 86 |
| Active therapy | 679 (58.4) | 178 (54.8) | 190 (73.1) | 55 (31.4) | 24 (48.0) | 16 (61.5) | 50 (43.5) | 61 (66.3) | 29 (87.9) | 76 (88.4) |
| Conventional chemotherapy | 260 (22.4) | 112 (34.5) | 82 (31.5) | 3 (1.7) | 17 (34.0) | 13 (50.0) | 2 (1.7) | 31 (33.7) | 0 | 0 |
| Low-intensity chemotherapy | 71 (6.1) | 4 (1.2) | 8 (3.1) | 3 (1.7) | 0 | 1 (3.8) | 3 (2.6) | 0 | 4 (12.1) | 48 (55.8) |
| Molecular-targeted therapy | 130 (11.2) | 13 (4.0) | 20 (7.7) | 43 (24.6) | 0 | 1 (3.8) | 1 (0.9) | 5 (5.4) | 24 (72.7) | 23 (26.7) |
| Immunotherapy, mAb only ‡ | 56 (4.8) | 38 (11.7) | 10 (3.8) | 3 (1.7) | 4 (8.0) | 1 (3.8) | 0 | 0 | 0 | 0 |
| Immunomodulator drugs | 71 (6.1) | 1 (0.3) | 69 (26.5) | 0 | 0 | 0 | 1 (0.9) | 0 | 0 | 0 |
| Hypomethylating agents | 49 (4.2) | 1 (0.3) | 0 | 0 | 0 | 0 | 24 (20.9) | 24 (26.1) | 0 | 0 |
| Supportive therapy | 31 (2.7) | 5 (1.5) | 0 | 2 (1.1) | 0 | 0 | 19 (16.5) | 0 | 0 | 5 (5.8) |
| Active, not detailed | 11 (0.9) | 4 (1.2) | 1 (0.4) | 1 (0.6) | 3 (6.0) | 0 | 0 | 1 (1.1) | 1 (3.0) | 0 |
| No active therapy | 483 (41.6) | 147 (45.2) | 70 (26.9) | 120 (68.6) | 26 (52.0) | 10 (38.5) | 65 (56.5) | 31 (33.7) | 4 (12.1) | 10 (11.6) |
| Survival Estimate, % (95% CI) | Hazard Ratio (95% CI) | |||
|---|---|---|---|---|
| 30-d | 60-d | Unadjusted | Adjusted * | |
| All patients † | 68.4 (65.3–71.3) | 56.3 (52.6–59.9) | ||
| Age | ||||
| Age 18–49 y | 93.7 (86.6–97.1) | 90.1 (80.8–95.1) | reference | reference |
| Age 50–79 y | 72.8 (68.9–76.2) | 58.8 (54.0–63.3) | 3.59 (2.01–6.42) | 3.01 (1.67–5.43) |
| Age ≥ 80 y | 46.3 (39.8–52.5) | 35.1 (28.3–42.0) | 7.86 (4.36–14.2) | 6.24 (3.39–11.49) |
| Sex | ||||
| Female | 69.5 (64.5–74.0) | 60.0 (54.2–65.4) | reference | reference |
| Male | 67.4 (63.3–71.2) | 53.6 (48.6–58.3) | 1.12 (0.91–1.38) | 1.15 (0.93–1.41) |
| Comorbidities | ||||
| 0 | 79.3 (73.5–84.0) | 69.7 (62.3–76.0) | reference | reference |
| 1 | 70.9 (66.1–75.1) | 56.3 (50.4–61.7) | 1.49 (1.12–1.98) | 1.10 (0.83–1.48) |
| 2 | 61.4 (53.7–68.2) | 49.7 (41.0–57.9) | 1.89 (1.37–2.61) | 1.15 (0.82–1.61) |
| ≥3 | 50.4 (41.4–58.7) | 41.6 (32.0–51.0) | 2.57 (1.84–3.59) | 1.43 (1.01–2.03) |
| Hematologic malignancy | ||||
| NHL | 71.0 (64.9–76.2) | 57.2 (49.9–63.8) | reference | reference |
| MM | 69.7 (62.9–75.5) | 57.3 (49.1–64.7) | 0.98 (0.73–1.32) | 0.83 (0.61–1.12) |
| CLL | 59.1 (50.5–66.8) | 49.8 (39.8–59.0) | 1.37 (1.00–1.87) | 1.02 (0.74–1.41) |
| HL | 73.0 (55.6–84.4) | 68.1 (49.0–81.3) | 0.77 (0.43–1.41) | 0.89 (0.49–1.64) |
| ALL | 78.4 (52.2–91.3) | 47.0 (17.6–72.1) | 0.99 (0.46–2.13) | 2.31 (1.04–5.12) |
| MDS | 59.4 (48.9–68.4) | 48.7 (37.2–59.3) | 1.46 (1.04–2.05) | 0.96 (0.68–1.37) |
| AML | 63.8 (52.2–73.2) | 53.6 (41.3–64.3) | 1.41 (0.99–2.01) | 1.68 (1.17–2.40) |
| CML | 81.8 (58.5–92.8) | 81.8 (58.5–92.8) | 0.58 (0.24–1.43) | 0.44 (0.18–1.08) |
| Ph-MPN | 82.4 (71.0–89.6) | 66.4 (50.9–78.0) | 0.70 (0.43–1.13) | 0.51 (0.31–0.82) |
| Stem cell transplantation ‡ | ||||
| No | 65.7 (62.2–68.9) | 53.9 (49.8–57.8) | reference | reference |
| Autologous | 85.3 (75.1–91.6) | 80.8 (68.7–88.6) | 0.58 (0.34–0.99) | 0.54 (0.31–0.95) |
| Allogeneic | 86.2 (71.8–93.6) | 69.6 (51.2–82.2) | 0.35 (0.20–0.59) | 1.15 (0.64–2.07) |
| Cancer therapy, within 30 d ¶ | ||||
| No active therapy | 67.4 (62.3–71.9) | 58.7 (51.8–63.3) | reference | reference |
| Active therapy | 69.0 (65.0–72.7) | 55.4 (50.6–60.1) | 1.08 (0.88–1.33) | 1.10 (0.89–1.36) |
| Conventional chemotherapy | 66.4 (59.6–72.3) | 51.8 (44.0–59.2) | 1.16 (0.90–1.50) | 1.49 (1.14–1.93) |
| Low-intensity chemotherapy | 76.8 (63.4–85.8) | 63.1 (46.1–76.1) | 0.80 (0.48–1.32) | 0.65 (0.39–1. 08) |
| Molecular targeted therapy | 69.2 (59.4–77.1) | 60.4 (48.9–70.0) | 1.05 (0.75–1.47) | 1.02 (0.73–1.44) |
| Immunotherapy, mAb only | 68.9 (53.2–80.2) | 47.7 (30.2–63.2) | 1.14 (0.72–1.80) | 1.40 (0.88–2.24) |
| Immunomodulator drugs | 70.4 (56.8–80.5) | 58.2 (42.3–71.1) | 0.88 (0.56–1.39) | 0.84 (0.53–1.33) |
| Hypomethylating agents | 64.6 (47.6–77.3) | 60.5 (42.8–74.3) | 1.46 (0.94–2.27) | 1.07 (0.68–1.67) |
| Supportive therapy | 64.7 (43.1–79.8) | 41.2 (19.9–61.4) | 1.39 (0.79–2.46) | 0.90 (0.51–1.61) |
| Time period of COVID-19 diagnosis | ||||
| Early cohort (1st wave, February–June 2020) | 67.4 (63.7–70.8) | 56.3 (52.0–60.4) | reference | reference |
| Later cohort (2nd/3rd wave, July 2020–February 2021) | 70.9 (64.9–76.1) | 55.8 (48.0–62.9) | 0.93 (0.73–1.17) | 0.99 (0.79–1.26) |
| Care setting of COVID-19 treatment | ||||
| Outpatient | 99.4 (95.5–99.9) | 93.8 (85.3–97.4) | reference | reference |
| Inpatient | 62.1 (58.6–65.4) | 49.3 (45.2–53.2) | 10.8 (5.37–21.8) | 8.81 (4.37–17.8) |
| Intensive care unit | 45.2 (38.9–51.2) | 28.0 (22.1–34.1) | 2.21 (1.80–2.71) | 2.42 (1.97–2.99) |
| Pharmacologic therapies for COVID-19 ¶¶ | ||||
| (Hydroxy)chloroquine | 67.7 (63.6–71.4) | 56.9 (52.2–61.2) | 1.00 (0.81–1.23) | 0.96 (0.77–1.19) |
| Azithromycin | 67.7 (62.5–72.5) | 56.6 (50.3–62.3) | 1.06 (0.86–1.30) | 1.03 (0.83–1.27) |
| Lopinavir/darunavir | 66.1 (60.9–70.7) | 56.1 (50.3–61.5) | 1.03 (0.84–1.26) | 1.09 (0.88–1.35) |
| Remdesivir | 80.5 (68.2–88.4) | 61.5 (46.3–73.6) | 0.71 (0.46–1.08) | 0.84 (0.55–1.28) |
| Tocilizumab | 66.3 (58.3–73.2) | 52.0 (43.1–60.1) | 1.07 (0.83–1.37) | 1.25 (0.96–1.62) |
| Corticosteroids | 59.8 (55.4–63.8) | 45.2 (40.4–49.9) | 2.15 (1.71–2.69) | 2.06 (1.64–2.59) |
| Oxygen support during COVID-19 treatment | ||||
| No | 98 (94–99) | 91 (85–95) | reference | reference |
| Low-flow oxygen support | 67.5 (63.0–71.6) | 57.7 (52.4–62.6) | 4.9 (3.09–7.62) | 3.68 (2.33–5.81) |
| High-flow oxygen support or mechanical ventilation | 44.3 (37.9–50.4) | 26.8 (20.9–33.0) | 10.1 (6.4–15.9) | 8.52 (5.38–13.5) |
| Clinical severity of COVID-19 | ||||
| Mild | 96.1 (91.6–98.2) | 90.5 (82.3–95.7) | reference | reference |
| Moderate | 92.9 (88.2–95.7) | 85.8 (78.9–90.6) | 1.45 (0.77–2.74) | 1.17 (0.62–2.22) |
| Severe | 57.8 (52.5–62.8) | 46.8 (40.8–52.5) | 7.34 (4.26–12.7) | 5.64 (3.26–9.79) |
| Critical | 40.9 (34.0–47.7) | 21.7 (15.7–28.4) | 12.4 (7.17–21.5) | 11.0 (6.32–19.2) |
| Patients with COVID-19 Severity Data, N = 1131 | Odds Ratio (95% CI) | ||||
|---|---|---|---|---|---|
| Total, N = 1131* | Mild/Moderate, n = 508 | Severe/Critical, n = 623 | Unadjusted | Adjusted † | |
| Age, y | n = 1112 | n = 491 | n = 621 | ||
| Median (IQR) | 71 (60–79) | 66 (54–76) | 73 (65–82) | n/a | n/a |
| Age 18–49 y, n (%) | 129 (11.6) | 88 (17.9) | 41 (6.6) | reference | reference |
| Age 50–79 y, n (%) | 718 (64.6) | 318 (64.8) | 400 (64.4) | 2.70 (1.81–4.02) | 2.19 (1.44–3.33) |
| Age ≥80 y, n (%) | 265 (23.8) | 85 (17.3) | 180 (29.0) | 4.54 (2.89–7.14) | 3.37 (2.08–5.46) |
| Sex, n (%) | N = 1117 | n = 501 | n = 616 | ||
| Female | 448 (40.1) | 212 (42.3) | 236 (38.3) | reference | reference |
| Male | 669 (59.9) | 289 (57.7) | 380 (61.7) | 1.18 (0.93–1.50) | 1.16 (0.90–1.50) |
| Comorbidity count | N = 1131 | n = 508 | n = 623 | ||
| 0 | 305 (27.0) | 181 (35.6) | 124 (19.9) | reference | reference |
| 1 | 469 (41.5) | 199 (39.2) | 270 (43.3) | 1.98 (1.48–2.65) | 1.53 (1.12–2.10) |
| ≥2 | 357 (31.6) | 128 (25.2) | 229 (36.8) | 2.61 (1.91–3.58) | 1.62 (1.14–2.30) |
| Hematologic malignancy, n (%) | N = 1131 | n = 508 | n = 623 | ||
| Lymphoid malignancy | 816 (72.1) | 386 (76.0) | 430 (69.0) | reference | reference |
| Myeloid malignancy | 315 (27.9) | 122 (24.0) | 193 (31.0) | 1.42 (1.09–1.85) | 1.30 (0.98–1.72) |
| NHL | 315 (27.9) | 165 (32.5) | 150 (24.1) | reference | reference |
| MM | 258 (22.8) | 130 (25.6) | 128 (20.5) | 1.08 (0.78–1.51) | 0.97 (0.69–1.38) |
| CLL | 169 (14.9) | 55 (10.8) | 114 (18.3) | 2.28 (1.54–3.37) | 2.02 (1.34–3.05) |
| HL | 48 (4.2) | 24 (4.7) | 24 (3.9) | 1.10 (0.60–2.02) | 1.61 (0.82–3.16) |
| ALL | 26 (2.3) | 12 (2.4) | 14 (2.2) | 1.28 (0.58–2.86) | 2.88 (1.22–6.82) |
| MDS | 111 (9.8) | 41 (8.1) | 70 (11.2) | 1.81 (1.18–2.76) | 1.31 (0.82–2.11) |
| AML | 91 (8.0) | 29 (5.7) | 62 (10.0) | 2.35 (1.44–3.85) | 3.13 (1.83–5.34) |
| CML | 31 (2.7) | 21 (4.1) | 10 (1.6) | 0.52 (0.24–1.15) | 0.57 (0.24–1.32) |
| Ph-MPN | 82 (7.3) | 31 (6.1) | 51 (8.2) | 1.81 (1.10–2.98) | 1.43 (0.84–2.42) |
| Stem cell transplantation, ‡ n (%) | N = 1098 | n = 494 | n = 604 | ||
| Autologous | 100 (9.1) | 65 (13.2) | 35 (5.8) | 0.39 (0.26–0.61) | 0.56 (0.35–0.90) |
| Allogeneic | 56 (5.1) | 31 (6.3) | 25 (4.1) | 0.59 (0.34–1.02) | 1.02 (0.56–1.84) |
| No | 942 (85.8) | 398 (80.6) | 544 (90.1) | reference | reference |
| Cancer therapy, within 30 d, ¶ n (%) | N = 1131 | n = 508 | n = 623 | ||
| No active therapy | 461 (41.8) | 208 (40.9) | 253 (40.6) | reference | reference |
| Active therapy | 670 (59.2) | 300 (59.1) | 370 (59) | 1.01 (0.80–1.29) | 1.02 (0.79–1.31) |
| Conventional chemotherapy | 255 (23) | 125 (24.6) | 130 (20.9) | 0.86 (0.63–1.16) | 1.05 (0.76–1.46) |
| Low-intensity chemotherapy | 67 (6) | 28 (5.5) | 39 (6.3) | 1.15 (0.68–1.92) | 0.88 (0.51–1.52) |
| Molecular-targeted therapy | 129 (11.4) | 56 (11.0) | 73 (11.7) | 1.07 (0.72–1.59) | 1.06 (0.70–1.61) |
| Immunotherapy, mAb only | 56 (5) | 24 (4.7) | 32 (8.7) | 1.10 (0.63–1.92) | 1.21 (0.67–2.21) |
| Immunomodulator drugs | 70 (6) | 33 (6.6) | 37 (5.9) | 0.92 (0.56–1.53) | 0.83 (0.49–1.41) |
| Hypomethylating agents | 49 (4) | 16 (3.2) | 33 (5.3) | 1.70 (0.91–3.17) | 1.23 (0.65–2.33) |
| Supportive therapy | 30 (2.7) | 11 (2.2) | 19 (3.1) | 1.42 (0.66–3.05) | 0.98 (0.51–1.52) |
| Active, not detailed | 14 (1.2) | 7 (1.4) | 7 (1.1) | 0.69 (0.21; 2.2) | 0.60 (0.16–2.24) |
| Early Cohort | Later Cohort | |||||
|---|---|---|---|---|---|---|
| Patients with Hematologic Malignancies n = 681 | Non-Cancer Inpatients n = 5227 | Odds Ratio (95% CI) | Patients with Hematologic Malignancies n = 215 | Non-Cancer Inpatients n = 5312 | Odds Ratio (95% CI) | |
| Age, y | n = 207 | |||||
| Median (IQR) | 72 (62–80) | 66 (53–68) | – | 72 (64–80) | 70 (57–81) | – |
| Age ≥ 65 y, n (%) | 483 (70.9) | 2829 (54.1) | 2.68 (1.74–2.46) | 151 (73.0) | 3248 (61.1) | 1.71 (1.25–2.34) |
| Sex, n (%) | n = 669 | n = 5218 | ||||
| Female | 259 (38.7) | 2213 (42.4) | reference | 89 (41.4) | 2272 (42.8) | reference |
| Male | 410 (61.3) | 3005 (57.6) | 1.17 (0.99–1.37) | 126 (58.6) | 3040 (57.2) | 1.06 (0.80–1.40) |
| Patients matched by characteristics | n = 669 | n = 669 | n = 207 | n = 207 | ||
| Age, y | ||||||
| Median (IQR) | 72 (62–80) | 72 (62–80) | – | 72 (64–80) | 72 (64–80) | – |
| Sex, n (%) | ||||||
| Female | 259 (38.7) | 259 (38.7) | – | 84 (40.6) | 84 (40.6) | – |
| Male | 410 (61.3) | 410 (61.3) | – | 123 (59.4) | 123 (59.4) | – |
| Comorbidities | ||||||
| Cardiac disease | 148 (22.1) | 420 (62.8) | 0.17 (0.13- 0.21) | 46 (22.2) | 138 (66.7) | 0.14 (0.09–0.22) |
| Respiratory disease | 102 (15.2) | 143 (21.4) | 0.66 (0.50–0.88) | 34 (16.4) | 49 (23.7) | 0.63 (0.39–1.03) |
| Renal disease | 81 (12.1) | 41 (6.1) | 2.11 (1.43–3.12) | 28 (13.5) | 7 (3.4) | 4.47 (1.91–10.5) |
| Diabetes | 126 (18.8) | 145 (21.7) | 0.80 (0.62–1.05) | 45 (21.7) | 57 (27.5) | 0.73 (0.47–1.15) |
| Hypertension | 291 (43.5) | 391 (58.4) | 0.55 (0.44–0.68) | 84 (40.6) | 129 (62.3) | 0.41 (0.28–0.61) |
| Pharmacologic therapies for COVID-19 | ||||||
| (Hydroxy)chloroquine | 590 (88.2) | 567 (84.8) | 1.34 (0.98–1.84) | 0 | 0 | n/a |
| Azithromycin | 318 (47.5) | 343 (51.3) | 0.86 (0.69–1.07) | 27 (13.0) | 43 (20.8) | 0.57 (0.34–0.97) |
| Lopinavir/darunavir | 383 (57.2) | 424 (63.4) | 0.77 (0.62–0.96) | 0 | 0 | n/a |
| Remdesivir | 22 (3.3) | 3 (0.4) | 7.55 (2.25–25.3) | 53 (25.6) | 54 (26.1) | 0.98 (0.63–1.51) |
| Tocilizumab | 131 (19.6) | 44 (6.6) | 3.46 (2.41–4.96) | 41 (19.8) | 35 (16.9) | 1.21 (0.74–2.00) |
| Corticosteroids | 283 (42.3) | 172 (25.7) | 2.12 (1.68–2.67) | 191 (92.3) | 182 (87.9) | 1.64 (0.85–3.17) |
| Oxygen support during COVID-19 treatment | ||||||
| No or Low-flow oxygen support | 511 (76.4) | 575 (86.0) | reference | 107 (51.7) | 126 (60.9) | reference |
| High-flow oxygen support or mechanical ventilation | 158 (23.6) | 94 (14.0) | 1.89 (1.43–2.51) | 100 (48.3) | 81 (39.1) | 1.45 (0.98–2.15) |
| Inpatient 30-d mortality * | 216/669 (32.3) | 198/669 (29.6) | 1.13 (0.90–1.43) | 72/207 (34.8) | 26/207 (12.6) | 3.71 (2.25–6.13) |
| Patients with PCC Data, N = 278 * | Odds Ratio (95% CI) | ||||
|---|---|---|---|---|---|
| Total, N = 278 | PCC, n = 76 | No PCC, n = 202 | Unadjusted | Adjusted † | |
| Age, y | N = 276 | n = 200 | |||
| Median (IQR) | 67 (54.5–76) | 69 (54–76) | 67 (54.5–75) | n/a | n/a |
| Age 18–49 y, n (%) | 47 (17.0) | 11 (14.5) | 36 (18) | reference | reference |
| Age 50–79 y, n (%) | 191 (69.2) | 54 (71.1) | 142 (71.0) | ||
| Age ≥ 80 y, n (%) | 33 (12.0) | 11 (14.5) | 22 (11) | 1.64 (0.61–4.40) | 1.24 (0.42–3.69) |
| Sex, n (%) | N = 271 | n = 72 | n = 199 | ||
| Female | 149 (55.0) | 42 (58.3) | 107 (53.8) | reference | reference |
| Male | 122 (45.0) | 30 (41.7) | 92 (46.2) | 1.20 (0.70–2.08) | 1.20 (0.69–2.08) |
| Comorbidities | |||||
| Number of 6 specified comorbidities | |||||
| 0 | 78 (28.1) | 16 (21.1) | 62 (30.7) | reference | reference |
| ≥1 | 200 (71.9) | 60 (79.0) | 140 (69.3) | 1.66 (0.89–3.11) | 1.57 (0.78–3.16) |
| Other comorbidities | 144 (51.8) | 44 (57.9) | 100 (49.5) | 1.40 (0.82–2.39) | 1.36 (0.77–2.42) |
| Hematologic malignancy | |||||
| NHL | 83 (29.9) | 16 (21.1) | 67 (33.2) | reference | reference |
| MM | 66 (23.7) | 21 (27.6) | 45 (22.3) | 1.95 (0.92–4.15) | 1.86 (0.85–4.05) |
| CLL | 29 (10.4) | 10 (13.2) | 19 (9.4) | 2.20 (0.86–5.64) | 2.10 (0.81–5.44) |
| HL | 16 (5.8) | 4 (5.3) | 12 (5.9) | 1.40 (0.38–4.90) | 1.06 (0.25–4.41) |
| ALL | 3 (1.1) | 1 (1.3) | 2 (1) | 2.09 (0.18–24.5) | 2.16 (0.17–27.1) |
| MDS | 23 (8.3) | 6 (7.9) | 17 (8.4) | 1.48 (0.50–4.35) | 1.47 (0.48–4.47) |
| AML | 28 (10.1) | 8 (10.5) | 20 (9.9) | 1.68 (0.63–4.84) | 1.58 (0.58–4.30) |
| CML | 7 (2.5) | 1 (1.3) | 6 (3.0) | 0.70 (0.08–6.21) | 0.58 (0.06–5.31) |
| Ph-MPN | 23 (8.3) | 9 (11.8) | 14 (6.9) | 2.69 (0.99–7.31) | 2.02 (0.68–6.02) |
| Stem cell transplantation ‡ | N = 274 | n = 72 | |||
| No | 219 (79.9) | 59 (81.9) | 160 (79.2) | reference | reference |
| Autologous | 35 (12.8) | 7 (9.7) | 28 (13.9) | 0.68 (0.28–1.64) | 0.68 (0.25–1.84) |
| Allogeneic | 20 (7.3) | 6 (8.3) | 14 (6.9) | 2.16 (0.43–3.17) | 1.36 (0.46–4.05) |
| Cancer therapy, within 30 d § | N = 276 | ||||
| No active therapy | 105 (38.0) | 28 (36.8) | 77 (38.1) | reference | reference |
| Active therapy | 173 (62.0) | 48 (63.2) | 125 (61.9) | 1.06 (0.61–1.82) | 0.95 (0.54–1.67) |
| Conventional chemotherapy | 62 (22.5) | 17 (22.7) | 45 (22.4) | 1.04 (0.51–2.11) | 0.99 (0.47–2.08) |
| Low-intensity chemotherapy | 16 (5.8) | 5 (6.7) | 11 (5.5) | 1.25 (0.40–3.92) | 0.98 (0.28–3.50) |
| Molecular targeted therapy | 34 (12.3) | 11 (14.7) | 23 (11.4) | 1.32 (0.57–3.04) | 1.03 (0.42–2.56) |
| Immunotherapy, mAb only | 16 (5.8) | 2 (2.7) | 14 (7.0) | 0.39 (0.08–1.84) | 0.41 (0.09–1.99) |
| Immunomodulator drugs | 19 (6.9) | 4 (5.3) | 15 (7.5) | 0.73 (0.22–2.40) | 0.63 (0.19–2.11) |
| Hypomethylating agents | 16 (5.8) | 4 (5.3) | 12 (6.0) | 0.92 (0.27–3.08) | 0.76 (0.21–2.71) |
| Supportive therapy | 5 (1.8) | 2 (2.7) | 3 (1.5) | 1.83 (0.29–11.6) | 1.35 (0.20–9.02) |
| Time period of COVID-19 diagnosis | |||||
| Early cohort (1st wave, March–June 2020) | 209 (75.2) | 63 (82.9) | 146 (72.3) | reference | reference |
| Later cohort (2nd/3rd wave, July 2020–February 2021) | 69 (24.8) | 13 (17.1) | 56 (27.7) | 0.54 (0.28–1.05) | 0.60 (0.30–1.20) |
| Care setting of COVID-19 treatment | |||||
| Outpatient | 72 (25.9) | 11 (14.5) | 61 (30.2) | reference | reference |
| Inpatient | 206 (74.1) | 65 (85.5) | 141 (69.8) | 2.56 (1.26–5.18) | 2.37 (1.15–4.90) |
| Intensive care unit | 44/206 (21.4) | 17/65 (26.2) | 27/141 (19.1) | 1.50 (0.75–2.99) | 1.59 (0.75–3.31) |
| Pharmacologic therapies for COVID-19 | |||||
| (Hydroxy)chloroquine | 181 (65.1) | 58 (76.3) | 123 (60.9) | 2.07 (1.14–3.80) | 1.91 (1.03–3.53) |
| Azithromycin | 87 (31.3) | 26 (34.2) | 61 (30.2) | 1.20 (0.69–2.11) | 0.99 (0.54–1.80) |
| Lopinavir/darunavir | 132 (47.5) | 46 (60.5) | 86 (42.6) | 2.07 (1.21–3.54) | 2.03 (1.16–3.56) |
| Remdesivir | 31 (11.2) | 13 (17.1) | 18 (8.9) | 2.11 (0.98–4.55) | 2.26 (1.03–4.98) |
| Tocilizumab | 54 (19.4) | 21 (27.6) | 33 (16.3) | 1.96 (1.05–3.66) | 1.97 (1.03–3.77) |
| Corticosteroids | 138 (49.6) | 45 (59.2) | 93 (46.0) | 1.70 (1.00–2.90) | 1.68 (0.97–2.92) |
| Oxygen support during COVID-19 treatment | |||||
| No | 104 (37.4) | 24 (31.6) | 80 (39.6) | reference | reference |
| Low-flow oxygen support | 133 (47.8) | 36 (47.4) | 97 (48.0) | 1.24 (0.68–2.24) | 1.24 (0.66–2.35) |
| High-flow oxygen support or mechanical ventilation | 41 (14.7) | 16 (21.1) | 25 (12.4) | 2.13 (0.98–4.64) | 2.20 (0.98–4.94) |
| Clinical severity of COVID-19 | N = 273 | n = 75 | n = 198 | ||
| Mild | 69 (25.3) | 14 (18.7) | 55 (27.8) | reference | reference |
| Moderate | 89 (32.6) | 22 (29.3) | 67 (33.8) | 1.29 (0.60–2.76) | 1.48 (0.66–3.37) |
| Severe | 83 (30.4) | 24 (32.0) | 59 (29.8) | 1.60 (0.75–3.40) | 1.73 (0.77–3.90) |
| Critical | 32 (11.7) | 15 (20.0) | 17 (8.6) | 3.47 (1.40–8.60) | 3.60 (1.35–9.62) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-López, J.; De la Cruz, J.; Gil-Manso, R.; Alegre, A.; Ortiz, J.; Llamas, P.; Martínez, Y.; Hernández-Rivas, J.-Á.; González-Gascón, I.; Benavente, C.; et al. COVID-19 Severity and Survival over Time in Patients with Hematologic Malignancies: A Population-Based Registry Study. Cancers 2023, 15, 1497. https://doi.org/10.3390/cancers15051497
Martínez-López J, De la Cruz J, Gil-Manso R, Alegre A, Ortiz J, Llamas P, Martínez Y, Hernández-Rivas J-Á, González-Gascón I, Benavente C, et al. COVID-19 Severity and Survival over Time in Patients with Hematologic Malignancies: A Population-Based Registry Study. Cancers. 2023; 15(5):1497. https://doi.org/10.3390/cancers15051497
Chicago/Turabian StyleMartínez-López, Joaquín, Javier De la Cruz, Rodrigo Gil-Manso, Adrián Alegre, Javier Ortiz, Pilar Llamas, Yolanda Martínez, José-Ángel Hernández-Rivas, Isabel González-Gascón, Celina Benavente, and et al. 2023. "COVID-19 Severity and Survival over Time in Patients with Hematologic Malignancies: A Population-Based Registry Study" Cancers 15, no. 5: 1497. https://doi.org/10.3390/cancers15051497