
The Impact of Prior Mammograms on the Diagnostic Performance of Radiologists in Early Breast Cancer Detection: A Focus on Breast Density, Lesion Features and Vendors Using Wholly Digital Screening Cases
 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Background
2. Methods
2.1. Oversight
2.2. Study Population
2.3. Mammogram Collection
2.4. Mammogram Display and Reading Environments
2.5. Mammogram Reading Procedure
2.6. Statistical Analysis
3. Results
3.1. Radiologists’ Performances among Cases without Prior, with Prior Images from Same Vendor and Different Vendor in Cancer-Enriched Test Sets
3.2. Comparison of Odds Ratio of True Positive and True Negative for Three Groups of Cases
3.3. Comparison of Odds Ratio of True Cancer Lesion Location for Three Groups of Cases
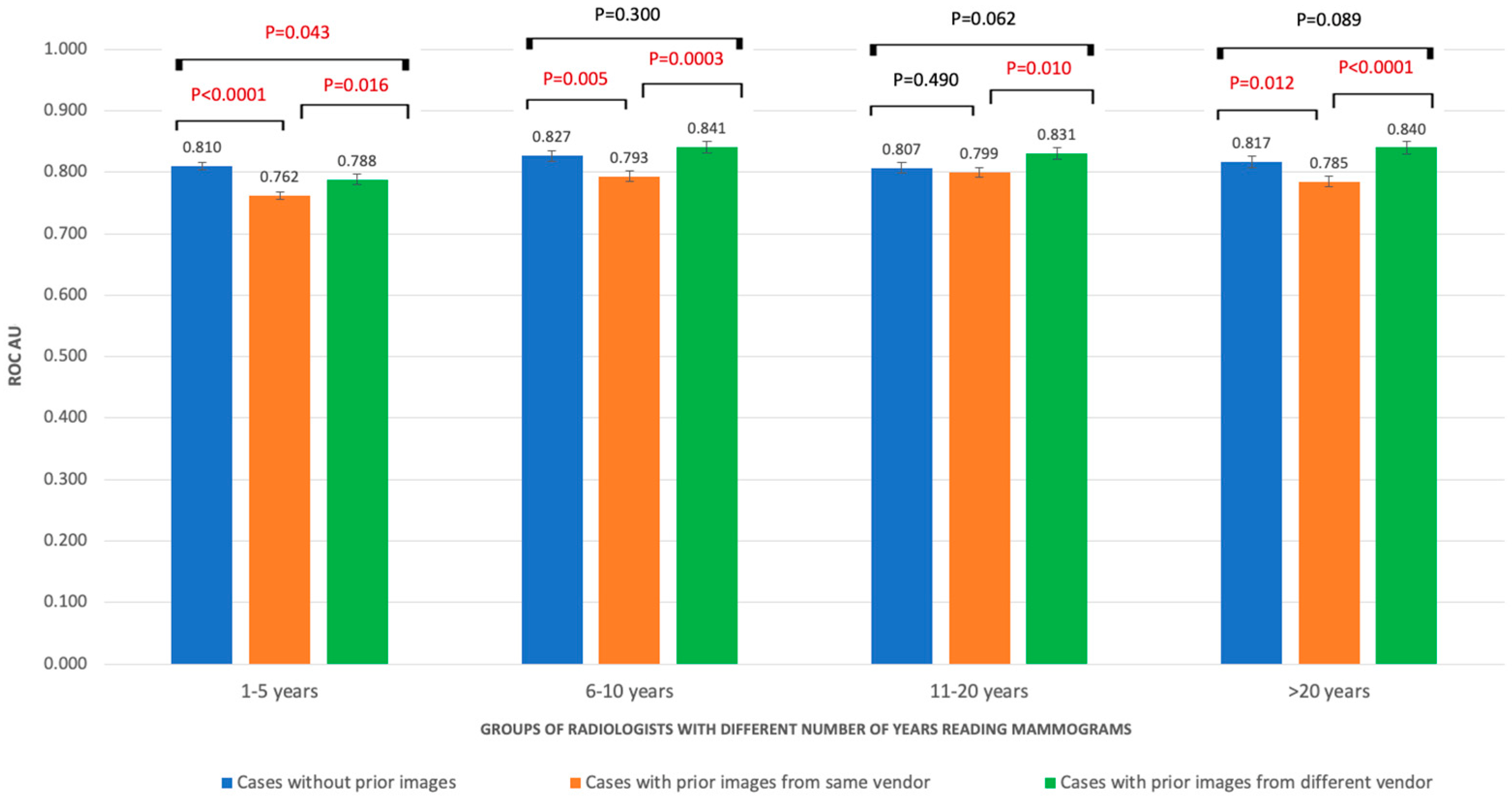
3.4. Performances of Radiologists with Different Levels of Working Experience
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kemp Jacobsen, K.; O’Meara, E.S.; Key, D.; SM Buist, D.; Kerlikowske, K.; Vejborg, I.; Sprague, B.L.; Lynge, E.; von Euler-Chelpin, M. Comparing sensitivity and specificity of screening mammography in the United States and Denmark. Int. J. Cancer 2015, 137, 2198–2207. [Google Scholar] [CrossRef] [PubMed]
- BreastScreenAustraliaNationalAccreditationStandards. BreastScreen Australia Quality Improvement Program. 2008. Available online: https://wiki.cancer.org.au/policy/Citation:BreastScreen_Australia_2008 (accessed on 15 June 2022).
- Rawashdeh, M.A.; Lee, W.B.; Bourne, R.M.; Ryan, E.A.; Pietrzyk, M.W.; Reed, W.M.; Heard, R.C.; Black, D.A.; Brennan, P.C. Markers of good performance in mammography depend on number of annual readings. Radiology 2013, 269, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Boyd, N.F.; Guo, H.; Martin, L.J.; Sun, L.; Stone, J.; Fishell, E.; Jong, R.A.; Hislop, G.; Chiarelli, A.; Minkin, S.; et al. Mammographic density and the risk and detection of breast cancer. N. Engl. J. Med. 2007, 356, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Frankel, S.D.; Sickles, E.A.; Curpen, B.N.; Sollitto, R.A.; Ominsky, S.H.; Galvin, H.B. Initial versus subsequent screening mammography: Comparison of findings and their prognostic significance. AJR Am. J. Roentgenol. 1995, 164, 1107–1109. [Google Scholar] [CrossRef] [PubMed]
- Thurfjell, M.G.; Vitak, B.; Azavedo, E.; Svane, G.; Thurfjell, E. Effect on sensitivity and specificity of mammography screening with or without comparison of old mammograms. Acta Radiol. 2000, 41, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Richard, C.; Gilmore, P.C.; Sarah, Z.; Lisa, K.J. Screening for Breast Cancer. In Current Surgical Therapy, 13th ed.; Cameron, J.L., Cameron, A.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 660–666. [Google Scholar]
- Hambly, N.M.; McNicholas, M.M.; Phelan, N.; Hargaden, G.C.; O’Doherty, A.; Flanagan, F.L. Comparison of digital mammography and screen-film mammography in breast cancer screening: A review in the Irish breast screening program. AJR Am. J. Roentgenol. 2009, 193, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Rawashdeh, M.L.W.; Pietrzyk, M.; Ryan, E.; Brennan, P. Experience with soft copy reading may lower specificity in mammography. In Proceedings of the ASMMIRT, 9th Annual Scientific Meeting of Medical Imaging and Radiation Therapy, Sydney, Australia, 9 July 2017. [Google Scholar]
- Brennan, P.C.; Trieu, P.D.; Tapia, K.; Ryan, J.; Mello-Thoms, C.; Lee, W. BREAST: A Novel Strategy to Improve the Detection of Breast Cancer. In Lecture Notes in Computer Science—The 12th International Workshop on Breast Imaging; Fujita, H., Chisako Muramatsu, T.H., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; Volume 8539, pp. 438–443. [Google Scholar]
- Trieu, P.D.Y.; Tapia, K.; Frazer, H.; Lee, W.; Brennan, P. Improvement of Cancer Detection on Mammograms via BREAST Test Sets. Acad. Radiol. 2019, 26, e341–e347. [Google Scholar] [CrossRef] [PubMed]
- Trieu, P.D.Y.; Lewis, S.J.; Li, T.; Ho, K.; Wong, D.J.; Tran, O.T.M.; Puslednik, L.; Black, D.; Brennan, P.C. Improving radiologist’s ability in identifying particular abnormal lesions on mammograms through training test set with immediate feedback. Sci. Rep. 2021, 11, 9899. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Burnside, E.S.; Sickles, E.A.; Sohlich, R.E.; Dee, K.E. Differential value of comparison with previous examinations in diagnostic versus screening mammography. AJR Am. J. Roentgenol. 2002, 179, 1173–1177. [Google Scholar] [CrossRef] [PubMed]
- Roelofs, A.A.; Karssemeijer, N.; Wedekind, N.; Beck, C.; van Woudenberg, S.; Snoeren, P.R.; Hendriks, J.H.; Rosselli del Turco, M.; Bjurstam, N.; Junkermann, H.; et al. Importance of comparison of current and prior mammograms in breast cancer screening. Radiology 2007, 242, 70–77. [Google Scholar] [CrossRef] [PubMed]
- AIHW (Ed.) BreastScreen Australia Monitoring Report 2021; Australian Government: Canberra, Australia, 2021. [Google Scholar] [CrossRef]
- Berlin, L. Malpractice issues in radiology. Alliterative errors. AJR Am. J. Roentgenol. 2000, 174, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Waite, S.; Scott, J.; Gale, B.; Fuchs, T.; Kolla, S.; Reede, D. Interpretive Error in Radiology. AJR Am. J. Roentgenol. 2017, 208, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Breastscreen_Australia. Breastscreen National Accreditation Standards; Department of Health: Canberra, Australia, 2019. [Google Scholar]
- Kan, L.; Olivotto, I.A.; Warren Burhenne, L.J.; Sickles, E.A.; Coldman, A.J. Standardized abnormal interpretation and cancer detection ratios to assess reading volume and reader performance in a breast screening program. Radiology 2000, 215, 563–567. [Google Scholar] [CrossRef] [PubMed]
- NHS Breast Screening Radiologists Quality Assurance Committee. Quality Assurance Guidelines for Radiologists; NHSBSP Publications: Sheffield, UK, 1997. [Google Scholar]
- Reed, W.M.; Lee, W.B.; Cawson, J.N.; Brennan, P.C. Malignancy detection in digital mammograms: Important reader characteristics and required case numbers. Acad. Radiol. 2010, 17, 1409–1413. [Google Scholar] [CrossRef] [PubMed]
- Hayward, J.H.; Ray, K.M.; Wisner, D.J.; Kornak, J.; Lin, W.; Joe, B.N.; Sickles, E.A. Improving Screening Mammography Outcomes Through Comparison with Multiple Prior Mammograms. AJR Am. J. Roentgenol. 2016, 207, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Soh, B.P.; Lee, W.; McEntee, M.F.; Kench, P.L.; Reed, W.M.; Heard, R.; Chakraborty, D.P.; Brennan, P.C. Screening mammography: Test set data can reasonably describe actual clinical reporting. Radiology 2013, 268, 46–53. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Categories | Number of Readers (%) | |
|---|---|---|
| Number of mammograms read per week | <20 | 185 (30.2%) |
| 20–60 | 112 (18.3%) | |
| 61–100 | 73 (11.9%) | |
| 101–150 | 84 (13.7%) | |
| 151–200 | 90 (14.7%) | |
| >200 | 68 (11.2%) | |
| Number of years reading mammograms | ≤5 | 168 (27.5%) |
| 6–10 | 181 (29.6%) | |
| 11–15 | 72 (11.8%) | |
| 16–20 | 71 (11.6%) | |
| >20 | 120 (19.5%) | |
| Cases with No Prior Images | Cases with Prior Images from Same Vendor | Cases with Prior Images from Different Vendor | Total Cases (%) | ||
|---|---|---|---|---|---|
| Normal cases | Breast density A | 7 | 15 | 16 | 38 (10.5%) |
| Breast density B | 38 | 73 | 33 | 144 (39.9%) | |
| Breast density C | 44 | 65 | 26 | 135 (37.4%) | |
| Breast density D | 14 | 23 | 7 | 44 (12.2%) | |
| Total | 103 | 176 | 82 | 361 | |
| Cancer cases | Breast density A | 4 | 9 | 5 | 18 (10.1%) |
| Breast density B | 21 | 33 | 22 | 76 (42.5%) | |
| Breast density C | 30 | 19 | 17 | 66 (36.9%) | |
| Breast density D | 8 | 8 | 3 | 19 (10.6%) | |
| Total | 63 | 69 | 47 | 179 | |
| Lesion types | Architectural distortion | 6 | 4 | 5 | 15 (8.4%) |
| Asymmetric density | 7 | 7 | 7 | 21 (11.7%) | |
| Calcifications | 12 | 10 | 8 | 30 (16.8%) | |
| Discrete mass | 10 | 11 | 13 | 34 (19%) | |
| Stellate/Spiculated mass | 18 | 22 | 13 | 53 (29.6%) | |
| Mix of types | 9 | 14 | 3 | 26 (14.5%) | |
| Total | 49 | 57 | 37 | 143 | |
| Lesion sizes | ≤10 mm | 35 | 35 | 27 | 97 (54.2%) |
| >10 mm | 28 | 34 | 20 | 82 (45.8%) | |
| Total | 63 | 69 | 47 | 179 |
| NP vs. SP | DP vs. SP | NP vs. DP | ||
|---|---|---|---|---|
| All cases | Recall rate | 0.444–0.353 | 0.461–0.353 | 0.444–0.461 |
| True positive rate | 0.803–0.712 | 0.785–0.712 | 0.803–0.785 | |
| True negative rate | 0.749–0.787 | 0.771–0.787 | 0.749–0.771 | |
| ROC AUC | 0.814–0.782; p < 0.0001 * | 0.82–0.782; p < 0.0001 * | 0.814–0.82; p = 0.349 | |
| Cases with low breast density (A–B) | Recall rate | 0.430–0.365 | 0.436–0.365 | 0.430–0.436 |
| True positive rate | 0.806–0.733 | 0.768–0.733 | 0.806–0.768 | |
| True negative rate | 0.754–0.806 | 0.779–0.806 | 0.754–0.779 | |
| ROC AUC | 0.819–0.800; p = 0.0172 * | 0.819–0.800; p = 0.0207 * | 0.819–0.819; p = 0.97 | |
| Cases with high breast density (C–D) | Recall rate | 0.454–0.340 | 0.491–0.340 | 0.454–0.491 |
| True positive rate | 0.800–0.683 | 0.803–0.683 | 0.800–0.803 | |
| True negative rate | 0.746–0.769 | 0.761–0.769 | 0.746–0.761 | |
| ROC AUC | 0.810–0.759; p < 0.0001 * | 0.818–0.759; p < 0.0001 * | 0.810–0.818; p = 0.364 |
| Comparison | OR (95% CI) | p-Value | ||
|---|---|---|---|---|
| True positive | NP vs. SP | 1.643 (1.489–1.812) | <0.0001 * | |
| All cases | DP vs. SP | 1.478 (1.33–1.643) | <0.0001 * | |
| NP vs. DP | 1.111 (0.991–1.246) | 0.07 | ||
| NP vs. SP | 1.517 (1.306–1.762) | <0.0001 * | ||
| Cases with low breast density (A–B) | DP vs. SP | 1.205 (1.043–1.393) | 0.011 * | |
| NP vs. DP | 1.259 (1.06–1.494) | 0.008 * | ||
| NP vs. SP | 1.859 (1.626–2.126) | <0.0001 * | ||
| Cases with high breast density (C–D) | DP vs. SP | 1.884 (1.613–2.202) | <0.0001 * | |
| NP vs. DP | 0.987 (0.843–1.154) | 0.866 | ||
| True negative | NP vs. SP | 0.808 (0.756–0.864) | <0.0001 * | |
| All cases | DP vs. SP | 0.909 (0.837–0.987) | 0.023 * | |
| NP vs. DP | 0.889 (0.815–0.971) | 0.008 * | ||
| NP vs. SP | 0.736 (0.665–0.815) | <0.0001 * | ||
| Cases with low breast density (A–B) | DP vs. SP | 0.844 (0.752–0.948) | 0.004 * | |
| NP vs. DP | 0.872 (0.769–0.988) | 0.031 * | ||
| NP vs. SP | 0.884 (0.808–0.966) | 0.006 | ||
| Cases with high breast density (C–D) | DP vs. SP | 0.958 (0.85–1.079) | 0.481 | |
| NP vs. DP | 0.922 (0.815–1.044) | 0.199 |
| Lesion Characteristics | Comparison | OR (95% CI) | p-Value |
|---|---|---|---|
| Architectural distortion | NP vs. SP | 1.746 (1.313–2.322) | <0.0001 * |
| DP vs. SP | 3.232 (2.37–4.408) | <0.0001 * | |
| NP vs. DP | 0.54 (0.417–0.7) | <0.0001 * | |
| Calcification | NP vs. SP | 1.158 (0.942–1.423) | 0.163 |
| DP vs. SP | 2.854 (2.223–3.664) | <0.0001 * | |
| NP vs. DP | 0.406 (0.317–0.52) | <0.0001 * | |
| Discrete mass | NP vs. SP | 1.343 (1.073–1.68) | 0.01 * |
| DP vs. SP | 1.016 (0.813–1.27) | 0.89 | |
| NP vs. DP | 1.322 (1.038–1.683) | 0.023 * | |
| Asymmetric density | NP vs. SP | 1.03 (0.819–1.297) | 0.798 |
| DP vs. SP | 1.187 (0.922–1.527) | 0.183 | |
| NP vs. DP | 0.868 (0.68–1.109) | 0.257 | |
| Stellate/Spiculated mass | NP vs. SP | 1.984 (1.671–2.355) | <0.0001 * |
| DP vs. SP | 1.297 (1.09–1.544) | 0.003 * | |
| NP vs. DP | 1.529 (1.257–1.861) | <0.0001 * | |
| Lesion ≤ 10 mm | NP vs. SP | 1.115 (1.011–1.23) | 0.029 * |
| DP vs. SP | 1.18 (1.058–1.316) | 0.003 * | |
| NP vs. DP | 0.945 (0.846–1.056) | 0.317 | |
| Lesion > 10 mm | NP vs. SP | 1.254 (1.04–1.512) | 0.018 * |
| DP vs. SP | 1.748 (1.498–2.041) | <0.0001 * | |
| NP vs. DP | 0.564 (0.448–0.711) | <0.0001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trieu, P.D.; Borecky, N.; Li, T.; Brennan, P.C.; Barron, M.L.; Lewis, S.J. The Impact of Prior Mammograms on the Diagnostic Performance of Radiologists in Early Breast Cancer Detection: A Focus on Breast Density, Lesion Features and Vendors Using Wholly Digital Screening Cases. Cancers 2023, 15, 1339. https://doi.org/10.3390/cancers15041339
Trieu PD, Borecky N, Li T, Brennan PC, Barron ML, Lewis SJ. The Impact of Prior Mammograms on the Diagnostic Performance of Radiologists in Early Breast Cancer Detection: A Focus on Breast Density, Lesion Features and Vendors Using Wholly Digital Screening Cases. Cancers. 2023; 15(4):1339. https://doi.org/10.3390/cancers15041339
Chicago/Turabian StyleTrieu, Phuong Dung (Yun), Natacha Borecky, Tong Li, Patrick C. Brennan, Melissa L. Barron, and Sarah J. Lewis. 2023. "The Impact of Prior Mammograms on the Diagnostic Performance of Radiologists in Early Breast Cancer Detection: A Focus on Breast Density, Lesion Features and Vendors Using Wholly Digital Screening Cases" Cancers 15, no. 4: 1339. https://doi.org/10.3390/cancers15041339