

Increased Early Cancer Diagnosis: Unveiling Immune-Cancer Biology to Explain Clinical “Overdiagnosis”

{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Overdiagnosis and Pathology Classification
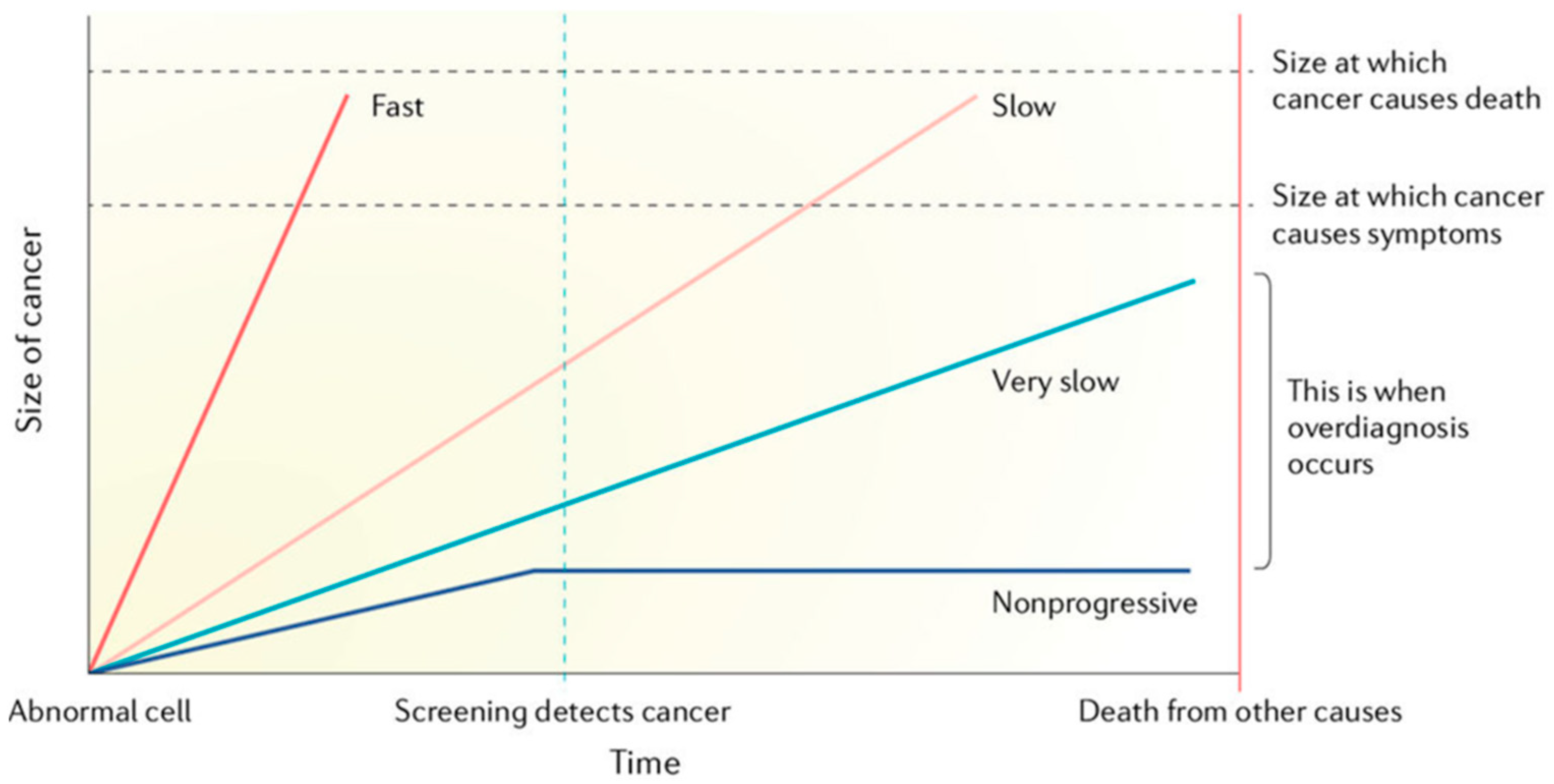
3. Overdiagnosis and Cell Growth Rates
4. Reflecting on Excess- or Overdiagnosis
5. Cancer and the Immune Dynamic
- Filtering entry. This is at points of entry to the body.
- Filtering presence. This process of filtering occurs by monitoring the rate of change. This has been historically called ‘immunosurveillance’.
- Promotion of cooperation between the body elements.

- Increased diagnosis rates
- Increased in situ/invasive ratios
- Increased claims of overdiagnosis
6. A Model for Overdiagnosis and the Immune System through Melanoma
- (1)
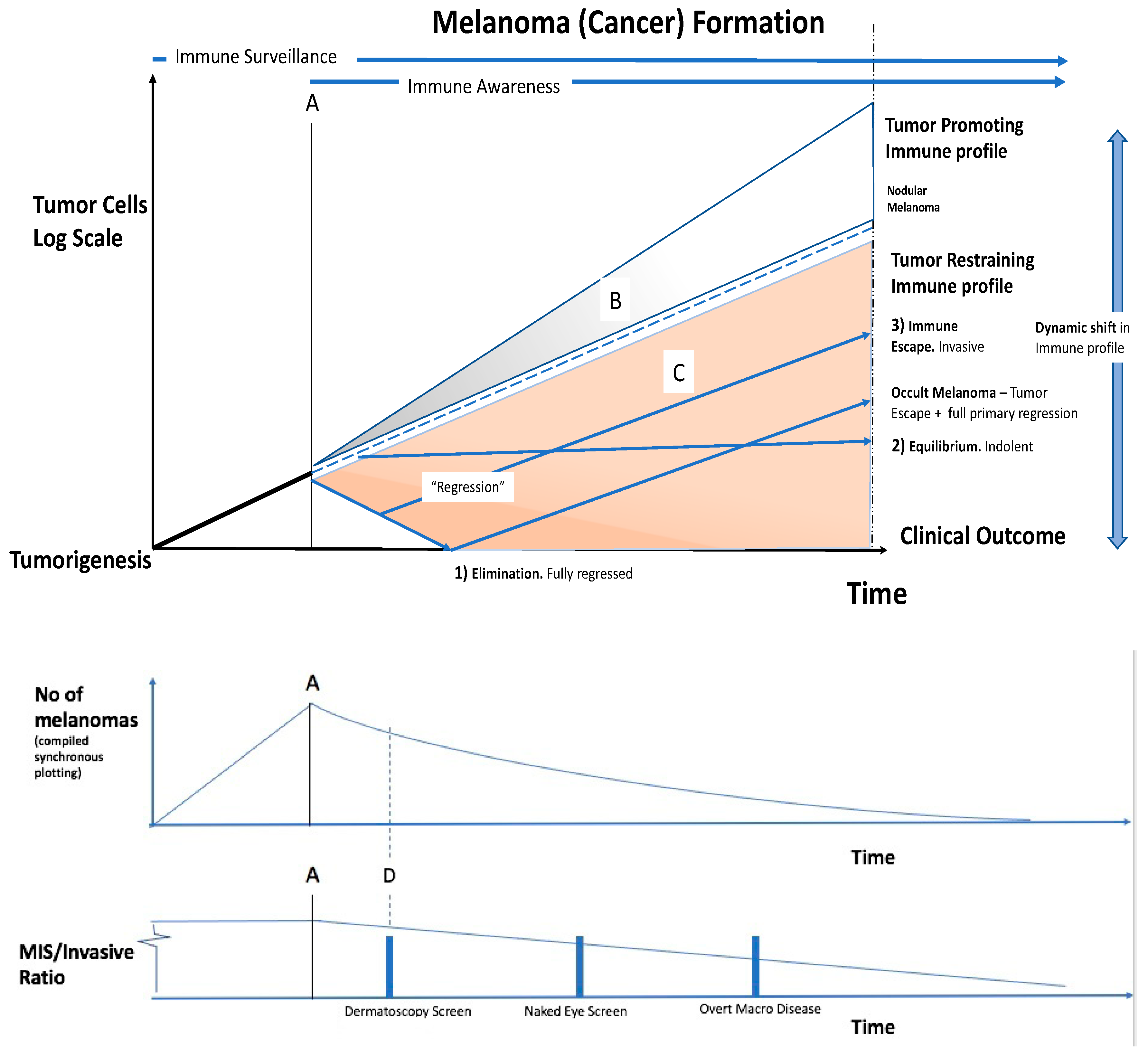
- Elimination of the tumour: Immune ‘regression’ associated with lymphocytes may remove all histopathological evidence of melanoma. Clinically this is seen as spontaneous regression, or primary regressing/regressed melanoma.
- (2)
- Equilibrium: The immune system has not removed the tumour, but has restrained it. The tumour and the immune system may reach a steady state. Clinically, this is found in the post-mortem data of people dying with, but not from, cancers. This may be much of the reservoir in overdiagnosis.The cancer is evolving, and the immune profile is dynamic, thus this situation can shift. The immune system can overcome the tumour causing regression and elimination. Conversely, the tumour may overcome the immune restraint, and ‘escape’.
- (3)
- Immune escape: The cancer may initially be restrained by the immune system, but then overcome it. If the immune system eliminates the primary tumour after metastases are released, metastatic secondaries with no known primary occurs. Clinically, this is known as ‘occult melanoma or ‘melanoma of unknown primary origin’ which occurs in about 3% (range 1.2–31%) of advanced melanomas [39]. This also occurs in some other cancer types.
- A higher Melanoma detection rate and an even larger increase in the detection rate of in situ melanomas than would otherwise be present in a population-based cancer registry. This gives,
- An increased MIS/Invasive ratio. The raised melanoma and in situ detection despite no reduction in mortality, to give;
- Relative overdiagnosis.
7. Discussion
- Which cancers will (or will not) progress and become clinically significant?
- Which cancers will translate through to metastasis and mortality?
- Which immune profiles are operating on a tumour and at what time?
- How might we alter immune profiles in a clinically useful way?
8. Conclusions
- Cancer overdiagnosis with screening may also have an immune basis; this is supported by accumulating evidence.
- Cellular/immune profiling is currently lacking to identify which lesions will be held in check by immunological defence, or will be eliminated, or progress to metastasis.
- There are no current available clinical or pathology-based means of quantifying the immune—tumour interaction when deciding on need for treatment.
- The immune—tumour interaction should be an important focus of increased research to better understand and improve cancer control. Skin, being an external organ, is ideally accessible for this research pursuit.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Welch, H.G.; Black, W.C. Overdiagnosis in cancer. J. Natl. Cancer Inst. 2010, 102, 605–613. [Google Scholar] [CrossRef]
- Srivastava, S.; Reid, B.J.; Ghosh, S.; Kramer, B.S. Research Needs for Understanding the Biology of Overdiagnosis in Cancer Screening. J. Cell. Physiol. 2015, 231, 1870–1875. [Google Scholar] [CrossRef]
- Srivastava, S.; Koay, E.J.; Borowsky, A.D.; De Marzo, A.M.; Ghosh, S.; Wagner, P.D.; Kramer, B.S. Cancer overdiagnosis: A biological challenge and clinical dilemma. Nat. Rev. Cancer 2019, 19, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Whiteman, D.C.; Olsen, C.M.; MacGregor, S.; Law, M.H.; Thompson, B.; Dusingize, J.C.; Green, A.C.; Neale, R.E.; Pandeya, N.; for the QSkin Study. The effect of screening on melanoma incidence and biopsy rates. Br. J. Dermatol. 2022, 187, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.S.; Kim, H.J.; Welch, H.G. Korea’s thyroid-cancer “epidemic”–screening and overdiagnosis. N. Engl. J. Med. 2014, 371, 1765–1767. [Google Scholar] [CrossRef] [PubMed]
- Oke, J.L.; O’Sullivan, J.W.; Perera, R.; Nicholson, B.D. The mapping of cancer incidence and mortality trends in the UK from 1980–2013 reveals a potential for overdiagnosis. Sci. Rep. 2018, 8, 14663. [Google Scholar] [CrossRef] [PubMed]
- Welch, H.G.; Mazer, B.L.; Adamson, A.S. The Rapid Rise in Cutaneous Melanoma Diagnoses. N. Engl. J. Med. 2021, 384, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Burton, R.C.; Armstrong, B.K. Non-metastasizing melanoma? J. Surg. Oncol. 1998, 67, 73–76. [Google Scholar] [CrossRef]
- Burton, R.C.; Armstrong, B.K. Current melanoma epidemic: A nonmetastasizing form of melanoma? World J. Surg. 1995, 19, 330–333. [Google Scholar] [CrossRef]
- Burton, R.C.; Armstrong, B.K. Recent incidence trends imply a nonmetastasizing form of invasive melanoma. Melanoma Res. 1994, 4, 107–113. [Google Scholar] [CrossRef]
- Burton, R.C.; Coates, M.S.; Hersey, P.; Roberts, G.; Chetty, M.P.; Chen, S.; Hayes, M.H.; Howe, C.G.; Armstrong, B.K. An analysis of a melanoma epidemic. Int. J. Cancer 1993, 55, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Frangos, J.E.; Duncan, L.M.; Piris, A.; Nazarian, R.M.; Mihm, M.C.; Hoang, M.P.; Gleason, B.; Flotte, T.J.; Byers, H.R.; Barnhill, R.L.; et al. Increased diagnosis of thin superficial spreading melanomas: A 20-year study. J. Am. Acad. Dermatol. 2011, 67, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Glasziou, P.P.; A Jones, M.; Pathirana, T.; Barratt, A.L.; Bell, K.J. Estimating the magnitude of cancer overdiagnosis in Australia. Med. J. Aust. 2019, 212, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Nikiforov, Y.E.; Seethala, R.R.; Tallini, G.; Baloch, Z.W.; Basolo, F.; Thompson, L.D.R.; Barletta, J.A.; Wenig, B.M.; Ghuzlan, A.A.; Kakudo, K.; et al. Nomenclature Revision for Encapsulated Follicular Variant of Papillary Thyroid Carcinoma: A Paradigm Shift to Reduce Overtreatment of Indolent Tumors. JAMA Oncol. 2016, 2, 1023–1029. [Google Scholar] [CrossRef]
- Cardozo, J.M.N.L.; Drukker, C.A.; Rutgers, E.J.T.; Schmidt, M.K.; Glas, A.M.; Witteveen, A.; Cardoso, F.; Piccart, M.; Esserman, L.J.; Poncet, C.; et al. Outcome of Patients With an Ultralow-Risk 70-Gene Signature in the MINDACT Trial. J. Clin. Oncol. 2022, 40, 1335–1345. [Google Scholar] [CrossRef]
- Johansson, A.; Yu, N.Y.; Iftimi, A.; Tobin, N.P.; van’t Veer, L.; Nordenskjöld, B.; Benz, C.C.; Fornander, T.; Perez-Tenorio, G.; Stål, O.; et al. Clinical and molecular characteristics of estrogen receptor-positive ultralow risk breast cancer tumors identified by the 70-gene signature. Int. J. Cancer 2022, 150, 2072–2082. [Google Scholar] [CrossRef]
- Esserman, L.J.; Yau, C.; Thompson, C.K.; van’t Veer, L.J.; Borowsky, A.D.; Hoadley, K.; Tobin, N.P.; Nordenskjöld, B.; Fornander, T.; Stål, O.; et al. Use of Molecular Tools to Identify Patients with Indolent Breast Cancers with Ultralow Risk Over 2 Decades. JAMA Oncol. 2017, 3, 1503–1510. [Google Scholar] [CrossRef]
- Lindelöf, B.; Sigurgeirsson, B.; Gäbel, H.; Stern, R.S. Incidence of skin cancer in 5356 patients following organ transplantation. Br. J. Dermatol. 2000, 143, 513–519. [Google Scholar]
- Vajdic, C.M.S.; McCredie, M. Cancer incidence before and after kidney transplantation. JAMA 2006, 296, 2823–2831. [Google Scholar] [CrossRef]
- Serraino, D.; Piselli, P.; Busnach, G.; Burra, P.; Citterio, F.; Arbustini, E.; Baccarani, U.; De Juli, E.; Pozzetto, U.; Bellelli, S.; et al. Risk of cancer following immunosuppression in organ transplant recipients and in HIV-positive individuals in southern Europe. Eur. J. Cancer 2007, 43, 2117–2123. [Google Scholar] [CrossRef]
- Hoshida, Y.; Tsukuma, H.; Yasunaga, Y.; Xu, N.; Fujita, M.Q.; Satoh, T.; Ichikawa, Y.; Kurihara, K.; Imanishi, M.; Matsuno, T.; et al. Cancer risk after renal transplantation in Japan. Int. J. Cancer 1997, 71, 517–520. [Google Scholar] [CrossRef]
- Seidel, J.; Otsuka, A.; Kabashima, K. Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Pradeu, T. Philosophy of Immunology; Cambridge University Press (CUP): Cambridge, UK, 2019. [Google Scholar]
- Cann, S.H.; van Netten, J.; van Netten, C.; Glover, D. Spontaneous regression: A hidden treasure buried in time. Med. Hypotheses 2002, 58, 115–119. [Google Scholar] [CrossRef] [PubMed]
- de Visser, K.E.; Eichten, A.; Coussens, L.M. Paradoxical roles of the immune system during cancer development. Nat. Rev. Cancer 2006, 6, 24–37. [Google Scholar] [CrossRef]
- Chen, R.; Gong, Y.; Zou, D.; Wang, L.; Yuan, L.; Zhou, Q. Correlation between subsets of tumor-infiltrating immune cells and risk stratification in patients with cervical cancer. Peerj 2019, 7, e7804. [Google Scholar] [CrossRef]
- Kunimasa, K.; Goto, T. Immunosurveillance and Immunoediting of Lung Cancer: Current Perspectives and Challenges. Int. J. Mol. Sci. 2020, 21, 597. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.F.; Cui, J.W. The Role of Tumor-Infiltrating B Cells in Tumor Immunity. J. Oncol. 2019, 2019, 2592419. [Google Scholar] [CrossRef]
- Wang, S.-S.; Liu, W.; Ly, D.; Xu, H.; Qu, L.; Zhang, L. Tumor-infiltrating B cells: Their role and application in anti-tumor immunity in lung cancer. Cell. Mol. Immunol. 2018, 16, 6–18. [Google Scholar] [CrossRef]
- Li, L.; Ouyang, Y.; Wang, W.; Hou, D.; Zhu, Y. The landscape and prognostic value of tumor-infiltrating immune cells in gastric cancer. Peerj 2019, 7, e7993. [Google Scholar] [CrossRef]
- Wu, M.; Mei, F.; Liu, W.; Jiang, J. Comprehensive characterization of tumor infiltrating natural killer cells and clinical significance in hepatocellular carcinoma based on gene expression profiles. Biomed. Pharmacother. 2019, 121, 109637. [Google Scholar] [CrossRef]
- Germann, M.; Zangger, N.; Sauvain, M.O.; Sempoux, C.; Bowler, A.D.; Wirapati, P.; Kandalaft, L.E.; Delorenzi, M.; Tejpar, S.; Coukos, G.; et al. Neutrophils suppress tumor-infiltrating T cells in colon cancer via matrix metalloproteinase-mediated activation of TGF β. EMBO Mol. Med. 2020, 12, e10681. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.-C.; Hu, Z.-Q.; Long, J.-H.; Zhu, G.-M.; Wang, Y.; Jia, Y.; Zhou, J.; Ouyang, Y.; Zeng, Z. Clinical Implications of Tumor-Infiltrating Immune Cells in Breast Cancer. J. Cancer 2019, 10, 6175–6184. [Google Scholar] [CrossRef]
- Ye, L.; Zhang, T.; Kang, Z.; Guo, G.; Sun, Y.; Lin, K.; Huang, Q.; Shi, X.; Ni, Z.; Ding, N.; et al. Tumor-Infiltrating Immune Cells Act as a Marker for Prognosis in Colorectal Cancer. Front. Immunol. 2019, 10, 2368. [Google Scholar] [CrossRef] [PubMed]
- Barry, K.C.; Hsu, J.; Broz, M.L.; Cueto, F.J.; Binnewies, M.; Combes, A.J.; Nelson, A.E.; Loo, K.; Kumar, R.; Rosenblum, M.D.; et al. A natural killer–dendritic cell axis defines checkpoint therapy–responsive tumor microenvironments. Nat. Med. 2018, 24, 1178–1191. [Google Scholar] [CrossRef] [PubMed]
- Binnewies, M.; Roberts, E.W.; Kersten, K.; Chan, V.; Fearon, D.F.; Merad, M.; Coussens, L.M.; Gabrilovich, D.I.; Ostrand-Rosenberg, S.; Hedrick, C.C.; et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat. Med. 2018, 24, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Senovilla, L.; Vacchelli, E.; Galon, J.; Adjemian, S.; Eggermont, A.; Fridman, W.H.; Sautès-Fridman, C.; Ma, Y.; Tartour, E.; Zitvogel, L.; et al. Trial watch: Prognostic and predictive value of the immune infiltrate in cancer. Oncoimmunology 2012, 1, 1323–1343. [Google Scholar] [CrossRef] [PubMed]
- Coventry, B.J.; Henneberg, M. The Immune System and Responses to Cancer: Coordinated Evolution. F1000Reserch 2015, 4, 552. [Google Scholar] [CrossRef]
- Kamposioras, K.; Pentheroudakis, G.; Pectasides, D.; Pavlidis, N. Malignant melanoma of unknown primary site. To make the long story short. A systematic review of the literature. Crit. Rev. Oncol. 2011, 78, 112–126. [Google Scholar] [CrossRef]
- Guitera, P.; Menzies, S.W.; Coates, E.; Azzi, A.; Fernandez-Penas, P.; Lilleyman, A.; Badcock, C.; Schmid, H.; Watts, C.G.; Collgros, H.; et al. Efficiency of Detecting New Primary Melanoma Among Individuals Treated in a High-risk Clinic for Skin Surveillance. JAMA Dermatol. 2021, 157, 521. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wauchope, B.A.; Coventry, B.J.; Roder, D.M. Increased Early Cancer Diagnosis: Unveiling Immune-Cancer Biology to Explain Clinical “Overdiagnosis”. Cancers 2023, 15, 1139. https://doi.org/10.3390/cancers15041139
Wauchope BA, Coventry BJ, Roder DM. Increased Early Cancer Diagnosis: Unveiling Immune-Cancer Biology to Explain Clinical “Overdiagnosis”. Cancers. 2023; 15(4):1139. https://doi.org/10.3390/cancers15041139
Chicago/Turabian StyleWauchope, Bruce A., Brendon J. Coventry, and David M. Roder. 2023. "Increased Early Cancer Diagnosis: Unveiling Immune-Cancer Biology to Explain Clinical “Overdiagnosis”" Cancers 15, no. 4: 1139. https://doi.org/10.3390/cancers15041139