
Real-World Data Validation of NAPOLI-1 Nomogram for the Prediction of Overall Survival in Metastatic Pancreatic Cancer
 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
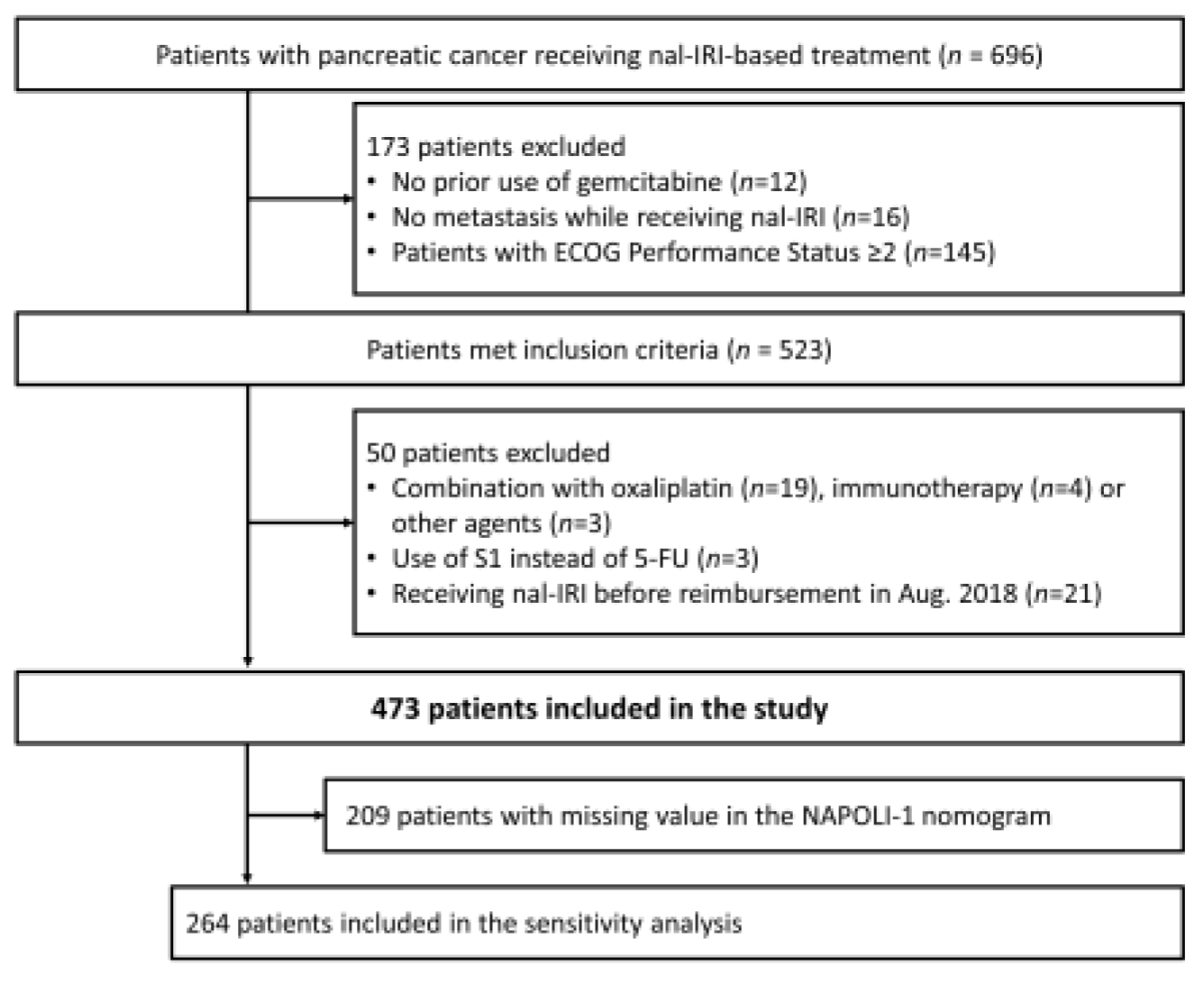
2. Materials and Methods
3. Results
3.1. Patient Demographics
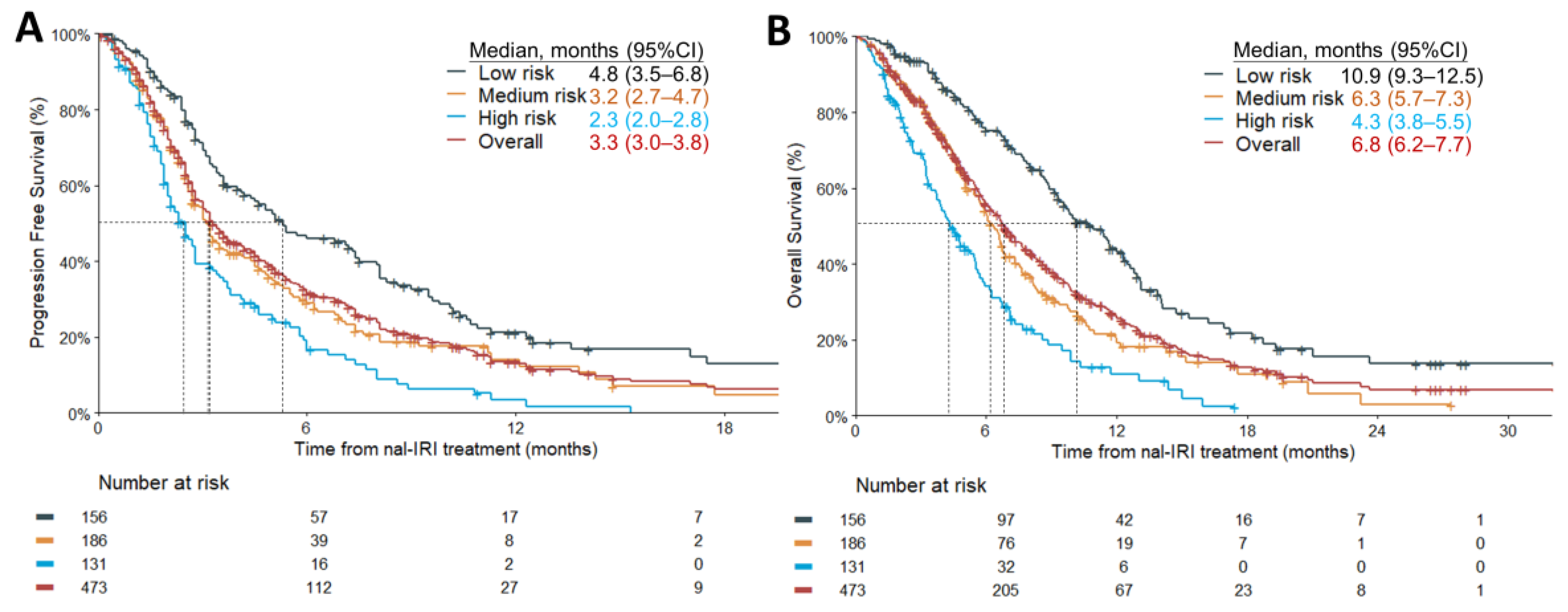
3.2. Model Performance
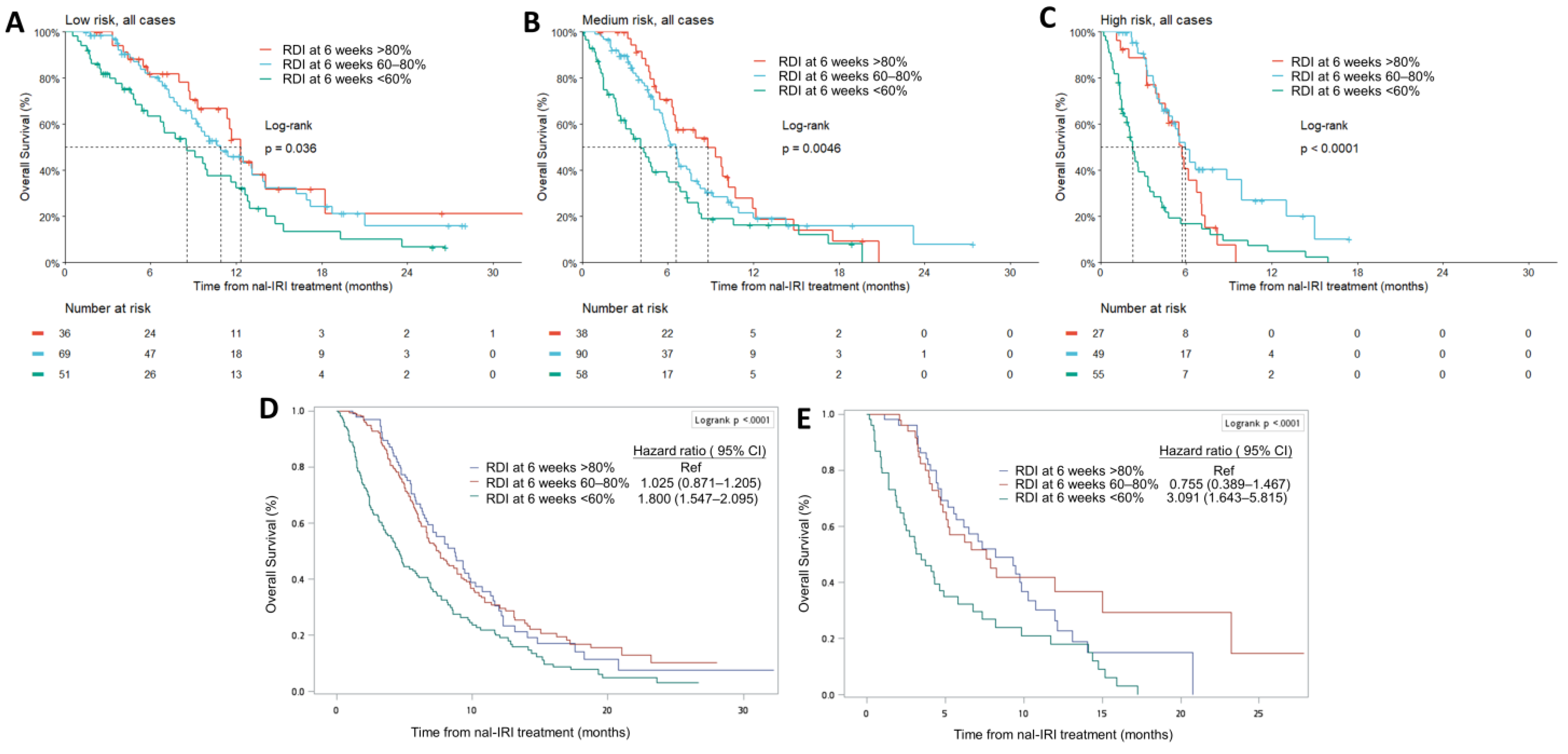
3.3. Relative Dose Intensity at 6 Weeks Is an Independent Prognostic Factor
3.4. Real-World Safety Profile
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang-Gillam, A.; Li, C.-P.; Bodoky, G.; Dean, A.; Shan, Y.-S.; Jameson, G.; Macarulla, T.; Lee, K.-H.; Cunningham, D.; Blanc, J.F.; et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): A global, randomised, open-label, phase 3 trial. Lancet 2016, 387, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Miki, M.; Fujimori, N.; Ueda, K.; Lee, L.; Murakami, M.; Takamatsu, Y.; Shimokawa, Y.; Niina, Y.; Oono, T.; Hisano, T.; et al. Treatment Effect and Safety of Nanoliposomal Irinotecan with Fluorouracil and Folinic Acid after Gemcitabine-Based Therapy in Patients with Advanced Pancreatic Cancer: A Multicenter, Prospective Observational Study. J. Clin. Med. 2022, 11, 5084. [Google Scholar] [CrossRef] [PubMed]
- Glassman, D.C.; Palmaira, R.L.; Covington, C.M.; Desai, A.M.; Ku, G.Y.; Li, J.; Harding, J.J.; Varghese, A.M.; O’Reilly, E.M.; Yu, K.H. Nanoliposomal irinotecan with fluorouracil for the treatment of advanced pancreatic cancer, a single institution experience. BMC Cancer 2018, 18, 693. [Google Scholar] [CrossRef] [PubMed]
- Kieler, M.; Unseld, M.; Bianconi, D.; Scheithauer, W.; Prager, G.W. A real-world analysis of second-line treatment options in pancreatic cancer: Liposomal-irinotecan plus 5-fluorouracil and folinic acid. Ther. Adv. Med. Oncol. 2019, 11, 1758835919853196. [Google Scholar] [CrossRef]
- Yoo, C.; Im, H.-S.; Kim, K.-P.; Oh, D.-Y.; Lee, K.-H.; Chon, H.J.; Kim, J.H.; Kang, M.; Kim, I.; Lee, G.J.; et al. Real-world efficacy and safety of liposomal irinotecan plus fluorouracil/leucovorin in patients with metastatic pancreatic adenocarcinoma: A study by the Korean Cancer Study Group. Ther. Adv. Med. Oncol. 2019, 11, 1758835919871126. [Google Scholar] [CrossRef]
- Tossey, J.C.; Reardon, J.; VanDeusen, J.B.; Noonan, A.M.; Porter, K.; Arango, M.J. Comparison of conventional versus liposomal irinotecan in combination with fluorouracil for advanced pancreatic cancer: A single-institution experience. Med. Oncol. 2019, 36, 87. [Google Scholar] [CrossRef]
- Barzi, A.; Miksad, R.; Surinach, A.; Corvino, F.A.; Wang, S.; Torres, A.Z.; Mamlouk, K.; Pulgar, S.; Valderrama, A.; Bekaii-Saab, T.; et al. Real-World Dosing Patterns and Outcomes of Patients With Metastatic Pancreatic Cancer Treated With a Liposomal Irinotecan Regimen in the United States. Pancreas 2020, 49, 193–200. [Google Scholar] [CrossRef]
- Su, Y.-Y.; Chiang, N.-J.; Tsai, H.-J.; Yen, C.-J.; Shan, Y.-S.; Chen, L.-T. The Impact of Liposomal Irinotecan on the Treatment of Advanced Pancreatic Adenocarcinoma: Real-World Experience in a Taiwanese Cohort. Sci. Rep. 2020, 10, 7420. [Google Scholar] [CrossRef]
- Kim, G.P.; Surinach, A.; Corvino, F.A.; Cockrum, P.; Belanger, B.; Abushahin, L. Real-world outcomes associated with liposomal irinotecan dose reductions in metastatic pancreatic ductal adenocarcinoma. Futur. Oncol. 2021, 17, 675–688. [Google Scholar] [CrossRef]
- Kasi, A.; McGinnis, T.; Naik, G.; Handa, S.; Williams, G.; Paluri, R. Efficacy and tolerability of the combination of nano-liposomal irinotecan and 5-fluorouracil/leucovorin in advanced pancreatic adenocarcinoma: Post-approval clinic experience. J. Gastrointest. Oncol. 2021, 12, 464–473. [Google Scholar] [CrossRef]
- Park, H.; Kang, B.; Chon, H.; Im, H.-S.; Lee, C.-K.; Kim, I.; Kang, M.; Hwang, J.; Bae, W.; Cheon, J.; et al. Liposomal irinotecan plus fluorouracil/leucovorin versus FOLFIRINOX as the second-line chemotherapy for patients with metastatic pancreatic cancer: A multicenter retrospective study of the Korean Cancer Study Group (KCSG). ESMO Open 2021, 6, 100049. [Google Scholar] [CrossRef] [PubMed]
- Bang, K.; Cheon, J.; Jeong, J.H.; Im, H.-S.; Kim, K.-P.; Ryoo, B.-Y.; Yoo, C. Clinical outcomes of liposomal irinotecan plus fluorouracil/leucovorin for metastatic pancreatic adenocarcinoma in patients previously treated with conventional irinotecan-containing chemotherapy. Ther. Adv. Med. Oncol. 2021, 13, 17588359211003053. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.H.; Hendifar, A.E.; Alese, O.B.; Draper, A.; Abdelrahim, M.; Burns, E.; Khan, G.; Cockrum, P.; Bhak, R.H.; Nguyen, C.; et al. Clinical Outcomes Among Patients With Metastatic Pancreatic Ductal Adenocarcinoma Treated With Liposomal Irinotecan. Front. Oncol. 2021, 11, 678070. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-H.; Chiang, N.-J.; Chiu, S.-C.; Chou, W.-C.; Bai, L.-Y.; Li, C.-P.; Su, Y.-Y.; Chiu, T.-J.; Chuang, S.-C.; Peng, C.-M.; et al. The impact of spleen volume on the survival of metastatic pancreatic adenocarcinoma patients receiving nanoliposomal irinotecan. Am. J. Cancer Res. 2022, 12, 1884–1898. [Google Scholar]
- Yu, H.-Y.; Lee, C.-Y.; Lin, L.-G.; Chao, Y.; Li, C.-P. Nanoliposomal irinotecan with 5-fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy: A real-world experience. J. Chin. Med. Assoc. 2022, 85, 42–50. [Google Scholar] [CrossRef]
- Iasonos, A.; Schrag, D.; Raj, G.V.; Panageas, K.S. How to build and interpret a nomogram for cancer prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef]
- Hsu, C.; Liu, K.; Chang, P.; Chen, P.; Hung, C.; Hsueh, S.; Yeh, K.; Chen, Y.; Lu, C.; Hung, Y.; et al. Development and validation of a prognostic nomogram to predict survival in patients with advanced pancreatic cancer receiving second-line palliative chemotherapy. J. Gastroenterol. Hepatol. 2020, 35, 1694–1703. [Google Scholar] [CrossRef]
- Chen, L.-T.; Macarulla, T.; Blanc, J.-F.; Mirakhur, B.; de Jong, F.A.; Belanger, B.; Bekaii-Saab, T.; Siveke, J.T. Nomogram for Predicting Survival in Patients Treated with Liposomal Irinotecan Plus Fluorouracil and Leucovorin in Metastatic Pancreatic Cancer. Cancers 2019, 11, 1068. [Google Scholar] [CrossRef]
- Chen, L.-T.; Siveke, J.T.; Wang-Gillam, A.; Li, C.-P.; Bodoky, G.; Dean, A.P.; Shan, Y.-S.; Jameson, G.S.; Macarulla, T.; Lee, K.-H.; et al. Survival with nal-IRI (liposomal irinotecan) plus 5-fluorouracil and leucovorin versus 5-fluorouracil and leucovorin in per-protocol and non-per-protocol populations of NAPOLI-1: Expanded analysis of a global phase 3 trial. Eur. J. Cancer 2018, 105, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.-Y.; Chiang, N.-J.; Li, C.-P.; Yen, C.-J.; Yang, S.-H.; Chou, W.-C.; Chen, J.-S.; Chiu, T.-J.; Chen, Y.-Y.; Chuang, S.-C.; et al. Dosing Pattern and Early Cumulative Dose of Liposomal Irinotecan in Metastatic Pancreatic Cancer: A Real-World Multicenter Study. Front. Oncol. 2022, 12, 800842. [Google Scholar] [CrossRef] [PubMed]
- van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Bang, Y.; Li, C.; Lee, K.; Chiu, C.; Park, J.O.; Shan, Y.; Kim, J.S.; Chen, J.; Shim, H.; Rau, K.; et al. Liposomal irinotecan in metastatic pancreatic adenocarcinoma in Asian patients: Subgroup analysis of the NAPOLI-1 study. Cancer Sci. 2020, 111, 513–527. [Google Scholar] [CrossRef]
- Adiwijaya, B.; Kim, J.; Lang, I.; Csõszi, T.; Cubillo, A.; Chen, J.-S.; Wong, M.; Park, J.; Rau, K.; Melichar, B.; et al. Population Pharmacokinetics of Liposomal Irinotecan in Patients With Cancer. Clin. Pharmacol. Ther. 2017, 102, 997–1005. [Google Scholar] [CrossRef]
- Su, Y.-Y.; Chiang, N.-J.; Chang, J.; Wang, Y.-W.; Shen, B.-N.; Li, Y.-J.; Hwang, D.-Y.; Shan, Y.-S.; Chen, L.-T. The association between UGT1A1 polymorphisms and treatment toxicities of liposomal irinotecan. ESMO Open 2022, 8, 100746. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. Multiple Imputation After 18+ Years. J. Am. Stat. Assoc. 1996, 91, 473–489. [Google Scholar] [CrossRef]
- Rezvan, P.H.; Lee, K.J.; Simpson, J.A. The rise of multiple imputation: A review of the reporting and implementation of the method in medical research. BMC Med. Res. Methodol. 2015, 15, 30. [Google Scholar] [CrossRef]
- Tan, P.-T.; Cro, S.; Van Vogt, E.; Szigeti, M.; Cornelius, V.R. A review of the use of controlled multiple imputation in randomised controlled trials with missing outcome data. BMC Med. Res. Methodol. 2021, 21, 72. [Google Scholar] [CrossRef]
- Ch’Ang, H.-J.; Wang, C.-C.; Cheng, A.-L.; Hsu, C.; Lu, Y.-S.; Chang, M.-C.; Lin, J.-T.; Wang, H.-P.; Shiah, H.-S.; Liu, T.-W.; et al. Phase I study of biweekly gemcitabine followed by oxaliplatin and simplified 48-h infusion of fluorouracil/leucovorin for advanced pancreatic cancer. J. Gastroenterol. Hepatol. 2006, 21, 874–879. [Google Scholar] [CrossRef]
- Ch’Ang, H.-J.; Huang, C.-L.; Wang, H.-P.; Shiah, H.-S.; Chang, M.-C.; Jan, C.-M.; Chen, J.-S.; Tien, Y.-W.; Lin, J.-T.; Cheng, A.-L.; et al. Phase II study of biweekly gemcitabine followed by oxaliplatin and simplified 48-h infusion of 5-fluorouracil/leucovorin (GOFL) in advanced pancreatic cancer. Cancer Chemother. Pharmacol. 2009, 64, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Chiang, N.-J.; Tsai, K.K.; Hsiao, C.-F.; Yang, S.-H.; Hsiao, H.-H.; Shen, W.-C.; Hsu, C.; Lin, Y.-L.; Chen, J.-S.; Shan, Y.-S.; et al. A multicenter, phase I/II trial of biweekly S-1, leucovorin, oxaliplatin and gemcitabine in metastatic pancreatic adenocarcinoma-TCOG T1211 study. Eur. J. Cancer 2020, 124, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Y.-Y.; Chiu, Y.-F.; Li, C.-P.; Yang, S.-H.; Lin, J.; Lin, S.-J.; Chang, P.-Y.; Chiang, N.-J.; Shan, Y.-S.; Ch’Ang, H.-J.; et al. A phase II randomised trial of induction chemotherapy followed by concurrent chemoradiotherapy in locally advanced pancreatic cancer: The Taiwan Cooperative Oncology Group T2212 study. Br. J. Cancer 2022, 126, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Chiang, N.-J.; Shan, Y.-S.; Bai, L.-Y.; Li, C.-P.; Chen, J.-S.; Yang, S.-H.; Kuo, Y.-C.; Chao, Y.; Hsieh, Y.-Y.; Kao, H.-F.; et al. TCOG T5217 trial: A phase II randomized study of SLOG versus modified FOLFIRINOX as the first-line treatment in locally advanced or metastatic pancreatic ductal adenocarcinoma. J. Clin. Oncol. 2021, 39, 4143. [Google Scholar] [CrossRef]
- Su, Y.-Y.; Ting, Y.-L.; Wang, C.-J.; Chao, Y.-J.; Liao, T.-K.; Su, P.-J.; Chiang, N.-J.; Liao, I.-C.; Yu, Y.-T.; Liu, Y.-S.; et al. Improved survival with induction chemotherapy and conversion surgery in locally advanced unresectable pancreatic cancer: A single institution experience. Am. J. Cancer Res. 2022, 12, 2189–2202. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Group | Low | Intermediate | High | Overall |
|---|---|---|---|---|
| (n = 156) | (n = 186) | (n = 131) | (n = 473) | |
| Gender | ||||
| Female | 67 (42.9%) | 83 (44.6%) | 48 (36.6%) | 198 (41.9%) |
| Male | 89 (57.1%) | 103 (55.4%) | 83 (63.4%) | 275 (58.1%) |
| Age, median (range) | 62.5 (27–82) | 63.0 (34–86) | 63 (33–86) | 63 (27–86) |
| Disease stage at diagnosis | ||||
| Stage I-III | 108 (69.2%) | 40 (21.5%) | 6 (4.6%) | 154 (32.6%) |
| Stage IV | 48 (30.8%) | 146 (78.5%) | 125 (95.4%) | 319 (67.4%) |
| Primary tumor location | ||||
| Head | 90 (57.7%) | 95 (51.1%) | 64 (48.9%) | 249 (52.6%) |
| Body | 34 (21.8%) | 52 (28.0%) | 22 (16.8%) | 108 (22.8%) |
| Tail | 24 (15.4%) | 32 (17.2%) | 37 (28.2%) | 93 (19.7%) |
| Body + Tail | 7 (4.5%) | 6 (3.2%) | 7 (5.3%) | 20 (4.2%) |
| Head + Body or Tail | 1 (0.6%) | 1 (0.5%) | 1 (0.8%) | 3 (0.6%) |
| Albumin | ||||
| <4 | 45 (28.8%) | 69 (37.1%) | 65 (49.6%) | 179 (37.8%) |
| ≥4 | 55 (35.3%) | 37 (19.9%) | 22 (16.8%) | 114 (24.1%) |
| Not checked | 56 (35.9%) | 80 (43.0%) | 44 (33.6%) | 180 (38.1%) |
| Number of metastatic sites | ||||
| 1 | 117 (75.0%) | 90 (48.4%) | 47 (35.9%) | 254 (53.7%) |
| 2 | 34 (21.8%) | 66 (35.5%) | 41 (31.3%) | 141 (29.8%) |
| 3 | 5 (3.2%) | 27 (14.5%) | 33 (25.2%) | 65 (13.7%) |
| ≥4 | 0 (0%) | 3 (1.6%) | 10 (7.6%) | 13 (2.7%) |
| Site of metastasis | ||||
| Liver | 69 (44.2%) | 125 (67.2%) | 125 (95.4%) | 319 (67.4%) |
| Lung | 35 (22.4%) | 47 (25.3%) | 40 (30.5%) | 122 (25.8%) |
| Peritoneum | 38 (24.4%) | 55 (29.6%) | 37 (28.2%) | 130 (27.5%) |
| CA-19.9 | ||||
| <40 U/mL | 37 (23.7%) | 26 (14.0%) | 6 (4.6%) | 69 (14.6%) |
| ≥40 U/mL | 109 (69.9%) | 138 (74.2%) | 99 (75.6%) | 346 (73.2%) |
| Not checked | 10 (6.4%) | 22 (11.8%) | 26 (19.8%) | 58 (12.3%) |
| Prior treatment | ||||
| Gemcitabine-containing | 156 (100%) | 186 (100%) | 131 (100%) | 473 (100%) |
| Fluorouracil-containing | 112 (71.8%) | 150 (80.6%) | 104 (79.4%) | 366 (77.4%) |
| Irinotecan-containing | 16 (10.3%) | 28 (15.1%) | 20 (15.3%) | 64 (13.5%) |
| Platinum-containing | 59 (37.8%) | 86 (46.2%) | 73 (55.7%) | 218 (46.1%) |
| Taxane-containing | 47 (30.1%) | 56 (30.1%) | 41 (31.3%) | 144 (30.4%) |
| Prior lines of systemic treatment † | ||||
| 0 | 2 (1.3%) | 5 (2.7%) | 0 (0%) | 7 (1.5%) |
| 1 | 101 (64.7%) | 110 (59.1%) | 84 (64.1%) | 295 (62.4%) |
| ≥2 | 53 (34.0%) | 71 (38.2%) | 47 (35.9%) | 171 (36.2%) |
| Operation history | ||||
| No surgery | 74 (47.4%) | 119 (64.0%) | 88 (67.2%) | 281 (59.4%) |
| Whipple operation | 26 (16.7%) | 34 (18.3%) | 17 (13.0%) | 77 (16.3%) |
| Distal pancreatectomy | 20 (12.8%) | 13 (7.0%) | 9 (6.9%) | 42 (8.9%) |
| Total pancreatectomy | 3 (1.9%) | 4 (2.2%) | 3 (2.3%) | 10 (2.1%) |
| Other procedures | 33 (21.2%) | 16 (8.6%) | 14 (10.7%) | 63 (13.3%) |
| Interval between the last therapy and nal-IRI+5-FU/LV | ||||
| Median (IQR) | 0.754 (0.475–1.28) | 0.672 (0.459–1.08) | 0.689 (0.459–1.11) | 0.689 (0.459–1.15) |
| Not recorded | 21 (13.5%) | 28 (15.1%) | 16 (12.2%) | 65 (13.7%) |
| Model 1 NAPOLI-1 Nomogram | Model 2 NAPOLI-1 Nomogram and Cumulative Dose | ||||
|---|---|---|---|---|---|
| Parameter | HR (95%CI) | p-Value | Parameter | HR (95%CI) | p-Value |
| Nomogram risk score | 0.996 (0.995–0.997) | <0.0001 | Nomogram risk score | 0.996 (0.995–0.997) | <0.0001 |
| Age | 1.009 (0.996–1.023) | 0.1607 | RDI6-week > 80% | Reference | - |
| Gender: male | 1.406 (1.118–1.766) | 0.0034 | 60–80% | 1.050 (0.777–1.419) | 0.9148 |
| <60% | 1.975 (1.461–2.670) | <0.0001 | |||
| Age | 1.008 (0.994–1.021) | 0.2786 | |||
| Gender: male | 1.287 (1.022–1.620) | 0.0317 | |||
| Risk Group | Low | Intermediate (n = 186) | High | Overall |
|---|---|---|---|---|
| (n = 156) | (n = 131) | (n = 473) | ||
| Neutropenia | ||||
| All-grade | 69 (44.2%) | 76 (40.9%) | 52 (39.7%) | 197 (41.6%) |
| ≥grade 3 | 36 (23.1%) | 44 (23.7%) | 30 (22.9%) | 110 (23.3%) |
| Febrile neutropenia | 4 (2.6%) | 7 (3.8%) | 5 (3.8%) | 16 (3.4%) |
| Not recorded | 4 (2.1%) | 2 (1.2%) | 3 (2.4%) | 9 (1.9%) |
| Anemia | ||||
| All-grade | 83 (53.2%) | 121 (65.1%) | 97 (74.0%) | 301(63.6%) |
| ≥grade 3 | 23 (14.7%) | 37 (19.9%) | 32 (24.4%) | 92 (19.5%) |
| Not recorded | 2 (1.1%) | 2 (1.2%) | 2 (1.6%) | 6 (1.3%) |
| Thrombocytopenia | ||||
| All-grade | 26 (16.7%) | 47 (25.3%) | 42 (32.1%) | 115 (24.3%) |
| ≥grade 3 | 5 (3.2%) | 10 (5.4%) | 9 (6.9%) | 24 (5.1%) |
| Not recorded | 3 (1.6%) | 1 (0.6%) | 2 (1.6%) | 6 (1.3%) |
| AST or ALT increased | ||||
| All-grade | 43 (27.6%) | 61 (32.8%) | 40 (30.5%) | 144 (30.4%) |
| ≥grade 3 | 6 (3.8%) | 7 (3.8%) | 0 (0%) | 13 (2.7%) |
| Not recorded | 40 (21.4%) | 44 (27.2%) | 33 (26.6%) | 117 (24.7%) |
| Blood bilirubin increased | ||||
| All-grade | 20 (12.8%) | 47 (25.3%) | 35 (26.7%) | 102 (21.6%) |
| ≥grade 3 | 10 (6.4%) | 15 (8.1%) | 10 (7.6%) | 35 (7.4%) |
| Not recorded | 23 (12.3%) | 8 (4.9%) | 9 (7.3%) | 40 (8.5%) |
| Creatinine increased | ||||
| All-grade | 28 (17.9%) | 30 (16.1%) | 22 (16.8%) | 80 (16.9%) |
| ≥grade 3 | 0 (0%) | 2 (1.1%) | 1 (0.8%) | 3 (0.6%) |
| Not recorded | 16 (8.6%) | 3 (1.9%) | 6 (4.8%) | 25 (5.3%) |
| Hypokalemia | ||||
| All-grade | 44 (28.2%) | 61 (32.8%) | 47 (35.9%) | 152 (32.1%) |
| ≥grade 3 | 21 (13.5%) | 21 (11.3%) | 18 (13.7%) | 60 (12.7%) |
| Not recorded | 42 (22.5%) | 34 (21.0%) | 29 (23.4%) | 105 (22.2%) |
| Fatigue | ||||
| All-grade | 64 (41.0%) | 84 (45.2%) | 63 (48.1%) | 211 (44.6%) |
| ≥ grade 3 | 1 (0.6%) | 5 (2.7%) | 2 (1.5%) | 8 (1.7%) |
| Not recorded | 12 (6.4%) | 13 (8.0%) | 10 (8.1%) | 35 (7.4%) |
| Vomiting | ||||
| All grade | 62 (39.7%) | 78 (41.9%) | 46 (35.1%) | 186 (39.3%) |
| ≥grade 3 | 5 (3.2%) | 8 (4.3%) | 2 (1.5%) | 15 (3.2%) |
| Not recorded | 3 (1.6%) | 2 (1.2%) | 4 (3.2%) | 9 (1.9%) |
| Diarrhea | ||||
| All-grade | 53 (34.0%) | 55 (29.6%) | 34 (26.0%) | 142 (30.0%) |
| ≥grade 3 | 3 (1.9%) | 5 (2.7%) | 5 (3.8%) | 13 (2.7%) |
| Not recorded | 5 (2.7%) | 3 (1.9%) | 5 (4.0%) | 13 (2.7%) |
| Hypoalbuminemia | ||||
| All-grade | 29 (18.6%) | 50 (26.9%) | 44 (33.6%) | 123 (26.0%) |
| ≥grade 3 | 1 (0.6%) | 5 (2.7%) | 0 (0%) | 6 (1.3%) |
| Not recorded | 28 (15.0%) | 22 (13.6%) | 15 (12.1%) | 65 (13.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, Y.-Y.; Chiang, N.-J.; Yang, Y.-H.; Yen, C.-J.; Bai, L.-Y.; Chiu, C.-F.; Chuang, S.-C.; Yang, S.-H.; Chou, W.-C.; Chen, J.-S.; et al. Real-World Data Validation of NAPOLI-1 Nomogram for the Prediction of Overall Survival in Metastatic Pancreatic Cancer. Cancers 2023, 15, 1008. https://doi.org/10.3390/cancers15041008
Su Y-Y, Chiang N-J, Yang Y-H, Yen C-J, Bai L-Y, Chiu C-F, Chuang S-C, Yang S-H, Chou W-C, Chen J-S, et al. Real-World Data Validation of NAPOLI-1 Nomogram for the Prediction of Overall Survival in Metastatic Pancreatic Cancer. Cancers. 2023; 15(4):1008. https://doi.org/10.3390/cancers15041008
Chicago/Turabian StyleSu, Yung-Yeh, Nai-Jung Chiang, Yi-Hsin Yang, Chia-Jui Yen, Li-Yuan Bai, Chang-Fang Chiu, Shih-Chang Chuang, Shih-Hung Yang, Wen-Chi Chou, Jen-Shi Chen, and et al. 2023. "Real-World Data Validation of NAPOLI-1 Nomogram for the Prediction of Overall Survival in Metastatic Pancreatic Cancer" Cancers 15, no. 4: 1008. https://doi.org/10.3390/cancers15041008