
Hormone Receptor Expression in Meningiomas: A Systematic Review

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
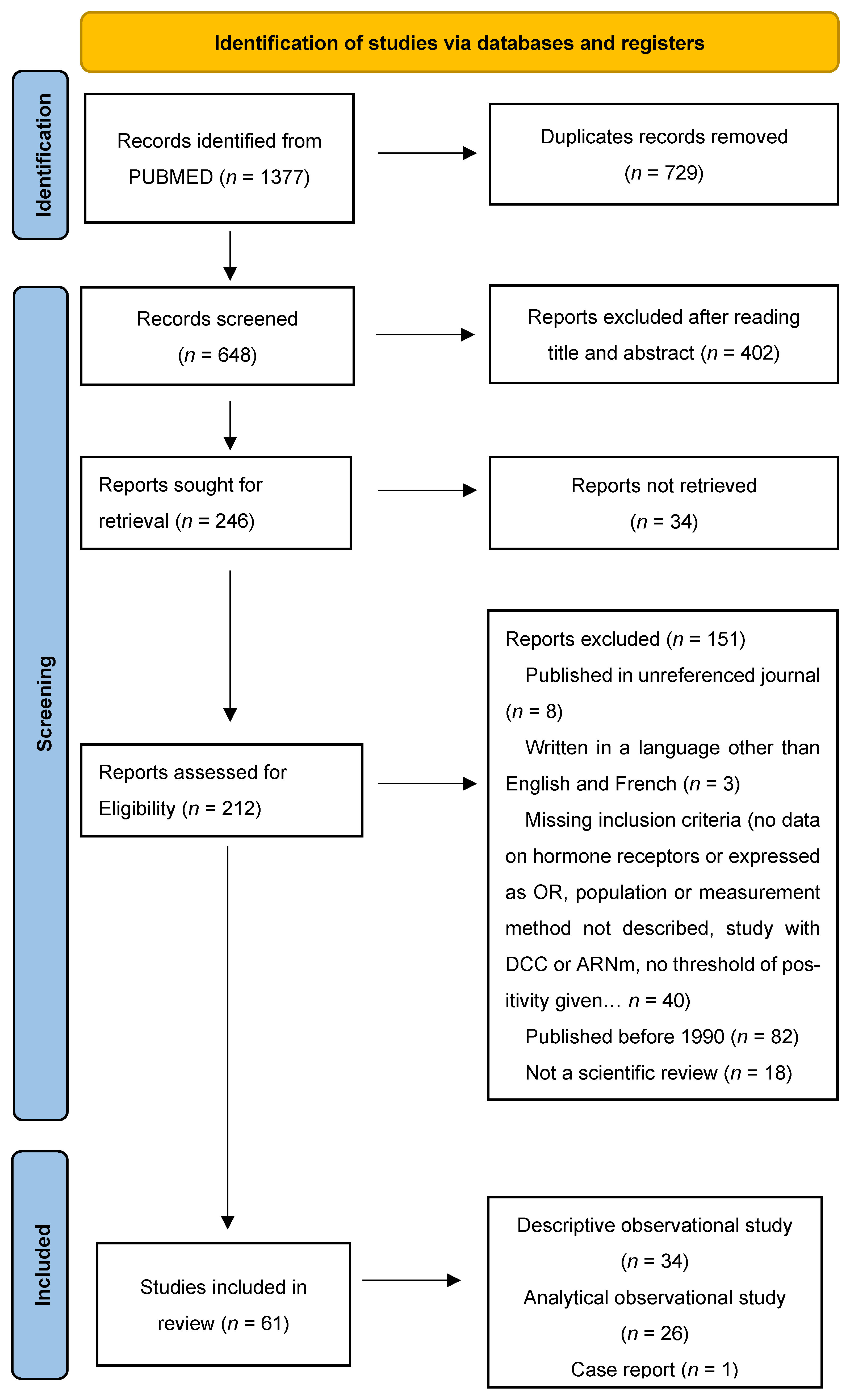
2. Materials and Methods
3. Results
3.1. Risk of Bias
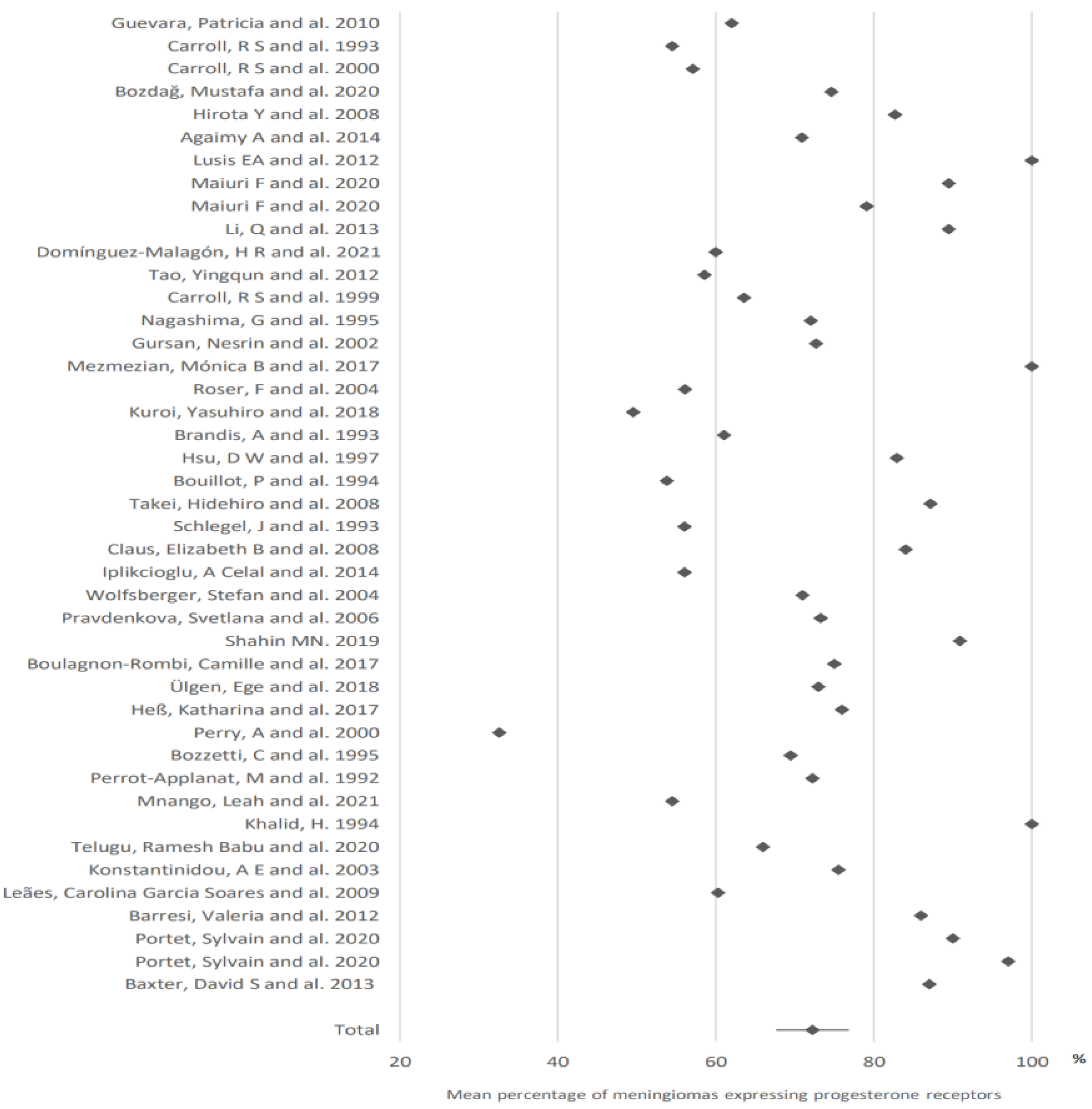
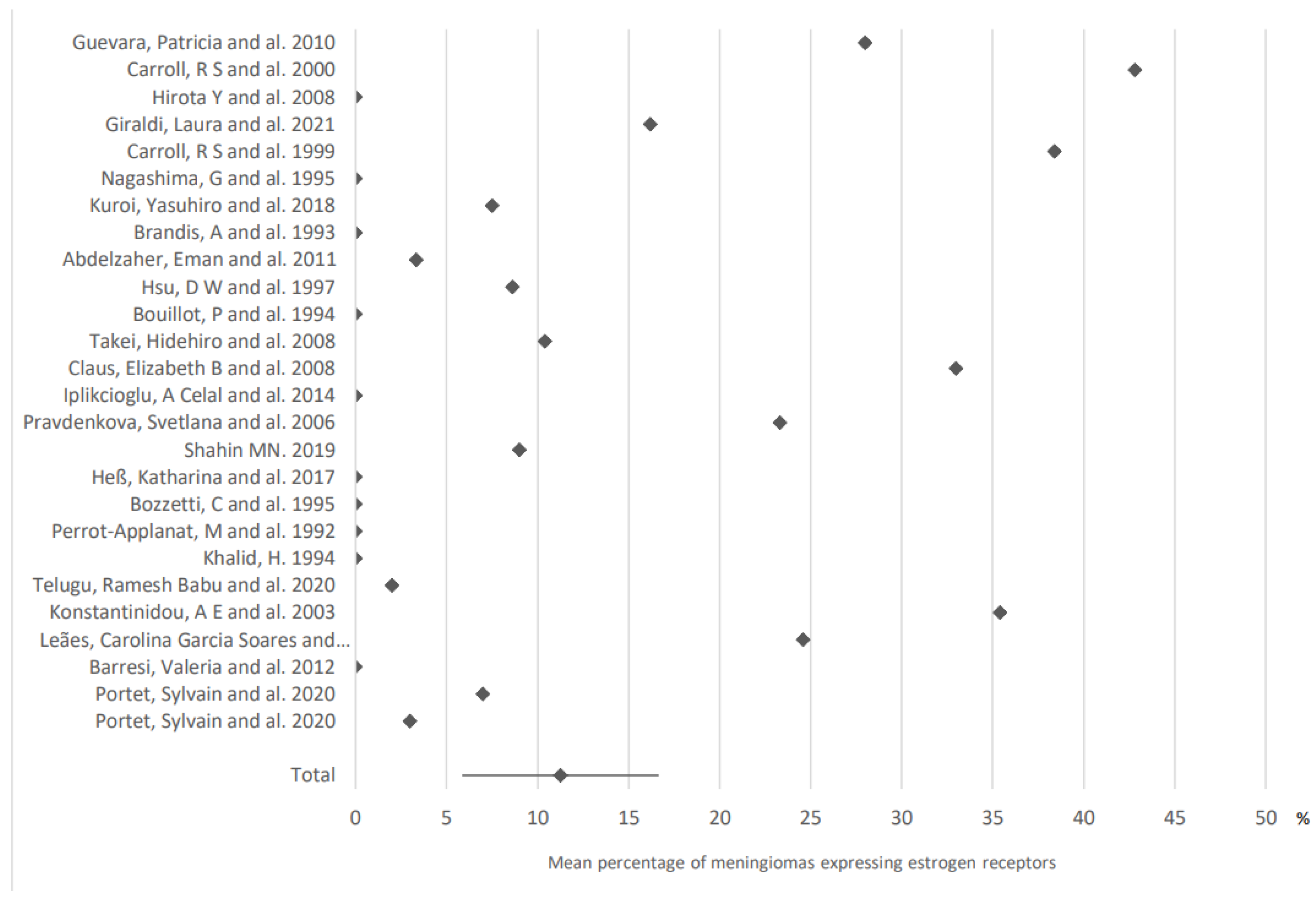
3.2. Hormone Receptor Expression in Meningiomas
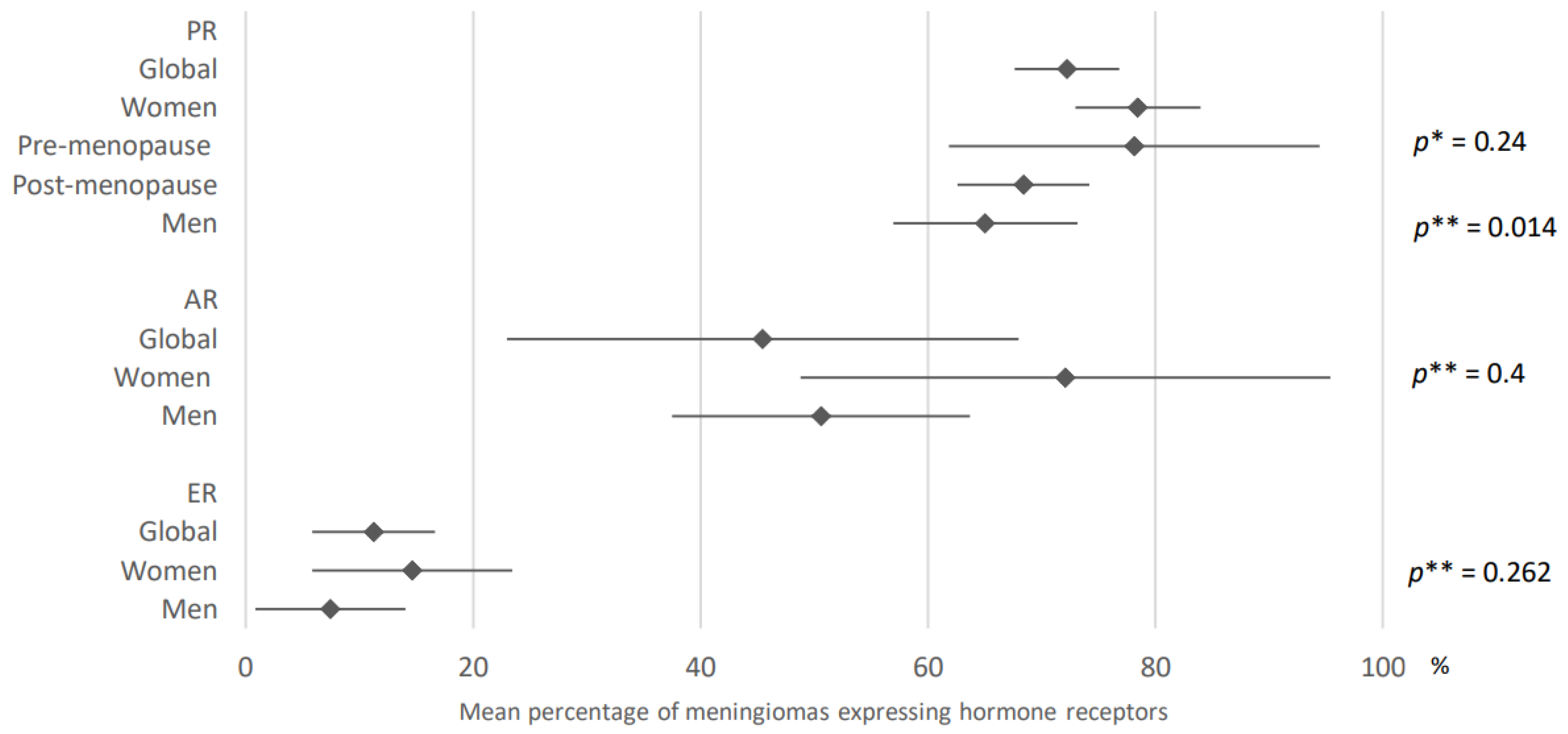
3.3. Hormone Receptor Expression in Meningiomas According to Hormonal Status
3.3.1. Gender and Hormonal Context
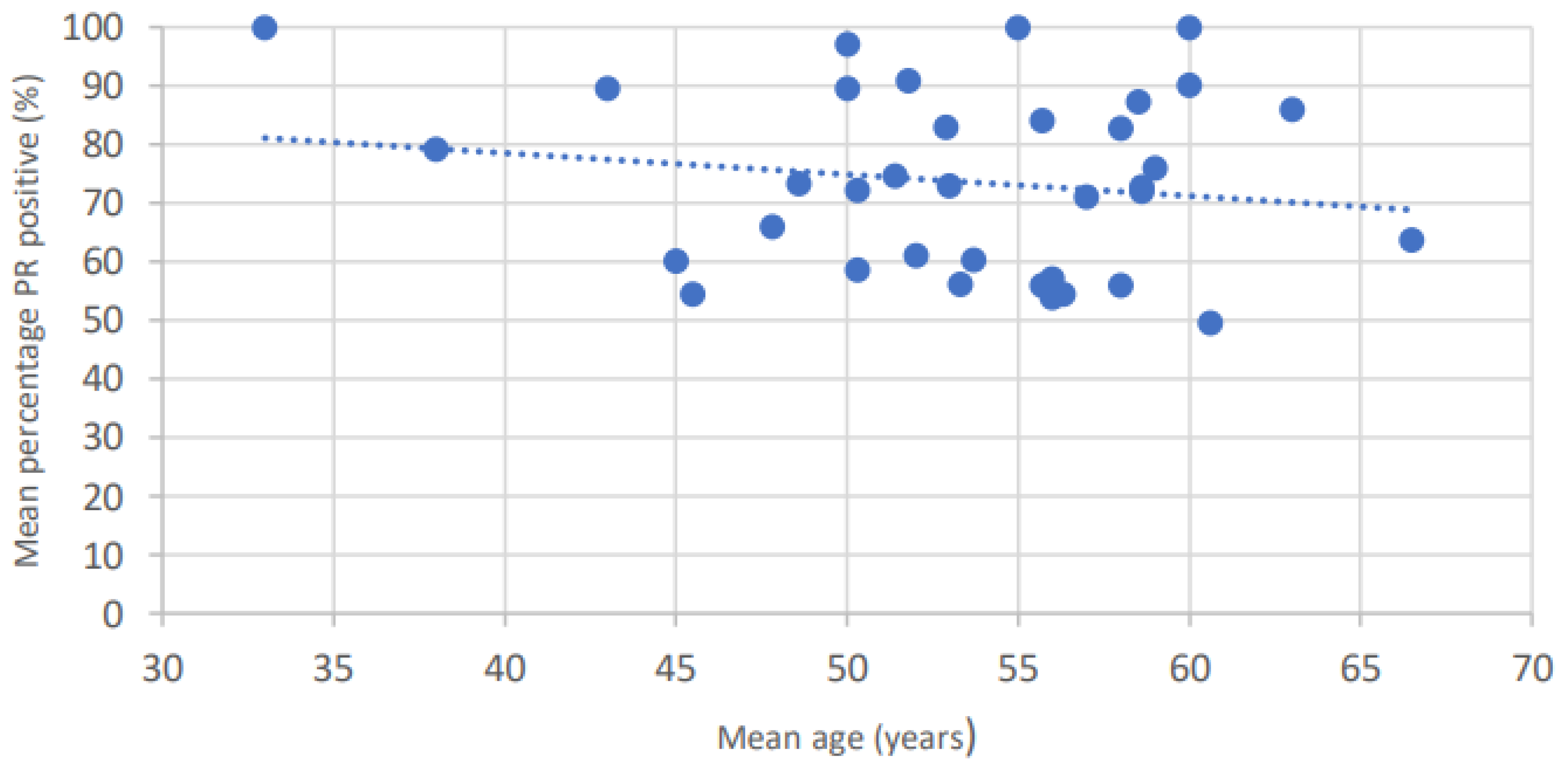
3.3.2. Age
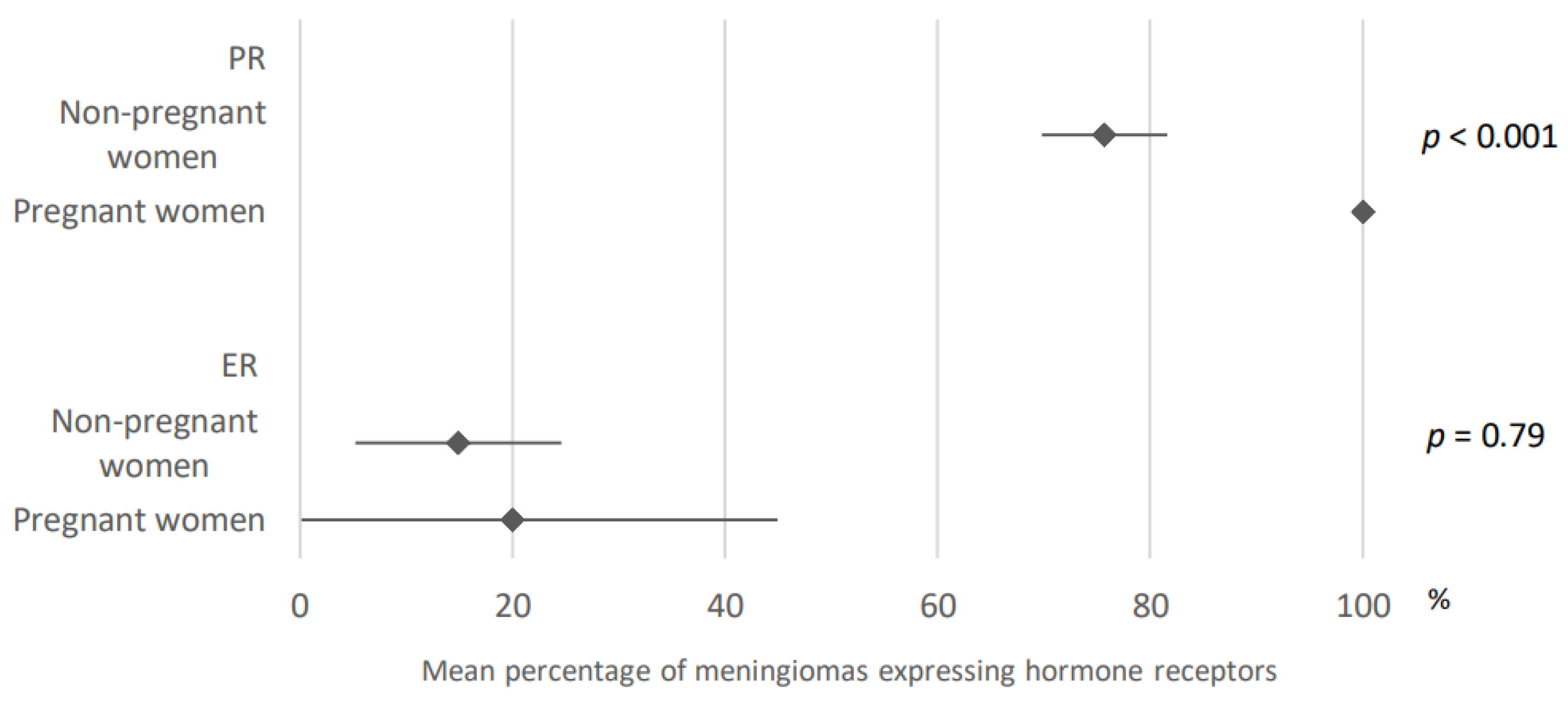
3.3.3. Pregnancy
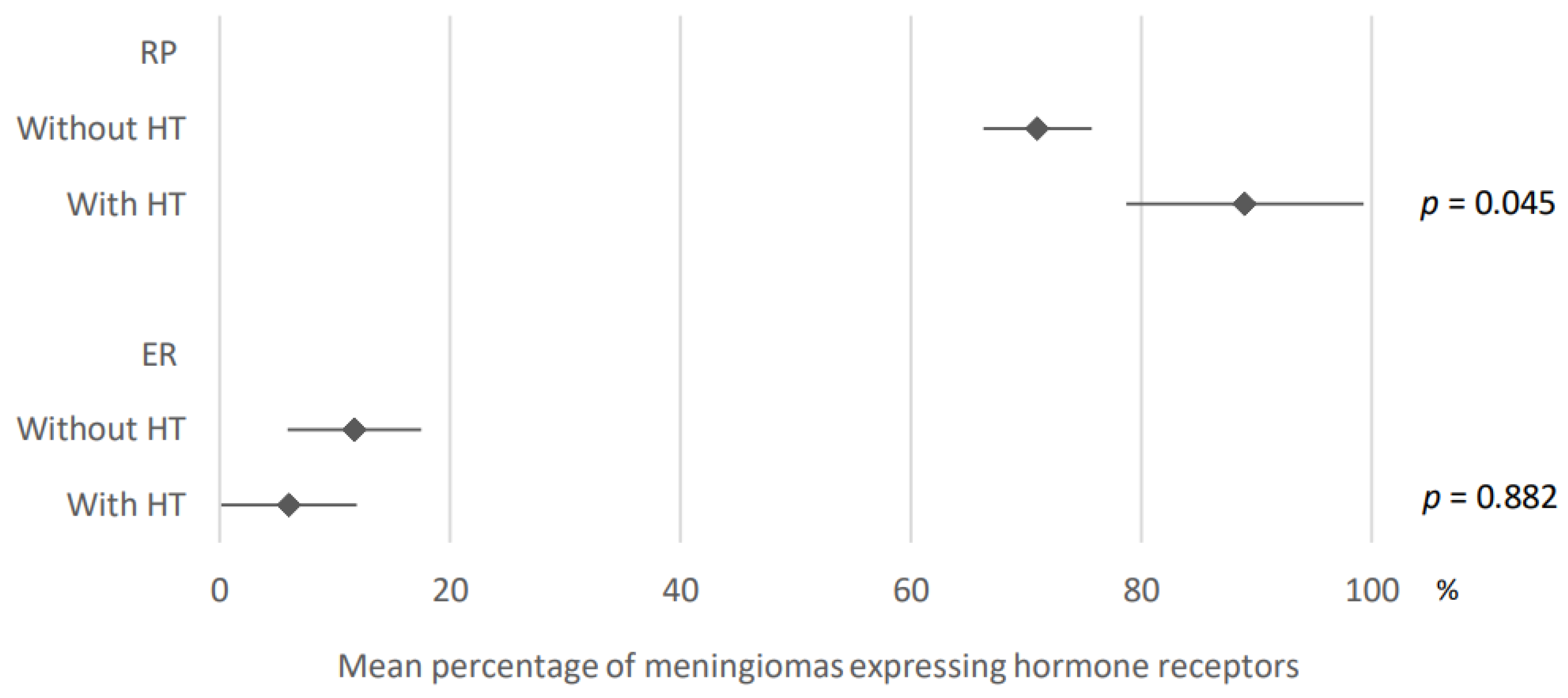
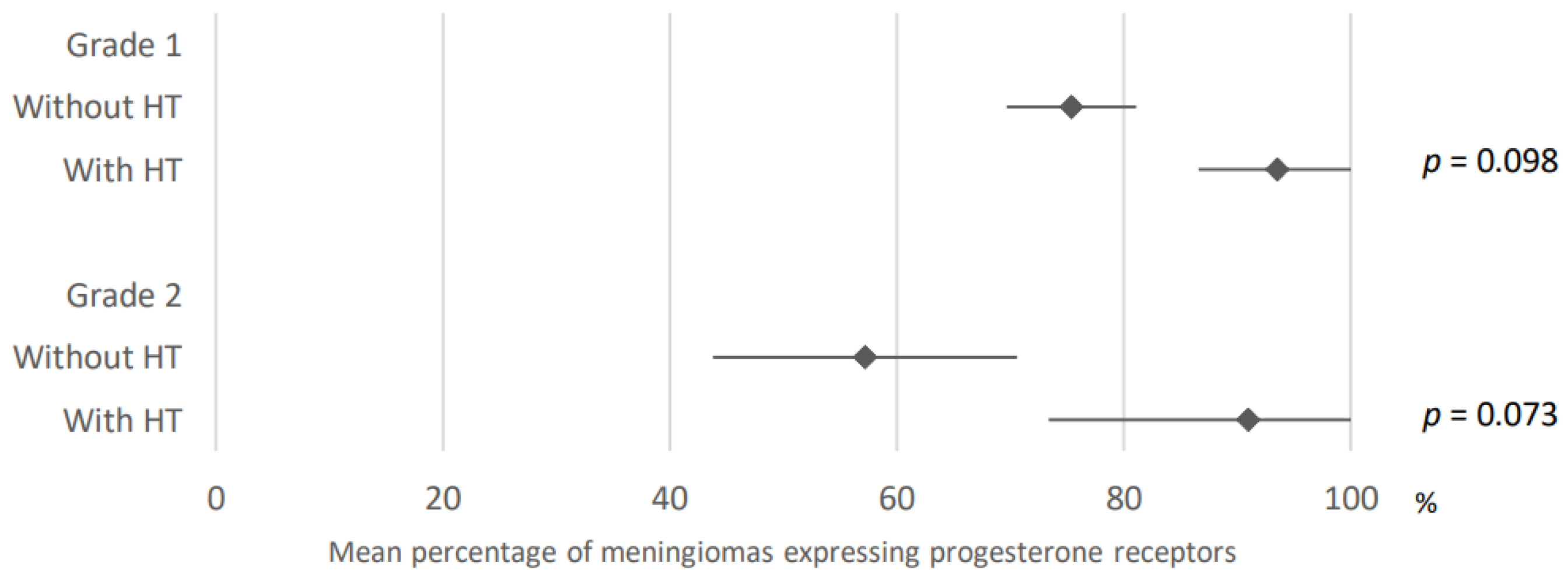
3.3.4. Hormonal Treatment
3.4. Hormone Receptor Expression in Meningiomas According to Localization and Histological Features
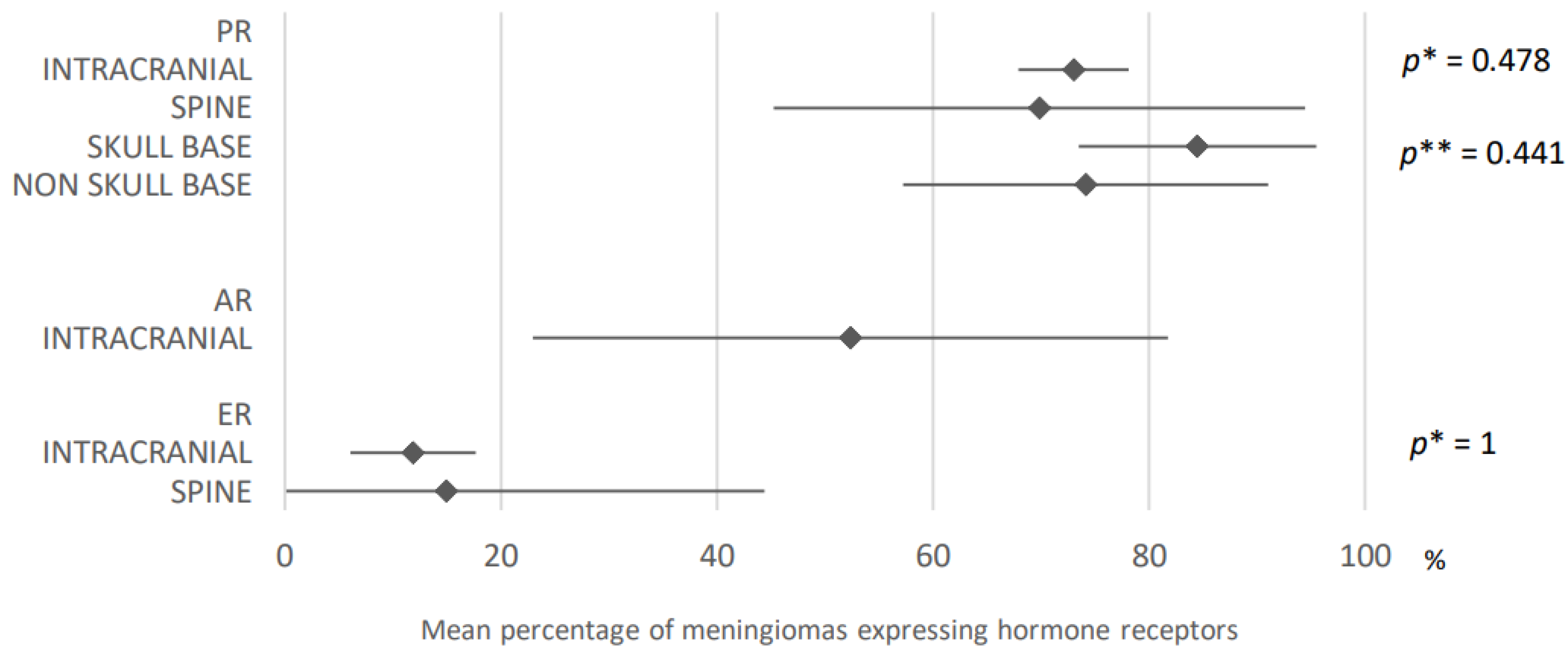
3.4.1. Localization
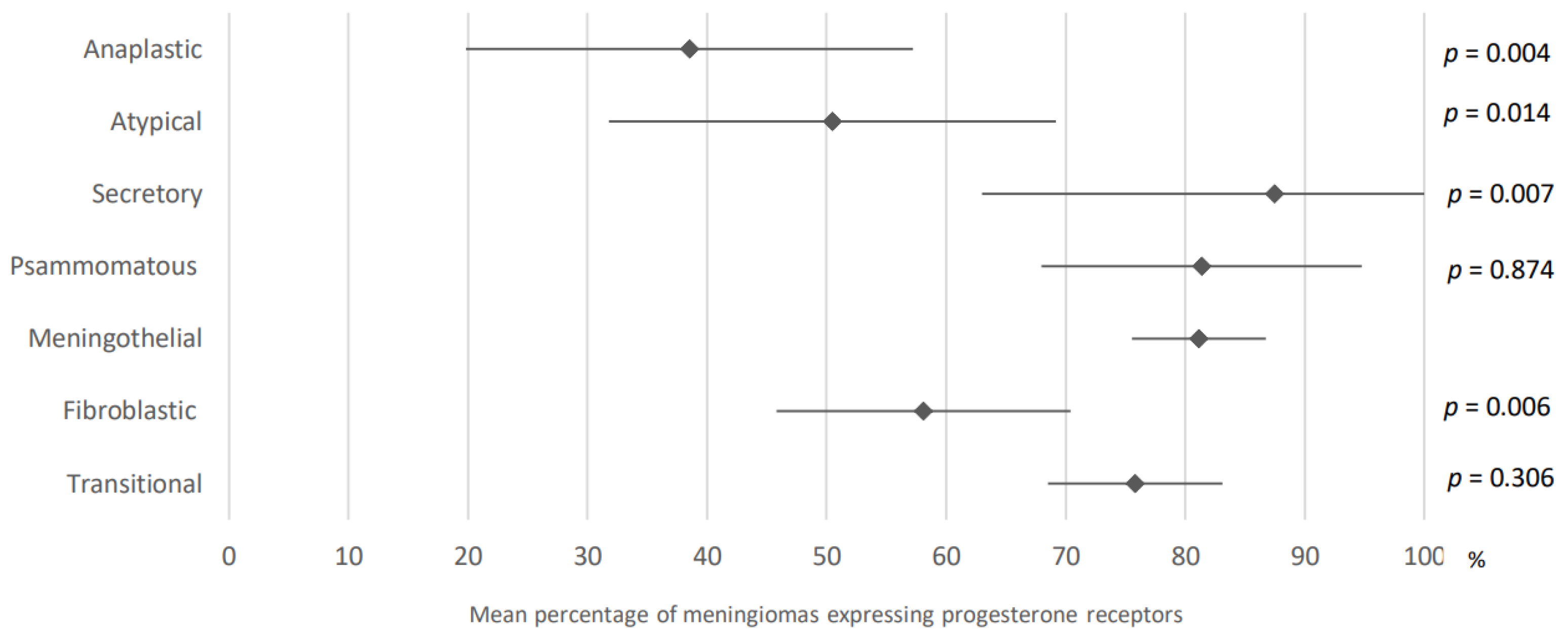
3.4.2. Histological Subtype
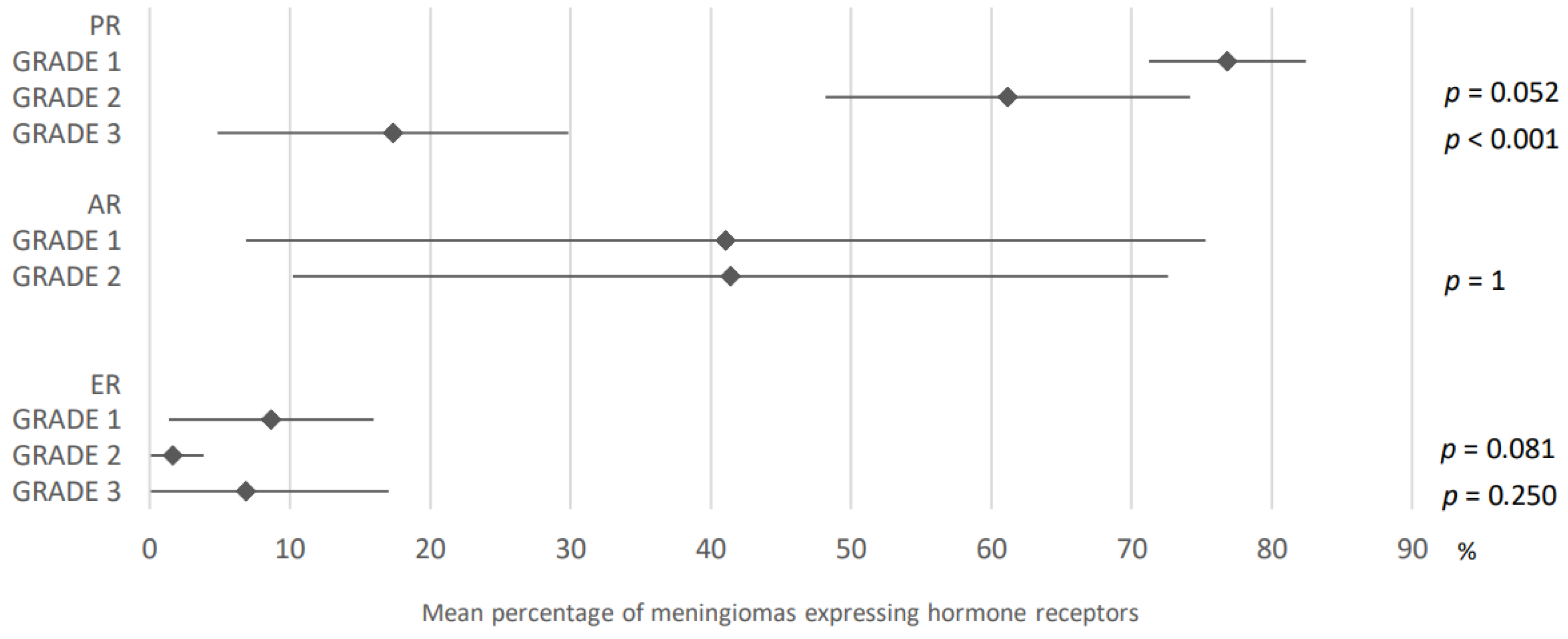
3.4.3. Grade
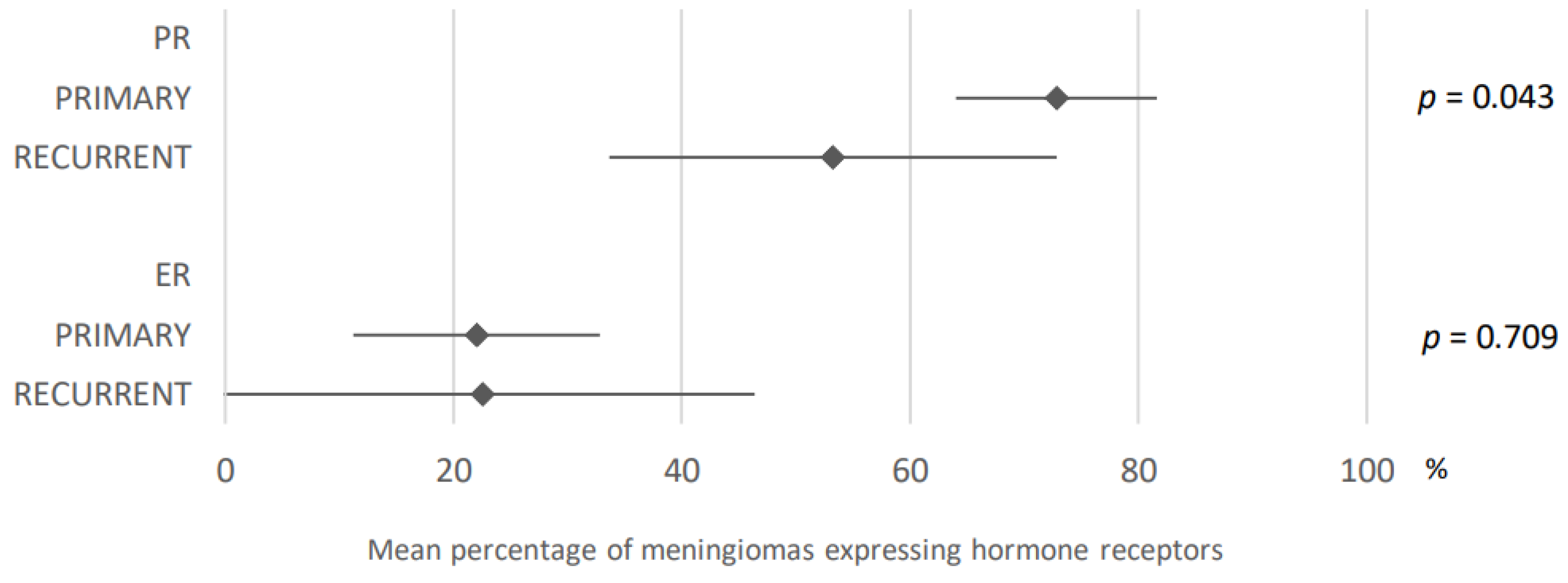
3.4.4. Recurrence
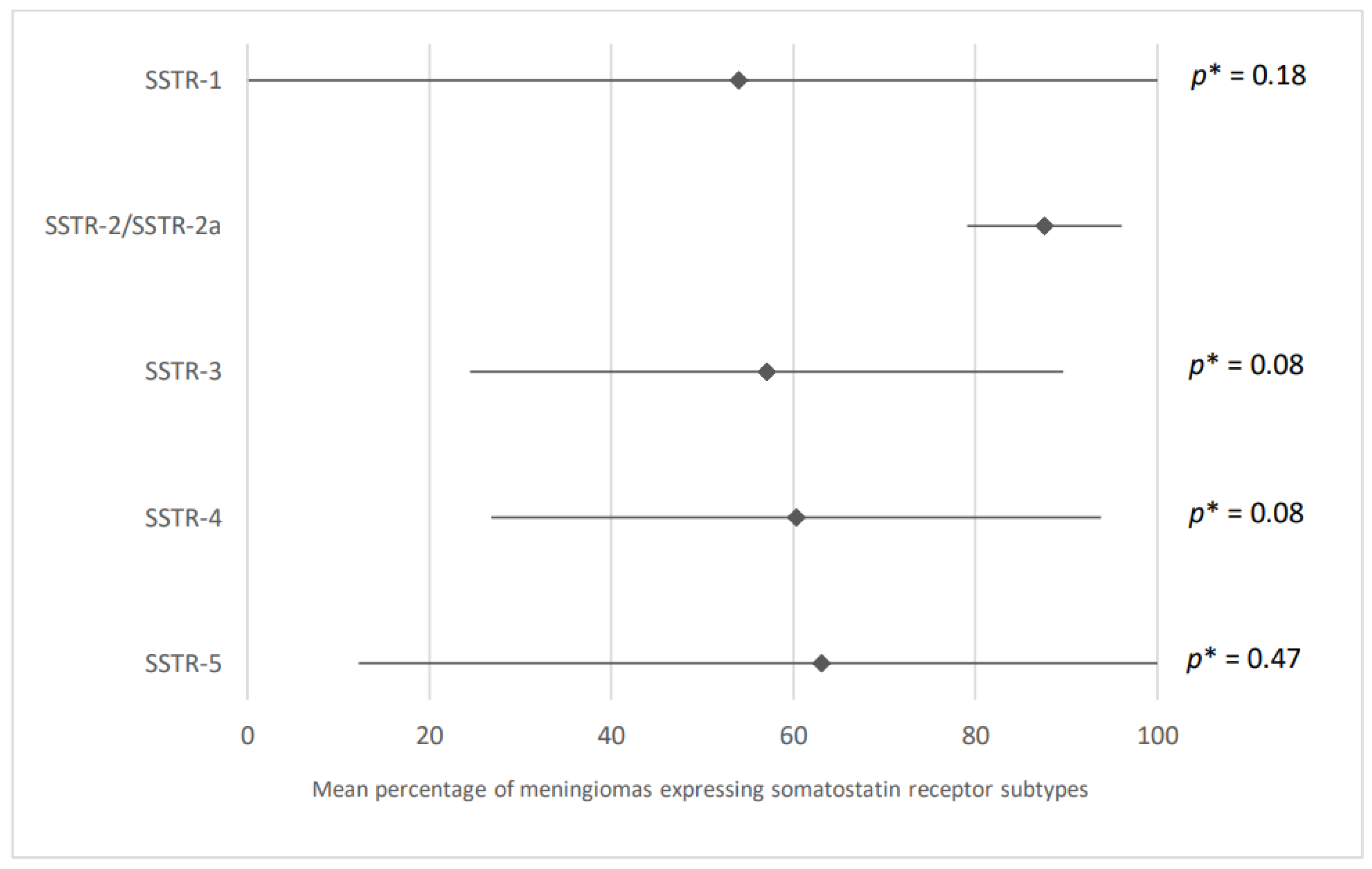
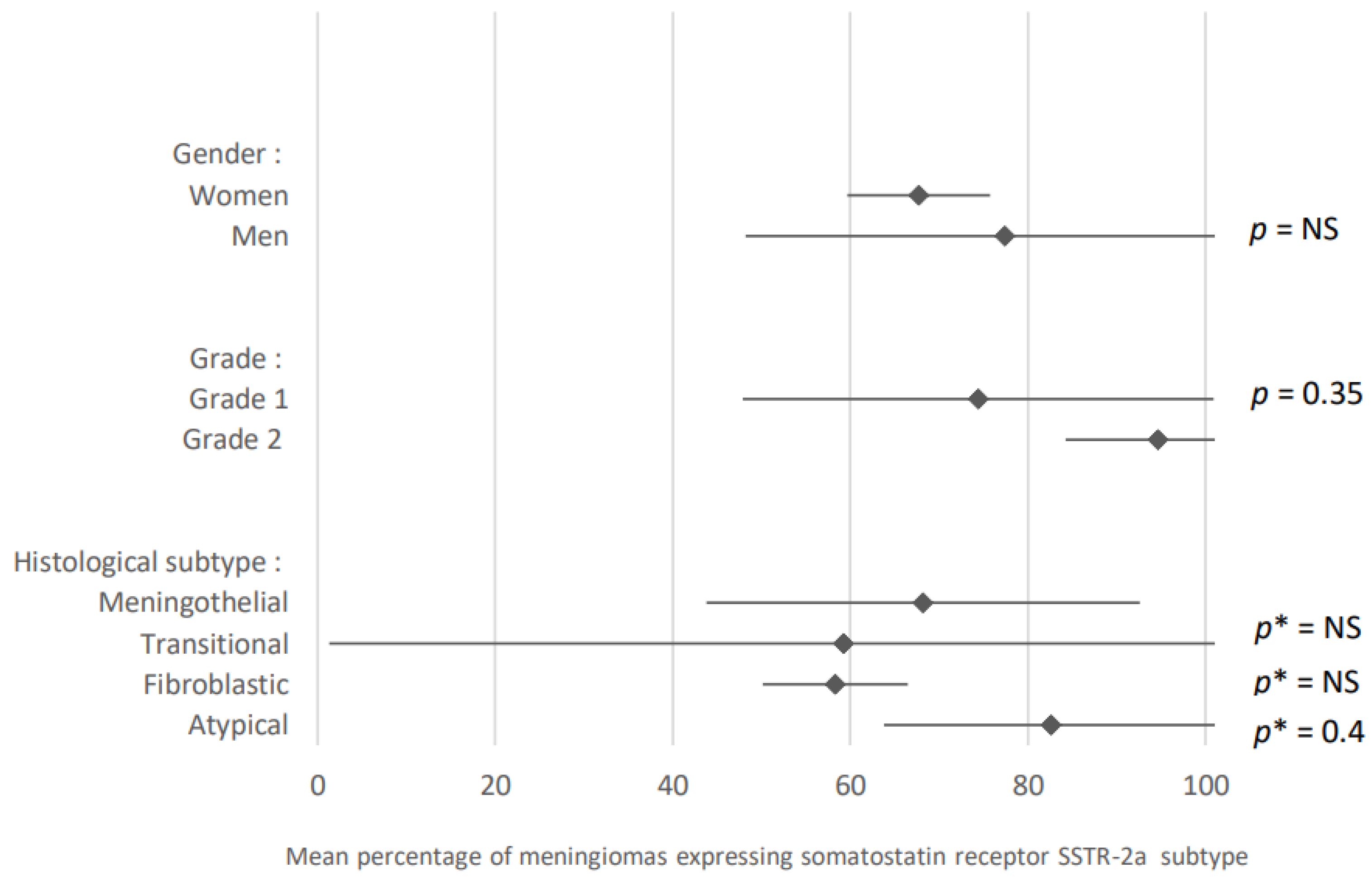
3.5. Focus on Somatostatin Receptor Expression in Meningiomas
4. Discussion
5. Limitations of This Review
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A. PRISMA Flow Diagram

References
- Ostrom, Q.T.; Gittleman, H.; Fulop, J.; Liu, M.; Blanda, R.; Kromer, C.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008–2012. Neuro Oncol. 2015, 17 (Suppl. S4), iv1–iv62. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A Summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Claus, E.B.; Bondy, M.L.; Schildkraut, J.M.; Wiemels, J.L.; Wrensch, M.; Black, P.M. Epidemiology of Intracranial Meningioma. Neurosurgery 2005, 57, 1088–1095. [Google Scholar] [CrossRef]
- Wiemels, J.; Wrensch, M.; Claus, E.B. Epidemiology and Etiology of Meningioma. J. Neurooncol. 2010, 99, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Michelsen, J.J.; New, P.F. Brain Tumour and Pregnancy. J. Neurol. Neurosurg. Psychiatry 1969, 32, 305–307. [Google Scholar] [CrossRef]
- Chakravarthy, V.; Kaplan, B.; Gospodarev, V.; Myers, H.; De Los Reyes, K.; Achiriloaie, A. Houdini Tumor: Case Report and Literature Review of Pregnancy-Associated Meningioma. World Neurosurg. 2018, 114, e1261–e1265. [Google Scholar] [CrossRef]
- Custer, B.S.; Koepsell, T.D.; Mueller, B.A. The Association between Breast Carcinoma and Meningioma in Women. Cancer 2002, 94, 1626–1635. [Google Scholar] [CrossRef]
- Kuroi, Y.; Matsumoto, K.; Shibuya, M.; Kasuya, H. Progesterone Receptor Is Responsible for Benign Biology of Skull Base Meningioma. World Neurosurg. 2018, 118, e918–e924. [Google Scholar] [CrossRef]
- Verheijen, F.M.; Sprong, M.; Jacobs, H.M.; Donker, G.H.; Amelink, G.J.; Thijssen, J.H.; Blankenstein, M.A. Progesterone Receptor Isoform Expression in Human Meningiomas. Eur. J. Cancer 2001, 37, 1488–1495. [Google Scholar] [CrossRef]
- Hsu, D.W.; Efird, J.T.; Hedley-Whyte, E.T. Progesterone and Estrogen Receptors in Meningiomas: Prognostic Considerations. J. Neurosurg. 1997, 86, 113–120. [Google Scholar] [CrossRef]
- Roser, F.; Nakamura, M.; Bellinzona, M.; Rosahl, S.K.; Ostertag, H.; Samii, M. The Prognostic Value of Progesterone Receptor Status in Meningiomas. J. Clin. Pathol. 2004, 57, 1033–1037. [Google Scholar] [CrossRef]
- Carroll, R.S.; Zhang, J.; Black, P.M. Expression of Estrogen Receptors Alpha and Beta in Human Meningiomas. J. Neurooncol. 1999, 42, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, K.; Salminen, T.; Raitanen, J.; Auvinen, A.; Isola, J.; Haapasalo, H. Female Predominance in Meningiomas Can Not Be Explained by Differences in Progesterone, Estrogen, or Androgen Receptor Expression. J. Neurooncol. 2006, 80, 1–7. [Google Scholar] [CrossRef]
- Omulecka, A.; Papierz, W.; Nawrocka-Kunecka, A.; Lewy-Trenda, I. Immunohistochemical Expression of Progesterone and Estrogen Receptors in Meningiomas. Folia Neuropathol. 2006, 44, 111–115. [Google Scholar]
- Pravdenkova, S.; Al-Mefty, O.; Sawyer, J.; Husain, M. Progesterone and Estrogen Receptors: Opposing Prognostic Indicators in Meningiomas. J. Neurosurg. 2006, 105, 163–173. [Google Scholar] [CrossRef]
- Hua, L.; Zhu, H.; Li, J.; Tang, H.; Kuang, D.; Wang, Y.; Tang, F.; Chen, X.; Zhou, L.; Xie, Q.; et al. Prognostic Value of Estrogen Receptor in WHO Grade III Meningioma: A Long-Term Follow-up Study from a Single Institution. J. Neurosurg. 2018, 128, 1698–1706. [Google Scholar] [CrossRef]
- Portet, S.; Banor, T.; Bousquet, J.; Simonneau, A.; Flores, M.; Ingrand, P.; Milin, S.; Karayan-Tapon, L.; Bataille, B. New Insights into Expression of Hormonal Receptors by Meningiomas. World Neurosurg. 2020, 140, e87–e96. [Google Scholar] [CrossRef] [PubMed]
- Lesch, K.P.; Engl, H.G.; Gross, S. Androgen Receptor Binding Activity in Meningiomas. Surg. Neurol. 1987, 28, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Weill, A.; Nguyen, P.; Labidi, M.; Cadier, B.; Passeri, T.; Duranteau, L.; Bernat, A.-L.; Yoldjian, I.; Fontanel, S.; Froelich, S.; et al. Use of High Dose Cyproterone Acetate and Risk of Intracranial Meningioma in Women: Cohort Study. BMJ 2021, 372, n37. [Google Scholar] [CrossRef]
- Devalckeneer, A.; Aboukais, R.; Bourgeois, P.; De Witte, O.; Racape, J.; Caron, S.; Perbet, R.; Maurage, C.-A.; Lejeune, J.-P. Preliminary Report of Patients with Meningiomas Exposed to Cyproterone Acetate, Nomegestrol Acetate and Chlormadinone Acetate-Monocentric Ongoing Study on Progestin Related Meningiomas. Clin. Neurol. Neurosurg. 2021, 210, 106959. [Google Scholar] [CrossRef]
- Ji, Y.; Rankin, C.; Grunberg, S.; Sherrod, A.E.; Ahmadi, J.; Townsend, J.J.; Feun, L.G.; Fredericks, R.K.; Russell, C.A.; Kabbinavar, F.F.; et al. Double-Blind Phase III Randomized Trial of the Antiprogestin Agent Mifepristone in the Treatment of Unresectable Meningioma: SWOG S9005. J. Clin. Oncol. 2015, 33, 4093–4098. [Google Scholar] [CrossRef]
- Champeaux-Depond, C.; Weller, J. Tamoxifen. A Treatment for Meningioma? Cancer Treat. Res. Commun. 2021, 27, 100343. [Google Scholar] [CrossRef]
- Behling, F.; Fodi, C.; Skardelly, M.; Renovanz, M.; Castaneda, S.; Tabatabai, G.; Honegger, J.; Tatagiba, M.; Schittenhelm, J. Differences in the Expression of SSTR1-5 in Meningiomas and Its Therapeutic Potential. Neurosurg. Rev. 2022, 45, 467–478. [Google Scholar] [CrossRef]
- Boulagnon-Rombi, C.; Fleury, C.; Fichel, C.; Lefour, S.; Marchal Bressenot, A.; Gauchotte, G. Immunohistochemical Approach to the Differential Diagnosis of Meningiomas and Their Mimics. J. Neuropathol. Exp. Neurol. 2017, 76, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.R.; Kimmel, D.W.; Burch, P.A.; Cascino, T.L.; Giannini, C.; Wu, W.; Buckner, J.C. Phase II Study of Subcutaneous Octreotide in Adults with Recurrent or Progressive Meningioma and Meningeal Hemangiopericytoma. Neuro Oncol. 2011, 13, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Abdelzaher, E.; El-Gendi, S.M.; Yehya, A.; Gowil, A.G. Recurrence of Benign Meningiomas: Predictive Value of Proliferative Index, BCL2, P53, Hormonal Receptors and HER2 Expression. Br. J. Neurosurg. 2011, 25, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Agaimy, A.; Buslei, R.; Coras, R.; Rubin, B.P.; Mentzel, T. Comparative Study of Soft Tissue Perineurioma and Meningioma Using a Five-Marker Immunohistochemical Panel. Histopathology 2014, 65, 60–70. [Google Scholar] [CrossRef]
- Barresi, V.; Alafaci, C.; Caffo, M.; Barresi, G.; Tuccari, G. Clinicopathological Characteristics, Hormone Receptor Status and Matrix Metallo-Proteinase-9 (MMP-9) Immunohistochemical Expression in Spinal Meningiomas. Pathol. Res. Pract. 2012, 208, 350–355. [Google Scholar] [CrossRef]
- Battu, S.; Kumar, A.; Pathak, P.; Purkait, S.; Dhawan, L.; Sharma, M.C.; Suri, A.; Singh, M.; Sarkar, C.; Suri, V. Clinicopathological and Molecular Characteristics of Pediatric Meningiomas. Neuropathology 2018, 38, 22–33. [Google Scholar] [CrossRef]
- Baxter, D.S.; Orrego, A.; Rosenfeld, J.V.; Mathiesen, T. An Audit of Immunohistochemical Marker Patterns in Meningioma. J. Clin. Neurosci. 2014, 21, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Bouillot, P.; Pellissier, J.F.; Devictor, B.; Graziani, N.; Bianco, N.; Grisoli, F.; Figarella-Branger, D. Quantitative Imaging of Estrogen and Progesterone Receptors, Estrogen-Regulated Protein, and Growth Fraction: Immunocytochemical Assays in 52 Meningiomas. Correlation with Clinical and Morphological Data. J. Neurosurg. 1994, 81, 765–773. [Google Scholar] [CrossRef]
- Bozdağ, M.; Er, A.; Ekmekçi, S. Association of Apparent Diffusion Coefficient with Ki-67 Proliferation Index, Progesterone-Receptor Status and Various Histopathological Parameters, and Its Utility in Predicting the High Grade in Meningiomas. Acta Radiol. 2021, 62, 401–413. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, C.; Camisa, R.; Nizzoli, R.; Manotti, L.; Guazzi, A.; Naldi, N.; Mazza, S.; Nizzoli, V.; Cocconi, G. Estrogen and Progesterone Receptors in Human Meningiomas: Biochemical and Immunocytochemical Evaluation. Surg. Neurol. 1995, 43, 230–233, discussion 234. [Google Scholar] [CrossRef] [PubMed]
- Brandis, A.; Mirzai, S.; Tatagiba, M.; Walter, G.F.; Samii, M.; Ostertag, H. Immunohistochemical Detection of Female Sex Hormone Receptors in Meningiomas: Correlation with Clinical and Histological Features. Neurosurgery 1993, 33, 212–217, discussion 217–218. [Google Scholar] [CrossRef] [PubMed]
- Buhl, R.; Hugo, H.H.; Mihajlovic, Z.; Mehdorn, H.M. Secretory Meningiomas: Clinical and Immunohistochemical Observations. Neurosurgery 2001, 48, 297–301, discussion 301–302. [Google Scholar] [CrossRef]
- Carroll, R.S.; Brown, M.; Zhang, J.; DiRenzo, J.; Font De Mora, J.; Black, P.M. Expression of a Subset of Steroid Receptor Cofactors Is Associated with Progesterone Receptor Expression in Meningiomas. Clin. Cancer Res. 2000, 6, 3570–3575. [Google Scholar] [PubMed]
- Carroll, R.S.; Glowacka, D.; Dashner, K.; Black, P.M. Progesterone Receptor Expression in Meningiomas. Cancer Res. 1993, 53, 1312–1316. [Google Scholar]
- Carroll, R.S.; Zhang, J.; Dashner, K.; Sar, M.; Wilson, E.M.; Black, P.M. Androgen Receptor Expression in Meningiomas. J. Neurosurg. 1995, 82, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Claus, E.B.; Park, P.J.; Carroll, R.; Chan, J.; Black, P.M. Specific Genes Expressed in Association with Progesterone Receptors in Meningioma. Cancer Res. 2008, 68, 314–322. [Google Scholar] [CrossRef]
- de Carvalho, G.T.C.; da Silva-Martins, W.C.; de Magalhães, K.C.S.F.; Nunes, C.B.; Soares, A.N.; Tafuri, L.S. de A.; Simões, R.T. Recurrence/Regrowth in Grade I Meningioma: How to Predict? Front. Oncol. 2020, 10, 1144. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Malagón, H.R.; Serrano-Arévalo, M.L.; Maldonado, J.; Chávez, J.; Toussaint-Caire, S.; de Almeida, O.P.D.; Lino-Silva, L.S. Perineurioma versus Meningioma. A Multi-Institutional Immunohistochemical and Ultrastructural StudY. Ultrastruct. Pathol. 2021, 45, 71–77. [Google Scholar] [CrossRef]
- Giraldi, L.; Lauridsen, E.K.; Maier, A.D.; Hansen, J.V.; Broholm, H.; Fugleholm, K.; Scheie, D.; Munch, T.N. Pathologic Characteristics of Pregnancy-Related Meningiomas. Cancers 2021, 13, 3879. [Google Scholar] [CrossRef] [PubMed]
- Guevara, P.; Escobar-Arriaga, E.; Saavedra-Perez, D.; Martinez-Rumayor, A.; Flores-Estrada, D.; Rembao, D.; Calderon, A.; Sotelo, J.; Arrieta, O. Angiogenesis and Expression of Estrogen and Progesterone Receptors as Predictive Factors for Recurrence of Meningioma. J. Neurooncol. 2010, 98, 379–384. [Google Scholar] [CrossRef]
- Gursan, N.; Gundogdu, C.; Albayrak, A.; Kabalar, M.E. Immunohistochemical Detection of Progesterone Receptors and the Correlation with Ki-67 Labeling Indices in Paraffin-Embedded Sections of Meningiomas. Int. J. Neurosci. 2002, 112, 463–470. [Google Scholar] [CrossRef]
- Hatiboglu, M.A.; Cosar, M.; Iplikcioglu, A.C.; Ozcan, D. Sex Steroid and Epidermal Growth Factor Profile of Giant Meningiomas Associated with Pregnancy. Surg. Neurol. 2008, 69, 356–362, discussion 362–363. [Google Scholar] [CrossRef] [PubMed]
- Heß, K.; Spille, D.C.; Wagner, A.; Stummer, W.; Paulus, W.; Brokinkel, B. Letter: Brain Invasion in Meningiomas-Sex-Associated Differences Are Not Related to Estrogen- and Progesterone Receptor Expression. Neurosurgery 2017, 81, E25–E27. [Google Scholar] [CrossRef] [PubMed]
- Hirota, Y.; Tachibana, O.; Uchiyama, N.; Hayashi, Y.; Nakada, M.; Kita, D.; Watanabe, T.; Higashi, R.; Hamada, J.; Hayashi, Y. Gonadotropin-Releasing Hormone (GnRH) and Its Receptor in Human Meningiomas. Clin. Neurol. Neurosurg. 2009, 111, 127–133. [Google Scholar] [CrossRef]
- Ichimura, S.; Ohara, K.; Kono, M.; Mizutani, K.; Kitamura, Y.; Saga, I.; Kanai, R.; Akiyama, T.; Toda, M.; Kohno, M.; et al. Molecular Investigation of Brain Tumors Progressing during Pregnancy or Postpartum Period: The Association between Tumor Type, Their Receptors, and the Timing of Presentation. Clin. Neurol. Neurosurg. 2021, 207, 106720. [Google Scholar] [CrossRef]
- Iplikcioglu, A.C.; Hatiboglu, M.A.; Ozek, E.; Ozcan, D. Is Progesteron Receptor Status Really a Prognostic Factor for Intracranial Meningiomas? Clin. Neurol. Neurosurg. 2014, 124, 119–122. [Google Scholar] [CrossRef]
- Khalid, H. Immunohistochemical Study of Estrogen Receptor-Related Antigen, Progesterone and Estrogen Receptors in Human Intracranial Meningiomas. Cancer 1994, 74, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidou, A.E.; Korkolopoulou, P.; Mahera, H.; Kotsiakis, X.; Hranioti, S.; Eftychiadis, C.; Patsouris, E. Hormone Receptors in Non-Malignant Meningiomas Correlate with Apoptosis, Cell Proliferation and Recurrence-Free Survival. Histopathology 2003, 43, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Leães, C.G.S.; Meurer, R.T.; Coutinho, L.B.; Ferreira, N.P.; Pereira-Lima, J.F.S.; da Costa Oliveira, M. Immunohistochemical Expression of Aromatase and Estrogen, Androgen and Progesterone Receptors in Normal and Neoplastic Human Meningeal Cells. Neuropathology 2010, 30, 44–49. [Google Scholar] [CrossRef]
- Li, Q.; Coulson, H.; Klaassen, Z.; Sharma, S.; Ramalingam, P.; Moses, K.A.; Terris, M.K. Emerging Association between Androgen Deprivation Therapy and Male Meningioma: Significant Expression of Luteinizing Hormone-Releasing Hormone Receptor in Male Meningioma. Prostate Cancer Prostatic Dis. 2013, 16, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Lusis, E.A.; Chicoine, M.R.; Perry, A. High Throughput Screening of Meningioma Biomarkers Using a Tissue Microarray. J. Neuro-Oncol. 2005, 73, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Lusis, E.A.; Scheithauer, B.W.; Yachnis, A.T.; Fischer, B.R.; Chicoine, M.R.; Paulus, W.; Perry, A. Meningiomas in Pregnancy: A Clinicopathologic Study of 17 Cases. Neurosurgery 2012, 71, 951–961. [Google Scholar] [CrossRef]
- Maiuri, F.; Mariniello, G.; Somma, T.; Guadagno, E.; Corvino, S.; Pagano, S.; Orlando, V.; Del Basso De Caro, M. Meningiomas in Premenopausal Women: Role of the Hormone Related Conditions. Front. Oncol. 2020, 10, 556701. [Google Scholar] [CrossRef]
- Mezmezian, M.B.; B Carassai, M.; Dopazo, V.; Deforel, M.L.; Puzzo, M.Á. Immunohistochemical Expression of Progesterone Receptors in Nonmeningothelial Central Nervous System Tumors. Appl. Immunohistochem. Mol. Morphol. 2017, 25, 439–444. [Google Scholar] [CrossRef]
- Mnango, L.; Mwakimonga, A.; Ngaiza, A.I.; Yahaya, J.J.; Vuhahula, E.; Mwakigonja, A.R. Expression of Progesterone Receptor and Its Association with Clinicopathological Characteristics in Meningiomas: A Cross-Sectional Study. World Neurosurg. X 2021, 12, 100111. [Google Scholar] [CrossRef]
- Nagashima, G.; Aoyagi, M.; Wakimoto, H.; Tamaki, M.; Ohno, K.; Hirakawa, K. Immunohistochemical Detection of Progesterone Receptors and the Correlation with Ki-67 Labeling Indices in Paraffin-Embedded Sections of Meningiomas. Neurosurgery 1995, 37, 478–482, discussion 483. [Google Scholar] [CrossRef]
- Perrot-Applanat, M.; Groyer-Picard, M.T.; Kujas, M. Immunocytochemical Study of Progesterone Receptor in Human Meningioma. Acta Neurochir. 1992, 115, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.; Cai, D.X.; Scheithauer, B.W.; Swanson, P.E.; Lohse, C.M.; Newsham, I.F.; Weaver, A.; Gutmann, D.H. Merlin, DAL-1, and Progesterone Receptor Expression in Clinicopathologic Subsets of Meningioma: A Correlative Immunohistochemical Study of 175 Cases. J. Neuropathol. Exp. Neurol. 2000, 59, 872–879. [Google Scholar] [CrossRef] [Green Version]
- Probst-Cousin, S.; Villagran-Lillo, R.; Lahl, R.; Bergmann, M.; Schmid, K.W.; Gullotta, F. Secretory Meningioma: Clinical, Histologic, and Immunohistochemical Findings in 31 Cases. Cancer 1997, 79, 2003–2015. [Google Scholar] [CrossRef]
- Schlegel, J.; Ullrich, B.; Stumm, G.; Gass, P.; Harwerth, I.M.; Hynes, N.E.; Kiessling, M. Expression of the C-ErbB-2-Encoded Oncoprotein and Progesterone Receptor in Human Meningiomas. Acta Neuropathol. 1993, 86, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Shahin, M.N.; Magill, S.T.; Dalle Ore, C.L.; Viner, J.A.; Peters, P.N.; Solomon, D.A.; McDermott, M.W. Fertility Treatment Is Associated with Multiple Meningiomas and Younger Age at Diagnosis. J. Neurooncol. 2019, 143, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Quiñones-Hinojosa, A.; Harmon-Smith, M.; Bollen, A.W.; McDermott, M.W. Sex Steroid and Growth Factor Profile of a Meningioma Associated with Pregnancy. Can. J. Neurol. Sci. 2005, 32, 122–127. [Google Scholar] [CrossRef]
- Takei, H.; Buckleair, L.W.; Powell, S.Z. Immunohistochemical Expression of Apoptosis Regulating Proteins and Sex Hormone Receptors in Meningiomas. Neuropathology 2008, 28, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Liang, G.; Li, Z.; Wang, Y.; Wu, A.; Wang, H.; Lu, Y.; Liu, Z.; Hu, G. Clinical Features and Immunohistochemical Expression Levels of Androgen, Estrogen, Progesterone and Ki-67 Receptors in Relationship with Gross-Total Resected Meningiomas Relapse. Br. J. Neurosurg. 2012, 26, 700–704. [Google Scholar] [CrossRef]
- Telugu, R.B.; Chowhan, A.K.; Rukmangadha, N.; Patnayak, R.; Phaneendra, B.V.; Mowliswara Prasad, B.C.; Reddy, M.K. Estrogen and Progesterone Receptor in Meningiomas: An Immunohistochemical Analysis. J. Cancer Res. Ther. 2020, 16, 1482–1487. [Google Scholar] [CrossRef]
- Ülgen, E.; Bektaşoğlu, P.K.; Sav, M.A.; Can, Ö.; Danyeli, A.E.; Hızal, D.B.; Pamir, M.N.; Özduman, K. Meningiomas Display a Specific Immunoexpression Pattern in a Rostrocaudal Gradient: An Analysis of 366 Patients. World Neurosurg. 2019, 123, e520–e535. [Google Scholar] [CrossRef]
- Wolfsberger, S.; Doostkam, S.; Boecher-Schwarz, H.-G.; Roessler, K.; van Trotsenburg, M.; Hainfellner, J.A.; Knosp, E. Progesterone-Receptor Index in Meningiomas: Correlation with Clinico-Pathological Parameters and Review of the Literature. Neurosurg. Rev. 2004, 27, 238–245. [Google Scholar] [CrossRef]
- Schulz, S.; Pauli, S.; Schulz, S.; Händel, M.; Dietzmann, K.; Firsching, R.; Höllt, V. Immunohistochemical Determination of Five Somatostatin Receptors in Meningioma Reveals Frequent Overexpression of Somatostatin Receptor Subtype Sst2A. Clin. Cancer Res. 2000, 6, 1865–1874. [Google Scholar] [PubMed]
- Menke, J.R.; Raleigh, D.R.; Gown, A.M.; Thomas, S.; Perry, A.; Tihan, T. Somatostatin Receptor 2a Is a More Sensitive Diagnostic Marker of Meningioma than Epithelial Membrane Antigen. Acta Neuropathol. 2015, 130, 441–443. [Google Scholar] [CrossRef] [PubMed]
- Körner, M.; Eltschinger, V.; Waser, B.; Schonbrunn, A.; Reubi, J.C. Value of Immunohistochemistry for Somatostatin Receptor Subtype Sst2A in Cancer Tissues: Lessons from the Comparison of Anti-Sst2A Antibodies with Somatostatin Receptor Autoradiography. Am. J. Surg. Pathol. 2005, 29, 1642–1651. [Google Scholar] [CrossRef] [PubMed]
- Lazow, M.A.; Fuller, C.; Trout, A.T.; Stanek, J.R.; Reuss, J.; Turpin, B.K.; Szabo, S.; Salloum, R. Immunohistochemical Assessment and Clinical, Histopathologic, and Molecular Correlates of Membranous Somatostatin Type-2A Receptor Expression in High-Risk Pediatric Central Nervous System Tumors. Front. Oncol. 2022, 12, 996489. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Silva, C.B.; Ongaratti, B.R.; Trott, G.; Haag, T.; Ferreira, N.P.; Leães, C.G.S.; Pereira-Lima, J.F.S.; da Costa Oliveira, M. Expression of Somatostatin Receptors (SSTR1-SSTR5) in Meningiomas and Its Clinicopathological Significance. Int. J. Clin. Exp. Pathol. 2015, 8, 13185–13192. [Google Scholar]
- Barresi, V.; Alafaci, C.; Salpietro, F.; Tuccari, G. Sstr2A immunohistochemical expression in human meningiomas: Is there a correlation with the histological grade, proliferation or microvessel density? Oncol. Rep. 2008, 20, 485–492. [Google Scholar] [CrossRef]
- Ottawa Hospital Research Institute. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 8 December 2022).
- Samoyeau, T.; Provost, C.; Roux, A.; Legrand, L.; Dezamis, E.; Plu-Bureau, G.; Pallud, J.; Oppenheim, C.; Benzakoun, J. Meningioma in Patients Exposed to Progestin Drugs: Results from a Real-Life Screening Program. J. Neurooncol. 2022, 160, 127–136. [Google Scholar] [CrossRef]
- Giraldi, L.; Hansen, J.V.; Wohlfahrt, J.; Melbye, M.; Fugleholm, K.; Munch, T.N. Male Hormone-Interfering Drugs and Meningioma Development. Neurooncol. Adv. 2019, 1, vdz046. [Google Scholar] [CrossRef]
- Apra, C.; Peyre, M.; Kalamarides, M. Current Treatment Options for Meningioma. Expert Rev. Neurother. 2018, 18, 241–249. [Google Scholar] [CrossRef]
- Maggio, I.; Franceschi, E.; Tosoni, A.; Nunno, V.D.; Gatto, L.; Lodi, R.; Brandes, A.A. Meningioma: Not Always a Benign Tumor. A Review of Advances in the Treatment of Meningiomas. CNS Oncol. 2021, 10, CNS72. [Google Scholar] [CrossRef]
- Nunes, F.P.; Merker, V.L.; Jennings, D.; Caruso, P.A.; di Tomaso, E.; Muzikansky, A.; Barker, F.G.; Stemmer-Rachamimov, A.; Plotkin, S.R. Bevacizumab Treatment for Meningiomas in NF2: A Retrospective Analysis of 15 Patients. PLoS ONE 2013, 8, e59941. [Google Scholar] [CrossRef]
- Shih, K.C.; Chowdhary, S.; Rosenblatt, P.; Weir, A.B.; Shepard, G.C.; Williams, J.T.; Shastry, M.; Burris, H.A.; Hainsworth, J.D. A Phase II Trial of Bevacizumab and Everolimus as Treatment for Patients with Refractory, Progressive Intracranial Meningioma. J. Neurooncol. 2016, 129, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Miyagishima, D.F.; Moliterno, J.; Claus, E.; Günel, M. Hormone Therapies in Meningioma—Where Are We? J. Neurooncol. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Palmisciano, P.; Watanabe, G.; Conching, A.; Ogasawara, C.; Ferini, G.; Bin-Alamer, O.; Haider, A.S.; Sabini, M.G.; Cuttone, G.; Cosentino, S.; et al. The Role of [68Ga]Ga-DOTA-SSTR PET Radiotracers in Brain Tumors: A Systematic Review of the Literature and Ongoing Clinical Trials. Cancers 2022, 14, 2925. [Google Scholar] [CrossRef]
- Pelak, M.J.; Flechl, B.; Mumot, M.; Galalae, R.; Tubin, S.; Hug, E.; Lütgendorf-Caucig, C. The Value of SSTR2 Receptor-Targeted PET/CT in Proton Irradiation of Grade I Meningioma. Cancers 2021, 13, 4707. [Google Scholar] [CrossRef] [PubMed]














Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agopiantz, M.; Carnot, M.; Denis, C.; Martin, E.; Gauchotte, G. Hormone Receptor Expression in Meningiomas: A Systematic Review. Cancers 2023, 15, 980. https://doi.org/10.3390/cancers15030980
Agopiantz M, Carnot M, Denis C, Martin E, Gauchotte G. Hormone Receptor Expression in Meningiomas: A Systematic Review. Cancers. 2023; 15(3):980. https://doi.org/10.3390/cancers15030980
Chicago/Turabian StyleAgopiantz, Mikaël, Mélanie Carnot, Constance Denis, Elena Martin, and Guillaume Gauchotte. 2023. "Hormone Receptor Expression in Meningiomas: A Systematic Review" Cancers 15, no. 3: 980. https://doi.org/10.3390/cancers15030980