


The Risk of Endometrial Cancer and Uterine Sarcoma Following Endometriosis or Pelvic Inflammatory Disease
 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Identification of Study Cohort and Exclusion Criteria
2.3. Study Events and Covariates and Primary Outcomes
2.4. Propensity Score Matching
2.5. Sensitivity and Subgroup Analyses
2.6. Statistical Analysis
3. Results
3.1. Baseline Demographics and Comorbidity Characteristics among Study Groups
3.2. Uterine Corpus Cancer Risk Differences and Ratios among Study Groups
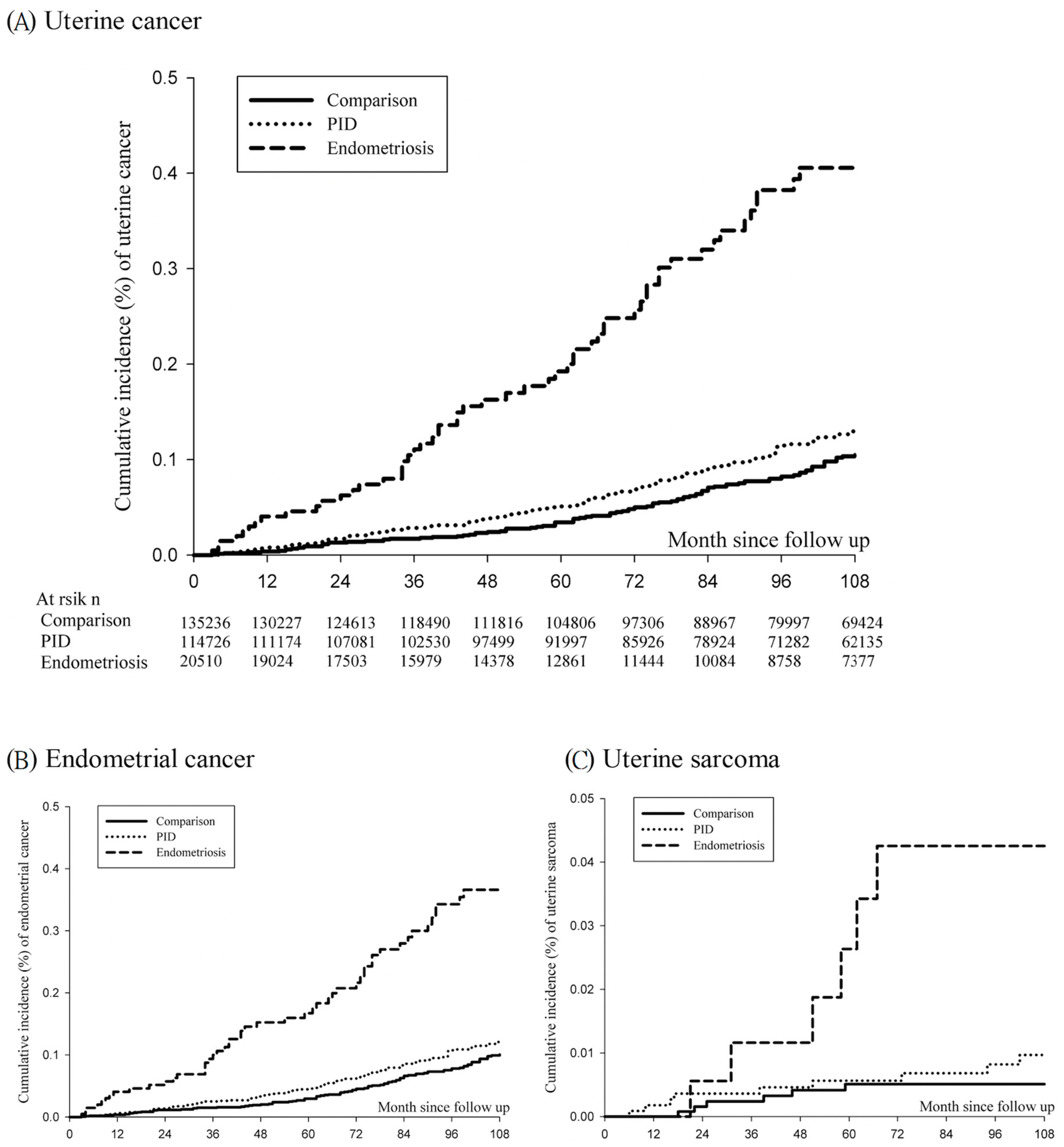
3.3. Cumulative Incidence of Uterine Cancer
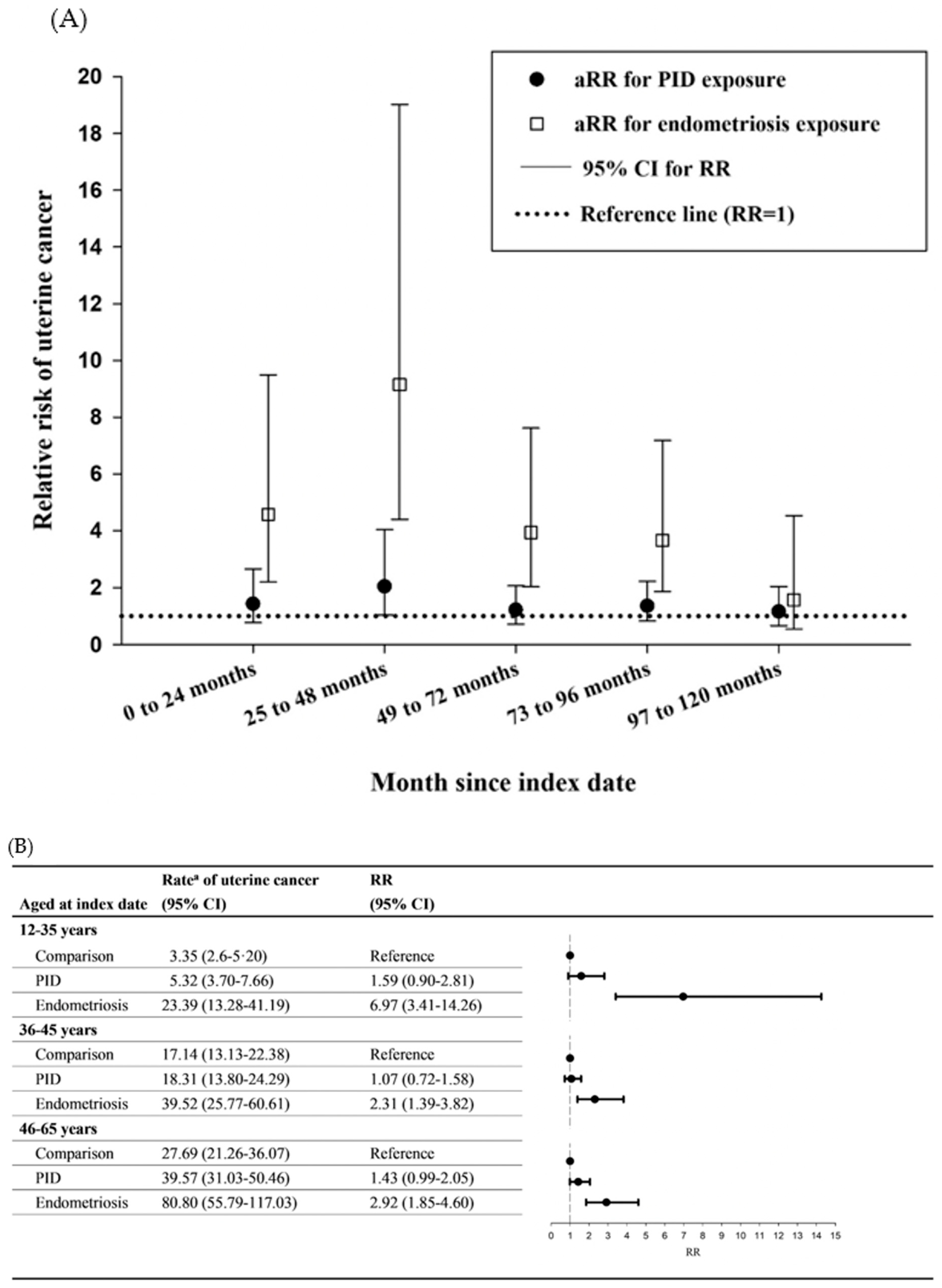
3.4. Sensitivity and Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malvezzi, H.; Marengo, E.B.; Podgaec, S.; Piccinato, C.A. Endometriosis: Current challenges in modeling a multifactorial disease of unknown etiology. J. Transl. Med. 2020, 18, 311. [Google Scholar] [PubMed]
- Shafrir, A.L.; Farland, L.V.; Shah, D.K.; Harris, H.R.; Kvaskoff, M.; Zondervan, K.; Missmer, S.A. Risk for and consequences of endometriosis: A critical epidemiologic review. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 51, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ciou, H.-H.; Lee, T.-H.; Wang, H.-C.; Ding, Y.-R.; Tseng, C.-J.; Wang, P.-H.; Tsai, M.-H.; Tzeng, S.-L. Repurposing gestrinone for tumor suppressor through P21 reduction regulated by JNK in gynecological cancer. Transl. Res. 2022, 243, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Reis, F.M.; Petraglia, F.; Taylor, R.N. Endometriosis: Hormone regulation and clinical consequences of chemotaxis and apoptosis. Hum. Reprod. Update 2013, 19, 406–418. [Google Scholar] [PubMed] [Green Version]
- Montoya-Estrada, A.; Coria-Garcia, C.F.; Cruz-Orozco, O.P.; Aguayo-Gonzalez, P.; Torres-Ramos, Y.D.; Flores-Herrera, H.; Hicks, J.J.; Medina-Navarro, R.; Guzman-Grenfell, A.M. Increased systemic and peritoneal oxidative stress biomarkers in endometriosis are not related to retrograde menstruation. Redox Rep. 2019, 24, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Fuseya, C.; Horiuchi, A.; Hayashi, A.; Suzuki, A.; Miyamoto, T.; Hayashi, T.; Shiozawa, T. Involvement of pelvic inflammation-related mismatch repair abnormalities and microsatellite instability in the malignant transformation of ovarian endometriosis. Hum. Pathol. 2012, 43, 1964–1972. [Google Scholar] [CrossRef] [PubMed]
- Brunham, R.C.; Gottlieb, S.L.; Paavonen, J. Pelvic inflammatory disease. N. Engl. J. Med. 2015, 372, 2039–2048. [Google Scholar] [CrossRef] [PubMed]
- Zucchetto, A.; Serraino, D.; Polesel, J.; Negri, E.; De Paoli, A.; Dal Maso, L.; Montella, M.; La Vecchia, C.; Franceschi, S.; Talamini, R. Hormone-related factors and gynecological conditions in relation to endometrial cancer risk. Eur. J. Cancer Prev. 2009, 18, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Marquardt, R.M.; Kim, T.H.; Shin, J.H.; Jeong, J.W. Progesterone and Estrogen Signaling in the Endometrium: What Goes Wrong in Endometriosis? Int. J. Mol. Sci. 2019, 20, 3822. [Google Scholar] [CrossRef]
- Maeda, H.; Akaike, T. Nitric oxide and oxygen radicals in infection, inflammation, and cancer. Biochemistry 1998, 63, 854–865. [Google Scholar]
- Landskron, G.; De la Fuente, M.; Thuwajit, P.; Thuwajit, C.; Hermoso, M.A. Chronic inflammation and cytokines in the tumor microenvironment. J. Immunol. Res. 2014, 2014, 149185. [Google Scholar]
- Modugno, F.; Ness, R.B.; Chen, C.; Weiss, N.S. Inflammation and endometrial cancer: A hypothesis. Cancer Epidemiol. Biomarkers Prev. 2005, 14, 2840–2847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balkwill, F.; Coussens, L.M. Cancer: An inflammatory link. Nature 2004, 431, 405–406. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. Cancer registry annual report, Taiwan, ROC. In Cancer Registry Annual Report, Taiwan; Ministry of Health and Welfare: Taiwan, China, 2020. [Google Scholar]
- Bafligil, C.; Thompson, D.J.; Lophatananon, A.; Smith, M.J.; Ryan, N.A.; Naqvi, A.; Evans, D.G.; Crosbie, E.J. Association between genetic polymorphisms and endometrial cancer risk: A systematic review. J. Med. Genet. 2020, 57, 591–600. [Google Scholar] [CrossRef]
- Tzur, T.; Kessous, R.; Weintraub, A.Y. Current strategies in the diagnosis of endometrial cancer. Arch. Gynecol. Obstet. 2017, 296, 5–14. [Google Scholar]
- Mogensen, J.B.; Kjaer, S.K.; Mellemkjaer, L.; Jensen, A. Endometriosis and risks for ovarian, endometrial and breast cancers: A nationwide cohort study. Gynecol. Oncol. 2016, 143, 87–92. [Google Scholar] [CrossRef]
- Rowlands, I.J.; Nagle, C.M.; Spurdle, A.B.; Webb, P.M.; Australian National Endometrial Cancer Study; Australian Ovarian Cancer Study. Gynecological conditions and the risk of endometrial cancer. Gynecol. Oncol. 2011, 123, 537–541. [Google Scholar] [CrossRef]
- Kok, V.C.; Tsai, H.J.; Su, C.F.; Lee, C.K. The Risks for Ovarian, Endometrial, Breast, Colorectal, and Other Cancers in Women With Newly Diagnosed Endometriosis or Adenomyosis: A Population-Based Study. Int. J. Gynecol. Cancer 2015, 25, 968–976. [Google Scholar] [CrossRef]
- Saraswat, L.; Ayansina, D.; Cooper, K.G.; Bhattacharya, S.; Horne, A.W.; Bhattacharya, S. Impact of endometriosis on risk of further gynaecological surgery and cancer: A national cohort study. BJOG 2018, 125, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.K.; Chung, C.J.; Chung, S.D.; Muo, C.H.; Chang, C.H.; Huang, C.Y. Risk of Endometrial Cancer in Women with Pelvic Inflammatory Disease: A Nationwide Population-Based Retrospective Cohort Study. Medicine 2015, 94, e1278. [Google Scholar] [CrossRef]
- Shen, C.C.; Hu, L.Y.; Yang, A.C.; Chiang, Y.Y.; Hung, J.H.; Tsai, S.J. Risk of uterine, ovarian and breast cancer following pelvic inflammatory disease: A nationwide population-based retrospective cohort study. BMC Cancer 2016, 16, 839. [Google Scholar] [CrossRef] [Green Version]
- Guo, G. Event-history analysis for left-truncated data. Sociol. Methodol. 1993, 23, 217. [Google Scholar] [CrossRef]
- Henley, S.J.; Miller, J.W.; Dowling, N.F.; Benard, V.B.; Richardson, L.C. Uterine Cancer Incidence and Mortality-United States, 1999–2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1333–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinozaki, T.; Mansournia, M.A.; Matsuyama, Y. On hazard ratio estimators by proportional hazards models in matched-pair cohort studies. Emerg. Themes Epidemiol. 2017, 14, 6. [Google Scholar] [CrossRef] [Green Version]
- Morgan, C.J. Landmark analysis: A primer. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2019, 26, 391–393. [Google Scholar] [CrossRef] [Green Version]
- Birkeland, K.I.; Jorgensen, M.E.; Carstensen, B.; Persson, F.; Gulseth, H.L.; Thuresson, M.; Fenici, P.; Nathanson, D.; Nystrom, T.; Eriksson, J.W.; et al. Cardiovascular mortality and morbidity in patients with type 2 diabetes following initiation of sodium-glucose co-transporter-2 inhibitors versus other glucose-lowering drugs (CVD-REAL Nordic): A multinational observational analysis. Lancet Diabetes Endocrinol. 2017, 5, 709–717. [Google Scholar] [CrossRef]
- Wei, L.; Lai, E.C.; Kao-Yang, Y.H.; Walker, B.R.; MacDonald, T.M.; Andrew, R. Incidence of type 2 diabetes mellitus in men receiving steroid 5alpha-reductase inhibitors: Population based cohort study. BMJ 2019, 365, l1204. [Google Scholar] [CrossRef] [Green Version]
- Poole, E.M.; Lin, W.T.; Kvaskoff, M.; De Vivo, I.; Terry, K.L.; Missmer, S.A. Endometriosis and risk of ovarian and endometrial cancers in a large prospective cohort of U.S. nurses. Cancer Causes Control 2017, 28, 437–445. [Google Scholar] [CrossRef] [Green Version]
- Melin, A.; Sparen, P.; Bergqvist, A. The risk of cancer and the role of parity among women with endometriosis. Hum. Reprod. 2007, 22, 3021–3026. [Google Scholar] [CrossRef] [Green Version]
- Kalaitzopoulos, D.R.; Mitsopoulou, A.; Iliopoulou, S.M.; Daniilidis, A.; Samartzis, E.P.; Economopoulos, K.P. Association between endometriosis and gynecological cancers: A critical review of the literature. Arch. Gynecol. Obstet. 2020, 301, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Sharpe-Timms, K.L.; Nabli, H.; Zimmer, R.L.; Birt, J.A.; Davis, J.W. Inflammatory cytokines differentially up-regulate human endometrial haptoglobin production in women with endometriosis. Hum. Reprod. 2010, 25, 1241–1250. [Google Scholar] [CrossRef] [Green Version]
- Karin, M.; Delhase, M. The I kappa B kinase (IKK) and NF-kappa B: Key elements of proinflammatory signalling. Semin. Immunol. 2000, 12, 85–98. [Google Scholar] [CrossRef]
- Peng, C.; Ouyang, Y.; Lu, N.; Li, N. The NF-kappaB Signaling Pathway, the Microbiota, and Gastrointestinal Tumorigenesis: Recent Advances. Front. Immunol. 2020, 11, 1387. [Google Scholar] [CrossRef]
- Patel, B.G.; Rudnicki, M.; Yu, J.; Shu, Y.; Taylor, R.N. Progesterone resistance in endometriosis: Origins, consequences and interventions. Acta Obstet. Gynecol. Scand. 2017, 96, 623–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laschke, M.W.; Menger, M.D. The gut microbiota: A puppet master in the pathogenesis of endometriosis? Am. J. Obstet. Gynecol. 2016, 215, 68.e1–68.e4. [Google Scholar] [CrossRef]
- Rodriguez, A.C.; Blanchard, Z.; Maurer, K.A.; Gertz, J. Estrogen Signaling in Endometrial Cancer: A Key Oncogenic Pathway with Several Open Questions. Horm. Cancer 2019, 10, 51–63. [Google Scholar] [CrossRef] [Green Version]
- Painter, J.N.; O’Mara, T.A.; Morris, A.P.; Cheng, T.H.T.; Gorman, M.; Martin, L.; Hodson, S.; Jones, A.; Martin, N.G.; Gordon, S.; et al. Genetic overlap between endometriosis and endometrial cancer: Evidence from cross-disease genetic correlation and GWAS meta-analyses. Cancer Med. 2018, 7, 1978–1987. [Google Scholar] [CrossRef]
- Mikuš, M.; Goldštajn, M.; Brlečić, I.; Dumančić, S.; Laganà, A.S.; Chiantera, V.; Vujić, G.; Ćorić, M. CTLA4-Linked Autoimmunity in the Pathogenesis of Endometriosis and Related Infertility: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 10902. [Google Scholar] [CrossRef]
- Søgaard, K.K.; Leisner, M.Z.; Laugesen, K.; Farkas, D.K.; Karagas, M.R.; Sørensen, H.T. Pelvic inflammatory disease and risk of cancer: A nationwide cohort study. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2020, 149, 107–109. [Google Scholar] [CrossRef]
- Zang, Y.; Dong, M.; Zhang, K.; Gao, C.; Guo, F.; Wang, Y.; Xue, F. Hormonal therapy in uterine sarcomas. Cancer Med. 2019, 8, 1339–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osiński, M.; Wirstlein, P.; Wender-Ożegowska, E.; Mikołajczyk, M.; Jagodziński, P.P.; Szczepańska, M. HSD3B2, HSD17B1, HSD17B2, ESR1, ESR2 and AR expression in infertile women with endometriosis. Ginekol. Pol. 2018, 89, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dentillo, D.B.; Meola, J.; Ferriani, R.A.; Rosa-e-Silva, J.C. Common Dysregulated Genes in Endometriosis and Malignancies. Rev. Bras. Ginecol. Obs. 2016, 38, 253–262. [Google Scholar]
- Honda, H.; Barrueto, F.F.; Gogusev, J.; Im, D.D.; Morin, P.J. Serial analysis of gene expression reveals differential expression between endometriosis and normal endometrium. Possible roles for AXL and SHC1 in the pathogenesis of endometriosis. Reprod. Biol. Endocrinol. 2008, 6, 59. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.; Huang, X.; Lin, S.; Cai, M.; Liu, J. Endometrial stromal sarcoma arising from endometriosis: A clinicopathological study and literature review. Gynecol. Obstet. Investig. 2012, 74, 288–297. [Google Scholar] [CrossRef]
- Carbone, F.; Kaur, M.M.; Chok, A.Y.; Kontovounisios, C.; Ind, T.; Rasheed, S. Endometrial stromal sarcoma arising from polypoid endometriosis: Case report and literature review. Int. J. Surg. Case Rep. 2020, 72, 537–540. [Google Scholar] [CrossRef]
- Cain, K.C.; Harlow, S.D.; Little, R.J.; Nan, B.; Yosef, M.; Taffe, J.R.; Elliott, M.R. Bias due to left truncation and left censoring in longitudinal studies of developmental and disease processes. Am. J. Epidemiol. 2011, 173, 1078–1084. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.W.; Tu, Y.Y.; Lin, S.Y.; Su, W.J.; Lin, W.L.; Lin, W.Z.; Wu, S.C.; Lai, Y.L. Risk of ovarian cancer in women with pelvic inflammatory disease: A population-based study. Lancet Oncol. 2011, 12, 900–904. [Google Scholar] [CrossRef]
- Setiawan, V.W.; Yang, H.P.; Pike, M.C.; McCann, S.E.; Yu, H.; Xiang, Y.B.; Wolk, A.; Wentzensen, N.; Weiss, N.S.; Webb, P.M.; et al. Type I and II endometrial cancers: Have they different risk factors? J. Clin. Oncol. 2013, 31, 2607–2618. [Google Scholar] [CrossRef]
- Škegro, B.; Bjedov, S.; Mikuš, M.; Mustač, F.; Lešin, J.; Matijević, V.; Ćorić, M.; Elveđi Gašparović, V.; Medić, F.; Sokol Karadjole, V. Endometriosis, Pain and Mental Health. Psychiatr. Danub. 2021, 33 (Suppl. 4), 632–636. [Google Scholar]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan's National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. (%) | ||||
|---|---|---|---|---|
| Characteristics | Comparison | PID | Endometriosis | Max SMD |
| No. in cohort | 135,236 | 114,726 | 20,510 | |
| Birth year | 32.95% | |||
| 1937–1949 | 3474 (2.57%) | 3274 (2.85%) | 200 (0.98%) | |
| 1950–1962 | 29,272 (21.65%) | 23,653 (20.62%) | 5619 (27.40%) | |
| 1963–1975 | 49,587 (36.67%) | 40,605 (35.39%) | 8982 (43.79%) | |
| 1976–1988 | 46,103 (34.09%) | 41,117 (35.84%) | 4986 (24.31%) | |
| 1989–2002 | 6800 (5.03%) | 6077 (5.30%) | 723 (3.53%) | |
| Year of index | 45.67% | |||
| 2002–2006 | 80,807 (59.75%) | 71,948 (62.71%) | 8859 (43.19%) | |
| 2007–2010 | 31,435 (23.24%) | 25,854 (22.54%) | 5581 (27.21%) | |
| 2011–2014 | 22,994 (17.00%) | 16,924 (14.75%) | 6070 (29.60%) | |
| Age on index date | 50.14% | |||
| 12–25 | 29,606 (21.89%) | 27,304 (23.8%) | 2302 (11.22%) | |
| 26–35 | 43,757 (32.36%) | 38,537 (33.59%) | 5220 (25.45%) | |
| 36–45 | 36,730 (27.16%) | 29,119 (25.38%) | 7611 (37.11%) | |
| 46–55 | 21,304 (15.75%) | 16,168 (14.09%) | 5136 (25.04%) | |
| 56–65 | 3839 (2.84%) | 3598 (3.14%) | 241 (1.18%) | |
| Marital status | 21.24% | |||
| Single | 59,712 (44.15%) | 39,212 (34.18%) | 7096 (34.60%) | |
| Married | 65,558 (48.48%) | 63,066 (54.97%) | 11,873 (57.89%) | |
| Others | 9966 (7.37%) | 12,448 (10.85%) | 1541 (7.51%) | |
| Education level (years) | 27.58% | |||
| <7 | 25,079 (18.54%) | 23,337 (20.34%) | 2792 (13.61%) | |
| 7–9 | 25,627 (18.95%) | 25,655 (22.36%) | 3697 (18.03%) | |
| 10–12 | 52,137 (38.55%) | 47,233 (41.17%) | 8323 (40.58%) | |
| ≥13 | 32,393 (23.95%) | 18,501 (16.13%) | 5698 (27.78%) | |
| Comorbidities | ||||
| Obesity | 489 (0.36%) | 499 (0.43%) | 145 (0.71%) | 4.74% |
| Renal disease | 1036 (0.77%) | 1303 (1.14%) | 298 (1.45%) | 6.56% |
| Hypertension | 5037 (3.72%) | 5016 (4.37%) | 1359 (6.63%) | 13.13% |
| Diabetes mellitus | 2682 (1.98%) | 2959 (2.58%) | 712 (3.47%) | 9.15% |
| Lipid dysfunction | 4183 (3.09%) | 4749 (4.14%) | 1273 (6.21%) | 14.83% |
| CVD | 1317 (0.97%) | 1912 (1.67% | 409 (1.99%) | 8.45% |
| Ischemic stroke | 358 (0.26%) | 369 (0.32%) | 105 (0.51%) | 3.98% |
| Hyperthyroidism | 1591 (1.18%) | 1925 (1.68%) | 431 (2.10%) | 7.29% |
| Hypothyroidism | 511 (0.38%) | 597 (0.52%) | 227 (1.11%) | 8.50% |
| Chronic hepatitis | 4200 (3.11%) | 5528 (4.82%) | 1361 (6.64%) | 16.46% |
| COPD | 3949 (2.92%) | 4651 (4.05%) | 1034 (5.04%) | 10.87% |
| Comparison | PID | Endometriosis | |
|---|---|---|---|
| No. in cohort | 135,236 | 11,4726 | 20,510 |
| Follow up person-years | 1,109,867 | 971,163.2 | 139,105.3 |
| Median of follow up year | 9.1 | 9.4 | 6.8 |
| Uterine corpus cancer | |||
| Event | 129 | 142 | 61 |
| Rate a (95% CI) | 11.62 (9.78 to 13.81) | 14.62 (12.40 to 17.24) | 43.85 (34.12 to 56.36) |
| Risk difference b (95% CI) | Reference | 3.00 (−0.13 to 6.13) | 32.23 (21.04 to 43.41) |
| aHR c (95% CI) | Reference | 1.30 (1.02 to 1.65) | 2.94 (2.16 to 4.00) |
| Uterine cancer—endometrial cancer | |||
| Event | 121 | 133 | 55 |
| Rate a (95% CI) | 10.90 (9.12 to 13.03) | 13.69 (11.55 to 16.23) | 39.54 (30.36 to 51.50) |
| Risk difference b (95% CI) | Reference | 2.79 (−0.24 to 5.82) | 28.64 (18.01 to 39.2) |
| aHR c (95% CI) | Reference | 1.28 (1.00 to 1.64) | 2.92 (2.12 to 4.03) |
| Uterine cancer—sarcoma | |||
| Event | 8 | 9 | 6 |
| Rate a (95% CI) | 0.72 (0.36 to 1.44) | 0.93 (0.48 to 1.78) | 4.31 (1.94 to 9.60) |
| Risk difference b (95% CI) | Reference | 0.21 (−0.58 to 0.99) | 3.59 (0.11 to 7.08) |
| aHR c (95% CI) | Reference | 1.21 (0.46 to 3.14) | 5.83 (2.02 to 16.89) |
| Comparison | PID | Endometriosis | |
|---|---|---|---|
| No. in cohort | 20,478 | 20,478 | 20,478 |
| Follow up person-years | 139,142.4 | 140,099.2 | 139,049.3 |
| Median of follow up (year) | 6.8 | 6.9 | 6.8 |
| Uterine corpus cancer | |||
| Event | 20 | 22 | 61 |
| Rate a (95% CI) | 14.37 (9·27 to 22.28) | 15.70 (10.34 to 23.85) | 43.54 (33.88 to 55.96) |
| Risk difference b (95% CI) | Reference | 1.33 (−7.77 to 10.43) | 29.17 (16.55 to 41.78) |
| aHR c (95% CI) | Reference | 1.12 (0.61 to 2.05) | 2.83 (1.70 to 4.71) |
| Landmark Interval | Comparison | PID | Endometriosis |
|---|---|---|---|
| 0 to 24 months | |||
| Follow up person-years | 259,763.8 | 221,801.5 | 37,896.33 |
| Event | 18 | 22 | 12 |
| Rate a (95% CI) | 6.93 (4.37 to 11.00) | 9.92 (6.53 to 15.06) | 31.67 (17.98 to 55.76) |
| aRR (95% CI) | Reference | 1.43 (0.77 to 2.67) | 4.57 (2.20 to 9.49) |
| 25 to 48 months | |||
| Follow up person-years | 236,147.6 | 204,416.3 | 31,771.5 |
| Event | 13 | 23 | 16 |
| Rate a (95% CI) | 5.50 (3.20 to 9.48) | 11.25 (7.48 to 16.93) | 50.36 (30.85 to 82.21) |
| aRR (95% CI) | Reference | 2.04 (1.04 to 4.04) | 9.15 (4.40 to 19.02) |
| 49–72 months | |||
| Follow up person-years | 199,574 | 175,221.2 | 24,458.83 |
| Event | 27 | 29 | 13 |
| Rate a (95% CI) | 13.53 (9.28 to 19.73) | 16.55 (11.50 to 23.82) | 53.15 (30.86 to 91.54) |
| aRR (95% CI) | Reference | 1.22 (0.72 to 2.07) | 3.93 (2.03 to 7.61) |
| 73–96 months | |||
| Follow up person-years | 168,977.7 | 149,962.8 | 19,092.83 |
| Event | 29 | 35 | 12 |
| Rate a (95% CI) | 17.16 (11.93 to 24.70) | 23.34 (16.76 to 32.50) | 62.85 (35.69 to 110.67) |
| aRR (95% CI) | Reference | 1.36 (0.83 to 2.23) | 3.66 (1.87 to 7.18) |
| 97–120 months | |||
| Follow up person-years | 130,205 | 116,527.8 | 13,802.42 |
| Event | 24 | 25 | 4 |
| Rate a (95% CI) | 18.43 (12.36 to 27.50) | 21.45 (14.50 to 31.75) | 28.98 (10.88 to 77.22) |
| aRR (95% CI) | Reference | 1.16 (0.67 to 2.04) | 1.57 (0.55 to 4.53) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.-Y.; Ma, K.S.-K.; Wang, L.-T.; Chiang, C.-H.; Yang, S.-F.; Wang, C.-H.; Wang, P.-H. The Risk of Endometrial Cancer and Uterine Sarcoma Following Endometriosis or Pelvic Inflammatory Disease. Cancers 2023, 15, 833. https://doi.org/10.3390/cancers15030833
Huang J-Y, Ma KS-K, Wang L-T, Chiang C-H, Yang S-F, Wang C-H, Wang P-H. The Risk of Endometrial Cancer and Uterine Sarcoma Following Endometriosis or Pelvic Inflammatory Disease. Cancers. 2023; 15(3):833. https://doi.org/10.3390/cancers15030833
Chicago/Turabian StyleHuang, Jing-Yang, Kevin Sheng-Kai Ma, Li-Tzu Wang, Cho-Han Chiang, Shun-Fa Yang, Chun-Hao Wang, and Po-Hui Wang. 2023. "The Risk of Endometrial Cancer and Uterine Sarcoma Following Endometriosis or Pelvic Inflammatory Disease" Cancers 15, no. 3: 833. https://doi.org/10.3390/cancers15030833