

Hepatectomy versus Chemotherapy for Resectable Colorectal Liver Metastases in Progression after Perioperative Chemotherapy: Expanding the Boundaries of the Curative Intent
 , , , ,
, , , ,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Endpoint
2.2. Definitions and Follow-Up Protocol
2.3. Statistical Analysis
3. Results
3.1. Surgical Details about the HEP Group
3.2. Group Comparison
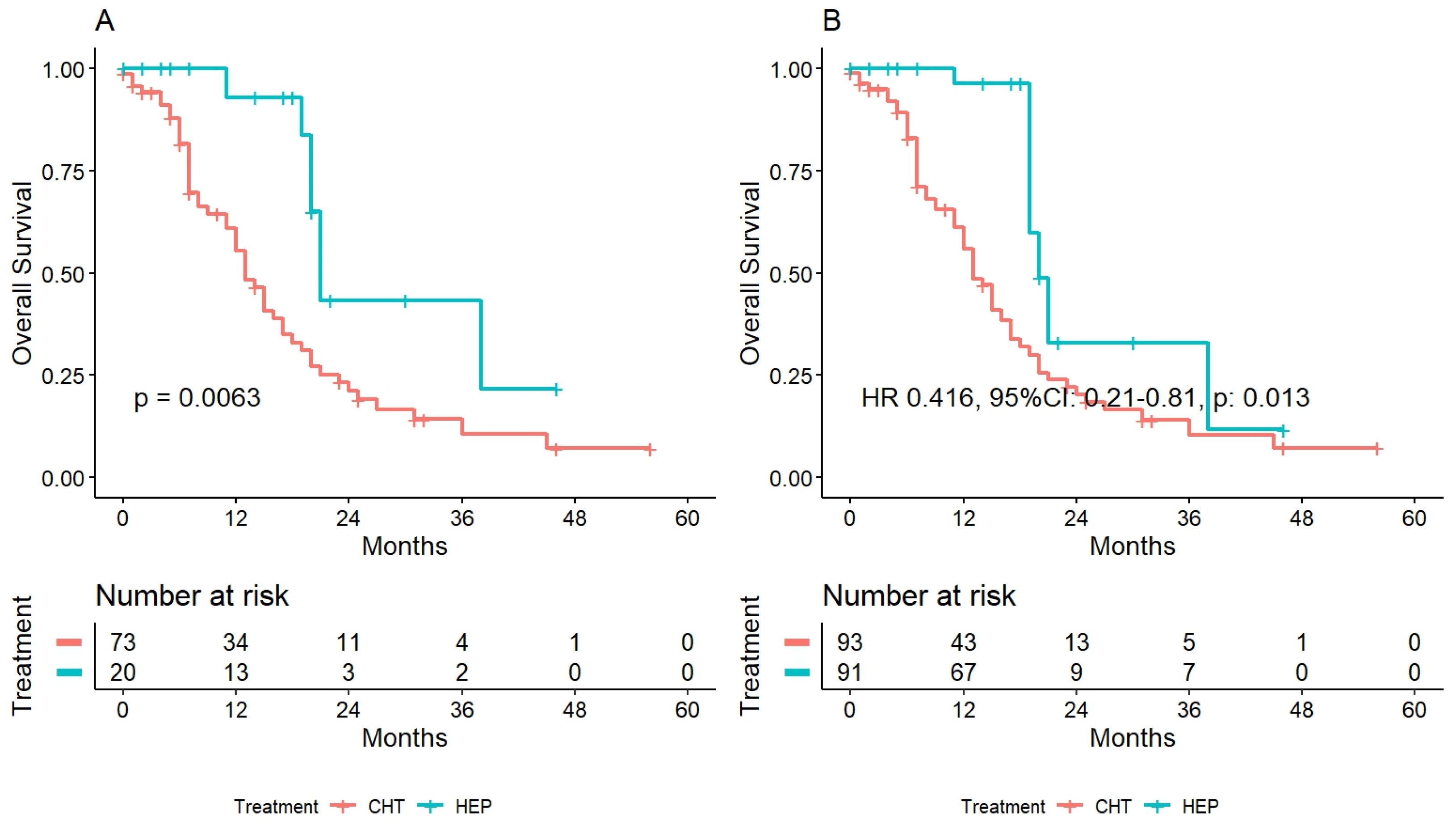
3.3. Survival Analysis
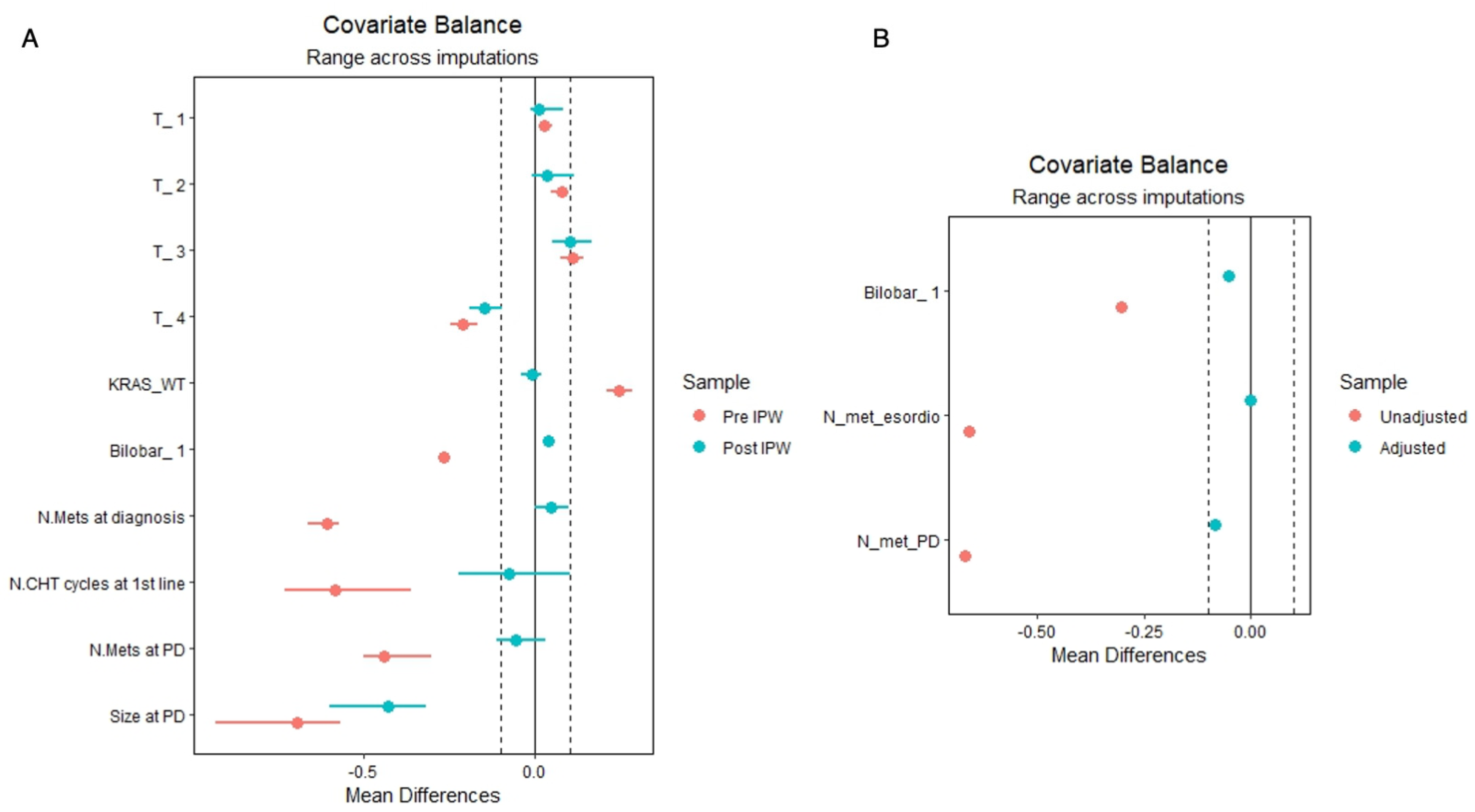
3.4. Survival Analysis after Inverse Probability Weighting
3.5. Patients with Disease Progression after Two Lines of Chemotherapy
3.6. HEP Vs CHT for Different Types of Disease Progression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Cucchetti, A.; Ferrero, A.; Cescon, M.; Donadon, M.; Russolillo, N.; Ercolani, G.; Stacchini, G.; Mazzotti, F.; Torzilli, G.; Pinna, A.D.; et al. Cure Model Survival Analysis after Hepatic Resection for Colorectal Liver Metastases. Ann. Surg. Oncol. 2015, 22, 1908–1914. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Pascal, G.; Castaing, D.; Azoulay, D.; Delvart, V.; Paule, B.; Levi, F.; Bismuth, H. Tumor progression while on chemotherapy: A contraindication to liver resection for multiple colorectal metastases? Ann. Surg. 2004, 240, 1052–1064. [Google Scholar] [CrossRef]
- Torzilli, G.; Viganò, L.; Gatti, A.; Costa, G.; Cimino, M.; Procopio, F.; Donadon, M.; Del Fabbro, D. Twelve-year experience of ‘radical but conservative’ liver surgery for colorectal metastases: Impact on surgical practice and oncologic efficacy. HPB 2017, 19, 775–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; van Krieken, J.H.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef]
- Sobrero, A.F.; Maurel, J.; Fehrenbacher, L.; Scheithauer, W.; Abubakr, Y.A.; Lutz, M.P.; Vega-Villegas, M.E.; Eng, C.; Steinhauer, E.U.; Prausova, J.; et al. EPIC: Phase III trial of cetuximab plus irinotecan after fluoropyrimidine and oxaliplatin failure in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 2311–2319. [Google Scholar] [CrossRef] [Green Version]
- Peeters, M.; Price, T.J.; Cervantes, A.; Sobrero, A.; Ducreux, M.; Hotko, Y.; André, T.; Chan, E.; Lordick, F.; Punt, C.J.A.; et al. Final results from a randomized phase 3 study of FOLFIRI {+/−} panitumumab for second-line treatment of metastatic colorectal cancer. Ann. Oncol. 2014, 25, 107–116. [Google Scholar] [CrossRef]
- Neumann, U.P.; Thelen, A.; Röcken, C.; Seehofer, D.; Bahra, M.; Riess, H.; Jonas, S.; Schmeding, M.; Pratschke, J.; Bova, R.; et al. Nonresponse to pre-operative chemotherapy does not preclude long-term survival after liver resection in patients with colorectal liver metastases. Surgery 2009, 146, 52–59. [Google Scholar] [CrossRef]
- Viganò, L.; Capussotti, L.; Barroso, E.; Nuzzo, G.; Laurent, C.; Ijzermans, J.N.M.; Gigot, J.-F.; Figueras, J.; Gruenberger, T.; Mirza, D.F.; et al. Progression while Receiving Preoperative Chemotherapy Should Not Be an Absolute Contraindication to Liver Resection for Colorectal Metastases. Ann. Surg. Oncol. 2012, 19, 2786–2796. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.; Egger, M.; Pocock, S.; Gøtzsche, P.; Vandenbroucke, J. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef]
- Schwartz, L.H.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; Hayes, W.; et al. RECIST 1.1-Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viganò, L.; Procopio, F.; Cimino, M.M.; Donadon, M.; Gatti, A.; Costa, G.; Del Fabbro, D.; Torzilli, G. Is Tumor Detachment from Vascular Structures Equivalent to R0 Resection in Surgery for Colorectal Liver Metastases? An Observational Cohort. Ann. Surg. Oncol. 2016, 23, 1352–1360. [Google Scholar] [CrossRef] [PubMed]
- Torzilli, G. Ultrasound-Guided Liver Surgery: An Atlas; Springer: Milan, Italy, 2014. [Google Scholar]
- Torzilli, G.; Garancini, M.; Donadon, M.; Cimino, M.; Procopio, F.; Montorsi, M. Intraoperative ultrasonographic detection of communicating veins between adjacent hepatic veins during hepatectomy for tumours at the hepatocaval confluence. Br. J. Surg. 2010, 97, 1867–1873. [Google Scholar] [CrossRef]
- Torzilli, G.; Cimino, M.M. Extending the Limits of Resection for Colorectal Liver Metastases ENHANCED ONE STAGE SURGERY. J. Gastrointest. Surg. 2017, 21, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Torzilli, G.; Procopio, F.; Botea, F.; Marconi, M.; Del Fabbro, D.; Donadon, M.; Palmisano, A.; Spinelli, A.; Montorsi, M. One-stage ultrasonographically guided hepatectomy for multiple bilobar colorectal metastases: A feasible and effective alternative to the 2-stage approach. Surgery 2009, 146, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo Classification of Surgical Complications. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Newgard, C.D.; Lewis, R.J. Missing Data: How to Best Account for What Is Not Known. JAMA 2015, 314, 940–941. [Google Scholar] [CrossRef]
- Kleinke, K.; Reinecke, J.; Salfrán, D.; Spiess, M. Applied Multiple Imputation: Advantages, Pitfalls, New Developments and Applications in R; Springer Nature: Cham, Switzerland, 2020. [Google Scholar]
- Kornprat, P.; Jarnagin, W.R.; Gonen, M.; Dematteo, R.P.; Fong, Y.; Blumgart, L.H.; D’Angelica, M. Outcome after hepatectomy for multiple (four or more) colorectal metastases in the era of effective chemotherapy. Ann. Surg. Oncol. 2007, 14, 1151–1160. [Google Scholar] [CrossRef]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): Long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013, 14, 1208–1215. [Google Scholar] [CrossRef]
- Gruenberger, B.; Tamandl, D.; Schueller, J.; Scheithauer, W.; Zielinski, C.; Herbst, F.; Gruenberger, T. Bevacizumab, capecitabine, and oxaliplatin as neoadjuvant therapy for patients with potentially curable metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 1830–1835. [Google Scholar] [CrossRef]
- Lech, G. Colorectal cancer tumour markers and biomarkers: Recent therapeutic advances. World J. Gastroenterol. 2016, 22, 1745. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| CHT | HEP | p | |
|---|---|---|---|
| n | 78 | 27 | |
| Age, years (median [IQR]) | 63.50 [55.25, 71.00] | 65.00 [60.00, 72.50] | 0.313 |
| Male sex (%) | 51 (65.4) | 20 (74.1) | 0.553 |
| ECOG (%) | 0.192 | ||
| 1 | 16 (20.5) | 6 (22.2) | |
| 2 | 12 (15.4) | 0 (0.0) | |
| Primitive T (%) | 0.016 | ||
| 1–2 | 4 (5.2) | 5 (18.5) | |
| 3–4 | 54 (69.2) | 20 (74.1) | |
| Primitive N (%) | 0.164 | ||
| 1 | 19 (24.4) | 11 (40.7) | |
| 2 | 25 (32.1) | 6 (22.2) | |
| KRAS Mut (%) | 40 (51.3) | 10 (37.0) | 0.008 |
| Metachronous (%) | 24 (30.8) | 12 (44.4) | 0.291 |
| Bilobar disease (%) | 58 (74.4) | 13 (48.1) | 0.027 |
| Extrahepatic disease (%) | 29 (37.2) | 9 (33.3) | 0.226 |
| N. courses I CHT line (median [IQR]) | 8.00 [5.00, 12.00] | 6.00 [3.50, 6.50] | 0.007 |
| II CHT lines (%) | 70 (89.7) | 20 (74.1) | 0.002 |
| N. courses II CHT line (median [IQR]) | 7.50 [4.00, 12.00] | 5.00 [4.00, 6.00] | 0.271 |
| First line CHT | |||
| Irinotecan (%) | 15 (19.2) | 3 (11.1) | 0.335 |
| Oxaliplatin (%) | 61 (78.2) | 20 (74.1) | 0.66 |
| Capecitabine (%) | 25 (32) | 13 (48.2) | 0.134 |
| Anti-VEGF (%) | 22 (28.2) | 4 (14.8) | 0.165 |
| Anti-EGFR (%) | 3 (3.8) | 3 (11.1) | 0.161 |
| Irinotecan+oxaliplatin (%) | 5 (6.4) | 0 (0) | 0.178 |
| Second line CHT | |||
| Irinotecan (%) | 41 (65.1) | 12 (60) | 0.68 |
| Oxaliplatin (%) | 13 (20.6) | 5 (25) | 0.68 |
| Capecitabine (%) | 7 (11.1) | 3 (15) | 0.642 |
| Anti-VEGF (%) | 23 (36.5) | 10 (50) | 0.283 |
| Anti-EGFR (%) | 4 (6.3) | 1 (5) | 0.825 |
| Irinotecan+oxaliplatin (%) | 1 (1.6) | 0 (0) | 0.571 |
| Type of PD (%) | 0.298 | ||
| Numeric | 4 (5.1) | 0 (0.0) | |
| Dimensional | 12 (15.4) | 8 (29.6) | |
| Biologic + Numeric | 0 (0.0) | 1 (3.7) | |
| Numeric +Dimensional | 16 (20.5) | 5 (18.5) | |
| Biologic + Dimensional | 9 (11.5) | 4 (14.8) | |
| All | 33 (42.3) | 9 (33.3) | |
| N. nodules at diagnosis (median [IQR]) | 4.00 [2.00, 7.25] | 2.00 [1.00, 4.00] | 0.016 |
| Size at diagnosis, cm (median [IQR]) | 3.00 [2.00, 4.80] | 2.20 [1.35, 3.90] | 0.121 |
| CEA at diagnosis (median [IQR]) | 27.00 [16.20, 132.25] | 28.35 [12.00, 86.00] | 0.613 |
| CA19.9 at diagnosis (median [IQR]) | 218.00 [17.50, 1128.00] | 48.00 [13.95, 495.15] | 0.577 |
| N. nodules at PD (median [IQR]) | 6.50 [3.00, 14.00] | 3.00 [2.00, 5.00] | 0.008 |
| Size at PD, cm (median [IQR]) | 4.80 [3.70, 6.80] | 3.30 [2.00, 4.50] | 0.004 |
| CEA at PD (median [IQR]) | 40.60 [17.50, 161.00] | 29.80 [6.62, 63.75] | 0.236 |
| CA19.9 at PD (median [IQR]) | 103.10 [16.95, 430.25] | 76.10 [15.78, 147.75] | 0.379 |
| PRE IPW | POST IPW | ||||
|---|---|---|---|---|---|
| HR (Univariable) | HR (Multivariable) | HR (Univariable) | HR (Multivariable) | ||
| ECOG | 0 | - | - | - | |
| 1 | 1.19 (0.61–2.32, p = 0.607) | - | 0.775 (0.24–2.45, p = 0.666) | - | |
| 2 | 1.14 (0.48–2.68, p = 0.764) | - | 1.452 (0.47–4.47, p = 0.519) | - | |
| G | 1 | - | - | - | - |
| 2 | 1.42 (0.60–3.37, p = 0.430) | - | 1.629 (0.13–19.43, p = 0.710) | - | |
| 3 | 1.60 (0.64–4.02, p = 0.315) | - | 2.735 (0.22–33.36, p = 0.458) | - | |
| T | 1 | - | - | - | - |
| 2 | 0.74 (0.24–2.35, p = 0.613) | - | 0.608 (0.09–3.93, p = 0.611) | - | |
| 3 | 0.72 (0.30–1.71, p = 0.458) | - | 0.496 (0.09–2.71, p = 0.441) | - | |
| 4 | 1.55 (0.59–4.06, p = 0.370) | - | 1.156 (0.20–6.47, p = 0.872) | - | |
| N | 0 | - | - | - | - |
| 1 | 1.11 (0.59–2.08, p = 0.738) | - | 0.619 (0.21–1.75, p = 0.370) | - | |
| 2 | 1.28 (0.70–2.33, p = 0.418) | - | 0.835 (0.33–2.06, p = 0.700) | - | |
| KRAS | Mut | - | - | - | - |
| WT | 0.52 (0.31–0.88, p = 0.016) | 0.54 (0.31–0.93, p = 0.028) | 0.757 (0.33–1.71, p = 0.507) | - | |
| Metachronous disease | no | - | - | - | - |
| yes | 0.94 (0.55–1.62, p = 0.829) | - | 1.182 (0.55–2.53, p = 0.669) | - | |
| Bilobar | no | - | - | - | - |
| yes | 1.44 (0.82–2.54, p = 0.208) | - | 1.117 (0.50–2.48, p = 0.787) | - | |
| Extrahepatic spread | no | - | - | - | - |
| yes | 0.76 (0.46–1.28, p = 0.301) | - | 0.797 (0.34–1.85, p = 0.601) | - | |
| Type of PD | Biologic | - | - | - | - |
| Numeric | 2.26 (0.23–21.86, p = 0.481) | - | 2.398 (0.67–8.47, p = 0.180) | 2.85 (0.61–13.23, p = 0.186) | |
| Dimensional | 0.90 (0.11–7.04, p = 0.920) | - | 0.457 (0.13–1.60, p = 0.228) | 1.323 (0.39–4.45, p = 0.654) | |
| N+D | 2.72 (0.35–20.94, p = 0.337) | - | 2.139 (1.41–3.24, p < 0.001) | 7.582 (2.80–20.49, p = 0.001) | |
| Bio+D | 1.62 (0.20–12.93, p = 0.650) | - | 1.362 (0.60–3.09, p = 0.463) | 3.548 (1.65–7.62, p = 0.004) | |
| All | 1.04 (0.14–7.70, p = 0.973) | - | 0.917 (0.48–1.72, p = 0.789) | 1.838 (0.97–3.45, p = 0.067) | |
| Treatment | CHT | - | - | - | - |
| HEP | 0.25 (0.12–0.50, p < 0.001) | 0.21 (0.10–0.44, p = < 0.001) | 0.256 (0.08–0.78, p = 0.033) | 0.198 (0.08–0.48, p = 0.001) | |
| Age, years | Mean (SD) | 1.00 (0.98–1.03, p = 0.659) | 1.02 (1.00–1.04, p = 0.113) | 1.002 (0.97–1.03, p = 0.879) | - |
| N. nodules at diagnosis | Mean (SD) | 1.03 (0.99–1.06, p = 0.101) | - | 1.002 (0.97–1.03, p = 0.879) | - |
| Size at diagnosis | Mean (SD) | 1.09 (1.01–1.17, p = 0.029) | 0.98 (0.90–1.06, p = 0.610) | 1.142 (1.00–1.29, p = 0.047) | - |
| CEA at diagnosis | Mean (SD) | 1.00 (1.00–1.00, p = 0.012) | 1.00 (1.00–1.00, p = 0.001) | 1.00 (0.99–1.01, p = 0.787) | - |
| CA19.9 at diagnosis | Mean (SD) | 1.00 (1.00–1.00, p = 0.944) | - | 1.00 (1.0–1.0, p = 0.663) | - |
| N. nodules at PD | Mean (SD) | 1.00 (0.99–1.02, p = 0.703) | - | 0.991 (0.95–1.02, p = 0.593) | - |
| Size at PD | Mean (SD) | 1.07 (1.00–1.15, p = 0.057) | - | 1.101 (0.98–1.23, p = 0.106) | - |
| CEA at PD | Mean (SD) | 1.00 (1.00–1.00, p = 0.545) | - | 1.0 (1.0–1.0, p = 0.542) | - |
| CA19.9 at PD | Mean (SD) | 1.00 (1.00–1.00, p = 0.476) | - | 1.0 (1.0–1.0, p = 0.113) | - |
| CHT | HEP | p | |
|---|---|---|---|
| n | 73 | 20 | |
| Age, years (median [IQR]) | 63.00 [54.00, 71.00] | 68.00 [62.50, 73.25] | 0.101 |
| Male (%) | 46 (63.0) | 14 (70.0) | 0.753 |
| ECOG (%) | NaN | ||
| 0 | 50 (68.5) | 15 (75.0) | |
| 1 | 16 (21.9) | 5 (25.0) | |
| 2 | 7 (9.6) | 0 (0.0) | |
| Primitive T (%) | 0.085 | ||
| 1–2 | 12 (16.4) | 5 (25.0) | |
| 3–4 | 61 (83.5) | 15 (75.0) | |
| Primitive N (%) | 0.309 | ||
| 0 | 19 (26.0) | 5 (25.0) | |
| 1 | 24 (32.9) | 10 (50.0) | |
| 2 | 30 (41.1) | 5 (25.0) | |
| KRAS = WT (%) | 27 (37.0) | 11 (55.0) | 0.232 |
| Metachronous (%) | 22 (30.1) | 11 (55.0) | 0.073 |
| Bilobar disease (%) | 55 (75.3) | 9 (45.0) | 0.02 |
| Extrahepatic disease (%) | 28 (38.4) | 8 (40.0) | 1 |
| N. nodules at diagnosis (median [IQR]) | 5.00 [2.00, 11.00] | 2.00 [1.00, 3.50] | 0.009 |
| Size at diagnosis, cm (median [IQR]) | 3.60 [1.40, 7.10] | 1.95 [1.20, 4.35] | 0.071 |
| CEA at diagnosis (median [IQR]) | 56.00 [5.00, 825.00] | 57.60 [4.50, 600.75] | 0.885 |
| CA19.9 at diagnosis (median [IQR]) | 85.00 [1.00, 3557.00] | 1629.00 [9.43, 2429.00] | 0.463 |
| N. courses CHT I line (median [IQR]) | 8.00 [5.00, 12.00] | 6.00 [4.00, 7.25] | 0.023 |
| N. courses CHT II line (median [IQR]) | 12.00 [5.00, 14.00] | 6.00 [4.75, 14.00] | 0.4 |
| Type of PD (%) | 0.415 | ||
| Biologic | 1 (1.4) | 0 (0.0) | |
| Numeric | 3 (4.1) | 0 (0.0) | |
| Dimensional | 13 (17.8) | 4 (20.0) | |
| Biologic + Numeric | 0 (0.0) | 1 (5.0) | |
| Numeric + Dimensional | 17 (23.3) | 4 (20.0) | |
| Biologic + Dimensional | 8 (11.0) | 4 (20.0) | |
| All | 31 (42.5) | 7 (35.0) | |
| N. nodules at PD (median [IQR]) | 8.00 [3.00, 20.00] | 3.00 [2.00, 4.25] | 0.004 |
| Size at PD, cm (median [IQR]) | 4.80 [2.00, 9.20] | 3.55 [2.15, 5.70] | 0.21 |
| CEA at PD (median [IQR]) | 41.00 [17.00, 383.00] | 42.35 [11.05, 82.50] | 0.333 |
| CA19.9 at PD (median [IQR]) | 166.00 [5.00, 12,000.00] | 76.10 [10.70, 205.57] | 0.583 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Famularo, S.; Milana, F.; Cimino, M.; Procopio, F.; Costa, G.; Galvanin, J.; Paoluzzi Tomada, E.; Bunino, F.M.; Palmisano, A.; Donadon, M.; et al. Hepatectomy versus Chemotherapy for Resectable Colorectal Liver Metastases in Progression after Perioperative Chemotherapy: Expanding the Boundaries of the Curative Intent. Cancers 2023, 15, 783. https://doi.org/10.3390/cancers15030783
Famularo S, Milana F, Cimino M, Procopio F, Costa G, Galvanin J, Paoluzzi Tomada E, Bunino FM, Palmisano A, Donadon M, et al. Hepatectomy versus Chemotherapy for Resectable Colorectal Liver Metastases in Progression after Perioperative Chemotherapy: Expanding the Boundaries of the Curative Intent. Cancers. 2023; 15(3):783. https://doi.org/10.3390/cancers15030783
Chicago/Turabian StyleFamularo, Simone, Flavio Milana, Matteo Cimino, Fabio Procopio, Guido Costa, Jacopo Galvanin, Elisa Paoluzzi Tomada, Francesca Margherita Bunino, Angela Palmisano, Matteo Donadon, and et al. 2023. "Hepatectomy versus Chemotherapy for Resectable Colorectal Liver Metastases in Progression after Perioperative Chemotherapy: Expanding the Boundaries of the Curative Intent" Cancers 15, no. 3: 783. https://doi.org/10.3390/cancers15030783