
Clinical Presentation, Management, and Evolution of Lymphomas in Patients with Inflammatory Bowel Disease: An ENEIDA Registry Study

 , , , , , , , , , , , and
, , , , , , , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Variables of Interest
2.4. Statistical Analysis
3. Results
3.1. Immunosuppressive and Biological Treatments before Lymphoma Diagnosis
3.2. Diagnosis of Lymphoma
3.3. Treatment of Lymphoma
3.4. Treatment and Evolution of IBD after Lymphoma Diagnosis
3.5. Relapse of Lymphoma
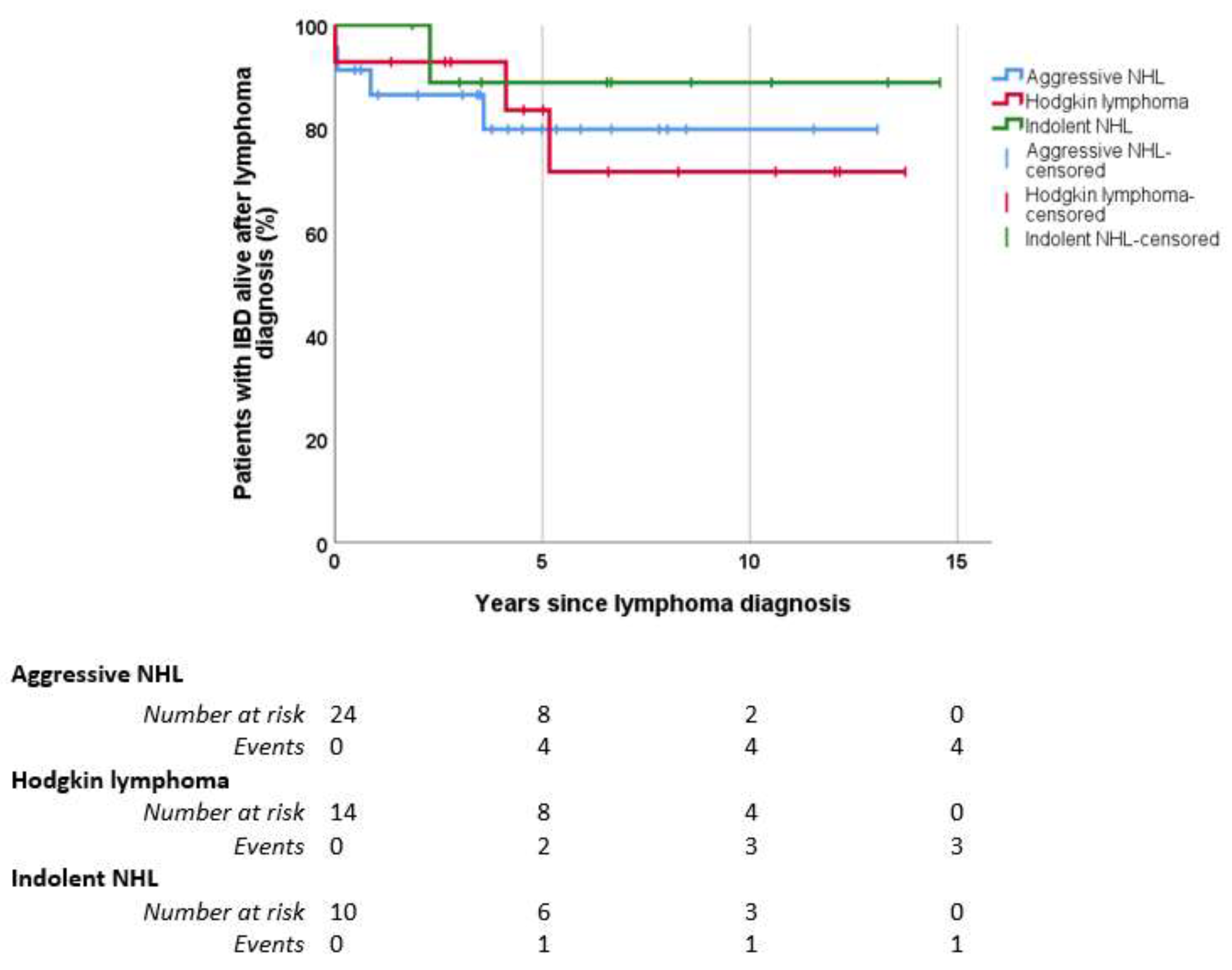
3.6. Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Annese, V.; Beaugerie, L.; Egan, L.; Biancone, L.; Bolling, C.; Brandts, C.; Dierickx, D.; Dummer, R.; Fiorino, G.; Gornet, J.M.; et al. European Evidence-Based Consensus: Inflammatory Bowel Disease and Malignancies. J. Crohn’s Colitis 2015, 9, 945–965. [Google Scholar] [CrossRef] [Green Version]
- Lo, B.; Zhao, M.; Vind, I.; Burisch, J. The Risk of Extraintestinal Cancer in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis of Population-Based Cohort Studies. Clin. Gastroenterol. Hepatol. 2021, 19, 1117–1138.e19. [Google Scholar] [CrossRef]
- Lemaitre, M.; Kirchgesner, J.; Rudnichi, A.; Carrat, F.; Zureik, M.; Carbonnel, F.; Dray-Spira, R. Association between Use of Thiopurines or Tumor Necrosis Factor Antagonists Alone or in Combination and Risk of Lymphoma in Patients with Inflammatory Bowel Disease. JAMA 2017, 318, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Kotlyar, D.S.; Lewis, J.D.; Beaugerie, L.; Tierney, A.; Brensinger, C.M.; Gisbert, J.P.; Loftus, E.V.; Peyrin-Biroulet, L.; Blonski, W.C.; Van Domselaar, M.; et al. Risk of Lymphoma in Patients with Inflammatory Bowel Disease Treated with Azathioprine and 6-Mercaptopurine: A Meta-Analysis. Clin. Gastroenterol. Hepatol. 2015, 13, 847–858.e4. [Google Scholar] [CrossRef]
- Zabana, Y.; Panés, J.; Nos, P.; Gomollón, F.; Esteve, M.; García-Sánchez, V.; Gisbert, J.P.; Barreiro-de-Acosta, M.; Domènech, E. The ENEIDA Registry (Nationwide Study on Genetic and Environmental Determinants of Inflammatory Bowel Disease) by GETECCU: Design, Monitoring and Functions. Gastroenterol. Hepatol. 2020, 43, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Lee Harris, N.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 Revision of the World Health Organization Classification of Lymphoid Neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. 2014, 32, 3059. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Jess, T.; Horváth-Puhó, E.; Fallingborg, J.; Rasmussen, H.H.; Jacobsen, B.A. Cancer Risk in Inflammatory Bowel Disease According to Patient Phenotype and Treatment: A Danish Population-Based Cohort Study. Am. J. Gastroenterol. 2013, 108, 1869–1876. [Google Scholar] [CrossRef]
- Rezazadeh Ardabili, A.; Jeuring, S.; Mujagic, Z.; Oostenbrug, L.; Romberg-Camps, M.; Jonkers, D.; van Bodegraven, A.; Pierik, M. Classic Drugs in the Time of New Drugs: Real-World, Long-Term Outcomes of Thiopurine Monotherapy in 1016 Patients with Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2022, 56, 1030–1043. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Udagawa, E.; Hibi, T. Lack of Increased Risk of Lymphoma with Thiopurine Therapy Regardless of Dose and Duration of Treatment in Japanese Patients with Inflammatory Bowel Diseases. Digestion 2022, 103, 169–173. [Google Scholar] [CrossRef]
- Ranjan, M.K.; Kante, B.; Vuyyuru, S.K.; Kumar, P.; Mundhra, S.K.; Golla, R.; Sharma, R.; Sahni, P.; Das, P.; Makharia, G.; et al. Minimal Risk of Lymphoma and Non-Melanoma Skin Cancer despite Long-Term Use of Thiopurines in Patients with Inflammatory Bowel Disease: A Longitudinal Cohort Analysis from Northern India. J. Gastroenterol. Hepatol. 2022, 37, 1544–1553. [Google Scholar] [CrossRef]
- Chupin, A.; Perduca, V.; Meyer, A.; Bellanger, C.; Carbonnel, F.; Dong, C. Systematic Review with Meta-Analysis: Comparative Risk of Lymphoma with Anti-Tumour Necrosis Factor Agents and/or Thiopurines in Patients with Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2020, 52, 1289–1297. [Google Scholar] [CrossRef]
- Cleveland, N.K.; Rubin, D.T. Cancer prevention in patients with inflammatory bowel disease. Pract. Gastroenterol. 2021, 45, 12–28. [Google Scholar]
- Beaugerie, L.; Rahier, J.F.; Kirchgesner, J. Predicting, Preventing, and Managing Treatment-Related Complications in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2020, 18, 1324–1335.e2. [Google Scholar] [CrossRef] [PubMed]
- Lewis, W.D.; Lilly, S.; Jones, K.L. Lymphoma: Diagnosis and Treatment. Am. Fam. Physician 2020, 101, 34–41. [Google Scholar] [PubMed]
- Ansell, S.M. Non-Hodgkin Lymphoma: Diagnosis and Treatment. Mayo Clin. Proc. 2015, 90, 1152–1163. [Google Scholar] [CrossRef] [Green Version]
- Ansell, S.M. Hodgkin Lymphoma: A 2020 Update on Diagnosis, Risk-Stratification, and Management. Am. J. Hematol. 2020, 95, 978–989. [Google Scholar] [CrossRef]
- Hori, Y.; Yamamoto, H.; Kawatoko, S.; Nozaki, Y.; Torisu, T.; Kato, K.; Koga, Y.; Miyoshi, H.; Ohshima, K.; Tateishi, Y.; et al. Lymphoid and Myeloid Proliferative Disorders Associated with Inflammatory Bowel Disease: A Clinicopathological Study of 15 Cases. Hum. Pathol. 2022, 120, 88–98. [Google Scholar] [CrossRef]
- Muller, M.; Broséus, J.; Feugier, P.; Thieblemont, C.; Beaugerie, L.; Danese, S.; Arnone, D.; Ndiaye, N.C.; Kokten, T.; Houlgatte, R.; et al. Characteristics of Lymphoma in Patients with Inflammatory Bowel Disease: A Systematic Review. J. Crohn’s Colitis 2021, 15, 827–839. [Google Scholar] [CrossRef]
- Zanelli, M.; Ragazzi, M.; Valli, R.; De Marco, L.; Cecinato, P.; Azzolini, F.; Ferrari, A.; Bacci, F.; Ascani, S. Unique Presentation of a Plasmablastic Lymphoma Superficially Involving the Entire Large Bowel. Pathol. Res. Pract. 2015, 211, 1030–1033. [Google Scholar] [CrossRef] [PubMed]
- Severyns, T.; Kirchgesner, J.; Lambert, J.; Thieblemont, C.; Amiot, A.; Abitbol, V.; Treton, X.; Cazals-Hatem, D.; Malamut, G.; Coppo, P.; et al. Prognosis of Lymphoma in Patients with Known Inflammatory Bowel Disease: A French Multicentre Cohort Study. J. Crohn’s Colitis 2020, 14, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- Cancer Reasearch UK. Non-Hodgkin’s Lymphoma Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/non-hodgkin-lymphoma#heading-Zero (accessed on 6 October 2022).
- SEER; National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Available online: https://seer.cancer.gov/statfacts/ (accessed on 6 October 2022).
- De Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global Burden of Cancer Attributable to Infections in 2018: A Worldwide Incidence Analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [CrossRef] [Green Version]
- Morton, L.M.; Slager, S.L.; Cerhan, J.R.; Wang, S.S.; Vajdic, C.M.; Skibola, C.F.; Bracci, P.M.; de Sanjosé, S.; Smedby, K.E.; Chiu, B.C.H.; et al. Etiologic Heterogeneity among Non-Hodgkin Lymphoma Subtypes: The InterLymph Non-Hodgkin Lymphoma Subtypes Project. J. Natl. Cancer Inst. Monogr. 2014, 2014, 130–144. [Google Scholar] [CrossRef] [Green Version]
- Miranda-Filho, A.; Piñeros, M.; Znaor, A.; Marcos-Gragera, R.; Steliarova-Foucher, E.; Bray, F. Global Patterns and Trends in the Incidence of Non-Hodgkin Lymphoma. Cancer Causes Control 2019, 30, 489–499. [Google Scholar] [CrossRef]
- Bastos-Oreiro, M.; Muntañola, A.; Panizo, C.; Gonzalez-Barca, E.; de Villambrosia, S.G.; Córdoba, R.; López, J.L.B.; González-Sierra, P.; Terol, M.J.; Gutierrez, A.; et al. RELINF: Prospective Epidemiological Registry of Lymphoid Neoplasms in Spain. A Project from the GELTAMO Group. Ann. Hematol. 2020, 99, 799–808. [Google Scholar] [CrossRef]
- Algaba, A.; Guerra, I.; Marín-Jiménez, I.; Quintanilla, E.; López-Serrano, P.; García-Sánchez, M.C.; Casis, B.; Taxonera, C.; Moral, I.; Chaparro, M.; et al. Incidence, Management, and Course of Cancer in Patients with Inflammatory Bowel Disease. J. Crohn’s Colitis 2015, 9, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Sebastian, S.; Neilaj, S. Practical Guidance for the Management of Inflammatory Bowel Disease in Patients with Cancer. Which Treatment? Therap. Adv. Gastroenterol. 2019, 12, 1756284818817293. [Google Scholar] [CrossRef] [PubMed]
- Dahmus, J.; Rosario, M.; Clarke, K. Risk of Lymphoma Associated with Anti-TNF Therapy in Patients with Inflammatory Bowel Disease: Implications for Therapy. Clin. Exp. Gastroenterol. 2020, 13, 339–350. [Google Scholar] [CrossRef] [PubMed]
- De Francisco, R.; Castaño-García, A.; Martínez-González, S.; Pérez-Martínez, I.; González-Huerta, A.J.; Morais, L.R.; Fernández-García, M.S.; Jiménez, S.; Díaz-Coto, S.; Flórez-Díez, P.; et al. Impact of Epstein-Barr Virus Serological Status on Clinical Outcomes in Adult Patients with Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2018, 48, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Reijasse, D.; Le Pendeven, C.; Cosnes, J.; Dehee, A.; Gendre, J.P.; Nicolas, J.C.; Beaugerie, L. Epstein-Barr Virus Viral Load in Crohn’s Disease: Effect of Immunosuppressive Therapy. Inflamm. Bowel Dis. 2004, 10, 85–90. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Number of Patients (%) | |
|---|---|
| Men | 35 (67) |
| Smokers or former smokers | 22 (51) * |
| Type of IBD | |
| Ulcerative colitis | 27 (57) |
| Extensive colitis | 12 (44) |
| Left-sided colitis | 9 (33) |
| Proctitis | 6 (22) |
| Crohn’s disease | 23 (44) |
| L1. Ileal | 5 (22) |
| L2. Colonic | 13 (56) |
| L3. Ileocolonic | 5 (22) |
| p. Perianal disease | 8 (35) |
| Unclassified colitis | 2 (3.9) |
| Median age at diagnosis of IBD | 45 years (IQR 28–57) |
| Median age at diagnosis of lymphoma | 59 years (IQR 48–67) |
| Non-Hodgkin lymphoma: 34 patients (65%) -Diffuse large B-cell lymphoma: 19 (36%) -Follicular lymphoma: 8 (15%) -Other: 7 (2 mantle cell lymphoma, 2 plasmablastic lymphoma, 1 cutaneous lymphoma, 1 lymphoplasmacytic lymphoma, 1 marginal zone lymphoma) Hodgkin lymphoma: 14 patients (27%) T-cell lymphoma: 4 patients (7.7%) |
| Number of Patients (%) | |
|---|---|
| Symptoms at diagnosis of lymphoma | |
| Adenopathy or mass | 20 (38) |
| Fever | 13 (25) |
| Weight loss | 13 (25) |
| Asthenia | 12 (23) |
| Abdominal pain | 6 (11) |
| Anorexia | 5 (10) |
| Profuse sweating | 5 (10) |
| Pruritus | 2 (4) |
| Asymptomatic | 8 (15) |
| Location of adenopathy or mass | |
| Cervical | 13 (65) |
| Inguinal | 4 (20) |
| Supraclavicular | 3 (15) |
| Mediastinal | 3 (15) |
| Retroperitoneal | 2 (10) |
| Axillar | 2 (10) |
| Ann Arbor stage | |
| Aggressive NHL (n = 24) | |
| I | 6 (25) |
| II | 1 (4) |
| III | 0 (0) |
| IV | 15 (63) |
| Unknown | 2 (8) |
| Hodgkin lymphoma (n = 14) | |
| I | 1 (7) |
| II | 3 (21) |
| III | 4 (29) |
| IV | 3 (21) |
| Unknown | 3 (21) |
| Indolent NHL (n = 10) | |
| I | 2 (20) |
| II | 2 (20) |
| III | 0 (0) |
| IV | 4 (40) |
| Unknown | 2 (20) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerra, I.; Bujanda, L.; Mañosa, M.; Pérez-Martínez, I.; Casanova, M.J.; de la Peña, L.; de Benito, M.; Rivero, M.; Varela, P.; Bernal, L.; et al. Clinical Presentation, Management, and Evolution of Lymphomas in Patients with Inflammatory Bowel Disease: An ENEIDA Registry Study. Cancers 2023, 15, 750. https://doi.org/10.3390/cancers15030750
Guerra I, Bujanda L, Mañosa M, Pérez-Martínez I, Casanova MJ, de la Peña L, de Benito M, Rivero M, Varela P, Bernal L, et al. Clinical Presentation, Management, and Evolution of Lymphomas in Patients with Inflammatory Bowel Disease: An ENEIDA Registry Study. Cancers. 2023; 15(3):750. https://doi.org/10.3390/cancers15030750
Chicago/Turabian StyleGuerra, Ivan, Luis Bujanda, Miriam Mañosa, Isabel Pérez-Martínez, María José Casanova, Luisa de la Peña, Marina de Benito, Montserrat Rivero, Pilar Varela, Lorena Bernal, and et al. 2023. "Clinical Presentation, Management, and Evolution of Lymphomas in Patients with Inflammatory Bowel Disease: An ENEIDA Registry Study" Cancers 15, no. 3: 750. https://doi.org/10.3390/cancers15030750