
Helicobacter Species and Hepato-Biliary Tract Malignancies: A Systematic Review and Meta-Analysis
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Statistical Analysis and Risk of Bias Assessment
3. Results
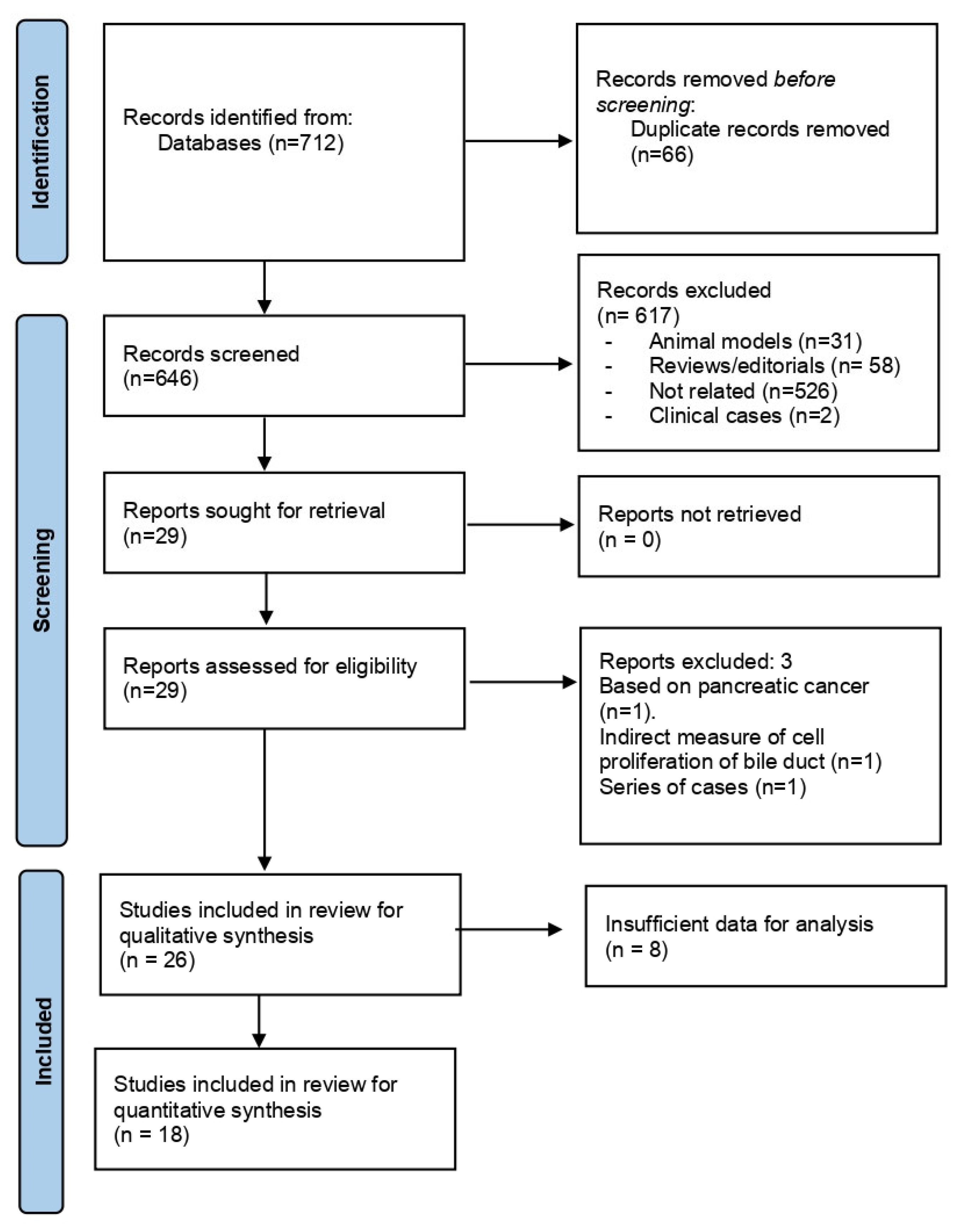
3.1. Description of the Literature Search Strategy
3.2. Search Results and Study Characteristics
3.3. Helicobacter spp. Isolation
3.3.1. Helicobacter spp. under Investigation
3.3.2. Controlling for Confounders and Risk of Bias Assessment
3.3.3. Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de Martel, C.; Franceschi, S. Infections and Cancer: Established Associations and New Hypotheses. Crit. Rev. Oncol. Hematol. 2009, 70, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Murata, M. Inflammation and Cancer. Environ. Health Prev. Med. 2018, 23, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global Burden of Cancer Attributable to Infections in 2018: A Worldwide Incidence Analysis. Lancet Glob. Heal. 2020, 8, e180–e190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic Cancer: A Review of Clinical Diagnosis, Epidemiology, Treatment and Outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef]
- Cherif, S.; Bouriat, K.; Rais, H.; Elantri, S.; Amine, A. Helicobacter Pylori and Biliary Tract Cancers: A Meta-Analysis. Can. J. Infect. Dis. Med. Microbiol. 2020, 2020, 9287157. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.S.; Tsai, C.R.; Chen, L.T. Medical Risk Factors Associated with Cholangiocarcinoma in Taiwan: A Population-Based Case-Control Study. PLoS ONE 2013, 8, e69981. [Google Scholar] [CrossRef]
- Matsukura, N.; Yokomuro, S.; Yamada, S.; Tajiri, T.; Sundo, T.; Hadama, T.; Kamiya, S.; Naito, Z.; Fox, J.G. Association between Helicobacter Bilis in Bile and Biliary Tract Malignancies: H. Bilis in Bile from Japanese and Thai Patients with Benign and Malignant Diseases in the Biliary Tract. Jpn. J. Cancer Res. 2002, 93, 842–847. [Google Scholar] [CrossRef]
- Sripa, B.; Deenonpoe, R.; Brindley, P.J. Co-Infections with Liver Fluke and Helicobacter Species: A Paradigm Change in Pathogenesis of Opisthorchiasis and Cholangiocarcinoma? Parasitol. Int. 2017, 66, 383–389. [Google Scholar] [CrossRef]
- Xiao, M.; Gao, Y.; Wang, Y. Helicobacter Species Infection May Be Associated with Cholangiocarcinoma: A Meta-Analysis. Int. J. Clin. Pract. 2014, 68, 262–270. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Tool to Assess Risk of Bias in Case Control Studies. Contributed by the CLARITY Group at McMaster University. Available online: http://www.distillersr.com/wp-content/uploads/2021/03/Tool-to-Assess-Risk-of-Bias-in-Case-Control-Studies-DistillerSR.pdf (accessed on 1 October 2022).
- Lin, T.T.; Yeh, C.T.; Wu, C.S.; Liaw, Y.F. Detection and Partial Sequence Analysis of Helicobacter Pylori DNA in the Bile Samples. Dig. Dis. Sci. 1995, 40, 2214–2219. [Google Scholar] [CrossRef]
- Roe, I.H.; Kim, J.T.; Lee, H.S.; Lee, J.H. Detection of Helicobacter DNA in Bile from Bile Duct Diseases. J. Korean Med. Sci. 1999, 14, 182–186. [Google Scholar] [CrossRef] [Green Version]
- Myung, S.J.; Kim, M.H.; Shim, K.N.; Kim, Y.S.; Kim, E.O.; Kim, H.J.; Park, E.T.; Yoo, K.S.; Lim, B.C.; Seo, D.W.; et al. Detection of Helicobacter Pylori DNA in Human Biliary Tree and Its Association with Hepatolithiasis. Dig. Dis. Sci. 2000, 45, 1405–1412. [Google Scholar] [CrossRef]
- Avenaud, P.; Marais, A.; Monteiro, L.; Le Bail, B.; Sage, P.B.; Balabaud, C.; Mégraud, F. Detection of Helicobacter Species in the Liver of Patients with and without Primary Liver Carcinoma. Cancer 2000, 89, 1431–1439. [Google Scholar] [CrossRef]
- Bulajic, M.; Maisonneuve, P.; Schneider-Brachert, W.; Müller, P.; Reischl, U.; Stimec, B.; Lehn, N.; Lowenfels, A.B.; Löhr, M. Helicobacter Pylori and the Risk of Benign and Malignant Biliary Tract Disease. Cancer 2002, 95, 1946–1953. [Google Scholar] [CrossRef]
- Fukuda, K.; Kuroki, T.; Tajima, Y.; Tsuneoka, N.; Kitajima, T.; Matsuzaki, S.; Furui, J.; Kanematsu, T. Comparative Analysis of Helicobacter DNAs and Biliary Pathology in Patients with and without Hepatobiliary Cancer. Carcinogenesis 2002, 23, 1927–1931. [Google Scholar] [CrossRef] [Green Version]
- Fallone, C.; Tran, S.; Semret, M.; Discepola, F.; Behr, M.; Barkin, A. Helicobacter DNA in Bile: Correlation with Hepato-Biliary Diseases. Aliment. Pharmacol. Ther. 2003, 17, 453–458. [Google Scholar] [CrossRef]
- Murata, H.; Tsuji, S.; Tsujii, M.; Fu, H.Y.; Tanimura, H.; Tsujimoto, M.; Matsuura, N.; Kawano, S.; Hori, M. Helicobacter Bilis Infection in Biliary Tract Cancer. Aliment. Pharmacol. Ther. Suppl. 2004, 20, 90–94. [Google Scholar] [CrossRef]
- Kobayashi, T.; Harada, K.; Miwa, K.; Nakanuma, Y. Helicobacter Genus DNA Fragments Are Commonly Detectable in Bile from Patients with Extrahepatic Biliary Diseases and Associated with Their Pathogenesis. Dig. Dis. Sci. 2005, 50, 862–867. [Google Scholar] [CrossRef]
- Tiwari, S.K.; Khan, A.A.; Ibrahim, M.; Habeeb, M.A.; Habibullah, C.M. Helicobacter Pylori and Other Helicobacter Species DNA in Human Bile Samples from Patients with Various Hepato-Biliary Diseases. World J. Gastroenterol. 2006, 12, 2181–2186. [Google Scholar] [CrossRef] [PubMed]
- Leelawat, K.; Suksumek, N.; Leelawat, S.; Lek-Uthai, U. Detection of VacA Gene Specific for Helicobactor Pylori in Hepatocellular Carcinoma and Cholangiocarcinoma Specimens of Thai Patients. Southeast Asian J. Trop. Med. Public Health 2007, 38, 881–885. [Google Scholar]
- Bohr, U.R.M.; Kuester, D.; Meyer, F.; Wex, T.; Stillert, M.; Csepregi, A.; Lippert, H.; Roessner, A.; Malfertheiner, P. Low Prevalence of Helicobacteraceae in Gall-Stone Disease and Gall-Bladder Carcinoma in the German Population. Clin. Microbiol. Infect. 2007, 13, 525–531. [Google Scholar] [CrossRef] [Green Version]
- Abu Al-Soud, W.; Stenram, U.; Ljungh, Å.; Tranberg, K.G.; Nilsson, H.O.; Wadström, T. DNA of Helicobacter Spp. and Common Gut Bacteria in Primary Liver Carcinoma. Dig. Liver Dis. 2008, 40, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Shimoyama, T.; Takahashi, R.; Abe, D.; Mizuki, I.; Endo, T.; Fukuda, S. Serological Analysis of Helicobacter Hepaticus Infection in Patients with Biliary and Pancreatic Diseases. J. Gastroenterol. Hepatol. 2010, 25, S86–S89. [Google Scholar] [CrossRef]
- Murakami, K.; Takahashi, R.; Ono, M.; Watanabe, K.; Okimoto, T.; Kodama, M.; Abe, D.; Kimura, M.; Fujioka, T. Serodiagnosis of Helicobacter Hepaticus Infection in Patients with Liver and Gastrointestinal Diseases: Western Blot Analysis and ELISA Using a Highly Specific Monoclonal Antibody for H. Hepaticus Antigen. J. Gastroenterol. 2011, 46, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Yakoob, J.; Khan, M.R.; Abbas, Z.; Jafri, W.; Azmi, R.; Ahmad, Z.; Naeem, S.; Lubbad, L. Helicobacter Pylori: Association with Gall Bladder Disorders in Pakistan. Br. J. Biomed. Sci. 2011, 68, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Boonyanugomol, W.; Chomvarin, C.; Sripa, B.; Bhudhisawasdi, V.; Khuntikeo, N.; Hahnvajanawong, C.; Chamsuwan, A. Helicobacter Pylori in Thai Patients with Cholangiocarcinoma and Its Association with Biliary Inflammation and Proliferation. HPB 2012, 14, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Jahani Sherafat, S.; Tajeddin, E.; Majidi, M.R.S.; Vaziri, F.; Alebouyeh, M.; Alizadeh, A.H.M.; Mojarad, E.N.; Zali, M.R. Lack of Association between Helicobacter Pylori Infection and Biliary Tract Diseases. Polish J. Microbiol. 2012, 61, 319–322. [Google Scholar] [CrossRef]
- Murphy, G.; Michel, A.; Taylor, P.R.; Albanes, D.; Weinstein, S.J.; Virtamo, J.; Parisi, D.; Snyder, K.; Butt, J.; Mcglynn, K.A.; et al. Association of Seropositivity to Helicobacter Species and Biliary Tract Cancer in the ATBC Study. Hepatology 2014, 60, 1963–1971. [Google Scholar] [CrossRef] [Green Version]
- Segura-López, F.K.; Avilés-Jiménez, F.; Güitrón-Cantú, A.; Valdéz-Salazar, H.A.; León-Carballo, S.; Guerrero-Pérez, L.; Fox, J.G.; Torres, J. Infection with Helicobacter Bilis but Not Helicobacter Hepaticus Was Associated with Extrahepatic Cholangiocarcinoma. Helicobacter 2015, 20, 223–230. [Google Scholar] [CrossRef]
- Avilés-Jiménez, F.; Guitron, A.; Segura-López, F.; Méndez-Tenorio, A.; Iwai, S.; Hernández-Guerrero, A.; Torres, J. Microbiota Studies in the Bile Duct Strongly Suggest a Role for Helicobacter Pylori in Extrahepatic Cholangiocarcinoma. Clin. Microbiol. Infect. 2016, 22, 178.e11–178.e22. [Google Scholar] [CrossRef] [Green Version]
- Deenonpoe, R.; Mairiang, E.; Mairiang, P.; Pairojkul, C.; Chamgramol, Y.; Rinaldi, G.; Loukas, A.; Brindley, P.J.; Sripa, B. Elevated Prevalence of Helicobacter Species and Virulence Factors in Opisthorchiasis and Associated Hepatobiliary Disease. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Makkar, R.; Butt, J.; Huang, W.Y.; McGlynn, K.A.; Koshiol, J.; Pawlita, M.; Waterboer, T.; Freedman, N.D.; Murphy, G. Seropositivity for Helicobacter Pylori and Hepatobiliary Cancers in the PLCO Study. Br. J. Cancer 2020, 123, 909–911. [Google Scholar] [CrossRef]
- Jala, I.; Almanfaluthi, M.L.; Laha, T.; Kanthawong, S.; Tangkawattana, S.; Saichua, P.; Suttiprapa, S.; Sripa, B. Helicobacter Pylori Groel Seropositivity Is Associated with an Increased Risk of Opisthorchis Viverrini-Associated Hepatobiliary Abnormalities and Cholangiocarcinoma. Korean J. Parasitol. 2021, 59, 363–368. [Google Scholar] [CrossRef]
- Osaki, T.; Lin, Y.; Sasahira, N.; Ueno, M.; Yonezawa, H.; Hojo, F.; Okuda, M.; Matsuyama, M.; Sasaki, T.; Kobayashi, S.; et al. Prevalence Estimates of Helicobacter Species Infection in Pancreatic and Biliary Tract Cancers. Helicobacter 2022, 27, e12866. [Google Scholar] [CrossRef]
- ATBC Cancer Prevention Study Group. The Alpha-Tocopherol, Beta-Carotene Lung Cancer Prevention Study: Design, Methods, Participant Characteristics, and Compliance. Ann. Epidemiol. 1994, 4, 1–10. [Google Scholar] [CrossRef]
- Hayes, R.B.; Reding, D.; Kopp, W.; Subar, A.F.; Bhat, N.; Rothman, N.; Caporaso, N.; Ziegler, R.G.; Johnson, C.C.; Weissfeld, J.L.; et al. Etiologic and Early Marker Studies in the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial. Control. Clin. Trials 2000, 21, 349S–355S. [Google Scholar] [CrossRef]
- Boonyanugomol, W.; Chomvarin, C.; Hahnvajanawong, C.; Sripa, B.; Kaparakis-Liaskos, M.; Ferrero, R.L. Helicobacter Pylori Cag Pathogenicity Island (CagPAI) Involved in Bacterial Internalization and IL-8 Induced Responses via NOD1- and MyD88-Dependent Mechanisms in Human Biliary Epithelial Cells. PLoS ONE 2013, 8, e77358. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; O’Morain, C.; et al. Management of Helicobacter Pylori Infection: The Maastricht VI/Florence Consensus Report. Gut 2022, 1724–1762. [Google Scholar] [CrossRef]
- Mateos-Muñoz, B.; Pérez-de-la-Serna, J.; Ruiz-de-León, A.; Serrano-Falcón, B.; Casabona-Francés, S.; Velasco-Cerrudo, A.; Rey-Díaz-Rubio, E. Enterohepatic Helicobacter Other than Helicobacter Pylori [Helicobacter Enterohepáticos Distintos de Helicobacter Pylori]. Rev. Esp. Enfermedades Dig. 2013, 105, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Ohshima, H.; Bartsch, H. Chronic Infections and Inflammatory Processes as Cancer Risk Factors: Possible Role of Nitric Oxide in Carcinogenesis. Mutat. Res. Fundam. Mol. Mech. Mutagen. 1994, 305, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Kawanishi, S.; Ohnishi, S.; Ma, N.; Hiraku, Y.; Oikawa, S.; Murata, M. Nitrative and Oxidative DNA Damage in Infection-Related Carcinogenesis in Relation to Cancer Stem Cells. Genes Environ. 2016, 38, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kawanishi, S.; Hiraku, Y.; Pinlaor, S.; Ma, N. Oxidative and Nitrative DNA Damage in Animals and Patients with Inflammatory Diseases in Relation to Inflammation-Related Carcinogenesis. Biol. Chem. 2006, 387, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Labib, P.; Goodchild, G.; Pereira, S. Molecular Pathogenesis of Cholangiocarcinoma. BMC Cancer 2019, 19, 185–201. [Google Scholar] [CrossRef] [Green Version]
- Garcí, A.; Erdman, S.E.; Xu, S.; Feng, Y.; Rogers, A.B.; Schrenzel, M.D.; Murphy, J.C.; Fox, J.G. Hepatobiliary Inflammation, Neoplasia, and Argyrophilic Bacteria in a Ferret Colony. Vet. Pathol. 2002, 39, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Boonyanugomol, W.; Chomvarin, C.; Song, J.Y.; Kim, K.M.; Kim, J.M.; Cho, M.J.; Lee, W.K.; Kang, H.L.; Rhee, K.H.; Sripa, B.; et al. Effects of Helicobacter Pylori C-Glutamyltranspeptidase on Apoptosis and Inflammation in Human Biliary Cells. Dig. Dis. Sci. 2012, 57, 2615–2624. [Google Scholar] [CrossRef]
- Warzecha, Z.; Dembinski, A.; Ceranowicz, P.; Dembinski, M.; Sendur, R.; Wieslawpawlik, W.; Stanislawkonturek, J. Deleterious Effect of Helicobacter Pylori Infection on the Course of Acute Pancreatitis in Rats. Pancreatology 2002, 2, 386–395. [Google Scholar] [CrossRef]
- Thanaphongdecha, P.; Karinshak, S.E.; Ittiprasert, W.; Mann, V.H.; Chamgramol, Y.; Pairojkul, C.; Fox, J.G.; Suttiprapa, S.; Sripa, B.; Brindley, P.J. Infection with Helicobacter Pylori Induces Epithelial to Mesenchymal Transition in Human Cholangiocytes. Pathogens 2020, 9, 971. [Google Scholar] [CrossRef]
- Avenaud, P.; Le Bail, B.; Mayo, K.; Marais, A.; Fawaz, R.; Bioulac-Sage, P.; Megraud, F. Natural History of Helicobacter Hepaticus Infection in Conventional A/J Mice, with Special Reference to Liver Involvement. Infect. Immun. 2003, 71, 3667–3672. [Google Scholar] [CrossRef] [Green Version]
- Scholte, L.L.S.; Pascoal-Xavier, M.A.; Nahum, L.A. Helminths and Cancers from the Evolutionary Perspective. Front. Med. 2018, 5, 90. [Google Scholar] [CrossRef]
- Suyapoh, W.; Tirnitz-Parker, J.E.E.; Tangkawattana, S.; Suttiprapa, S.; Sripa, B. Biliary Migration, Colonization, and Pathogenesis of o. Viverrini Co-Infected with Caga+ Helicobacter Pylori. Pathogens 2021, 10, 1089. [Google Scholar] [CrossRef]
- Prueksapanich, P.; Piyachaturawat, P.; Aumpansub, P.; Ridtitid, W.; Chaiteerakij, R.; Rerknimitr, R. Liver Fluke-Associated Biliary Tract Cancer. Gut Liver 2018, 12, 236–245. [Google Scholar] [CrossRef] [Green Version]
- Deenonpoe, R.; Chomvarin, C.; Pairojkul, C.; Chamgramol, Y.; Loukas, A.; Brindley, P.J.; Sripa, B. The Carcinogenic Liver Fluke Opisthorchis Viverrini Is a Reservoir for Species of Helicobacter. Asian Pacific J. Cancer Prev. 2015, 16, 1751–1758. [Google Scholar] [CrossRef] [Green Version]
- Zhou, D.; Zhang, Y.; Gong, W.; Mohamed, S.O.; Ogbomo, H.; Wang, X.; Liu, Y.; Quan, Z. Are Helicobacter Pylori and Other Helicobacter Species Infection Associated with Human Biliary Lithiasis? A Meta-Analysis. PLoS ONE 2011, 6, e27390. [Google Scholar] [CrossRef]
- Wang, L.; Chen, J.; Jiang, W.; Cen, L.; Pan, J.; Yu, C.; Li, Y.; Chen, W.; Chen, C.; Shen, Z. The Relationship between Helicobacter Pylori Infection of the Gallbladder and Chronic Cholecystitis and Cholelithiasis: A Systematic Review and Meta-Analysis. Can. J. Gastroenterol. Hepatol. 2021, 2021, 1–11. [Google Scholar] [CrossRef]
- Tsuchiya, Y.; Mishra, K.; Kapoor, V.K.; Vishwakarma, R.; Behari, A.; Ikoma, T.; Asai, T.; Endoh, K.; Nakamura, K. Plasma Helicobacter Pylori Antibody Titers and Helicobacter Pylori Infection Positivity Rates in Patients with Gallbladder Cancer or Cholelithiasis: A Hospital-Based Case-Control Study. Asian Pacific J. Cancer Prev. 2018, 19, 1911–1915. [Google Scholar] [CrossRef]
- Cen, L.; Pan, J.; Zhou, B.; Yu, C.; Li, Y.; Chen, W.; Shen, Z. Helicobacter Pylori Infection of the Gallbladder and the Risk of Chronic Cholecystitis and Cholelithiasis: A Systematic Review and Meta-Analysis. Helicobacter 2018, 23, e12457. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Imran, A.; Shami, A.; Chaudhary, A.A.; Khan, S. Decipher the Helicobacter Pylori Protein Targeting in the Nucleus of Host Cell and Their Implications in Gallbladder Cancer: An Insilico Approach. J. Cancer 2021, 12, 7214–7222. [Google Scholar] [CrossRef]
- Sharma, A.; Sharma, K.L.; Gupta, A.; Yadav, A.; Kumar, A. Gallbladder Cancer Epidemiology, Pathogenesis and Molecular Genetics: Recent Update. World J. Gastroenterol. 2017, 23, 3978–3998. [Google Scholar] [CrossRef]
- Zhou, D.; Wang, J.; Weng, M.; Zhang, Y.; Wang, X.; Gong, W.; Quan, Z. Infections of Helicobacter Spp. in the Biliary System Are Associated with Biliary Tract Cancer. Eur. J. Gastroenterol. Hepatol. 2013, 25, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Schulte, A.; Pandeya, N.; Fawcett, J.; Fritschi, L.; Risch, H.A.; Webb, P.M.; Whiteman, D.C.; Neale, R.E. Association between Helicobacter Pylori and Pancreatic Cancer Risk: A Meta-Analysis. Cancer Causes Control 2015, 26, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Liu, W.; Wu, J. Helicobacter Pylori Infection and Pancreatic Cancer Risk: A Meta-Analysis. J. Cancer Res. Ther. 2016, 12, 229. [Google Scholar] [CrossRef]
- Itoh, M.; Wada, K.; Tan, S.; Kitano, Y.; Kai, J.; Makino, I. Antibacterial Action of Bile Acids against Helicobacter Pylori and Changes in Its Ultrastructural Morphology: Effect of Unconjugated Dihydroxy Bile Acid. J. Gastroenterol. 1999, 34, 571–576. [Google Scholar] [CrossRef]
- Abdelmalek, S.; Shokry, K.; Hamed, W.; Abdelnaser, M.; Aboubakr, A.; Elenin, S.A.; Ali, M.; Mostafa, M.; Abou-Okada, M. The Validity Evaluation of Different 16srRNA Gene Primers for Helicobacter Detection Urgently Requesting to Design New Specific Primers. Sci. Rep. 2022, 12, 1–11. [Google Scholar] [CrossRef]
- Miftahussurur, M.; Yamaoka, Y. Diagnostic Methods of Helicobacter Pylori Infection for Epidemiological Studies: Critical Importance of Indirect Test Validation. Biomed Res. Int. 2016, 2016, 4819423. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.; Xu, Z.; Zhang, T.; Li, Y.; Li, W.; Tan, H. Whole-Genome-Based Helicobacter Pylori Geographic Surveillance: A Visualized and Expandable Webtool. Front. Microbiol. 2021, 12, 1769. [Google Scholar] [CrossRef]
- Ford, A.C.; Tsipotis, E.; Yuan, Y.; Leontiadis, G.I.; Moayyedi, P. Efficacy of Helicobacter Pylori Eradication Therapy for Functional Dyspepsia: Updated Systematic Review and Meta-Analysis. Gut 2022, 71, 1967–1975. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Specimen Type | Detection Method | Type of Malignancy in Case Group | Control Group | H. spp. Type | H. spp. + in Case Group | H. spp. + in Control Group | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Lin TT et al. [13] | 1995 | Taiwan | Gastric tissue & bile | PCR & CLOtest | PC, CCA, GC | Chronic cholecystitis | HP | PCR: 4/6 CLOtest 0/6 | PCR 0/1 CLOtest 0/1 | NR |
| Roe IH et al. [14] | 1999 | Korea | Bile | PCR & culture | CCA & PC | GS | H. spp. | PCR 9/21 Culture 0/21 | PCR 3/11 CLOtest 0/11 | NR |
| Myung SJ et al. [15] | 2000 | Korea | Bile, biliary tissue, GS & serum | PCR, ELISA, CLOtest & histology | G1: Hepatolithiasis, CCA, BS, papilomatosis, cystoadenocarcinoma. G2 (cholecystectomies) GS & GB polyp | GC | HP | Serum G1: 37/43 Serum G2: 20/23 PCR G1: 7/43 PCR G2: 0/23 CLOtest & histology G1 0/43, G2 0/23 | Serum 6/8 Histopathology and CLOtest 0/8 | NR |
| Avenaud P et al. [16] | 2000 | France | Liver tissue | PCR, culture & histology | HCC, CCA, hepatoCCA | PSC, Caroli, Hepatocellular adenoma, focal nodular hyperplasia | H. spp. | PCR 8/8 (7/8 H.Pylori & 1/8 H. Felis) Culture & histology 0/8 | PCR 1/8 Culture & histology 0/8 | NR |
| Bulajic M et al. [17] | 2002 | Yugoslavia | Gastric tissue & bile | PCR & CLOtest | BTC (GBC, CCA, Klatskin) & GS | PBC, Caroli, no stones/malignancy or not specified | H. spp. | PCR BTC 14/15 PCR GS 52/63 CLOtest BTC 12/15 CLOtest GS 37/63 | PCR 3/11 CLOtest 4/11 | BTC OR 9.9 (1.4–70.5) |
| Fukuda K et al. [18] | 2002 | Japan | Liver tissue & bile | PCR & IHQ | CCA, GBC & AoVC | GS, GB polyps, GB adenomyomatosis, | H. spp. | PCR bile 6/17 PCR tissue 8/16 IHQ 0/0 | PCR 1/19 IHQ 3/19 | BTC & H. spp. F value 5.05 (p = 0.041) |
| Matsukura N et al. [8] | 2002 | Japan & Thailand | Bile | PCR | Japan group: GS, BTC (CCA, GBC) Thai group: GS, BTC (CCA, GBC) | Non biliary disease | H. bilis | Japan: GS 9/16 Japan: BTC 13/15 Thai: GS 10/26 Thai: BTC 11/14 | Japan 4/14 | Japanese BTC OR 6.5 (1.09–38.63) Thai BTC OR 5.86 (1.21–26.33) Overall OR 6.4 (2.05–20.03) |
| Fallone CA et al. [19] | 2003 | Canada | Bile | PCR | CCA, AoVC, PC | GS, biliary stricture, pancreatitis, PSC & others not specified | H. spp. | 0/15 | 0/110 | NR |
| Murata H et al. [20] | 2004 | Japan | Gallbladder tissue | PCR | GBC, CCA, PC | GS | H. bilis | 4/18 | 2/16 | NR |
| Kobayashi T et al. [21] | 2005 | Japan | Bile | PCR & culture | BTC (GBC, CCA), GS | Non biliary disease | H. spp. | BTC: 5/6 GS 16/30 | 2/21 | BTC vs. GCC H. spp. p < 0.05 |
| Tiwari SK et al. [22] | 2006 | India | Gastric tissue & bile | PCR, CLOtest & culture | Hepatobiliary disorder (CCA, PC & others) | Gastric disorders | HP | Bile 29/30 Gastric 26/30 | Bile 2/30 Gastric 28/30 | NR |
| Leelawat K et al. [23] | 2007 | Thailand | Liver tissue | PCR | HCC & CCA | Liver metastasis from CRC, IH duct stones | HP VacA | 18/18 | 5/7 | NR |
| Bohr URM et al. [24] | 2007 | Germany | Gallbladder tissue | PCR, culture & IHQ | GBC & GB disease | Cholecystectomy | H. spp. | GBC 0/20 GBD 1/57 IHQ 0/77 Culture 0/77 | 0/22 | NR |
| Al-Soud WA et al. [25] | 2008 | Sweden | Liver tissue | PCR | HCC & CCA | Hepatocellular adenoma, focal nodular hyperplasia, fatty lesion & hematoma | H. spp. | HCC 7/12 CCA 8/13 | 3/24 | p < 0.01 |
| Shimoyama T et al. [26] | 2010 | Japan | Serum | Western Blot | GS, BTC (CCA, GBC), PC | Patients undergoing endoscopy with no gastric ulcer or cancer | H. hepaticus | GS 11/55 BTC 7/18 PC 2/19 | 4/34 | BTC vs. controls p < 0.05 |
| Murakami K et al. [27] | 2011 | Japan | Serum | ELISA | Liver disease, Upper GI disease, Lower GI disease, biliary tract disease, pancreas disease | Healthy blood donors | H. hepaticus | LD 34/69 UGID 6/38 LGID 1/17 BTD 6/26 PD 3/16 | 8/30 | H.hepaticus in LD vs. all the other groups p < 0.05 for each comparison |
| Yakoob J et al. [28] | 2011 | Pakistan | Gallbladder tissue & bile | PCR | GB polyps & GBC | Chronic cholecystitis | H. spp. | 5/55 | 28/89 | p = 0.03 |
| Boonyanugamol W et al. [29] | 2012 | Thailand | Bile, liver tissue, gallbladder tissue & gallstones | PCR & culture | CCA, GS, CCA, PC | Autopsies | H. spp. | CCA 58/87 GS 22/53 | 4/16 | p < 0.05 |
| Jahani S et al. [30] | 2012 | Iran | Bile | PCR & culture | BTC, PC | Gallstones, other diseases not cancer | H. spp. | PCR 1/15 Culture 0/15 | PCR 3/87 | NR |
| Murphy G et al. [31] | 2014 | Finland | Serum | Multiplex assay | BTC (GBC, CCA, AoVC), LC (IHDC, HCC) | Patients from ATBC study * | H. spp. | HP + BTC: 62/64 LC: 115/122 | 198/224 | OR for overall cases 2.63 (1.08–6.37) OR for BTC 5.47 (1.17–25.65) |
| Segura-López FK et al. [32] | 2015 | Mexico | Bile | PCR | CCA, AoVC, GBC | Benign biliary pathology | H. spp. | H.Bilis 44/103 H.Hepaticus 17/103 | H.Bilis 19/91 H.Hepaticus 13/91 | H. bilis & CCA OR 2.83(1.49–5.32) H. hepaticus & CCA OR 1.19 (0.54–2.60) |
| Aviles-Jiménez et al. [33] | 2016 | Mexico | Bile | PCR | BTC | Benign biliary pathology | HP | VacA &/or CagA+ 75/100 VacA+ 50/97 CagA+ 46/100 | VacA&/or CagA + 52/92 VacA+: 21/86 CagA+: 39/92 | HP + p = 0.035 VacA + p = 0.0003 |
| Deenonpoe R et al. [34] | 2017 | Thailand | Feces | PCR | OV + patients | OV- patients | H. spp. | HP+: 190/293 H.Bilis: 86/293 Both HP + HB: 79/293 | HP+: 77/260 H.Bilis 14/260 Both HP + HB: 10/260 | H. spp. more freq in OV+ p < 0.0001 Advanced periductal fibrosis in OV + HP+ cagA RRR 3.38 (1.52–7.58) |
| Makkar M et al. [35] | 2020 | Germany | Serum | PCR | CCA, HCC | Patients from the PLCO trial with no cancer ** | HP | CCA 35/74 HCC 57/105 | 162/357 | HP CagA+ HCC OR 1.96 (1.21–2.18) HP CagA + BTC OR 2.16 (1.03–4.50) |
| Jala I et al. [36] | 2021 | Thailand | Serum | ELISA | OV + with no HB abnormalities; OV+ with HB abnormalities, OV+ CCA | OV- patients with no HB abnormalities | HP | pCagA+: OV+ no HBA: 112/140 OV+ HBA: 119/144 OV + CCA: 117/145 GroEL+ OV+ no HBA: 98/140 OV + HBA: 117/144 OV + CCA: 118/145 | pCagA+: 98/122 GroEL+ 82/122 | HP + OV + OR for HBA 2.11 (1.20–3.71) OR for CCA 2.13 (1.21–3.75) |
| Osaki T et al. [37] | 2022 | Japan | Serum, bile, and biliary tissue | PCR, ELISA & culture | BTC (CCA, AoVC, GBC), PC | Cholelythiasis, GC, CRC & other suspected cancers not specified | H. hepaticus & H. bilis | PCR H. bilis BTC 2/35; PC 6/59 PCR H. hepaticus BTC 2/35; PC 1/59 ELISA H. bilis BTC 13/37; PC 24/59 ELISA H. hepaticus BTC 11/37; PC 19/59 | PCR H. bilis: 3/21 PCR H. hepaticus 1/21 ELISA H. bilis 8/21 ELISA H. hepaticus 7/21 | HB+ and HH+ PC vs. controls p = 0.046 |
| Study | Assessment of Exposure | Outcome of Interest in Cases but Not Controls | Cases Selection | Controls Selection | Case-Control Matching and Adjusted for Confounders |
|---|---|---|---|---|---|
| Lin TT et al. [13] | A | C | D | C | D |
| Roe IH et al. [14] | A | C | C | B | D |
| Myung SJ et al. [15] | A | C | B | A | D |
| Avenaud P et al. [16] | A | B | B | C | D |
| Bulajic M et al. [17] | A | B | A | B | B |
| Fukuda K et al. [18] | A | B | A | C | C |
| Matsukura N et al. [8] | A | B | A | C | D |
| Fallone CA et al. [19] | A | B | A | C | D |
| Murata H et al. [20] | A | B | A | C | D |
| Kobayashi T et al. [21] | A | B | A | B | D |
| Tiwari SK et al. [22] | A | C | A | C | D |
| Leelawat K et al. [23] | B | B | A | C | D |
| Bohr URM et al. [24] | A | B | A | B | B |
| Al-Soud WA et al. [25] | A | A | A | B | D |
| Shimoyama T et al. [26] | B | B | A | B | D |
| Murakami K et al. [27] | B | C | C | B | D |
| Yakoob J et al. [28] | A | C | B | C | D |
| Boonyanugamol W et al. [29] | A | B | A | B | D |
| Jahani S et al. [30] | A | B | A | C | D |
| Murphy G et al. [31] | B | A | A | A | B |
| Segura-López FK et al. [32] | A | B | A | B | B |
| Aviles-Jiménez et al. [33] | A | B | A | B | B |
| Deenonpoe R et al. [34] | B | A | B | B | B |
| Makkar M et al. [35] | B | A | A | B | A |
| Jala I et al. [36] | B | A | A | A | B |
| Osaki T et al. [37] | A | B | A | C | C |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gros, B.; Gómez Pérez, A.; Pleguezuelo, M.; Serrano Ruiz, F.J.; de la Mata, M.; Rodríguez-Perálvarez, M. Helicobacter Species and Hepato-Biliary Tract Malignancies: A Systematic Review and Meta-Analysis. Cancers 2023, 15, 595. https://doi.org/10.3390/cancers15030595
Gros B, Gómez Pérez A, Pleguezuelo M, Serrano Ruiz FJ, de la Mata M, Rodríguez-Perálvarez M. Helicobacter Species and Hepato-Biliary Tract Malignancies: A Systematic Review and Meta-Analysis. Cancers. 2023; 15(3):595. https://doi.org/10.3390/cancers15030595
Chicago/Turabian StyleGros, Beatriz, Alberto Gómez Pérez, María Pleguezuelo, Francisco Javier Serrano Ruiz, Manuel de la Mata, and Manuel Rodríguez-Perálvarez. 2023. "Helicobacter Species and Hepato-Biliary Tract Malignancies: A Systematic Review and Meta-Analysis" Cancers 15, no. 3: 595. https://doi.org/10.3390/cancers15030595