
Radiomics and Clinicopathological Characteristics for Predicting Lymph Node Metastasis in Testicular Cancer
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
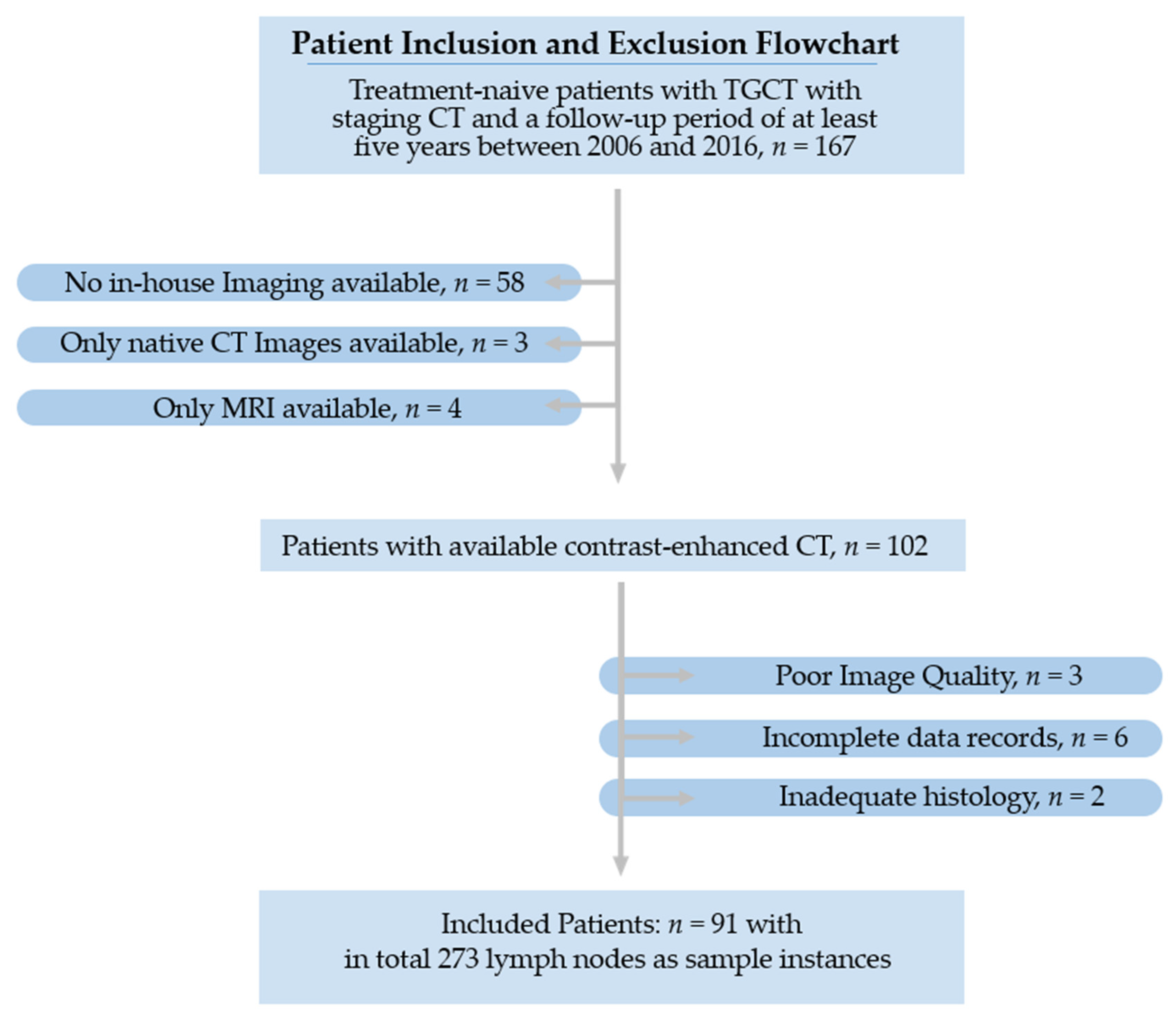
2.1. Patients
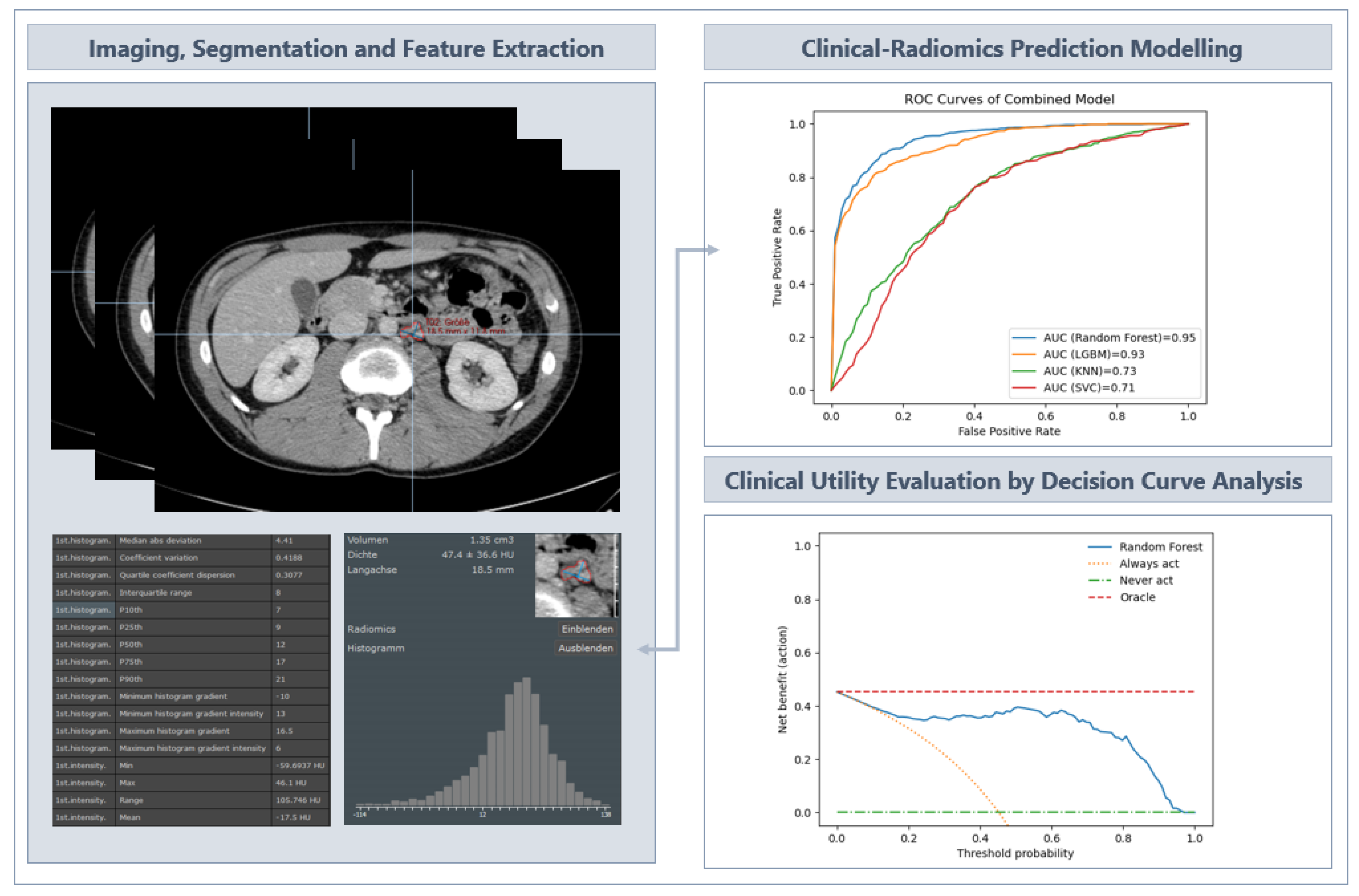
2.2. Image Acquisition and Segmentation
2.3. Segmentation and Radiomics Feature Extraction
2.4. Development of the Predictive Machine Learning Models
3. Results
3.1. Clinicopathological Characteristics
3.2. Dataset Characteristics and Preprocessing
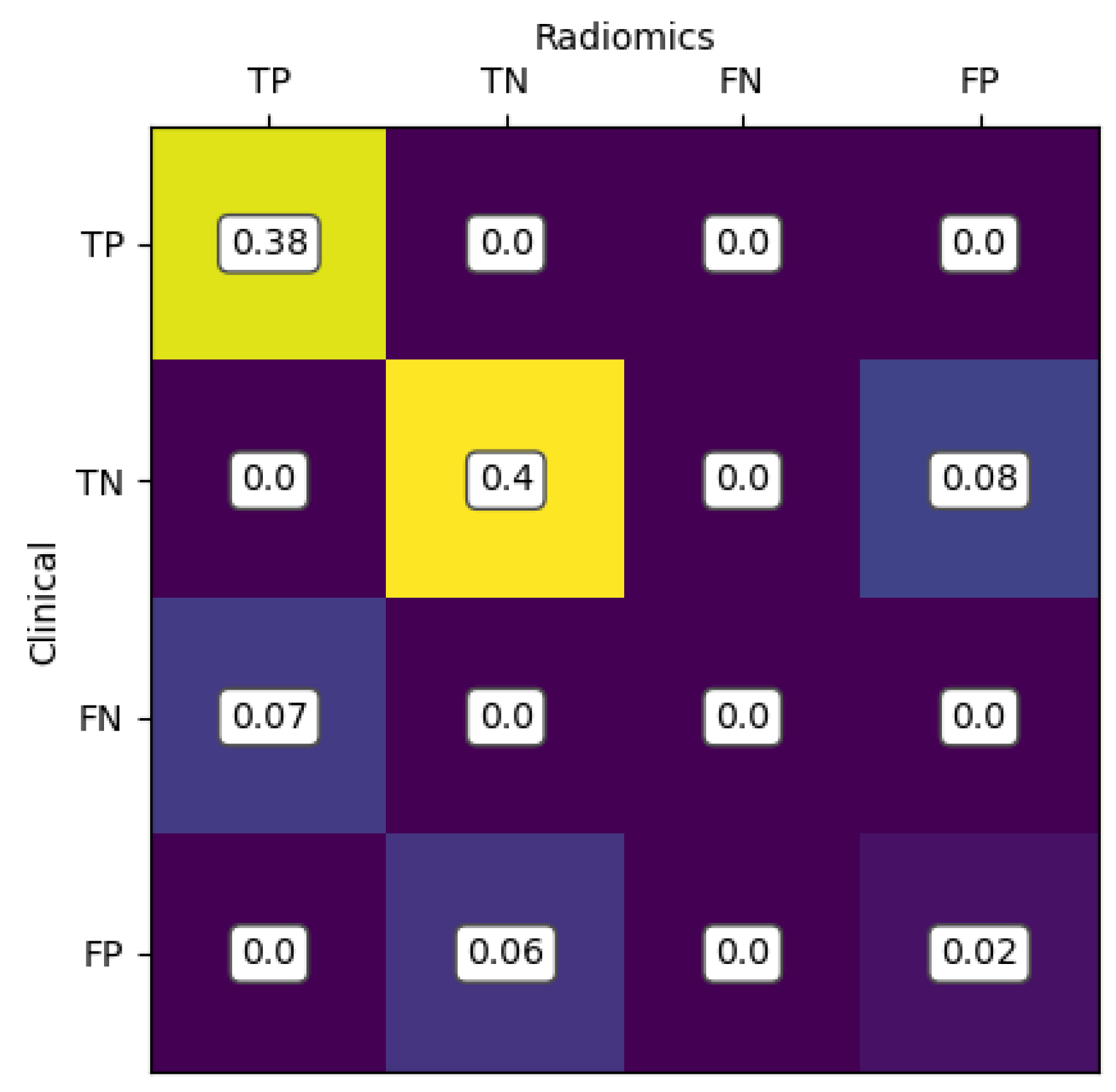
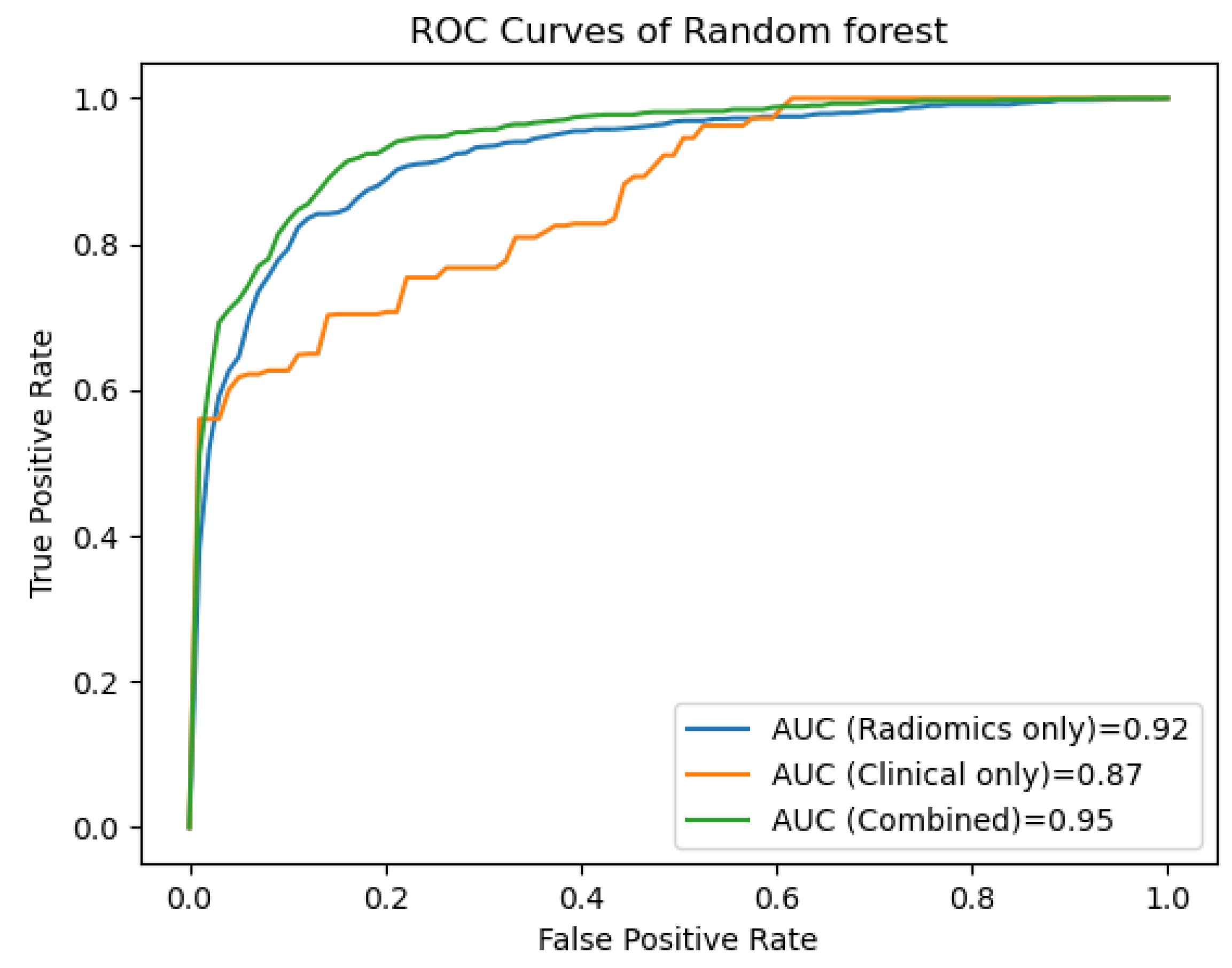
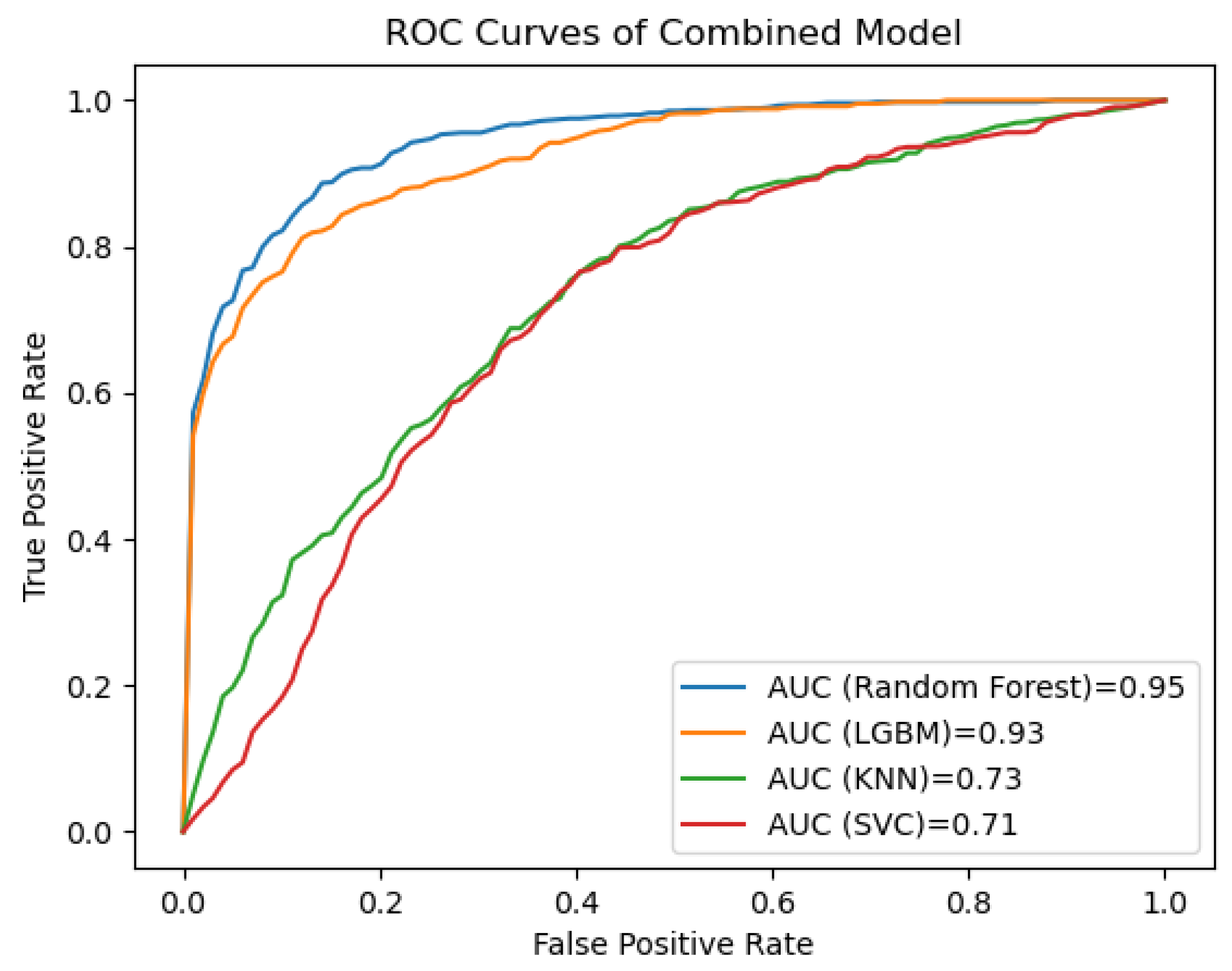
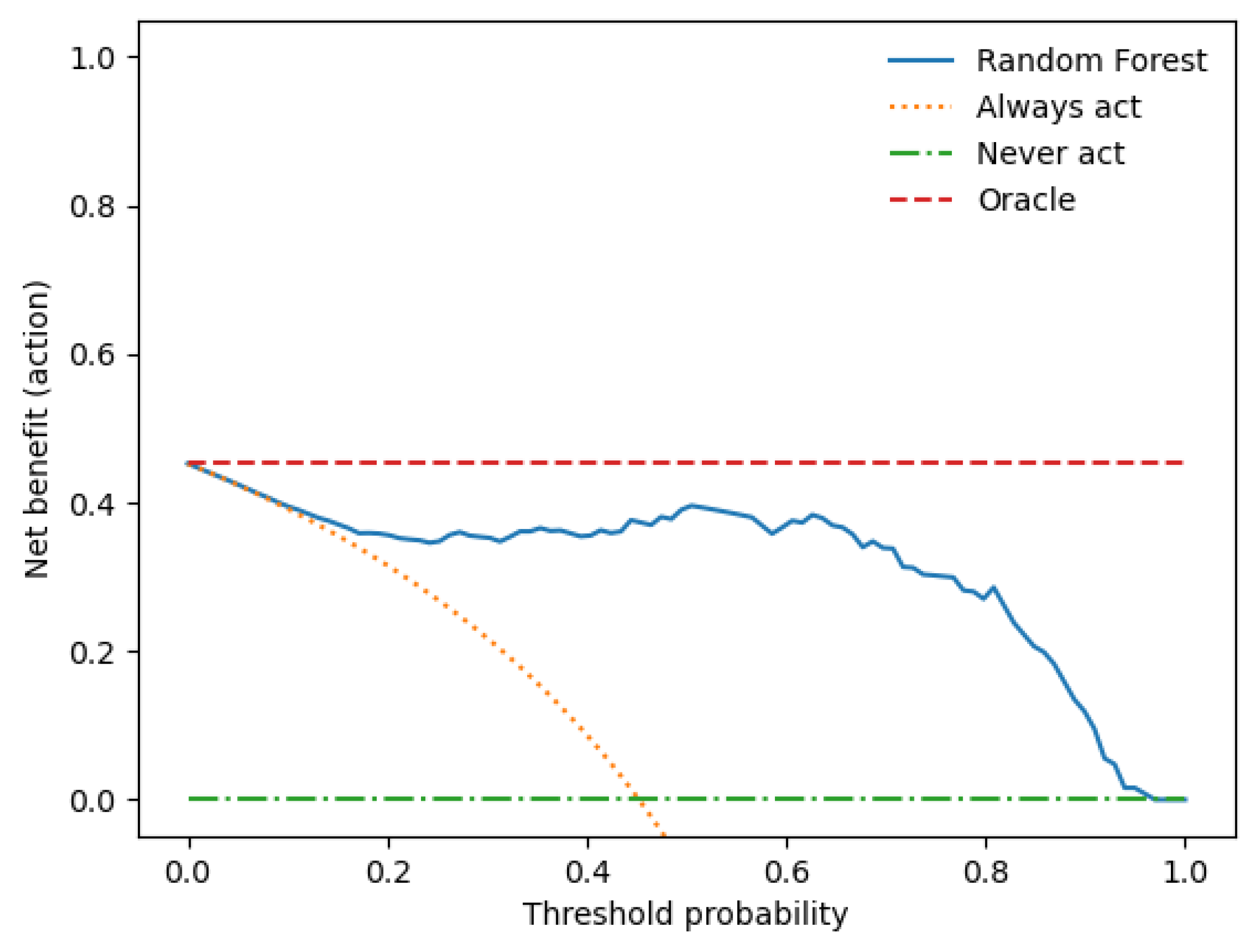
3.3. Performance Evaluation of the Prediction Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AFP | Alpha-fetoprotein |
| AUC | Area under the curve |
| CT | Computed tomography |
| hCG | Human chorionic gonadotropin |
| KNN | K-Nearest Neighbours |
| LGBM | Light Gradient Boosting Machine |
| LNs | Lymph nodes |
| LNM | Lymph node metastases |
| LR | Logistic regression |
| ML | Machine learning |
| RF | Random Forest |
| ROC | Receiver operating curve |
| ROI | Region of interest |
| SVC | Support Vector Machine Classifier |
| TGCT | Testicular germ cell tumour |
References
- Ruf, C.G.; Isbarn, H.; Wagner, W.; Fisch, M.; Matthies, C.; Dieckmann, K.-P. Changes in Epidemiologic Features of Testicular Germ Cell Cancer: Age at Diagnosis and Relative Frequency of Seminoma Are Constantly and Significantly Increasing. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 33.e1–33.e6. [Google Scholar] [CrossRef]
- Bray, F.; Richiardi, L.; Ekbom, A.; Pukkala, E.; Cuninkova, M.; Møller, H. Trends in Testicular Cancer Incidence and Mortality in 22 European Countries: Continuing Increases in Incidence and Declines in Mortality. Int. J. Cancer 2006, 118, 3099–3111. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2018. CA A Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Ghazarian, A.A.; Kelly, S.P.; Altekruse, S.F.; Rosenberg, P.S.; McGlynn, K.A. Future of Testicular Germ Cell Tumor Incidence in the United States: Forecast through 2026. Cancer 2017, 123, 2320–2328. [Google Scholar] [CrossRef]
- Znaor, A.; Skakkebaek, N.E.; Rajpert-De Meyts, E.; Kuliš, T.; Laversanne, M.; Gurney, J.; Sarfati, D.; McGlynn, K.A.; Bray, F. Global Patterns in Testicular Cancer Incidence and Mortality in 2020. Int. J. Cancer 2022, 151, 692–698. [Google Scholar] [CrossRef]
- Beyer, J.; Collette, L.; Sauvé, N.; Daugaard, G.; Feldman, D.R.; Tandstad, T.; Tryakin, A.; Stahl, O.; Gonzalez-Billalabeitia, E.; De Giorgi, U. Survival and New Prognosticators in Metastatic Seminoma: Results from the IGCCCG-Update Consortium. J. Clin. Oncol. 2021, 39, 1553. [Google Scholar] [CrossRef]
- Gillessen, S.; Sauvé, N.; Collette, L.; Daugaard, G.; de Wit, R.; Albany, C.; Tryakin, A.; Fizazi, K.; Stahl, O.; Gietema, J.A. Predicting Outcomes in Men with Metastatic Nonseminomatous Germ Cell Tumors (NSGCT): Results from the IGCCCG Update Consortium. J. Clin. Oncol. 2021, 39, 1563–1574. [Google Scholar] [CrossRef]
- Einhorn, L.H. Treatment of Testicular Cancer: A New and Improved Model. J. Clin. Oncol. 1990, 8, 1777–1781. [Google Scholar] [CrossRef]
- Gurney, J.K.; Florio, A.A.; Znaor, A.; Ferlay, J.; Laversanne, M.; Sarfati, D.; Bray, F.; McGlynn, K.A. International Trends in the Incidence of Testicular Cancer: Lessons from 35 Years and 41 Countries. Eur. Urol. 2019, 76, 615–623. [Google Scholar] [CrossRef]
- Huang, J.; Chan, S.C.; Tin, M.S.; Liu, X.; Lok, V.T.-T.; Ngai, C.H.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.-J.; et al. Worldwide Distribution, Risk Factors, and Temporal Trends of Testicular Cancer Incidence and Mortality: A Global Analysis. Eur. Urol. Oncol. 2022, 5, 566–576. [Google Scholar] [CrossRef]
- Chovanec, M.; Cheng, L. Advances in Diagnosis and Treatment of Testicular Cancer. BMJ 2022, 379, e070499. [Google Scholar] [CrossRef]
- Schmiedel, S.; Schüz, J.; Skakkebæk, N.E.; Johansen, C. Testicular Germ Cell Cancer Incidence in an Immigration Perspective, Denmark, 1978 to 2003. J. Urol. 2010, 183, 1378–1382. [Google Scholar] [CrossRef]
- Wilkinson, P.M.; Read, G. International Germ Cell Consensus Classification: A Prognostic Factor-Based Staging System for Metastatic Germ Cell Cancers. International Germ Cell Cancer Collaborative Group. J. Clin. Oncol. 1997, 15, 594–603. [Google Scholar]
- Gilligan, T.; Lin, D.W.; Aggarwal, R.; Chism, D.; Cost, N.; Derweesh, I.H.; Emamekhoo, H.; Feldman, D.R.; Geynisman, D.M.; Hancock, S.L. Testicular Cancer, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 1529–1554. [Google Scholar] [CrossRef]
- Oldenburg, J.; Berney, D.; Bokemeyer, C.; Climent, M.; Daugaard, G.; Gietema, J.; De Giorgi, U.; Haugnes, H.; Huddart, R.; Leão, R. Testicular Seminoma and Non-Seminoma: ESMO-EURACAN Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2022, 33, 362–375. [Google Scholar] [CrossRef]
- Kliesch, S.; Schmidt, S.; Wilborn, D.; Aigner, C.; Albrecht, W.; Bedke, J.; Beintker, M.; Beyersdorff, D.; Bokemeyer, C.; Busch, J. Management of Germ Cell Tumours of the Testis in Adult Patients. German Clinical Practice Guideline Part I: Epidemiology, Classification, Diagnosis, Prognosis, Fertility Preservation, and Treatment Recommendations for Localized Stages. Urol. Int. 2021, 105, 169–180. [Google Scholar] [CrossRef]
- Winter, C.; Zengerling, F.; Busch, J.; Heinzelbecker, J.; Pfister, D.; Ruf, C.; Lackner, J.; Albers, P.; Kliesch, S.; Schmidt, S. How to Classify, Diagnose, Treat and Follow-up Extragonadal Germ Cell Tumors? A Systematic Review of Available Evidence. World J. Urol. 2022, 40, 2863–2878. [Google Scholar] [CrossRef]
- Ferraro, S.; Trevisiol, C.; Gion, M.; Panteghini, M. Human Chorionic Gonadotropin Assays for Testicular Tumors: Closing the Gap between Clinical and Laboratory Practice. Clin. Chem. 2018, 64, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Dieckmann, K.-P.; Simonsen-Richter, H.; Kulejewski, M.; Anheuser, P.; Zecha, H.; Isbarn, H.; Pichlmeier, U. Serum Tumour Markers in Testicular Germ Cell Tumours: Frequencies of Elevated Levels and Extents of Marker Elevation Are Significantly Associated with Clinical Parameters and with Response to Treatment. BioMed Res. Int. 2019, 2019, 5030349. [Google Scholar] [CrossRef] [PubMed]
- de Wit, M.; Brenner, W.; Hartmann, M.; Kotzerke, J.; Hellwig, D.; Lehmann, J.; Franzius, C.; Kliesch, S.; Schlemmer, M.; Tatsch, K. [18F]-FDG–PET in Clinical Stage I/II Non-Seminomatous Germ Cell Tumours: Results of the German Multicentre Trial. Ann. Oncol. 2008, 19, 1619–1623. [Google Scholar] [CrossRef]
- Huddart, R.A.; O’Doherty, M.J.; Padhani, A.; Rustin, G.J.; Mead, G.M.; Joffe, J.K.; Vasey, P.; Harland, S.J.; Logue, J.; Daugaard, G. 18fluorodeoxyglucose Positron Emission Tomography in the Prediction of Relapse in Patients with High-Risk, Clinical Stage I Nonseminomatous Germ Cell Tumors: Preliminary Report of MRC Trial TE22—The NCRI Testis Tumour Clinical Study Group. J. Clin. Oncol. 2007, 25, 3090–3095. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, T.D.; Hayes, D.F.; Seidenfeld, J.; Temin, S. ASCO Clinical Practice Guideline on Uses of Serum Tumor Markers in Adult Males with Germ Cell Tumors. J. Oncol. Pract. 2010, 6, 199. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.J.; Huddart, R.A.; Coleman, N. The Present and Future of Serum Diagnostic Tests for Testicular Germ Cell Tumours. Nat. Rev. Urol. 2016, 13, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, S.; Panteghini, M. A Step Forward in Identifying the Right Human Chorionic Gonadotropin Assay for Testicular Cancer. Clin. Chem. Lab. Med. (CCLM) 2020, 58, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Albers, P.; Albrecht, W.; Algaba, F.; Bokemeyer, C.; Cohn-Cedermark, G.; Fizazi, K.; Horwich, A.; Laguna, M.P.; Nicolai, N.; Oldenburg, J. Guidelines on Testicular Cancer: 2015 Update. Eur. Urol. 2015, 68, 1054–1068. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.; Gerl, A.; Fossa, S.; Sleijfer, D.; de Wit, R.; Kirkels, W.; Schmeller, N.; Clemm, C.; Habbema, J.; Keizer, H. Validity of Predictions of Residual Retroperitoneal Mass Histology in Nonseminomatous Testicular Cancer. J. Clin. Oncol. 1998, 16, 269–274. [Google Scholar] [CrossRef]
- Vergouwe, Y.; Steyerberg, E.W.; Foster, R.S.; Habbema, J.D.F.; Donohue, J.P. Validation of a Prediction Model and Its Predictors for the Histology of Residual Masses in Nonseminomatous Testicular Cancer. J. Urol. 2001, 165, 84–88. [Google Scholar] [CrossRef]
- Lisson, C.S.; Manoj, S.; Wolf, D.; Schrader, J.; Schmidt, S.A.; Beer, M.; Goetz, M.; Zengerling, F.; Lisson, C.G.S. CT Radiomics and Clinical Feature Model to Predict Lymph Node Metastases in Early-Stage Testicular Cancer. Onco 2023, 3, 65–80. [Google Scholar] [CrossRef]
- Obermeyer, Z.; Emanuel, E.J. Predicting the Future—Big Data, Machine Learning, and Clinical Medicine. N. Engl. J. Med. 2016, 375, 1216. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.; Deist, T.M.; Peerlings, J.; De Jong, E.E.; Van Timmeren, J.; Sanduleanu, S.; Larue, R.T.; Even, A.J.; Jochems, A. Radiomics: The Bridge between Medical Imaging and Personalized Medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-Based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Tang, L.; Li, Z.-Y.; Fang, M.-J.; Gao, J.-B.; Shan, X.-H.; Ying, X.-J.; Sun, Y.-S.; Fu, J.; Wang, X.-X. Development and Validation of an Individualized Nomogram to Identify Occult Peritoneal Metastasis in Patients with Advanced Gastric Cancer. Ann. Oncol. 2019, 30, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Liang, C.; He, L.; Tian, J.; Liang, C.; Chen, X.; Ma, Z.; Liu, Z. Development and Validation of a Radiomics Nomogram for Preoperative Prediction of Lymph Node Metastasis in Colorectal Cancer. J. Clin. Oncol. 2016, 34, 2157–2164. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zheng, J.; Li, Y.; Yu, H.; Shi, S.; Xie, W.; Liu, H.; Su, Y.; Huang, J.; Lin, T. A Radiomics Nomogram for the Preoperative Prediction of Lymph Node Metastasis in Bladder CancerA Radiomics Nomogram for Bladder Cancer. Clin. Cancer Res. 2017, 23, 6904–6911. [Google Scholar] [CrossRef]
- Gao, J.; Han, F.; Jin, Y.; Wang, X.; Zhang, J. A Radiomics Nomogram for the Preoperative Prediction of Lymph Node Metastasis in Pancreatic Ductal Adenocarcinoma. Front. Oncol. 2020, 10, 1654. [Google Scholar] [CrossRef]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I.H. Textural Features for Image Classification. IEEE Trans. Syst. Man Cybern. 1973, SMC-3, 610–621. [Google Scholar] [CrossRef]
- Shen, C.; Liu, Z.; Guan, M.; Song, J.; Lian, Y.; Wang, S.; Tang, Z.; Dong, D.; Kong, L.; Wang, M. 2D and 3D CT Radiomics Features Prognostic Performance Comparison in Non-Small Cell Lung Cancer. Transl. Oncol. 2017, 10, 886–894. [Google Scholar] [CrossRef]
- Fosså, S.D.; Cvancarova, M.; Chen, L.; Allan, A.L.; Oldenburg, J.; Peterson, D.R.; Travis, L.B. Adverse Prognostic Factors for Testicular Cancer–Specific Survival: A Population-Based Study of 27,948 Patients. J. Clin. Oncol. 2011, 29, 963–970. [Google Scholar] [CrossRef]
- Parker, C.; Milosevic, M.; Panzarella, T.; Banerjee, D.; Jewett, M.; Catton, C.; Tew-George, B.; Gospodarowicz, M.; Warde, P. The Prognostic Significance of the Tumour Infiltrating Lymphocyte Count in Stage I Testicular Seminoma Managed by Surveillance. Eur. J. Cancer 2002, 38, 2014–2019. [Google Scholar] [CrossRef]
- Lerro, C.; McGlynn, K.; Cook, M. A Systematic Review and Meta-Analysis of the Relationship between Body Size and Testicular Cancer. Br. J. Cancer 2010, 103, 1467–1474. [Google Scholar] [CrossRef] [PubMed]
- Dieckmann, K.-P.; Hartmann, J.T.; Classen, J.; Diederichs, M.; Pichlmeier, U. Is Increased Body Mass Index Associated with the Incidence of Testicular Germ Cell Cancer? J. Cancer Res. Clin. Oncol. 2009, 135, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, T. Hyperparameter Optimization Using Scikit-Learn. In Hyperparameter Optimization in Machine Learning: Make Your Machine Learning and Deep Learning Models More Efficient; Apress: Berkeley, CA, USA, 2021; pp. 31–51. ISBN 978-1-4842-6579-6. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-Learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- van Rossum, G.; Drake, F.L. Python/C API Manual—Python 2.6; CreateSpace: Scotts Valley, CA, USA, 2009. [Google Scholar]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority over-Sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Kollmannsberger, C.; Tandstad, T.; Bedard, P.L.; Cohn-Cedermark, G.; Chung, P.W.; Jewett, M.A.; Powles, T.; Warde, P.R.; Daneshmand, S.; Protheroe, A. Patterns of Relapse in Patients with Clinical Stage I Testicular Cancer Managed with Active Surveillance. J. Clin. Oncol. 2015, 33, 51–57. [Google Scholar] [CrossRef]
- Fung, C.; Sesso, H.D.; Williams, A.M.; Kerns, S.L.; Monahan, P.; Zaid, M.A.; Feldman, D.R.; Hamilton, R.J.; Vaughn, D.J.; Beard, C.J. Multi-Institutional Assessment of Adverse Health Outcomes among North American Testicular Cancer Survivors after Modern Cisplatin-Based Chemotherapy. J. Clin. Oncol. 2017, 35, 1211. [Google Scholar] [CrossRef]
- Huddart, R.; Norman, A.; Shahidi, M.; Horwich, A.; Coward, D.; Nicholls, J.; Dearnaley, D. Cardiovascular Disease as a Long-Term Complication of Treatment for Testicular Cancer. J. Clin. Oncol. 2003, 21, 1513–1523. [Google Scholar] [CrossRef]
- Travis, L.B.; Ng, A.K.; Allan, J.M.; Pui, C.-H.; Kennedy, A.R.; Xu, X.G.; Purdy, J.A.; Applegate, K.; Yahalom, J.; Constine, L.S. Second Malignant Neoplasms and Cardiovascular Disease Following Radiotherapy. J. Natl. Cancer Inst. 2012, 104, 357–370. [Google Scholar] [CrossRef]
- Kerns, S.L.; Fung, C.; Monahan, P.O.; Ardeshir-Rouhani-Fard, S.; Zaid, M.I.A.; Williams, A.M.; Stump, T.E.; Sesso, H.D.; Feldman, D.R.; Hamilton, R.J. Cumulative Burden of Morbidity among Testicular Cancer Survivors after Standard Cisplatin-Based Chemotherapy: A Multi-Institutional Study. J. Clin. Oncol. 2018, 36, 1505. [Google Scholar] [CrossRef]
- Agrawal, V.; Dinh Jr, P.C.; Fung, C.; Monahan, P.O.; Althouse, S.K.; Norton, K.; Cary, C.; Einhorn, L.; Fossa, S.D.; Adra, N. Adverse Health Outcomes among US Testicular Cancer Survivors after Cisplatin-Based Chemotherapy vs Surgical Management. JNCI Cancer Spectr. 2020, 4, pkz079. [Google Scholar] [CrossRef]
- Tandstad, T.; Kollmannsberger, C.K.; Roth, B.J.; Jeldres, C.; Gillessen, S.; Fizazi, K.; Daneshmand, S.; Lowrance, W.T.; Hanna, N.H.; Albany, C. Practice Makes Perfect: The Rest of the Story in Testicular Cancer as a Model Curable Neoplasm. J. Clin. Oncol. 2017, 35, 3525. [Google Scholar] [CrossRef] [PubMed]
- Eyben, F.E. von Laboratory Markers and Germ Cell Tumors. Crit. Rev. Clin. Lab. Sci. 2003, 40, 377–427. [Google Scholar] [CrossRef] [PubMed]
- Trigo, J.M.; Tabernero, J.M.; Paz-Ares, L.; García-Llano, J.L.; Mora, J.; Lianes, P.; Esteban, E.; Salazar, R.; López-López, J.J.; Cortés-Funes, H. Tumor Markers at the Time of Recurrence in Patients with Germ Cell Tumors. Cancer 2000, 88, 162–168. [Google Scholar] [CrossRef]
- Baessler, B.; Nestler, T.; Pinto dos Santos, D.; Paffenholz, P.; Zeuch, V.; Pfister, D.; Maintz, D.; Heidenreich, A. Radiomics Allows for Detection of Benign and Malignant Histopathology in Patients with Metastatic Testicular Germ Cell Tumors Prior to Post-Chemotherapy Retroperitoneal Lymph Node Dissection. Eur. Radiol. 2020, 30, 2334–2345. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable Prognostic Models: Issues in Developing Models, Evaluating Assumptions and Adequacy, and Measuring and Reducing Errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Leão, R.; Nayan, M.; Punjani, N.; Jewett, M.A.S.; Fadaak, K.; Garisto, J.; Lewin, J.; Atenafu, E.G.; Sweet, J.; Anson-Cartwright, L.; et al. A New Model to Predict Benign Histology in Residual Retroperitoneal Masses After Chemotherapy in Nonseminoma. Eur. Urol. Focus 2018, 4, 995–1001. [Google Scholar] [CrossRef]
- Vergouwe, Y.; Steyerberg, E.W.; Foster, R.S.; Sleijfer, D.T.; Fosså, S.D.; Gerl, A.; de Wit, R.; Roberts, J.T.; Habbema, J.D.F. Predicting Retroperitoneal Histology in Postchemotherapy Testicular Germ Cell Cancer: A Model Update and Multicentre Validation with More Than 1000 Patients. Eur. Urol. 2007, 51, 424–432. [Google Scholar] [CrossRef]
- Dieckmann, K.-P.; Radtke, A.; Spiekermann, M.; Balks, T.; Matthies, C.; Becker, P.; Ruf, C.; Oing, C.; Oechsle, K.; Bokemeyer, C.; et al. Serum Levels of MicroRNA miR-371a-3p: A Sensitive and Specific New Biomarker for Germ Cell Tumours. Eur. Urol. 2017, 71, 213–220. [Google Scholar] [CrossRef]
- Bezan, A.; Gerger, A.; Pichler, M. MicroRNAs in Testicular Cancer: Implications for Pathogenesis, Diagnosis, Prognosis and Therapy. Anticancer. Res. 2014, 34, 2709–2713. [Google Scholar]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Alzamzami, F.; Hoda, M.; El Saddik, A. Light gradient boosting machine for general sentiment classification on short texts: A comparative evaluation. IEEE Access 2020, 8, 101840–101858. [Google Scholar] [CrossRef]
- Ke, G.; Meng, Q.; Finley, T.; Wang, T.; Chen, W.; Ma, W.; Ye, Q.; Liu, T.-Y. Lightgbm: A highly efficient gradient boosting decision tree. Adv. Neural Inf. Process. Syst. 2017, 30, 3149–3157. [Google Scholar]
- Cervantes, J.; Garcia-Lamont, F.; Rodríguez-Mazahua, L.; Lopez, A. A comprehensive survey on support vector machine classification: Applications, challenges and trends. Neurocomputing 2020, 408, 189–215. [Google Scholar] [CrossRef]
- Pisner, D.A.; Schnyer, D.M. Support vector machine. In Machine Learning; Elsevier: Amsterdam, The Netherlands, 2020; pp. 101–121. [Google Scholar]
- Laaksonen, J.; Oja, E. Classification with learning k-nearest neighbors. In Proceedings of the International Conference on Neural Networks (ICNN’96), Washington, DC, USA, 3–6 June 1996; pp. 1480–1483. [Google Scholar]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lisson, C.S.; Manoj, S.; Wolf, D.; Lisson, C.G.; Schmidt, S.A.; Beer, M.; Thaiss, W.; Bolenz, C.; Zengerling, F.; Goetz, M. Radiomics and Clinicopathological Characteristics for Predicting Lymph Node Metastasis in Testicular Cancer. Cancers 2023, 15, 5630. https://doi.org/10.3390/cancers15235630
Lisson CS, Manoj S, Wolf D, Lisson CG, Schmidt SA, Beer M, Thaiss W, Bolenz C, Zengerling F, Goetz M. Radiomics and Clinicopathological Characteristics for Predicting Lymph Node Metastasis in Testicular Cancer. Cancers. 2023; 15(23):5630. https://doi.org/10.3390/cancers15235630
Chicago/Turabian StyleLisson, Catharina Silvia, Sabitha Manoj, Daniel Wolf, Christoph Gerhard Lisson, Stefan A. Schmidt, Meinrad Beer, Wolfgang Thaiss, Christian Bolenz, Friedemann Zengerling, and Michael Goetz. 2023. "Radiomics and Clinicopathological Characteristics for Predicting Lymph Node Metastasis in Testicular Cancer" Cancers 15, no. 23: 5630. https://doi.org/10.3390/cancers15235630