

Investigating the Role of Tumor-Infiltrating Lymphocytes as Predictors of Lymph Node Metastasis in Deep Submucosal Invasive Colorectal Cancer: A Retrospective Cross-Sectional Study
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Histological Evaluation
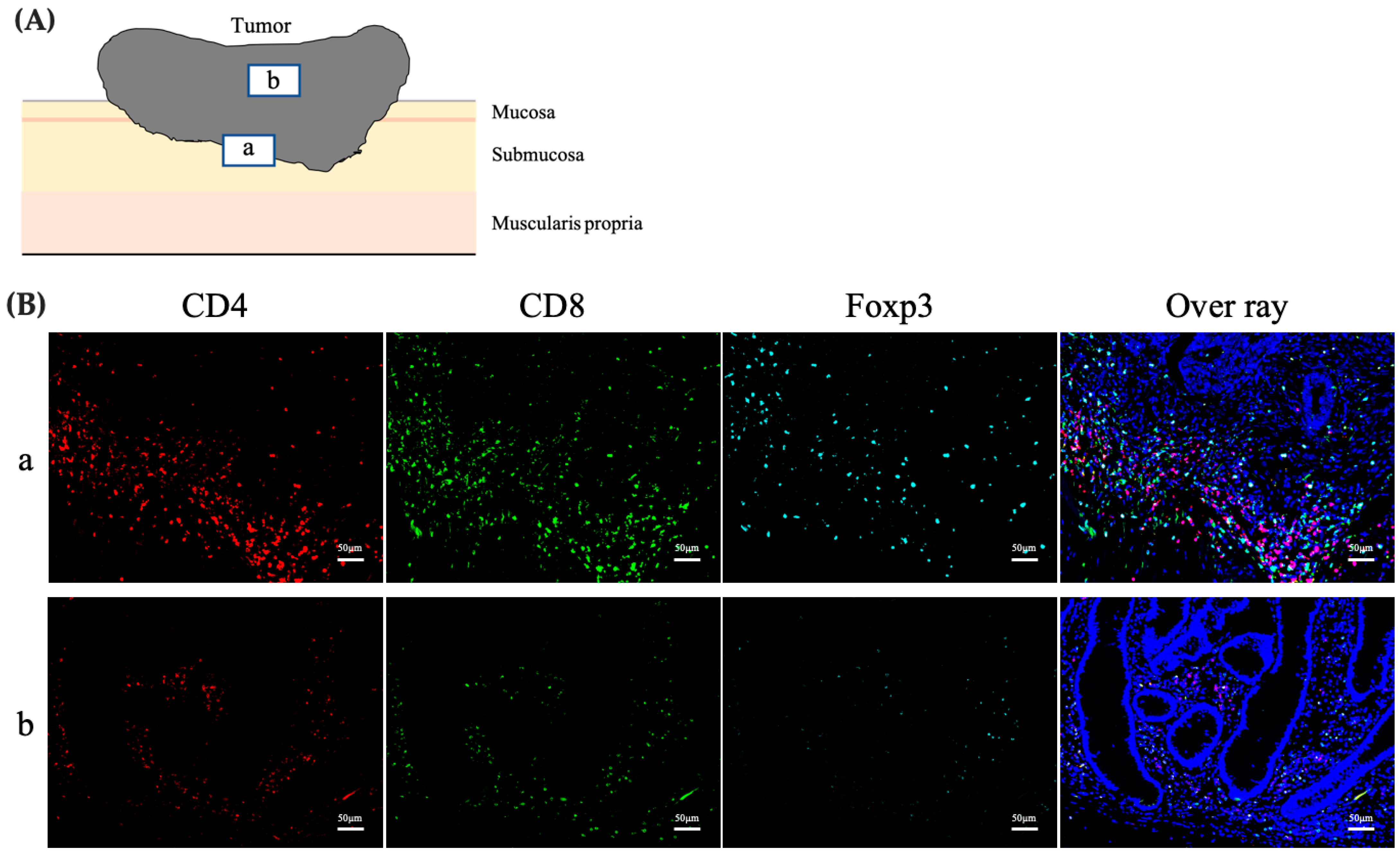
2.3. Assessment of the Phenotype, Number, and Distribution of TILs
2.4. Immunofluorescence Staining
2.5. Statistical Analyses
3. Results
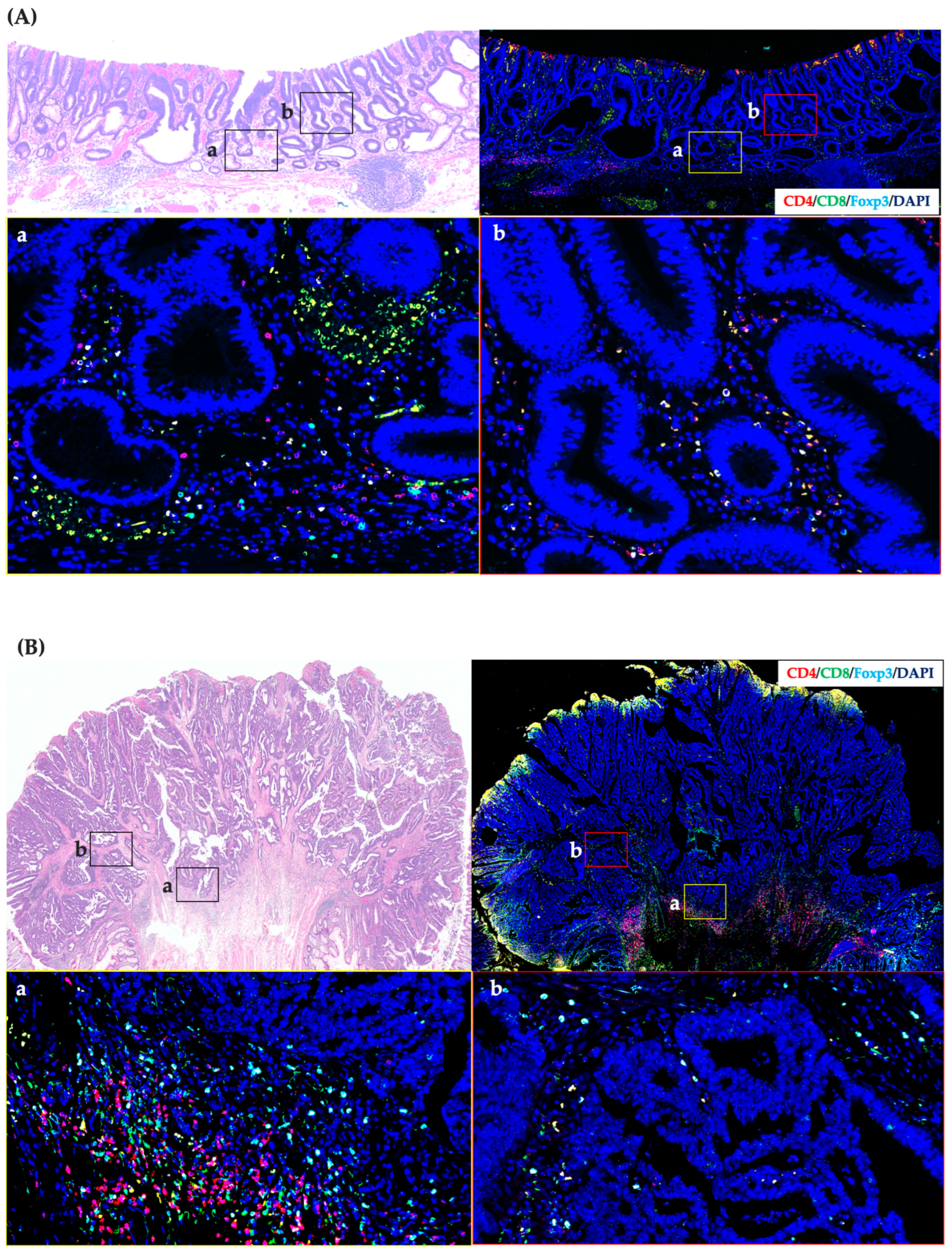
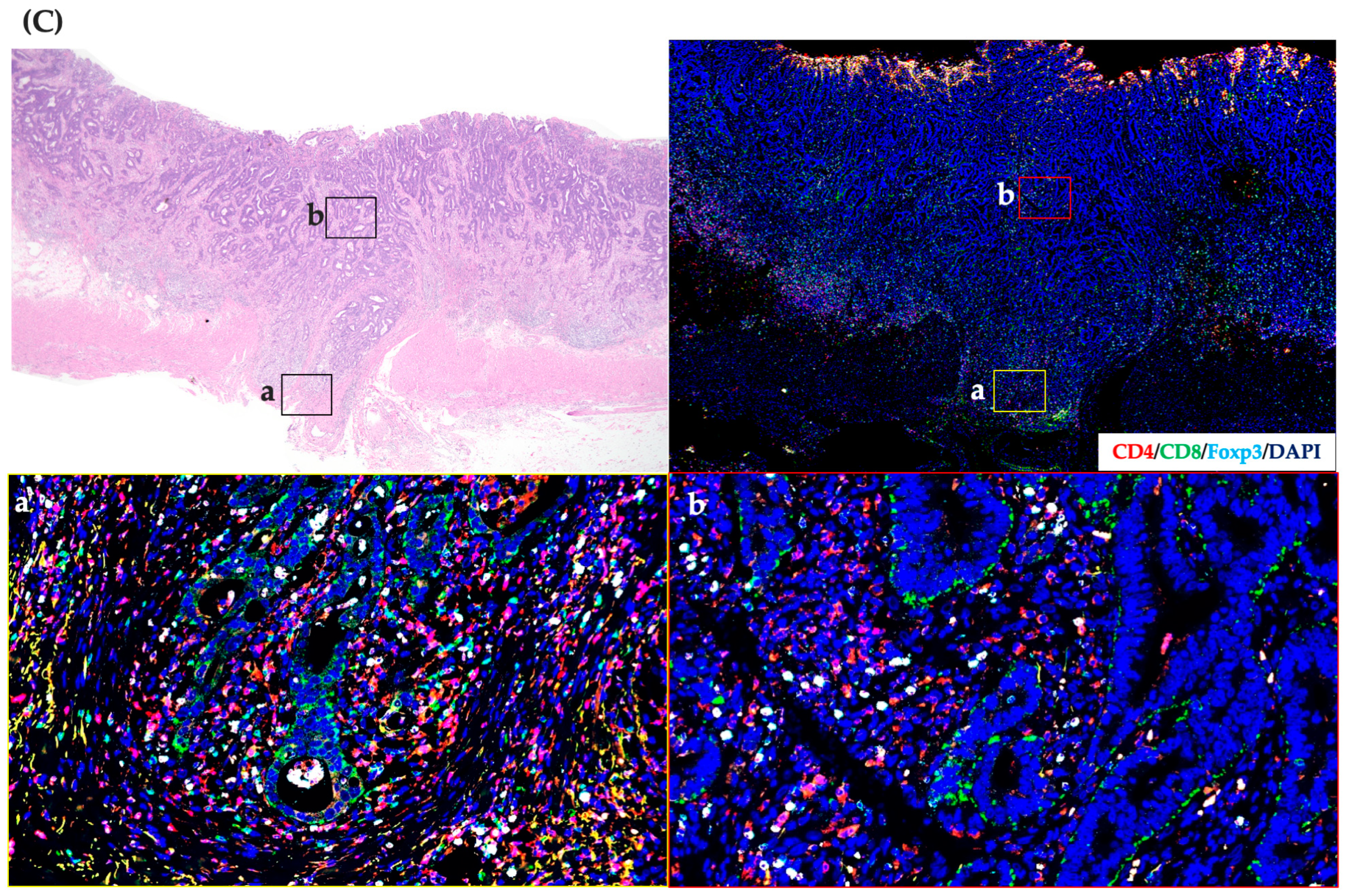
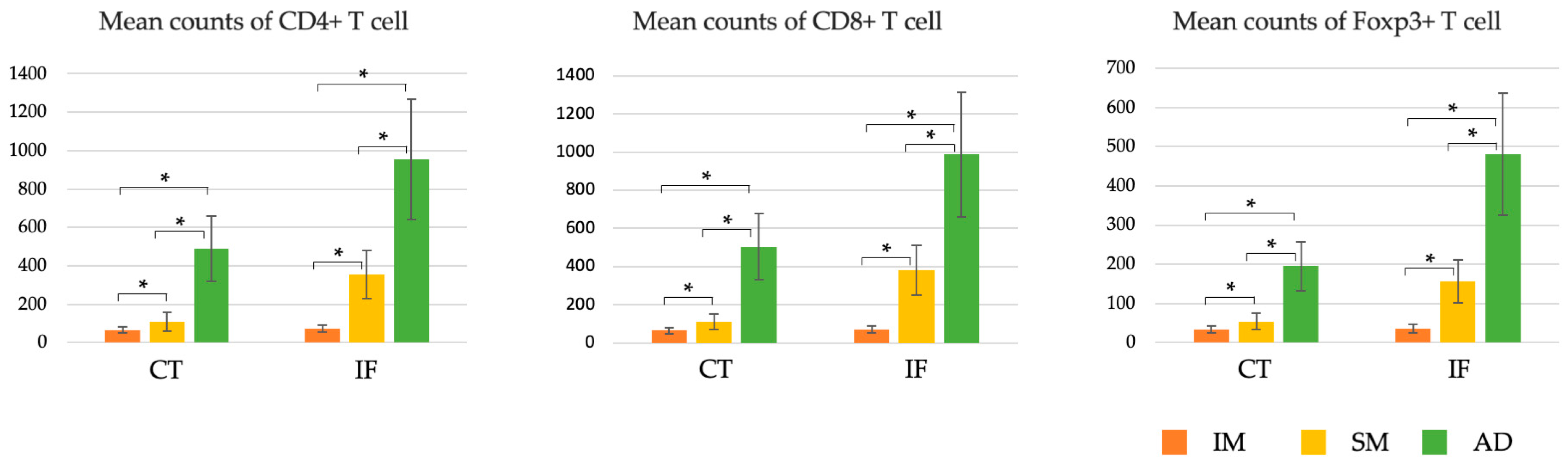
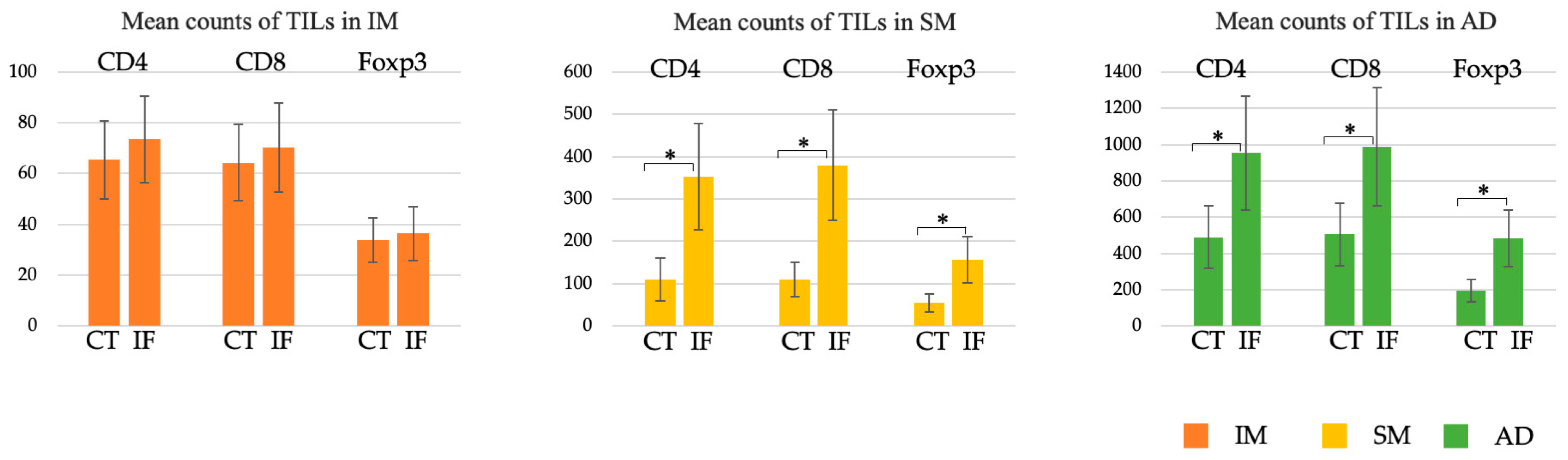
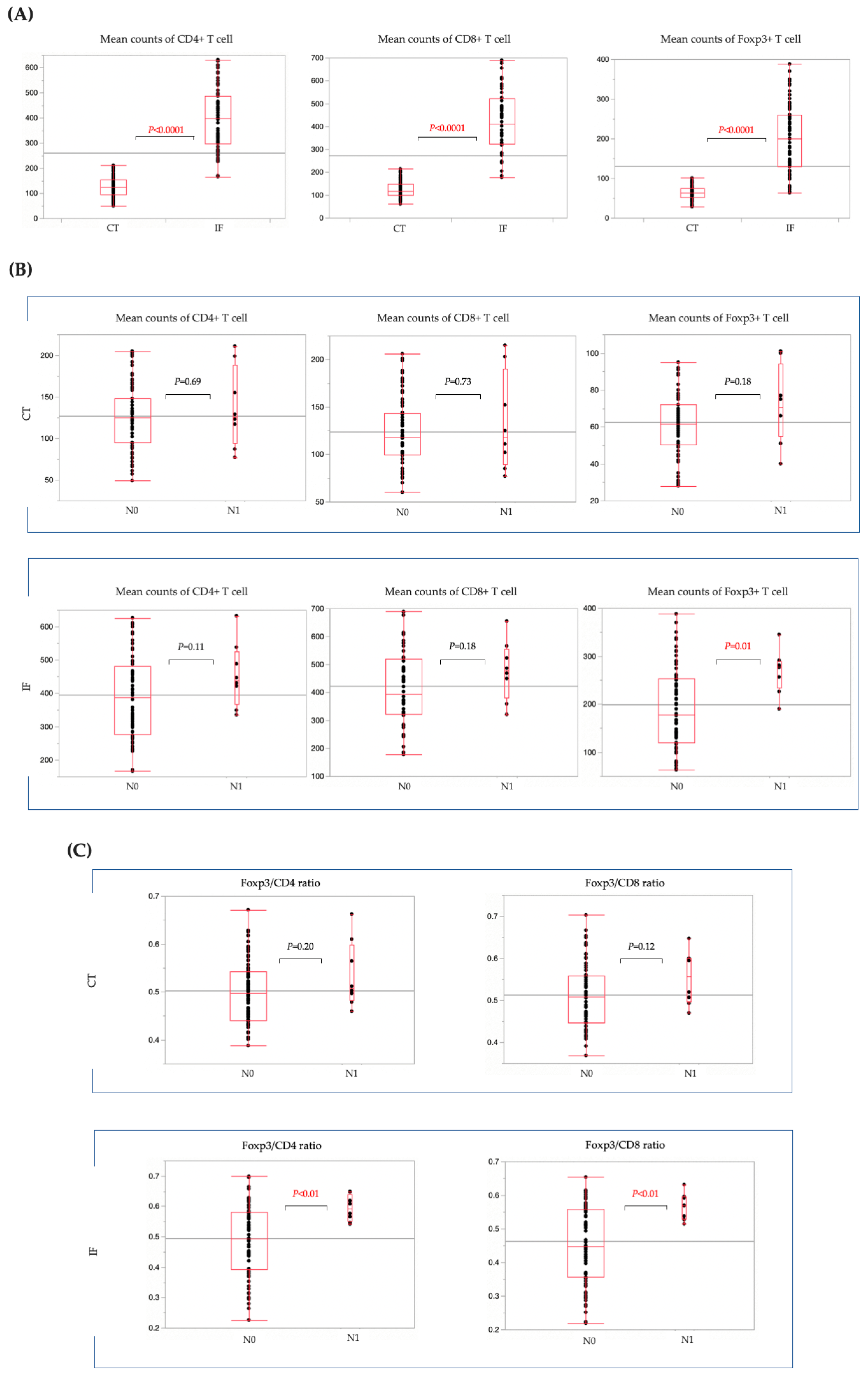
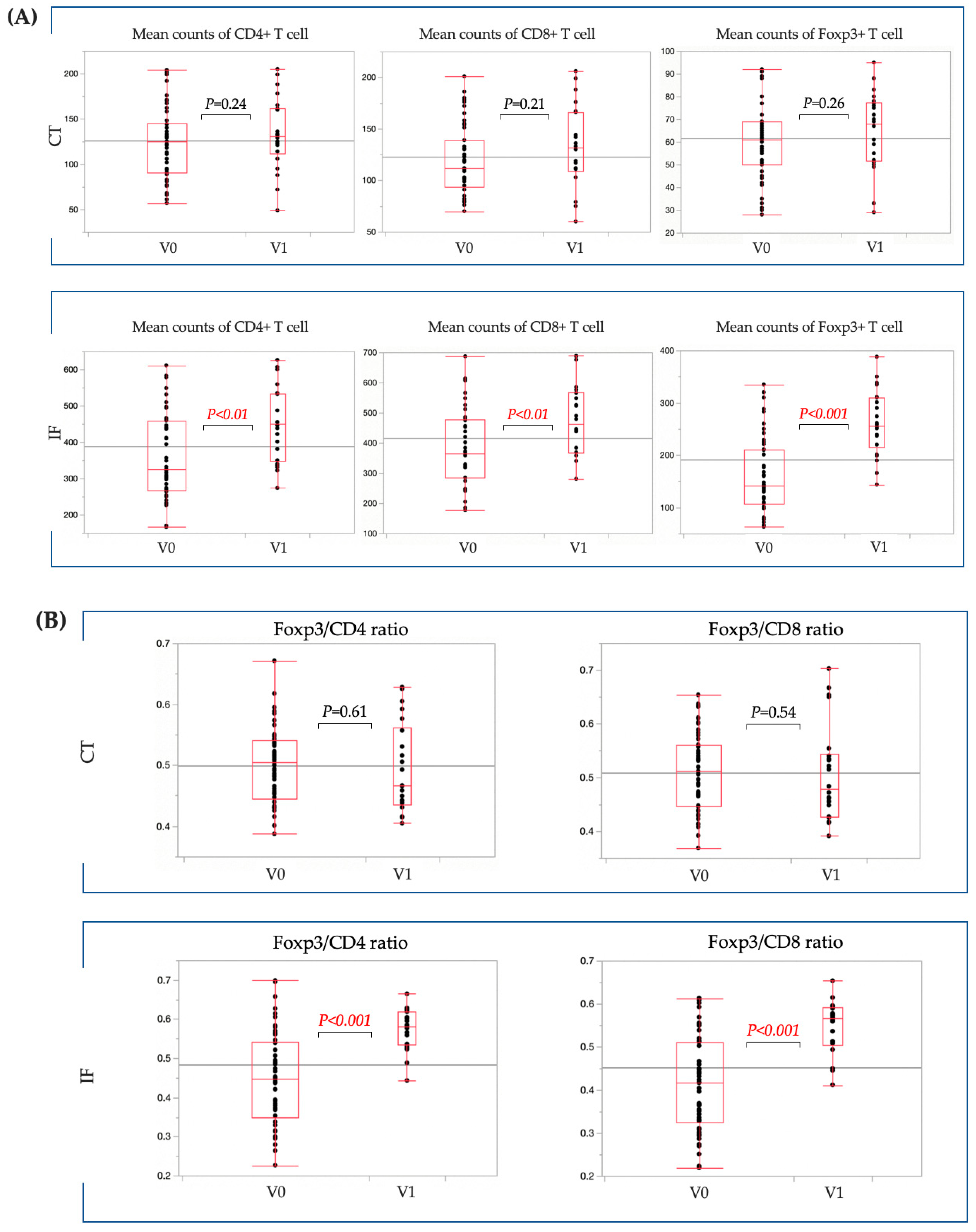
3.1. Changes in the Number, Phenotype, and Distribution of TILs during CRC Progression
3.2. Clinicopathological Characteristics of Patients with T1b CRC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F.; Mantovani, A. Inflammation and Cancer: Back to Virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Weigelin, B.; Krause, M.; Friedl, P. Cytotoxic T Lymphocyte Migration and Effector Function in the Tumor Microenvironment. Immunol. Lett. 2011, 138, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, F.; Takada, K.; Yamada, Y.; Oku, Y.; Kosai, K.; Ono, Y.; Tanaka, K.; Wakasu, S.; Oba, T.; Osoegawa, A.; et al. Combined Evaluation of Tumor-Infiltrating CD8 + and FoxP3 + Lymphocytes Provides Accurate Prognosis in Stage IA Lung Adenocarcinoma. Ann. Surg. Oncol. 2020, 27, 2102–2109. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, K.; Miyamoto, M.; Cho, Y.; Suzuoki, M.; Oshikiri, T.; Nakakubo, Y.; Itoh, T.; Ohbuchi, T.; Kondo, S.; Katoh, H. Concurrent Infiltration by CD8+ T Cells and CD4+ T Cells Is a Favourable Prognostic Factor in Non-Small-Cell Lung Carcinoma. Br. J. Cancer 2006, 94, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Kawai, O.; Ishii, G.; Kubota, K.; Murata, Y.; Naito, Y.; Mizuno, T.; Aokage, K.; Saijo, N.; Nishiwaki, Y.; Gemma, A.; et al. Predominant Infiltration of Macrophages and CD8(+) T Cells in Cancer Nests Is a Significant Predictor of Survival in Stage IV Nonsmall Cell Lung Cancer. Cancer 2008, 113, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, M.; Sasano, H.; Tamaki, K.; Hirakawa, H.; Takahashi, Y.; Nakagawa, S.; Watanabe, G.; Tada, H.; Suzuki, A.; Ohuchi, N.; et al. Prognostic Significance of Tumor-Infiltrating CD8+ and Foxp3+ Lymphocytes in Residual Tumors and Alterations in These Parameters After Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer: A Retrospective Multicenter Study. Breast Cancer Res. 2015, 17, 124. [Google Scholar] [CrossRef]
- Al-Mterin, M.A.; Murshed, K.; Alsalman, A.; Abu-Dayeh, A.; Elkord, E. Associations of Different Immune Checkpoints-Expressing CD4+ Treg/ T Cell Subsets with Disease Free Survival in Colorectal Cancer Patients. BMC Cancer 2022, 22, 601. [Google Scholar] [CrossRef]
- Huang, A.; Xiao, Y.; Peng, C.; Liu, T.; Lin, Z.; Yang, Q.; Zhang, T.; Liu, J.; Ma, H. 53BP1 Expression and Immunoscore Are Associated with the Efficacy of Neoadjuvant Chemoradiotherapy for Rectal Cancer. Strahlenther. Onkol. 2020, 196, 465–473. [Google Scholar] [CrossRef]
- Idos, G.E.; Kwok, J.; Bonthala, N.; Kysh, L.; Gruber, S.B.; Qu, C. The Prognostic Implications of Tumor Infiltrating Lymphocytes in Colorectal Cancer: A Systematic Review and Meta-analysis. Sci. Rep. 2020, 10, 3360. [Google Scholar] [CrossRef]
- Hashiguchi, Y.; Muro, K.; Saito, Y.; Ito, Y.; Ajioka, Y.; Hamaguchi, T.; Hasegawa, K.; Hotta, K.; Ishida, H.; Ishiguro, M.; et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) Guidelines 2019 for the Treatment of Colorectal Cancer. Int. J. Clin. Oncol. 2020, 25, 1–42. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, K.; Fujimori, T.; Fujii, S.; Takeda, J.; Ohkura, Y.; Kawamata, H.; Kumamoto, T.; Ishiguro, S.; Kato, Y.; Shimoda, T.; et al. Correlations Between Lymph Node Metastasis and Depth of Submucosal Invasion in Submucosal Invasive Colorectal Carcinoma: A Japanese Collaborative Study. J. Gastroenterol. 2004, 39, 534–543. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Haruma, K.; Oh-E, H.; Nagata, S.; Hirota, Y.; Furudoi, A.; Amioka, T.; Kitadai, Y.; Yoshihara, M.; Shimamoto, F. Conditions of Curability After Endoscopic Resection for Colorectal Carcinoma with Submucosally Massive Invasion. Oncol. Rep. 2000, 7, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.; Mochizuki, H.; Hashiguchi, Y.; Shimazaki, H.; Aida, S.; Hase, K.; Matsukuma, S.; Kanai, T.; Kurihara, H.; Ozawa, K.; et al. Risk Factors for an Adverse Outcome in Early Invasive Colorectal Carcinoma. Gastroenterology 2004, 127, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Nakadoi, K.; Tanaka, S.; Kanao, H.; Terasaki, M.; Takata, S.; Oka, S.; Yoshida, S.; Arihiro, K.; Chayama, K. Management of T1 Colorectal Carcinoma with Special Reference to Criteria for Curative Endoscopic Resection. J. Gastroenterol. Hepatol. 2012, 27, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumors of Digestive System, 5th ed.; World Health Organization: Geneva, Switzerland, 2019; Volume 1, pp. 157–188.
- Tanaka, S.; Haruma, K.; Teixeira, C.R.; Tatsuta, S.; Ohtsu, N.; Hiraga, Y.; Yoshihara, M.; Sumii, K.; Kajiyama, G.; Shimamoto, F. Endoscopic treatment of submucosal invasive colorectal carcinoma with special reference to risk factors for lymph node metastasis. J. Gastroenterol. 1995, 30, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Schnellhardt, S.; Hirneth, J.; Büttner-Herold, M.; Daniel, C.; Haderlein, M.; Hartmann, A.; Fietkau, R.; Distel, L. The Prognostic Value of FoxP3+ Tumour-Infiltrating Lymphocytes in Rectal Cancer Depends on Immune Phenotypes Defined by CD8+ Cytotoxic T Cell Density. Front. Immunol. 2022, 13, 781222. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Ma, J.; Yu, G.; Qiu, Q.; Zhang, W.; Cao, F. Effective Predictor of Colorectal Cancer Survival Based on Exclusive Expression Pattern Among Different Immune Cell Infiltration. J. Histochem. Cytochem. 2021, 69, 271–286. [Google Scholar] [CrossRef]
- Shi, W.; Zhang, F.; Chen, X.; Wang, S.; Zhang, H.; Yang, Z.; Wang, G.; Zheng, Y.; Han, Y.; Sun, Y.; et al. Tumor-Derived Immunoglobulin Like Transcript 5 Induces Suppressive Immunocyte Infiltration in Colorectal Cancer. Cancer Sci. 2022, 113, 1939–1954. [Google Scholar] [CrossRef]
- Sheu, B.C.; Chang, W.C.; Cheng, C.Y.; Lin, H.H.; Chang, D.Y.; Huang, S.C. Cytokine Regulation Networks in the Cancer Microenvironment. Front. Biosci. 2008, 13, 6255–6268. [Google Scholar] [CrossRef]
- Correale, P.; Rotundo, M.S.; Del Vecchio, M.T.; Remondo, C.; Migali, C.; Ginanneschi, C.; Tsang, K.Y.; Licchetta, A.; Mannucci, S.; Loiacono, L.; et al. Regulatory (Foxp3+) T-Cell Tumor Infiltration Is a Favorable Prognostic Factor in Advanced Colon Cancer Patients Undergoing Chemo or Chemoimmunotherapy. J. Immunother. 2010, 33, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Ling, A.; Edin, S.; Wikberg, M.L.; Öberg, Å.; Palmqvist, R. The Intratumoural Subsite and Relation of CD8(+) and Foxp3(+) T Lymphocytes in Colorectal Cancer Provide Important Prognostic Clues. Br. J. Cancer 2014, 110, 2551–2559. [Google Scholar] [CrossRef]
- Chen, Y.; Yuan, R.; Wu, X.; He, X.; Zeng, Y.; Fan, X.; Wang, L.; Wang, J.; Lan, P.; Wu, X. A Novel Immune Marker Model Predicts Oncological Outcomes of Patients with Colorectal Cancer. Ann. Surg. Oncol. 2016, 23, 826–832. [Google Scholar] [CrossRef] [PubMed]
- Richards, C.H.; Roxburgh, C.S.; Powell, A.G.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. The Clinical Utility of the Local Inflammatory Response in Colorectal Cancer. Eur. J. Cancer 2014, 50, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, K.; Kunisho, S.; Takigawa, H.; Yuge, R.; Oka, S.; Tanaka, S.; Shimamoto, F.; Chayama, K.; Kitadai, Y. Role of Tumor-Associated Macrophages at the Invasive Front in Human Colorectal Cancer Progression. Cancer Sci. 2021, 112, 2692–2704. [Google Scholar] [CrossRef]
- Shinto, E.; Hase, K.; Hashiguchi, Y.; Sekizawa, A.; Ueno, H.; Shikina, A.; Kajiwara, Y.; Kobayashi, H.; Ishiguro, M.; Yamamoto, J. CD8+ and FOXP3+ Tumor-Infiltrating T Cells Before and After Chemoradiotherapy for Rectal Cancer. Ann. Surg. Oncol. 2014, 21, S414–S421. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Grimmig, T.; Grimm, M.; Lazariotou, M.; Meier, E.; Rosenwald, A.; Tsaur, I.; Blaheta, R.; Heemann, U.; Germer, C.T.; et al. Expression of Foxp3 in Colorectal Cancer but Not in Treg Cells Correlates with Disease Progression in Patients with Colorectal Cancer. PLoS ONE 2013, 8, e53630. [Google Scholar] [CrossRef]
- Fu, J.; Xu, D.; Liu, Z.; Shi, M.; Zhao, P.; Fu, B.; Zhang, Z.; Yang, H.; Zhang, H.; Zhou, C.; et al. Increased Regulatory T Cells Correlate with CD8 T-Cell Impairment and Poor Survival in Hepatocellular Carcinoma Patients. Gastroenterology 2007, 132, 2328–2339. [Google Scholar] [CrossRef]
- Olguín, J.E.; Medina-Andrade, I.; Rodríguez, T.; Rodríguez-Sosa, M.; Terrazas, L.I. Relevance of Regulatory T Cells During Colorectal Cancer Development. Cancers 2020, 12, 1888. [Google Scholar] [CrossRef]
- Solinas, G.; Germano, G.; Mantovani, A.; Allavena, P. Tumor-Associated Macrophages (TAM) as Major Players of the Cancer-Related Inflammation. J. Leukoc. Biol. 2009, 86, 1065–1073. [Google Scholar] [CrossRef]
- Pollard, J.W. Macrophages Define the Invasive Microenvironment in Breast Cancer. J. Leukoc. Biol. 2008, 84, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Guan, Y.; Yu, S.; Zhao, Z.; Ciric, B.; Zhang, G.X.; Rostami, A. Antigen Presenting Cells Treated In Vitro by Macrophage Colony-Stimulating Factor and Autoantigen Protect Mice from Autoimmunity. J. Neuroimmunol. 2007, 192, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Cho, E.Y.; Park, Y.H.; Ahn, J.S.; Im, Y.H. Prognostic Impact of Foxp3 Expression in Triple-Negative Breast Cancer. Acta Oncol. 2013, 52, 73–81. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | IM | SM * | AD |
|---|---|---|---|
| (n = 20) | (n = 20) | (n = 20) | |
| Age, mean ± SD, years | 65 ± 10.2 | 67 ± 11.3 | 66 ± 8.8 |
| Sex | |||
| Male | 13 (65) | 12 (59) | 13 (65) |
| Female | 7 (35) | 8 (40) | 7 (35) |
| Tumor size, mean ± SD, mm | 14.7 ± 4.3 | 16.4 ± 5.2 | 28.8 ± 12.5 |
| Localization | |||
| Right colon | 7 (35) | 8 (40) | 7 (35) |
| Left colon | 6 (30) | 6 (30) | 8 (40) |
| Rectum | 7 (35) | 6 (30) | 5 (25) |
| Morphology | |||
| Protruded | 12 (60) | 7 (35) | 20 (100) |
| Superficial/Depressed | 8 (40) | 33 | 0 (0) |
| Dominant histological type | |||
| tub/pap | 20 (100) | 20 (100) | 16 (80) |
| por/sig/muc | 0 (0) | 0 (0) | 4 (20) |
| Venous invasion positive | 0 (0) | 2 (10) | 12 (60) |
| Lymphatic invasion positive | 0 (0) | 3 (15) | 15 (75) |
| LN metastasis positive | 0 (0) | 1 (5) | 9 (45) |
| Distant metastasis positive | 0 (0) | 0 (0) | 2 (10) |
| Recurrence | 0 (0) | 0 (0) | 2 (10) |
| (%) |
| Characteristics | LN Metastasis | ||
|---|---|---|---|
| (+), n = 8 | (−), n = 76 | p-Value | |
| Age, mean ± SD, years | 68 ± 10.5 | 67 ± 10.2 | 0.79 |
| Sex | 0.62 | ||
| Male | 4 (50) | 45 (59) | |
| Female | 4 (50) | 31 (41) | |
| Tumor size, mean ± SD, mm | 26 ± 16.6 | 24 ± 10.4 | 0.96 |
| Localization | 0.81 | ||
| Right colon | 2 (25) | 27 (36) | |
| Left colon | 4 (50) | 35 (46) | |
| Rectum | 2 (25) | 14 (18) | |
| Morphology | 0.022 | ||
| Protruded | 3 (38) | 59 (78) | |
| Superficial | 5 (62) | 17 (22) | |
| Treatment | 0.34 | ||
| Surgery alone | 5 (63) | 34 (45) | |
| Surgery after endoscopic resection | 3 (37) | 42 (55) | |
| Dominant histological type | 1 | ||
| tub/pap | 8 (100) | 76 (100) | |
| por/sig/muc | 0 (0) | 0 (0) | |
| SM invasion depth, mean ± SD, μm | 3687 ± 1614 | 3745 ± 2166 | 0.73 |
| Venous invasion positive | 5 (63) | 22 (29) | 0.063 |
| Lymphatic invasion positive | 7 (88) | 27 (36) | 0.0036 |
| Budding grade 2/3 | 6 (75) | 35(46) | 0.11 |
| Distant metastasis positive | 0 (0) | 0 (0) | 1 |
| Recurrence | 0 (0) | 0 (0) | 1 |
| (%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamari, H.; Kitadai, Y.; Takigawa, H.; Yuge, R.; Urabe, Y.; Shimamoto, F.; Oka, S. Investigating the Role of Tumor-Infiltrating Lymphocytes as Predictors of Lymph Node Metastasis in Deep Submucosal Invasive Colorectal Cancer: A Retrospective Cross-Sectional Study. Cancers 2023, 15, 5238. https://doi.org/10.3390/cancers15215238
Tamari H, Kitadai Y, Takigawa H, Yuge R, Urabe Y, Shimamoto F, Oka S. Investigating the Role of Tumor-Infiltrating Lymphocytes as Predictors of Lymph Node Metastasis in Deep Submucosal Invasive Colorectal Cancer: A Retrospective Cross-Sectional Study. Cancers. 2023; 15(21):5238. https://doi.org/10.3390/cancers15215238
Chicago/Turabian StyleTamari, Hirosato, Yasuhiko Kitadai, Hidehiko Takigawa, Ryo Yuge, Yuji Urabe, Fumio Shimamoto, and Shiro Oka. 2023. "Investigating the Role of Tumor-Infiltrating Lymphocytes as Predictors of Lymph Node Metastasis in Deep Submucosal Invasive Colorectal Cancer: A Retrospective Cross-Sectional Study" Cancers 15, no. 21: 5238. https://doi.org/10.3390/cancers15215238