
Clinical Characteristics and Postoperative Complications in Patients Undergoing Colorectal Cancer Surgery with Perioperative COVID-19 Infection

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
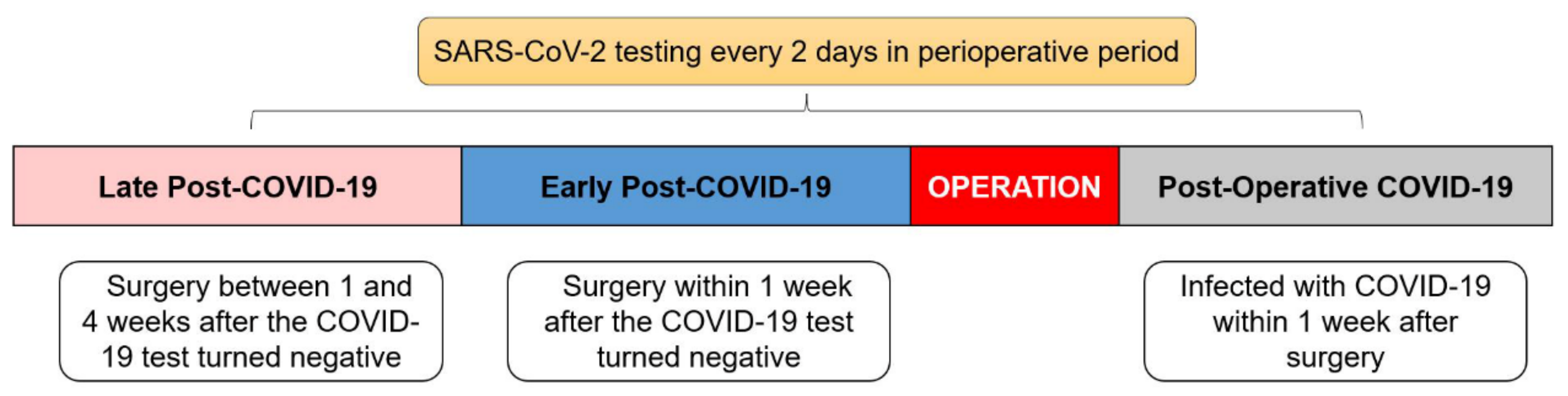
2.1. Study Population
2.2. Outcomes
2.3. Data Collection
- CCI = 0: none.
- 0 < CCI ≤ 20.9: mild.
- CCI > 20.9: severe.
2.4. Statistical Analysis
3. Result
3.1. Baseline Characteristics
3.2. Postoperative Complications and Laboratory Findings
3.3. Different Periods of COVID-19 Infection on Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deng, J.Z.; Chan, J.S.; Potter, A.L.; Chen, Y.-W.; Sandhu, H.S.M.; Panda, N.; Chang, D.C.; Yang, C.-F.J. The risk of postoperative complications after major elective surgery in active or resolved COVID-19 in the United States. Ann. Surg. 2022, 275, 242. [Google Scholar] [CrossRef] [PubMed]
- Nahshon, C.; Bitterman, A.; Haddad, R.; Hazzan, D.; Lavie, O. Hazardous postoperative outcomes of unexpected COVID-19 infected patients: A call for global consideration of sampling all asymptomatic patients before surgical treatment. World J. Surg. 2020, 44, 2477–2481. [Google Scholar] [CrossRef] [PubMed]
- COVIDSurg Collaborative. Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: An international cohort study. Lancet 2020, 396, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Knisely, A.; Zhou, Z.N.; Wu, J.; Huang, Y.; Holcomb, K.; Melamed, A.; Advincula, A.P.; Lalwani, A.; Khoury-Collado, F.; Tergas, A.I.; et al. Perioperative morbidity and mortality of patients with COVID-19 who undergo urgent and emergent surgical procedures. Ann. Surg. 2021, 273, 34. [Google Scholar] [CrossRef] [PubMed]
- Singhal, R.; Ludwig, C.; Rudge, G.; Gkoutos, G.V.; Tahrani, A.; Mahawar, K.; Pędziwiatr, M.; Major, P.; Zarzycki, P.; Pantelis, A.; et al. 30-day morbidity and mortality of bariatric surgery during the COVID-19 pandemic: A multinational cohort study of 7704 patients from 42 countries. Obes. Surg. 2021, 31, 4272–4288. [Google Scholar] [CrossRef] [PubMed]
- Lei, S.; Jiang, F.; Su, W.; Chen, C.; Chen, J.; Mei, W.; Zhan, L.-Y.; Jia, Y.; Zhang, L.; Liu, D.; et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. eClinicalMedicine 2020, 21, 100331. [Google Scholar] [CrossRef]
- Doglietto, F.; Vezzoli, M.; Gheza, F.; Lussardi, G.L.; Domenicucci, M.; Vecchiarelli, L.; Zanin, L.; Saraceno, G.; Signorini, L.; Panciani, P.P.; et al. Factors associated with surgical mortality and complications among patients with and without coronavirus disease 2019 (COVID-19) in Italy. JAMA Surg. 2020, 155, 691–702. [Google Scholar] [CrossRef]
- Dursun, P.; Dervisoglu, H.; Daggez, M.; Turan, T.; Kiliç, F.; Tekin, M.; Üreyen, I.; Toptaş, T.; Demirayak, G.; Önder, A.B.; et al. Performing gynecologic cancer surgery during the COVID-19 pandemic in Turkey: A multicenter retrospective observational study. Int. J. Gynecol. Obstet. 2020, 151, 33–38. [Google Scholar] [CrossRef]
- Liu, F.; Wang, S.; Meng, G. Primary assessment of the diversity of Omicron sublineages and the epidemiologic features of autumn/winter 2022 COVID-19 wave in Chinese mainland. Front. Med. 2022, 1–10. [Google Scholar] [CrossRef]
- Pan, Y.; Wang, L.; Feng, Z.; Xu, H.; Li, F.; Shen, Y.; Zhang, D.; Liu, W.J.; Gao, G.F.; Wang, Q. Characterisation of SARS-CoV-2 variants in Beijing during 2022: An epidemiological and phylogenetic analysis. Lancet 2023, 401, 664–672. [Google Scholar] [CrossRef]
- Deana, C.; Rovida, S.; Orso, D.; Bove, T.; Bassi, F.; De Monte, A.; Vetrugno, L. Learning from the Italian experience during COVID-19 pandemic waves: Be prepared and mind some crucial aspects. Acta Bio Med. Atenei Parm. 2021, 92, e2021097. [Google Scholar]
- Canet, J.; Gallart, L.; Gomar, C.; Paluzie, G.; Vallès, J.; Castillo, J.; Sabaté, S.; Mazo, V.; Briones, Z.; Sanchis, J.; et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. J. Am. Soc. Anesthesiol. 2010, 113, 1338–1350. [Google Scholar] [CrossRef] [PubMed]
- Canet, J.; Sabate, S.; Mazo, V.; Gallart, L.; De Abreu, M.G.; Belda, J.; Langeron, O.; Hoeft, A.; Pelosi, P. Development and validation of a score to predict postoperative respiratory failure in a multicentre European cohort: A prospective, observational study. Eur. J. Anaesthesiol. 2015, 32, 458–470. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; Oliveira, M.L.D.; Vauthey, J.N.; Makuuchi, M. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187. [Google Scholar] [CrossRef] [PubMed]
- Slankamenac, K.; Nederlof, N.; Pessaux, P.; Jonge, J.D.; Clavien, P.A. The comprehensive complication index: A novel and more sensitive endpoint for assessing outcome and reducing sample size in randomized controlled trials. Ann. Surg. 2014, 260, 762–763. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative GC. SARS-CoV-2 vaccination modelling for safe surgery to save lives: Data from an international prospective cohort study. Br. J. Surg. 2021, 108, 1056–1063. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, H.; Zhang, W. SARS-CoV-2 variants, immune escape, and countermeasures. Front. Med. 2022, 16, 196–207. [Google Scholar] [CrossRef]
- Jalali, N.; Brustad, H.K.; Frigessi, A.; MacDonald, E.A.; Meijerink, H.; Feruglio, S.L.; Nygård, K.M.; Rø, G.; Madslien, E.H.; De Blasio, B.F. Increased household transmission and immune escape of the SARS-CoV-2 Omicron compared to Delta variants. Nat. Commun. 2022, 13, 5706. [Google Scholar] [CrossRef]
- Bálint, G.; Vörös-Horváth, B.; Széchenyi, A. Omicron: Increased transmissibility and decreased pathogenicity. Signal Transduct. Target. Ther. 2022, 7, 151. [Google Scholar] [CrossRef]
- Ross, G.L. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. What are the implications for the commencement of elective surgery? eClinicalMedicine 2020, 23, 100385. [Google Scholar] [CrossRef] [PubMed]
- Bui, N.; Coetzer, M.; Schenning, K.J.; O’Glasser, A.Y. Preparing previously COVID-19-positive patients for elective surgery: A framework for preoperative evaluation. Perioper. Med. 2021, 10, 1. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Perioperative COVID-19 Infection, No. (%) | ||||
|---|---|---|---|---|
| Variable | No (n = 154) | Yes (n = 57) | Total (n = 211) | Pa |
| Age, mean (SD), y | 65.96 (10.86) | 64.81 (12.54) | 65.65 (11.32) | 0.512 b |
| Sex | ||||
| Male | 93 (60.4) | 34 (59.6) | 127 (60.2) | 0.922 c |
| Female | 61 (39.6) | 23 (40.4) | 84 (39.8) | |
| BMI, mean (SD) | 22.07 (3.38) | 22.74 (3.28) | 22.25 (3.36) | 0.202 b |
| ASA Class | 0.456 c | |||
| I | 65 (42.2) | 18 (31.6) | 83 (39.3) | |
| II | 45 (29.2) | 22 (38.6) | 67 (31.8) | |
| III | 34 (22.1) | 12 (21.1) | 46 (21.8) | |
| IV | 10 (6.5) | 5 (8.8) | 15 (7.1) | |
| Current smoker within 1 y | 21 (13.6) | 7 (12.3) | 28 (13.3) | 0.826 c |
| Preoperative Comorbidities | ||||
| Diabetes | 21 (13.6) | 9 (15.8) | 30 (14.2) | 0.825 c |
| Hypertension | 63 (40.9) | 24 (42.1) | 87 (41.2) | 0.875 c |
| Cerebrovascular disease | 12 (7.8) | 2 (3.5) | 14 (6.6) | 0.361 d |
| Cardiovascular disease | 13 (8.4) | 5 (8.8) | 18 (8.5) | 1.000 d |
| COPD | 31 (20.1) | 16 (28.1) | 47 (22.3) | 0.264 c |
| Pulmonary insufficiency | 96 (62.3) | 33 (57.9) | 129 (61.1) | 0.634 c |
| Primary Tumor Site | 0.457c | |||
| Cecum and ascending colon | 29 (18.8) | 12 (21.1) | 41 (19.4) | |
| Transverse colon | 4 (2.6) | 4 (7) | 8 (3.8) | |
| Descending colon | 14 (9.1) | 3 (5.3) | 17 (8.1) | |
| Sigmoid colon | 19 (12.3) | 9 (15.8) | 28 (13.3) | |
| Rectum | 88 (57.1) | 29 (50.9) | 117 (55.5) | |
| Operation | 0.166 c | |||
| Open surgery | 11 (7.1) | 9 (15.8) | 20 (9.5) | |
| Laparoscopic surgery | 126 (81.8) | 43 (75.4) | 169 (80.1) | |
| Robotic surgery | 17 (11) | 5 (8.8) | 22 (10.4) | |
| Pathology | 0.161 d | |||
| Adenocarcinoma | 114 (74) | 49 (86) | 163 (77.3) | |
| Mucinous carcinoma | 37 (24) | 8 (14) | 45 (21.3) | |
| Other | 3 (1.9) | 0 (0) | 3 (1.4) | |
| TNM staging | 0.831 c | |||
| I | 38 (24.7) | 15 (26.3) | 53 (25.1) | |
| II | 49 (31.8) | 21 (36.8) | 70 (33.2) | |
| III | 49 (31.8) | 16 (28.1) | 65 (30.8) | |
| IV | 18 (11.7) | 5 (8.8) | 23 (10.9) | |
| Perioperative COVID-19 Infection, No. (%) | ||||
|---|---|---|---|---|
| Variable | No (n = 154) | Yes (n = 57) | Total (n = 211) | Pa |
| Any Postoperative Complication | <0.001 **b | |||
| No | 141 (91.6) | 42 (73.7) | 183 (86.7) | |
| Yes | 13 (8.4) | 15 (26.3) | 28 (13.3) | |
| CCI | <0.001 **c | |||
| None | 144 (93.5) | 42 (73.7) | 186 (88.2) | |
| Mild | 3 (1.9) | 8 (14) | 11 (5.2) | |
| Severe | 7 (4.5) | 7 (12.3) | 14 (6.6) | |
| Postoperative Hospital Days Mean (SD), days | 10.70 (2.69) | 13.04 (5.04) | 11.33 (3.62) | 0.007 **d |
| Complications | ||||
| Anastomotic fistula | 2 (1.3) | 1 (1.8) | 3 (1.4) | 0.613 c |
| Pneumonia | 6 (3.9) | 9 (15.8) | 15 (7.1) | 0.005 **c |
| Sepsis | 1 (0.6) | 4 (7) | 5 (2.4) | 0.02 *c |
| Urinary tract infection | 1 (0.6) | 1 (1.8) | 2 (0.9) | 0.468 c |
| Ileus | 5 (3.2) | 6 (10.5) | 11 (5.2) | 0.035 *b |
| VTE | 1 (0.6) | 1 (1.8) | 2 (0.9) | 0.468 c |
| Myocardial infarction | 1 (0.6) | 0 (0) | 1 (0.5) | 1.000 c |
| Arrhythmia | 3 (1.9) | 1 (1.8) | 4 (1.9) | 1.000 c |
| Body temperature d, mean (SD) | 37.43 (0.72) | 37.74 (0.82) | 37.51 (0.76) | 0.009 **f |
| Laboratory Findings | ||||
| WBCd, 109/L, mean (SD) | 12.48 (4.00) | 12.40 (4.28) | 12.46 (4.07) | 0.623 f |
| Lymph e, 109/L, mean (SD) | 0.75 (0.29) | 0.66 (0.27) | 0.73 (0.29) | 0.048 *g |
| CRP d, mg/L, median [IQR] | 70.5 [21.7–136.2] | 94 [50–137.5] | 77 [34–136] | 0.013 *g |
| PCT d, ng/mL, median [IQR] | 0.19 [0.08–0.56] | 0.17 [0.07–0.71] | 0.19 [0.08–0.58] | 0.988 g |
| TnI d, ng/mL, median [IQR] | 0.008 [0.004–0.014] | 0.007 [0.003–0.013] | 0.008 [0.004–0.014] | 0.205 g |
| proBNPd, pg/mL, median [IQR] | 512 [231–903] | 302 [164–703] | 372 [201–754] | 0.288 g |
| D-dimerd, mg/L, median [IQR] | 3.6 [1.91–5.41] | 4.42 [3.22–8.45] | 3.92 [2.16–5.74] | 0.003 **g |
| ALT d, U/L, median [IQR] | 17.5 [12–33.2] | 20 [13–34] | 18 [12–33] | 0.214 g |
| AST d, U/L, median [IQR] | 30 [23–42] | 29 [22.5–42] | 30 [23–42] | 0.938 g |
| Cre d, umol/L, median [IQR] | 65.6 [56.5–74.1] | 67 [55.8–79.7] | 66 [56.4–75.9] | 0.672 g |
| Perioperative COVID-19 Infection, No. (%) | |||||
|---|---|---|---|---|---|
| Variable | No COVID-19 (n = 154) | Late Post- COVID-19 (n = 16) | Early Post-COVID-19 (n = 16) | Postoperative COVID-19 (n = 25) | Pa |
| Any Complication | 0.001 **b | ||||
| No | 141 (91.6) | 14 (87.5) | 12 (75) | 16 (64) | |
| Yes | 13 (8.4) | 2 (12.5) | 4 (25) | 9 (36) | |
| CCI | <0.001 **b | ||||
| None | 144 (93.5) | 14 (87.5) | 12 (75) | 16 (64) | |
| Mild | 3 (1.9) | 1 (6.3) | 3 (18.8) | 4 (16) | |
| Severe | 7 (4.5) | 1 (6.3) | 1 (6.3) | 5 (20) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dai, X.; Ding, W.; He, Y.; Huang, S.; Liu, Y.; Wu, T. Clinical Characteristics and Postoperative Complications in Patients Undergoing Colorectal Cancer Surgery with Perioperative COVID-19 Infection. Cancers 2023, 15, 4841. https://doi.org/10.3390/cancers15194841
Dai X, Ding W, He Y, Huang S, Liu Y, Wu T. Clinical Characteristics and Postoperative Complications in Patients Undergoing Colorectal Cancer Surgery with Perioperative COVID-19 Infection. Cancers. 2023; 15(19):4841. https://doi.org/10.3390/cancers15194841
Chicago/Turabian StyleDai, Xuan, Wenjun Ding, Yongshan He, Shiyong Huang, Yun Liu, and Tingyu Wu. 2023. "Clinical Characteristics and Postoperative Complications in Patients Undergoing Colorectal Cancer Surgery with Perioperative COVID-19 Infection" Cancers 15, no. 19: 4841. https://doi.org/10.3390/cancers15194841