
Pediatric Hepatocellular Adenomas: What Is Known and What Is New?

Abstract
:Simple Summary
Abstract
1. Introduction
2. Risk Factors and Epidemiology
3. Presentation and Clinical Features
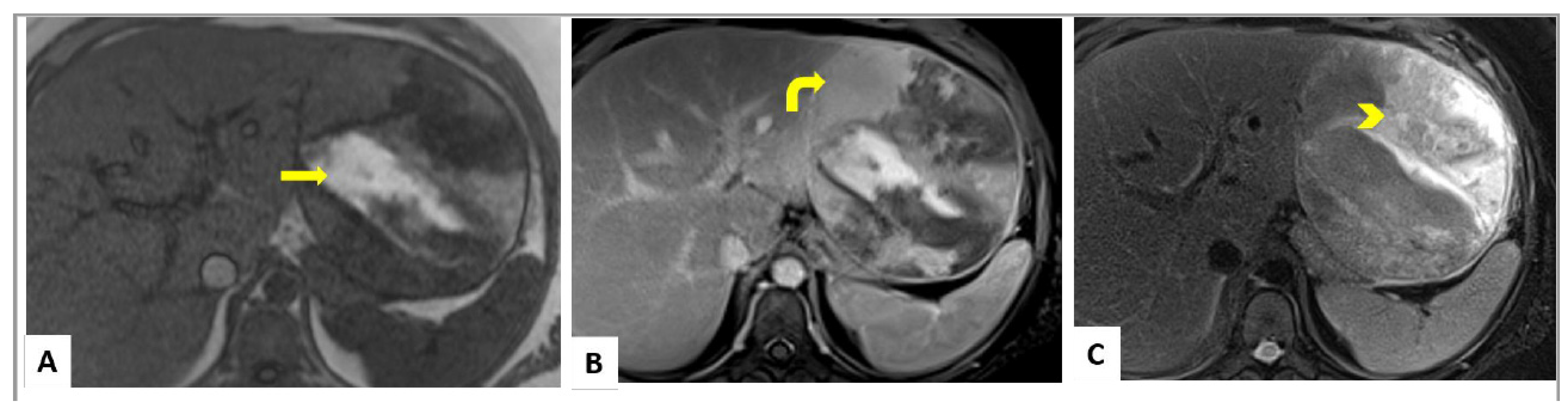
4. Imaging
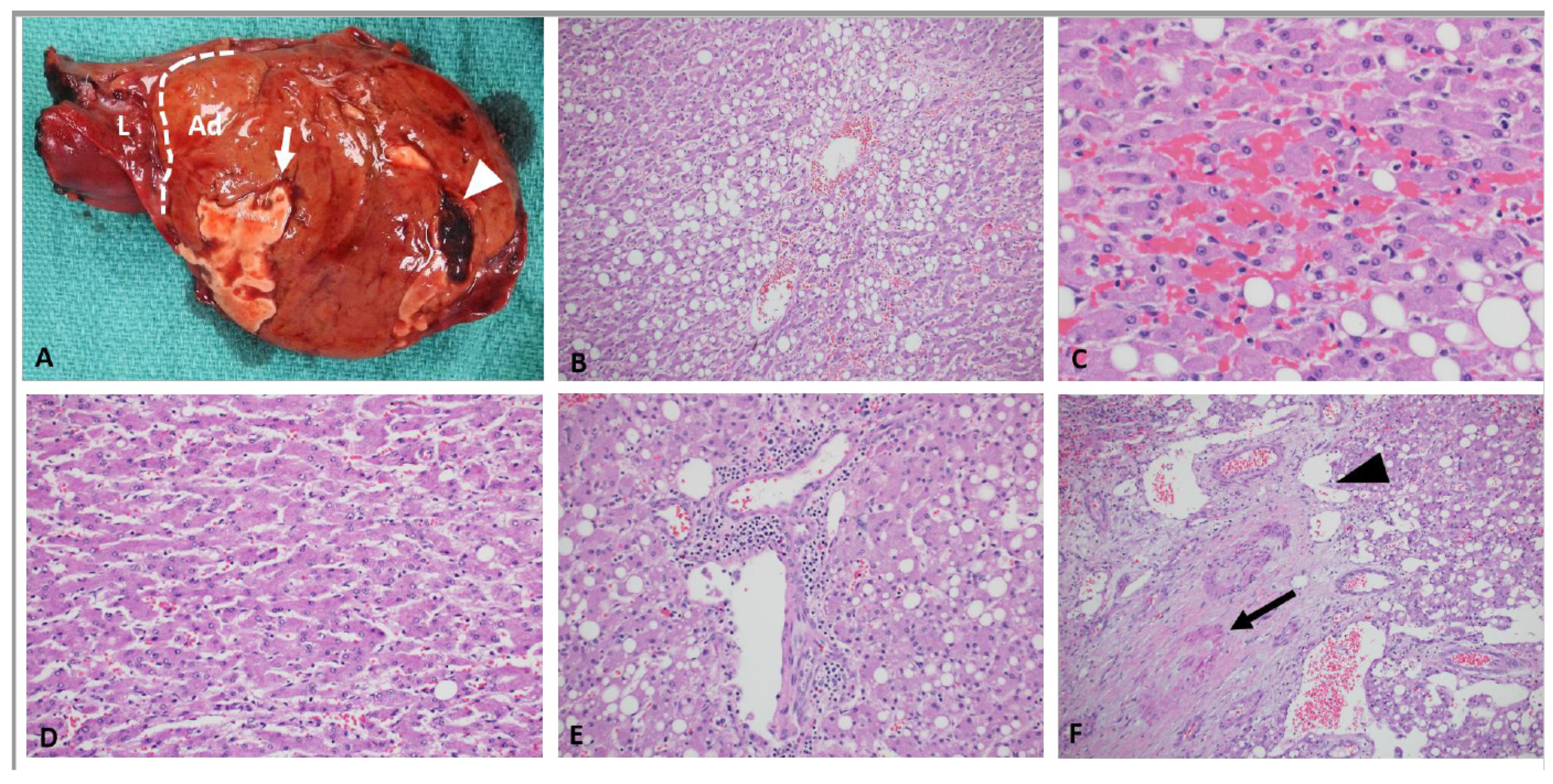
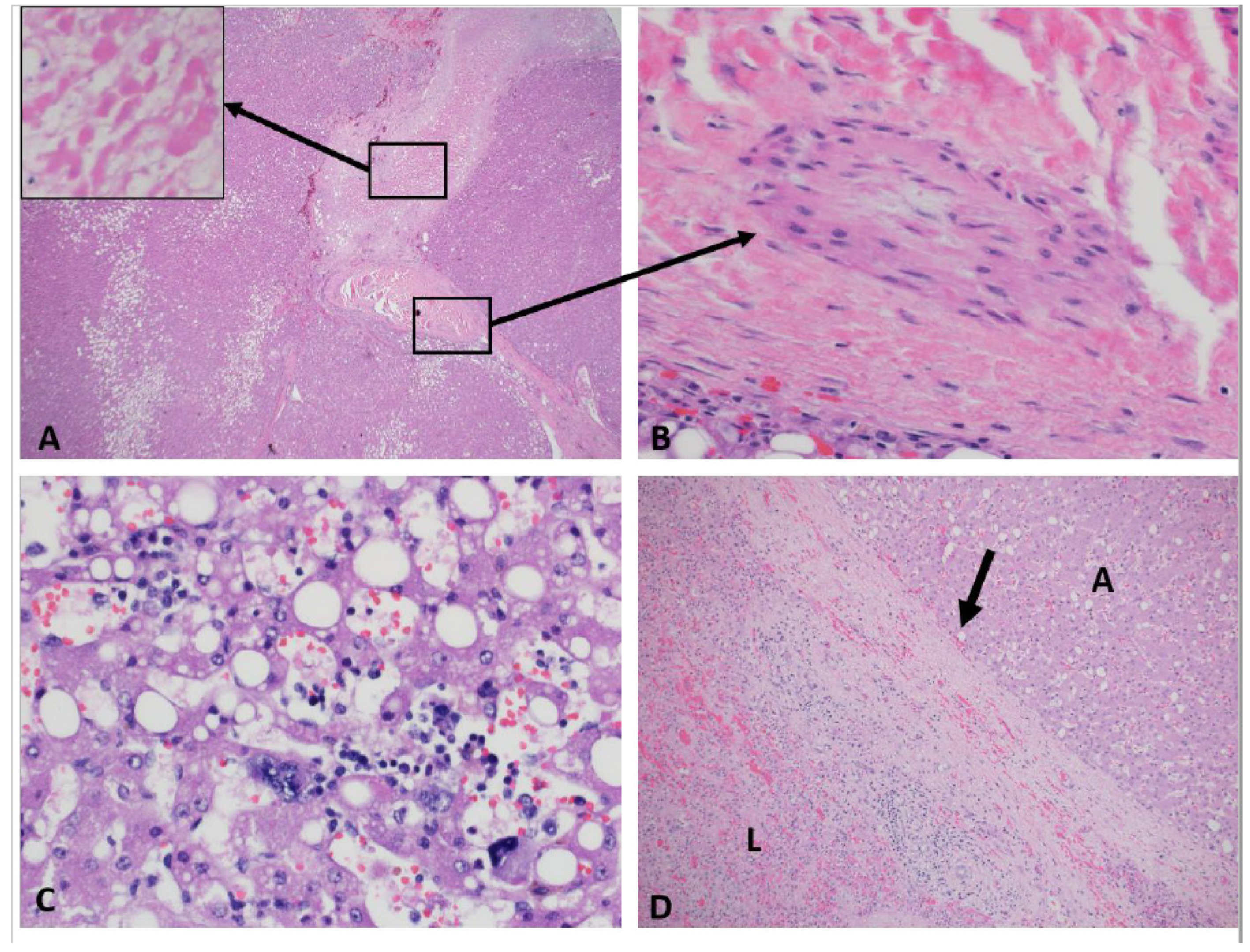
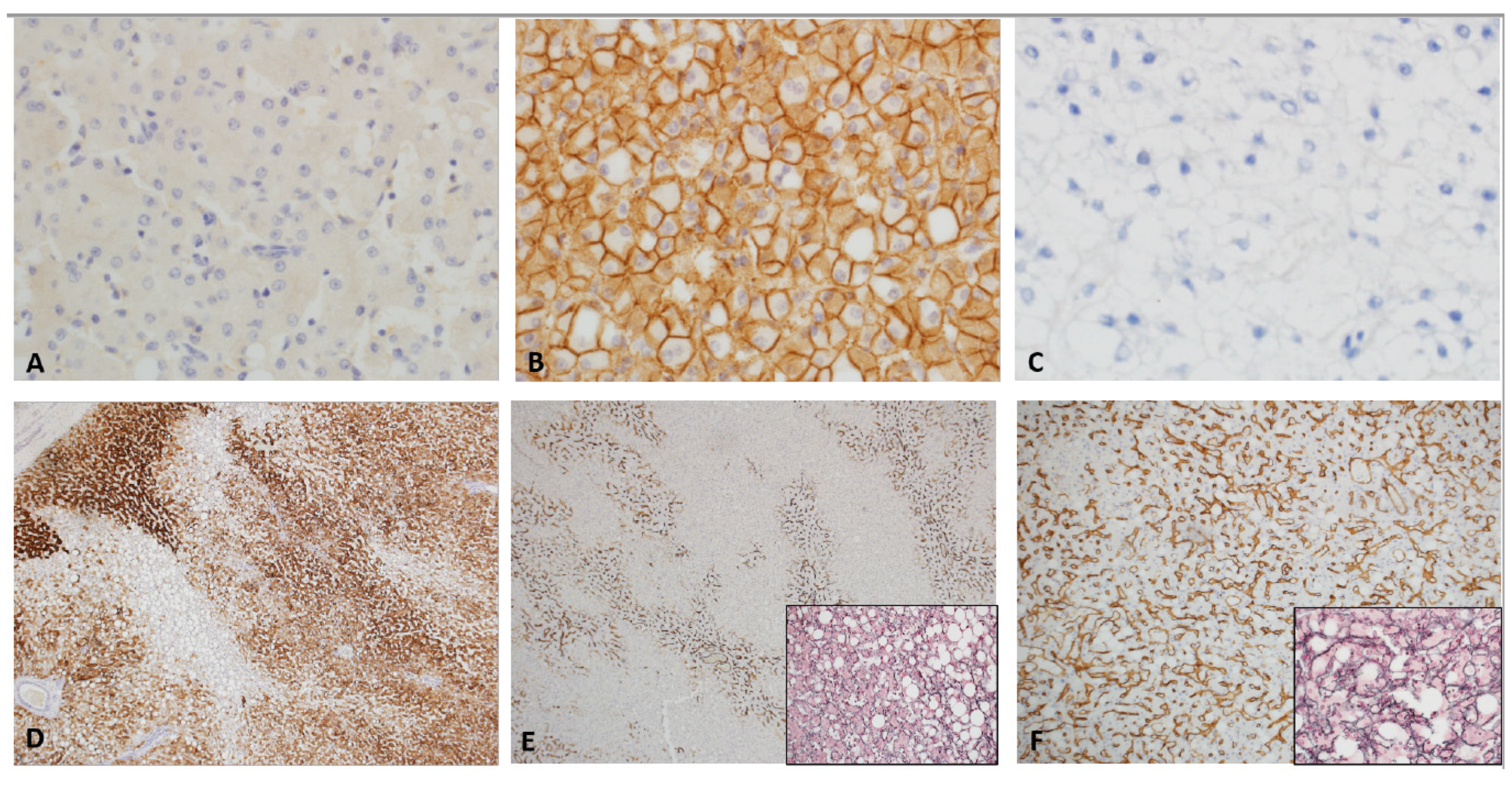
5. Histopathology, Genetics and Classification
6. Management, Complications and Prognosis
7. Future Perspective
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Resnick, M.B.; Kozakewich, H.P.; Perez-Atayde, A.R. Hepatic adenoma in the pediatric age group. Clinicopathological observations and assessment of cell proliferative activity. Am. J. Surg. Pathol. 1995, 19, 1181–1190. [Google Scholar] [CrossRef]
- Hahn, E.; Putra, J. Hepatocellular adenoma in the paediatric population: Molecular classification and clinical associations. World J. Gastroenterol. 2020, 26, 2294–2304. [Google Scholar] [CrossRef] [PubMed]
- Louie, C.Y.; Concepcion, W.; Park, J.K.; Rangaswami, A.; Finegold, M.J.; Hazard, F.K. Hepatoblastoma Arising in a Pigmented β-catenin-activated Hepatocellular Adenoma: Case Report and Review of the Literature. Am. J. Surg. Pathol. 2016, 40, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Sheridan, R.M.; Towbin, A.; Geller, J.I.; Tiao, G.; Bove, K.E. Multifocal hepatic neoplasia in 3 children with APC gene mutation. Am. J. Surg. Pathol. 2013, 37, 1058–1066. [Google Scholar] [CrossRef]
- Kammula, U.S.; Buell, J.F.; Labow, D.M.; Rosen, S.; Millis, J.M.; Posner, M.C. Surgical management of benign tumors of the liver. Int. J. Gastrointest. Cancer 2001, 30, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Bernardo, S.; Sellars, M.E.; Deganello, A.; Sidhu, P.S. Contrast-enhanced ultrasound in the diagnosis of pediatric focal nodular hyperplasia and hepatic adenoma: Interobserver reliability. Pediatr. Radiol. 2019, 49, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Vaithianathan, R.; Philipchandran Selvambigai, G.; Jayaganesh, P. Spontaneous hepatocellular adenoma in paediatric age group-case report. J. Clin. Diagn. Res. 2013, 7, 2962–2963. [Google Scholar] [CrossRef]
- Chiorean, L.; Cui, X.W.; Tannapfel, A.; Franke, D.; Stenzel, M.; Kosiak, W.; Schreiber-Dietrich, D.; Jüngert, J.; Chang, J.M.; Dietrich, C.F. Benign liver tumors in pediatric patients—Review with empHCAsis on imaging features. World J. Gastroenterol. 2015, 21, 8541–8561. [Google Scholar] [CrossRef]
- Nault, J.C.; Couchy, G.; Balabaud, C.; Morcrette, G.; Caruso, S.; Blanc, J.F.; Bacq, Y.; Calderaro, J.; Paradis, V.; Ramos, J.; et al. Molecular Classification of Hepatocellular Adenoma Associates With Risk Factors, Bleeding, and Malignant Transformation. Gastroenterology 2017, 152, 880–894. [Google Scholar] [CrossRef]
- Cheng, L.; Liu, Y.; Wang, W.; Merritt, J.L.; Yeh, M. Hepatocellular Adenoma in a Patient with Ornithine Transcarbamylase Deficiency. Case Rep. Hepatol. 2019, 2019, 2313791. [Google Scholar] [CrossRef]
- Paradis, V.; Bioulac-Sage, P.; Balabaud, C. Congenital hepatic fibrosis with multiple HNF1α hepatocellular adenomas. Clin. Res. Hepatol. Gastroenterol. 2014, 38, e115–e116. [Google Scholar] [CrossRef] [PubMed]
- Haddouche, A.; Bellanne-Chantelot, C.; Rod, A.; Fournier, L.; Chiche, L.; Gautier, J.F.; Timsit, J.; Laboureau, S.; Chaillous, L.; Valero, R.; et al. Liver adenomatosis in patients with hepatocyte nuclear factor-1 alpha maturity onset diabetes of the young (HNF1A-MODY): Clinical, radiological and pathological characteristics in a French series. J. Diabetes. 2020, 12, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Prunotto, G.; Cianci, P.; Cereda, A.; Scatigno, A.; Fossati, C.; Maitz, S.; Biondi, A.; Selicorni, A. Two cases of hepatic adenomas in patients with Wolf-Hirschhorn syndrome: A new rare complication? Am. J. Med. Genet. A 2013, 161, 1759–1762. [Google Scholar] [CrossRef] [PubMed]
- Masserot-Lureau, C.; Adoui, N.; Degos, F.; de Bazelaire, C.; Soulier, J.; Chevret, S.; Socié, G.; Leblanc, T. Incidence of liver abnormalities in Fanconi anemia patients. Am. J. Hematol. 2012, 87, 547–549. [Google Scholar] [CrossRef]
- Liu, Q.Y.; Zhang, W.D.; Lai, D.M.; Ou-Yang, Y.; Gao, M.; Lin, X.F. Hepatic focal nodular hyperplasia in children: Imaging features on multi-slice computed tomography. World J. Gastroenterol. 2012, 18, 7048–7055. [Google Scholar] [CrossRef]
- Ghaferi, A.A.; Hutchins, G.M. Progression of liver pathology in patients undergoing the Fontan procedure: Chronic passive congestion, cardiac cirrhosis, hepatic adenoma, and hepatocellular carcinoma. J. Thorac. Cardiovasc. Surg. 2005, 129, 1348–1352. [Google Scholar] [CrossRef]
- Kumar, A.R.; Wagner, J.E.; Auerbach, A.D.; Coad, J.E.; Dietz, C.A.; Schwarzenberg, S.J.; MacMillan, M.L. Fatal hemorrhage from androgen-related hepatic adenoma after hematopoietic cell transplantation. J. Pediatr. Hematol. Oncol. 2004, 26, 16–18. [Google Scholar] [CrossRef]
- Tonorezos, E.S.; Barnea, D.; Abou-Alfa, G.K.; Bromberg, J.; D’Angelica, M.; Sklar, C.A.; Shia, J.; Oeffinger, K.C. Hepatocellular adenoma among adult survivors of childhood and young adult cancer. Pediatr. Blood Cancer 2017, 64, e26294. [Google Scholar] [CrossRef]
- Lautz, T.B.; Finegold, M.J.; Chin, A.C.; Superina, R.A. Giant hepatic adenoma with atypical features in a patient on oxcarbazepine therapy. J. Pediatr. Surg. 2008, 43, 751–754. [Google Scholar] [CrossRef]
- Applegate, K.E.; Ghei, M.; Perez-Atayde, A.R. Prenatal detection of a solitary liver adenoma. Pediatr. Radiol. 1999, 29, 92–94. [Google Scholar] [CrossRef]
- Haring, M.P.D.; Peeks, F.; Oosterveer, M.H.; Brouwers, M.C.G.J.; Hollak, C.E.M.; Janssen, M.C.H.; Langendonk, J.G.; Rennings, A.J.M.; Wagenmakers, M.A.E.M.; Verkade, H.J.; et al. High childhood serum triglyceride concentrations associate with hepatocellular adenoma development in patients with glycogen storage disease type Ia. JHEP Rep. 2022, 4, 100512. [Google Scholar] [CrossRef] [PubMed]
- Laurent, A.; Dokmak, S.; Nault, J.C.; Pruvot, F.R.; Fabre, J.M.; Letoublon, C.; Bachellier, P.; Capussotti, L.; Farges, O.; Mabrut, J.Y.; et al. European Experience of 573 Liver Resections for Hepatocellular Adenoma: A Cross-Sectional Study by the AFC-HCA-2013 Study Group; HPB: Oxford, UK, 2016; Volume 18, pp. 748–755. [Google Scholar] [CrossRef]
- Sergi, C.M. (Ed.) Liver Cancer [Internet]; Exon Publications: Brisbane, Australia, 2021. [Google Scholar]
- Lucas, B.; Ravishankar, S.; Pateva, I. Pediatric Primary Hepatic Tumors: Diagnostic Considerations. Diagnostics 2021, 11, 333. [Google Scholar] [CrossRef] [PubMed]
- Dharmana, H.; Saravana-Bawan, S.; Girgis, S.; Low, G. Hepatocellular adenoma: Imaging review of the various molecular subtypes. Clin. Radiol. 2017, 72, 276–285. [Google Scholar] [CrossRef]
- van Aalten, S.M.; Thomeer, M.G.; Terkivatan, T.; Dwarkasing, R.S.; Verheij, J.; de Man, R.A.; Ijzermans, J.N. Hepatocellular adenomas: Correlation of MR imaging findings with pathologic subtype classification. Radiology 2011, 261, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Katabathina, V.S.; Menias, C.O.; Shanbhogue, A.K.; Jagirdar, J.; Paspulati, R.M.; Prasad, S.R. Genetics and imaging of hepatocellular adenomas: 2011 update. Radiographics 2011, 31, 1529–1543. [Google Scholar] [CrossRef]
- Pacheco, M.C.; Torbenson, M.S.; Wu, T.T.; Kakar, S.; Jain, D.; Yeh, M.M. Pediatric Hepatocellular Adenomas: The Influence of Age and Syndrome on Subtype. Am. J. Surg. Pathol. 2021, 45, 1641–1647. [Google Scholar] [CrossRef]
- Sasaki, M.; Yoneda, N.; Kitamura, S.; Sato, Y.; Nakanuma, Y. A serum amyloid A-positive hepatocellular neoplasm arising in alcoholic cirrhosis: A previously unrecognized type of inflammatory hepatocellular tumor. Mod. Pathol. 2012, 25, 1584–1593. [Google Scholar] [CrossRef]
- Seo, J.M.; Lee, S.J.; Kim, S.H.; Park, C.K.; Ha, S.Y. Hepatocellular carcinoma arising from hepatocellular adenoma in a hepatitis B virus-associated cirrhotic liver. Clin. Radiol. 2012, 67, 329–333. [Google Scholar] [CrossRef]
- Bioulac-Sage, P.; Rebouissou, S.; Thomas, C.; Blanc, J.F.; Saric, J.; Sa Cunha, A.; Rullier, A.; Cubel, G.; Couchy, G.; Imbeaud, S.; et al. Hepatocellular adenoma subtype classification using molecular markers and immunohistochemistry. Hepatology 2007, 46, 740–748. [Google Scholar] [CrossRef]
- Bioulac-Sage, P.; Taouji, S.; Possenti, L.; Balabaud, C. Hepatocellular adenoma subtypes: The impact of overweight and obesity. Liver Int. 2012, 32, 1217–1221. [Google Scholar] [CrossRef]
- Chavez, P.R.; Lian, F.; Chung, J.; Liu, C.; Paiva, S.A.; Seitz, H.K.; Wang, X.D. Long-term ethanol consumption promotes hepatic tumorigenesis but impairs normal hepatocyte proliferation in rats. J. Nutr. 2011, 141, 1049–1055. [Google Scholar] [CrossRef]
- Sakellariou, S.; Al-Hussaini, H.; Scalori, A.; Samyn, M.; Heaton, N.; Portmann, B.; Tobal, K.; Quaglia, A. Hepatocellular adenoma in glycogen storage disorder type I: A clinicopathological and molecular study. Histopathology 2012, 60, E58–E65. [Google Scholar] [CrossRef] [PubMed]
- Maylee, H.; Harada, K.; Igarashi, S.; Tohda, G.; Yamamoto, M.; Ren, X.S.; Osawa, T.; HCAsegawa, Y.; TakaHCAshi, N.; Nakanuma, Y. Case of telangiectatic/inflammatory hepatocellular adenoma arising in a patient with primary sclerosing cholangitis. Hepatol. Res. 2012, 42, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Paradis, V.; Benzekri, A.; Dargère, D.; Bièche, I.; Laurendeau, I.; Vilgrain, V.; Belghiti, J.; Vidaud, M.; Degott, C.; Bedossa, P. Telangiectatic focal nodular hyperplasia: A variant of hepatocellular adenoma. Gastroenterology 2004, 126, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Bioulac-Sage, P.; Rebouissou, S.; Sa Cunha, A.; Jeannot, E.; Lepreux, S.; Blanc, J.F.; Blanché, H.; Le Bail, B.; Saric, J.; Laurent-Puig, P.; et al. Clinical, morphologic, and molecular features defining so-called telangiectatic focal nodular hyperplasias of the liver. Gastroenterology 2005, 128, 1211–1218. [Google Scholar] [CrossRef]
- Rebouissou, S.; Amessou, M.; Couchy, G.; Poussin, K.; Imbeaud, S.; Pilati, C.; Izard, T.; Balabaud, C.; Bioulac-Sage, P.; Zucman-Rossi, J. Frequent in-frame somatic deletions activate gp130 in inflammatory hepatocellular tumours. Nature 2009, 457, 200–204. [Google Scholar] [CrossRef]
- Jeannot, E.; Poussin, K.; Chiche, L.; Bacq, Y.; Sturm, N.; Scoazec, J.Y.; Buffet, C.; Van Nhieu, J.T.; Bellanné-Chantelot, C.; de Toma, C.; et al. Association of CYP1B1 germ line mutations with hepatocyte nuclear factor 1alpha-mutated hepatocellular adenoma. Cancer Res. 2007, 67, 2611–2616. [Google Scholar] [CrossRef]
- Reznik, Y.; Dao, T.; Coutant, R.; Chiche, L.; Jeannot, E.; Clauin, S.; Rousselot, P.; Fabre, M.; Oberti, F.; Fatome, A.; et al. Hepatocyte nuclear factor-1 alpha gene inactivation: Cosegregation between liver adenomatosis and diabetes phenotypes in two maturity-onset diabetes of the young (MODY)3 families. J. Clin. Endocrinol. Metab. 2004, 89, 1476–1480. [Google Scholar] [CrossRef]
- Bacq, Y.; Jacquemin, E.; Balabaud, C.; Jeannot, E.; Scotto, B.; Branchereau, S.; Laurent, C.; Bourlier, P.; Pariente, D.; de Muret, A.; et al. Familial liver adenomatosis associated with hepatocyte nuclear factor 1alpha inactivation. Gastroenterology 2003, 125, 1470–1475. [Google Scholar] [CrossRef]
- Putra, J.; Ferrell, L.D.; Gouw, A.S.H.; Paradis, V.; Rishi, A.; Sempoux, C.; Balabaud, C.; Thung, S.N.; Bioulac-Sage, P. Malignant transformation of liver fatty acid binding protein-deficient hepatocellular adenomas: Histopathologic spectrum of a rare phenomenon. Mod. Pathol. 2020, 33, 665–675. [Google Scholar] [CrossRef]
- Garcia-Buitrago, M.T. Beta-Catenin Staining of Hepatocellular Adenomas. Gastroenterol. Hepatol. 2017, 13, 740–743. [Google Scholar]
- Bläker, H.; Sutter, C.; Kadmon, M.; Otto, H.F.; Von Knebel-Doeberitz, M.; Gebert, J.; Helmke, B.M. Analysis of somatic APC mutations in rare extracolonic tumors of patients with familial adenomatous polyposis coli. Genes. Chromosomes Cancer 2004, 41, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Jeannot, E.; Wendum, D.; Paye, F.; Mourra, N.; de Toma, C.; Fléjou, J.F.; Zucman-Rossi, J. Hepatocellular adenoma displaying a HNF1alpha inactivation in a patient with familial adenomatous polyposis coli. J. Hepatol. 2006, 45, 883–886. [Google Scholar] [CrossRef] [PubMed]
- Cekuolis, A.; Schreiber-Dietrich, D.; Augustinienė, R.; Taut, H.; Squires, J.; Chaves, E.L.; Dong, Y.; Dietrich, C.F. Incidental Findings in Pediatric Patients: How to Manage Liver Incidentaloma in Pediatric Patients. Cancers 2023, 15, 2360. [Google Scholar] [CrossRef]
- Herman, P.; Fonseca, G.M.; Kruger, J.A.P.; Jeismann, V.B.; Coelho, F.F. Guidelines for the Treatment of Hepatocellular Adenoma in the Era of Molecular Biology: An Experience-Based Surgeons’ Perspective. J. Gastrointest. Surg. 2021, 25, 1494–1502. [Google Scholar] [CrossRef]
- Rosencrantz, R.A.; Wu, Y.; Sonke, P.Y.; Yusuf, Y. Giant hepatocellular adenoma in a previously obese thirteen-year-old boy. Ann. Hepatol. 2015, 14, 559–563. [Google Scholar] [CrossRef]
- Dong, Q.; Jiang, B.; Lu, Y.; Zhang, H.; Jiang, Z.; Lu, H.; Yang, C.; Zhao, J.; Hao, X. Surgical management of giant liver tumor involving the hepatic hilum of children. World J. Surg. 2009, 33, 1520–1525. [Google Scholar] [CrossRef]
- Shreenath, A.P.; Kahloon, A. Hepatic Adenoma. 24 January 2022. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Bayik, D.; Lauko, A.J.; Roversi, G.A.; Serbinowski, E.; Acevedo-Moreno, L.A.; Lanigan, C.; Orujov, M.; Lo, A.; Alban, T.J.; Kim, A.; et al. Hepatobiliary malignancies have distinct peripheral myeloid-derived suppressor cell signatures and tumor myeloid cell profiles. Sci. Rep. 2020, 10, 18848. [Google Scholar] [CrossRef]
- Nault, J.C.; Paradis, V.; Cherqui, D.; Vilgrain, V.; Zucman-Rossi, J. Molecular classification of hepatocellular adenoma in clinical practice. J. Hepatol. 2017, 67, 1074–1083. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Pediatric HCA | Adult HCA |
|---|---|---|
| Background Liver | Often abnormal | Usually normal |
| Incidence | 1:1,000,000 | 4:100,000 |
| Risk factors | Genetic disorders, underlying hepatic parenchymal diseases, obesity | Obesity, alcoholism |
| Sex predisposition | Equal incidence in pre-pubertal girls and boys but higher in post-pubertal girls. | Females > Males |
| Hormonal abnormality | Elevated estrogen, exposure to anabolic steroids. | Elevated estrogen, exposure to oral contraceptive pills and anabolic steroids |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espinoza, A.F.; Vasudevan, S.A.; Masand, P.M.; Lòpez-Terrada, D.H.; Patel, K.R. Pediatric Hepatocellular Adenomas: What Is Known and What Is New? Cancers 2023, 15, 4790. https://doi.org/10.3390/cancers15194790
Espinoza AF, Vasudevan SA, Masand PM, Lòpez-Terrada DH, Patel KR. Pediatric Hepatocellular Adenomas: What Is Known and What Is New? Cancers. 2023; 15(19):4790. https://doi.org/10.3390/cancers15194790
Chicago/Turabian StyleEspinoza, Andres F., Sanjeev A. Vasudevan, Prakash M. Masand, Dolores H. Lòpez-Terrada, and Kalyani R. Patel. 2023. "Pediatric Hepatocellular Adenomas: What Is Known and What Is New?" Cancers 15, no. 19: 4790. https://doi.org/10.3390/cancers15194790