
A Real-World Comparative Analysis of Atezolizumab Plus Bevacizumab and Transarterial Chemoembolization Plus Radiotherapy in Hepatocellular Carcinoma Patients with Portal Vein Tumor Thrombosis
 , , , , , , , , , , , , , add
Show full author list
, , , , , , , , , , , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
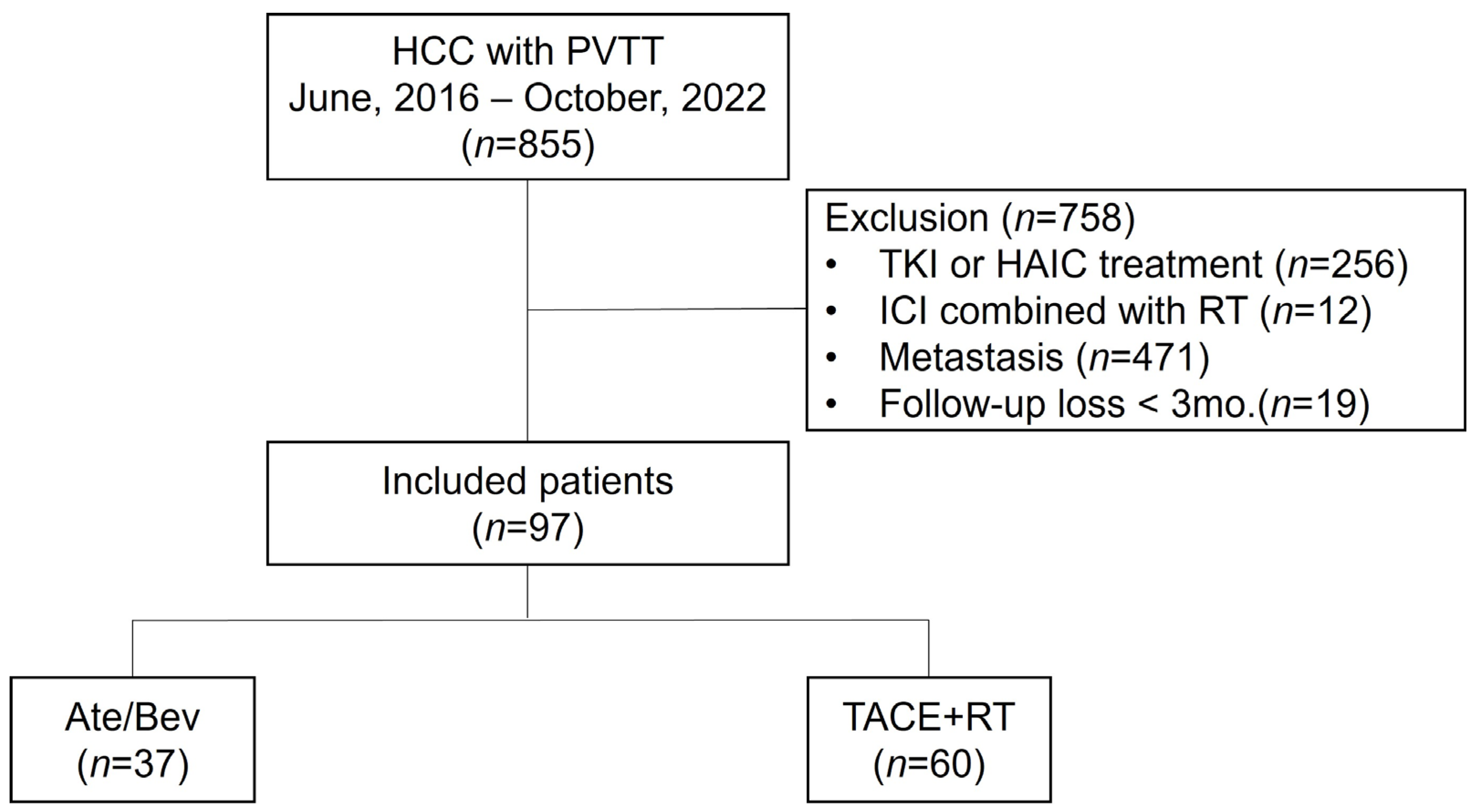
2.1. Patients
2.2. Treatment Regimens
2.3. Assessment of Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. One-Year Survival and PFS in the Entire Population
3.3. Treatment Responses and AEs
3.4. Subgroup Analysis
3.5. Factors Associated with One-Year Survival and PSM Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma. Hepatology 2021, 73 (Suppl. S1), 4–13. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kudo, M.; Venook, A.P.; Ye, S.L.; Bronowicki, J.P.; Chen, X.P.; Dagher, L.; Furuse, J.; Geschwind, J.H.; de Guevara, L.L.; et al. Observational registry of sorafenib use in clinical practice across Child-Pugh subgroups: The GIDEON study. J. Hepatol. 2016, 65, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Cheon, J.; Yoo, C.; Hong, J.Y.; Kim, H.S.; Lee, D.W.; Lee, M.A.; Kim, J.W.; Kim, I.; Oh, S.B.; Hwang, J.E.; et al. Efficacy and safety of atezolizumab plus bevacizumab in Korean patients with advanced hepatocellular carcinoma. Liver Int. 2022, 42, 674–681. [Google Scholar] [CrossRef]
- Su, G.L.; Altayar, O.; O’Shea, R.; Shah, R.; Estfan, B.; Wenzell, C.; Sultan, S.; Falck-Ytter, Y. AGA Clinical Practice Guideline on Systemic Therapy for Hepatocellular Carcinoma. Gastroenterology 2022, 162, 920–934. [Google Scholar] [CrossRef]
- Foerster, F.; Gairing, S.J.; Ilyas, S.I.; Galle, P.R. Emerging immunotherapy for HCC: A guide for hepatologists. Hepatology 2022, 75, 1604–1626. [Google Scholar] [CrossRef]
- Valery, M.; Cervantes, B.; Samaha, R.; Gelli, M.; Smolenschi, C.; Fuerea, A.; Tselikas, L.; Klotz-Prieux, C.; Hollebecque, A.; Boige, V.; et al. Immunotherapy and Hepatocellular Cancer: Where Are We Now? Cancers 2022, 14, 4523. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Yoon, S.M.; Ryoo, B.Y.; Lee, S.J.; Kim, J.H.; Shin, J.H.; An, J.H.; Lee, H.C.; Lim, Y.S. Efficacy and Safety of Transarterial Chemoembolization Plus External Beam Radiotherapy vs Sorafenib in Hepatocellular Carcinoma with Macroscopic Vascular Invasion: A Randomized Clinical Trial. JAMA Oncol. 2018, 4, 661–669. [Google Scholar] [CrossRef]
- 2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma. Clin. Mol. Hepatol. 2022, 28, 583–705. [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.R.; Wei, X.; Xu, X. Portal Vein Tumor Thrombosis and Hepatocellular Carcinoma—The Changing Tides. J. Hepatocell. Carcinoma 2021, 8, 1089–1115. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 5. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 27 November 2017).
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- Goh, M.J.; Sinn, D.H.; Kim, J.M.; Lee, M.W.; Hyun, D.H.; Yu, J.I.; Hong, J.Y.; Choi, M.S. Clinical practice guideline and real-life practice in hepatocellular carcinoma: A Korean perspective. Clin. Mol. Hepatol. 2023, 29, 197–205. [Google Scholar] [CrossRef]
- Guo, L.; Wei, X.; Feng, S.; Zhai, J.; Guo, W.; Shi, J.; Lau, W.Y.; Meng, Y.; Cheng, S. Radiotherapy prior to or after transcatheter arterial chemoembolization for the treatment of hepatocellular carcinoma with portal vein tumor thrombus: A randomized controlled trial. Hepatol. Int. 2022, 16, 1368–1378. [Google Scholar] [CrossRef]
- Facciorusso, A.; Serviddio, G.; Muscatiello, N. Transarterial radioembolization vs chemoembolization for hepatocarcinoma patients: A systematic review and meta-analysis. World J. Hepatol. 2016, 8, 770–778. [Google Scholar] [CrossRef]
- Chang, Y.; Jeong, S.W.; Young Jang, J.; Jae Kim, Y. Recent Updates of Transarterial Chemoembolilzation in Hepatocellular Carcinoma. Int. J. Mol. Sci. 2020, 21, 8165. [Google Scholar] [CrossRef]
- Raoul, J.L.; Forner, A.; Bolondi, L.; Cheung, T.T.; Kloeckner, R.; de Baere, T. Updated use of TACE for hepatocellular carcinoma treatment: How and when to use it based on clinical evidence. Cancer Treat Rev. 2019, 72, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Choi, J.Y.; Jung, E.S.; Kwon, J.H.; Jang, J.W.; Bae, S.H.; Yoon, S.K. An Immunological Perspective on the Mechanism of Drug Induced Liver Injury: Focused on Drugs for Treatment of Hepatocellular Carcinoma and Liver Transplantation. Int. J. Mol. Sci. 2023, 24, 5002. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lu, Y.; Qin, S. Atezolizumab and bevacizumab for hepatocellular carcinoma: Mechanism, pharmacokinetics and future treatment strategies. Future Oncol. 2021, 17, 2243–2256. [Google Scholar] [CrossRef] [PubMed]
- Rajapakse, J.; Khatiwada, S.; Akon, A.C.; Yu, K.L.; Shen, S.; Zekry, A. Unveiling the complex relationship between gut microbiota and liver cancer: Opportunities for novel therapeutic interventions. Gut Microbes 2023, 15, 2240031. [Google Scholar] [CrossRef]
- Lee, S.K.; Lee, S.W.; Jang, J.W.; Bae, S.H.; Choi, J.Y.; Yoon, S.K. Immunological Markers, Prognostic Factors and Challenges Following Curative Treatments for Hepatocellular Carcinoma. Int. J. Mol. Sci. 2021, 22, 10271. [Google Scholar] [CrossRef]
- Chen, Y.; Hu, H.; Yuan, X.; Fan, X.; Zhang, C. Advances in Immune Checkpoint Inhibitors for Advanced Hepatocellular Carcinoma. Front. Immunol. 2022, 13, 896752. [Google Scholar] [CrossRef]
- Donne, R.; Lujambio, A. The liver cancer immune microenvironment: Therapeutic implications for hepatocellular carcinoma. Hepatology 2023, 77, 1773–1796. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, Y.; Hong, W.; Wang, B.; Chen, Y.; Yang, P.; Zhou, J.; Fan, J.; Zeng, Z.; Du, S. Gut microbiota modulate radiotherapy-associated antitumor immune responses against hepatocellular carcinoma Via STING signaling. Gut Microbes 2022, 14, 2119055. [Google Scholar] [CrossRef]
- Wang, K.; Yu, H.M.; Xiang, Y.J.; Cheng, Y.Q.; Ni, Q.Z.; Guo, W.X.; Shi, J.; Feng, S.; Zhai, J.; Cheng, S.Q. Efficacy and safety of radiotherapy combined with atezolizumab plus bevacizumab in treating hepatocellular carcinoma with portal vein tumour thrombus: A study protocol. BMJ Open 2022, 12, e064688. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 97) | General Model | Propensity Score Matching Model | ||||
|---|---|---|---|---|---|---|---|
| Ate/Bev Group | TACE + RT Group | p-Value | Ate/Bev Group | TACE + RT Group | p-Value | ||
| (n = 37) | (n = 60) | (n = 27) | (n = 32) | ||||
| Age, years | 59.1 ± 10.7 | 60.7 ± 12.9 | 58.1 ± 9.0 | 0.283 | 58.1 ± 12.0 | 59.6 ± 9.1 | 0.578 |
| Male | 87 (89.7%) | 35 (94.6%) | 52 (86.7%) | 0.366 | 25 (92.6%) | 30 (93.8%) | 1.000 |
| Cause (n, %) | 0.074 | 0.954 | |||||
| HBV | 73 (76.0%) | 24 (64.9%) | 49 (81.7%) | 20 (74.1%) | 25 (78.1%) | ||
| Others | 23 (24.2%) | 13 (35.1%) | 11 (18.3%) | 7 (25.9%) | 7 (21.9%) | ||
| Treatment-naïve (n, %) | 67 (69.1%) | 22 (59.5%) | 45 (75.0%) | 0.167 | 16 (59.3%) | 25 (78.1%) | 0.199 |
| AST, IU/mL | 70.5 ± 46.1 | 64.1 ± 35.6 | 74.5 ± 51.5 | 0.245 | 68.5 ± 38.2 | 78.5 ± 56.6 | 0.425 |
| ALT, IU/mL | 42.2 ± 31.0 | 35.0 ± 23.7 | 46.5 ± 33.6 | 0.051 | 38.6 ± 26.6 | 49.2 ± 41.3 | 0.240 |
| T.bil, mg/dL | 1.0 ± 0.6 | 0.9 ± 0.7 | 1.1 ± 0.5 | 0.205 | 1.0 ± 0.7 | 1.1 ± 0.5 | 0.945 |
| Alb, g/dL | 3.7 ± 0.6 | 3.8 ± 0.4 | 3.7 ± 0.7 | 0.158 | 3.9 ± 0.4 | 3.9 ± 0.4 | 0.855 |
| PLT, 103/μL | 151.7 ± 64.2 | 162.6 ± 66.0 | 145.0 ± 62.6 | 0.190 | 169.0 ± 69.2 | 151.9 ± 66.6 | 0.339 |
| INR. | 1.1 [1.0; 1.2] | 1.1 [1.0; 1.1] | 1.1 [1.0; 1.2] | 0.293 | 1.1 [1.0; 1.2] | 1.1 [1.0; 1.2] | 0.976 |
| Cr, mg/dL | 0.8 [0.7; 0.9] | 0.7 [0.7; 0.9] | 0.8 [0.6; 0.9] | 0.442 | 0.7 [0.7; 0.9] | 0.9 [0.6; 1.0] | 0.488 |
| CP class A | 84 (86.6%) | 34 (91.9%) | 50 (83.3%) | 0.371 | 24 (88.9%) | 27 (84.4%) | 0.902 |
| AFP, ng/mL | 240.3 [23.9; 1917.6] | 484.4 [40.0; 3175.0] | 189.2 [20.4; 1408.4] | 0.277 | 237.0 [29.9; 2730.0] | 274.6 [27.1; 1408.4] | 0.632 |
| PIVKA, mAU/mL | 1723.0 [161.0; 6670.0] | 2877.0 [230.0; 7521.0] | 1344.0 [140.9; 5870.5] | 0.653 | 2877.0 [245.4; 7753.3] | 3436.3 [208.8; 7065.6] | 0.849 |
| Tumor Size, cm | 8.2 ± 4.6 | 7.6 ± 4.8 | 8.5 ± 4.5 | 0.354 | 7.8 ± 5.0 | 8.8 ± 4.9 | 0.448 |
| Multiple intrahepatic HCC (≥2 nodule) | 68 (70.1%) | 27 (73.0%) | 41 (68.3%) | 0.798 | 19 (70.4%) | 23 (71.9%) | 1.000 |
| Bilobar intrahepatic HCC | 34 (35.1%) | 14 (37.8%) | 20 (33.3%) | 0.816 | 10 (37.0%) | 12 (37.5%) | 1.000 |
| VP4 PVTT | 45 (46.4%) | 15 (40.5%) | 30 (50.0%) | 0.485 | 13 (48.1%) | 15 (46.9%) | 1.000 |
| Adverse Events (AEs) | Total | Ate/Bev | TACE + RT | p-Value |
|---|---|---|---|---|
| (n = 97) | (n = 37) | (n = 60) | ||
| AE yes | 16 (16.5%) | 7 (18.9%) | 9 (15.0%) | 0.823 |
| AE types according to grades | ||||
| Grade 1–2 | 0.068 | |||
| - Proteinuria | 3 (3.1%) | 3 (8.1%) | 0 (0.0%) | |
| - Others | 2 (2.1%) | 1 (2.7%) | 1 (1.7%) | |
| Grade 3–4 | 0.524 | |||
| - Varix bleeding | 7 (7.2%) | 2 (5.4%) | 5 (8.3%) | |
| - Hepatic encephalopathy | 2 (2.1%) | 1 (2.7%) | 1 (1.7%) | |
| - HCC rupture | 2 (2.1%) | 0 (0.0%) | 2 (3.3%) |
| Characteristics | HR | 95% CI | p-Value |
|---|---|---|---|
| Age ≥ 60 | 1.75 | 0.86, 3.54 | 0.12 |
| Male | 2.15 | 0.51, 9.03 | 0.3 |
| Ate/Bev Tx. | 0.38 | 0.15, 1.00 | 0.049 |
| AST ≥ 60, IU/mL | 1.47 | 0.73, 2.96 | 0.3 |
| ALT ≥ 40, IU/mL | 1.16 | 0.58, 2.31 | 0.7 |
| T.bil ≥ 1.0, mg/dL | 1.97 | 0.98, 3.96 | 0.058 |
| Alb ≤ 3.5, g/dL | 1.13 | 0.46, 2.75 | 0.8 |
| INR ≥ 1.1 | 1.00 | 0.50, 2.00 | 1.0 |
| AFP ≥ 200, ng/mL | 0.93 | 0.47, 1.87 | 0.8 |
| PIVKA ≥ 40, mAU/mL | 0.89 | 0.31, 2.55 | 0.8 |
| Size ≥ 8.0, cm | 1.42 | 0.71, 2.85 | 0.3 |
| Multiple intrahepatic HCC | 0.63 | 0.31, 1.28 | 0.2 |
| Bilobar intrahepatic HCC | 0.98 | 0.46, 2.07 | 1.0 |
| VP4 PVTT | 1.33 | 0.66, 2.66 | 0.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.K.; Kwon, J.H.; Lee, S.W.; Lee, H.L.; Kim, H.Y.; Kim, C.W.; Song, D.S.; Chang, U.I.; Yang, J.M.; Nam, S.W.; et al. A Real-World Comparative Analysis of Atezolizumab Plus Bevacizumab and Transarterial Chemoembolization Plus Radiotherapy in Hepatocellular Carcinoma Patients with Portal Vein Tumor Thrombosis. Cancers 2023, 15, 4423. https://doi.org/10.3390/cancers15174423
Lee SK, Kwon JH, Lee SW, Lee HL, Kim HY, Kim CW, Song DS, Chang UI, Yang JM, Nam SW, et al. A Real-World Comparative Analysis of Atezolizumab Plus Bevacizumab and Transarterial Chemoembolization Plus Radiotherapy in Hepatocellular Carcinoma Patients with Portal Vein Tumor Thrombosis. Cancers. 2023; 15(17):4423. https://doi.org/10.3390/cancers15174423
Chicago/Turabian StyleLee, Soon Kyu, Jung Hyun Kwon, Sung Won Lee, Hae Lim Lee, Hee Yeon Kim, Chang Wook Kim, Do Seon Song, U Im Chang, Jin Mo Yang, Soon Woo Nam, and et al. 2023. "A Real-World Comparative Analysis of Atezolizumab Plus Bevacizumab and Transarterial Chemoembolization Plus Radiotherapy in Hepatocellular Carcinoma Patients with Portal Vein Tumor Thrombosis" Cancers 15, no. 17: 4423. https://doi.org/10.3390/cancers15174423