
Cancer and Pregnancy: Estimates in Italy from Record-Linkage Procedures between Cancer Registries and the Hospital Discharge Database
 , , , , , , , , ,
, , , , , , , , , 
 , , add
Show full author list
, , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Hospital Discharge Records Are Selected If They Contain at Least One of the Following Criteria: | ||
|---|---|---|
| Condition | Code | System |
| Complications of Pregnancy, Childbirth, and the Puerperium | 630–677 | ICD9-cm principal or secondary diagnosis |
| Use of health services for pregnancy | V22, V23, V24, V27, V28 | ICD9-cm principal or secondary diagnosis |
| Livebirth or stillbirth | V30–V39 | ICD9-cm principal or secondary diagnosis |
| Obstetrical Procedures | 72–75 | ICD9-cm principal or secondary procedure |
| Obstetrical hospitalization | 370–384 | Diagnosis Related Groups (DRG) |
| Dilation and curettage for termination of pregnancy | 69.01 | ICD9-cm principal or secondary procedure |
| Dilation and curettage following delivery or abortion | 69.02 | ICD9-cm principal or secondary procedure |
| Aspiration curettage of uterus for termination of pregnancy | 69.51 | ICD9-cm principal or secondary procedure |
| Aspiration curettage following delivery or abortion | 69.52 | ICD9-cm principal or secondary procedure |
| Salpingectomy with removal of tubal pregnancy | 66.62 | ICD9-cm principal or secondary procedure |
Appendix B
- Cancer Registry of Alto Adige (2003–2013)
- Cancer Registry of Monza-Brianza (2007–2012)
- Cancer Registry of Cremona (2005–2012)
- Cancer Registry of Mantova (2003–2014)
- Cancer Registry of Bergamo (2007–2015)
- Cancer Registry of Veneto (2003–2015)
- Cancer Registry of Modena (2003–2015)
- Cancer Registry of Reggio Emilia (2003–2015)
- Cancer Registry of ASL Napoli 3 Sud (2003–2015)
- Cancer Registry of Barletta-Andria-Trani (2006–2014)
- Cancer Registry of Lecce (2003–2010)
- Cancer Registry of Catanzaro (2006–2010)
- Cancer Registry of Messina-Catania-Enna (2003–2015)
- Cancer Registry of Siracusa (2003–2015)
- Cancer Registry of Palermo (2003–2015)
- Cancer Registry of Trapani (2003–2011)
- Cancer Registry of Ragusa (2003–2014)
- Cancer Registry of Latina (2009–2013)
- Cancer Registry of Umbria (2003–2015)
References
- Niu, X.; Li, C.I.; Mueller, B.A. Obstetrical and infant outcomes among women with neoplasms during pregnancy. Cancer Causes Control 2019, 30, 651–661. [Google Scholar] [CrossRef]
- Pavlidis, N.A. Coexistence of pregnancy and malignancy. Oncologist 2002, 7, 279–287, Erratum in Oncologist 2002, 7, 585. [Google Scholar] [CrossRef]
- Salani, R.; Billingsley, C.C.; Crafton, S.M. Cancer and pregnancy: An overview for obstetricians and gynecologists. Am. J. Obstet. Gynecol. 2014, 211, 7–14. [Google Scholar] [CrossRef]
- Andersson, T.M.; Johansson, A.L.; Fredriksson, I.; Lambe, M. Cancer during pregnancy and the postpartum period: A population-based study. Cancer 2015, 121, 2072–2077. [Google Scholar] [CrossRef]
- De Haan, J.; Verheecke, M.; Van Calsteren, K.; Van Calster, B.; Shmakov, R.G.; Mhallem Gziri, M.; Halaska, M.J.; Fruscio, R.; Lok, C.A.R.; Boere, I.A.; et al. Oncological management and obstetric and neonatal outcomes for women diagnosed with cancer during pregnancy: A 20-year international cohort study of 1170 patients. Lancet Oncol. 2018, 19, 337–346, Erratum in Lancet Oncol. 2021, 22, e389. [Google Scholar] [CrossRef]
- Lee, Y.Y.; Roberts, C.L.; Dobbins, T.; Stavrou, E.; Black, K.; Morris, J.; Young, J. Incidence and outcomes of pregnancy-associated cancer in Australia, 1994–2008: A population-based linkage study. J. Obstet. Gynaecol. 2012, 119, 1572–1582. [Google Scholar] [CrossRef]
- Amant, F.; Vandenbroucke, T.; Verheecke, M.; Fumagalli, M.; Halaska, M.J.; Boere, I.; Han, S.; Gziri, M.M.; Peccatori, F.; Rob, L.; et al. Pediatric Outcome after Maternal Cancer Diagnosed during Pregnancy. N. Engl. J. Med. 2015, 373, 1824–1834. [Google Scholar] [CrossRef]
- Parazzini, F.; Franchi, M.; Tavani, A.; Negri, E.; Peccatori, F.A. Frequency of Pregnancy Related Cancer: A Population Based Linkage Study in Lombardy, Italy. Int. J. Gynecol. Cancer 2017, 27, 613–619. [Google Scholar] [CrossRef]
- Metcalfe, A.; Cairncross, Z.F.; Friedenreich, C.M.; Ray, J.G.; Nelson, G.; Fell, D.B.; Lisonkova, S.; Bhatti, P.; McMorris, C.; Sikdar, K.C.; et al. Incidence of Pregnancy-Associated Cancer in Two Canadian Provinces: A Population-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 3100. [Google Scholar] [CrossRef]
- Eibye, S.; Kjær, S.K.; Mellemkjær, L. Incidence of pregnancy-associated cancer in Denmark, 1977–2006. Obstet. Gynecol. 2013, 122, 608–617. [Google Scholar] [CrossRef]
- Dalmartello, M.; Negri, E.; La Vecchia, C.; Scarfone, G.; Buonomo, B.; Peccatori, F.A.; Parazzini, F. Frequency of Pregnancy-Associated Cancer: A Systematic Review of Population-Based Studies. Cancers 2020, 12, 1356. [Google Scholar] [CrossRef]
- Gatta, G.; Capocaccia, R.; Botta, L.; Mallone, S.; De Angelis, R.; Ardanaz, E.; Comber, H.; Dimitrova, N.; Leinonen, M.K.; Siesling, S.; et al. Burden and centralised treatment in Europe of rare tumours: Results of RARECAREnet-a population-based study. Lancet Oncol. 2017, 18, 1022–1039, Erratum in Lancet Oncol. 2017, 18, e433. [Google Scholar] [CrossRef] [PubMed]
- Cottreau, C.M.; Dashevsky, I.; Andrade, S.E.; Li, D.K.; Nekhlyudov, L.; Raebel, M.A.; Ritzwoller, D.P.; Partridge, A.H.; Pawloski, P.A.; Toh, S. Pregnancy-Associated Cancer: A U.S. Population-Based Study. J. Women’s Health 2019, 28, 250–257. [Google Scholar] [CrossRef]
- Johansson, A.L.V.; Fredriksson, I.; Mellemkjaer, L.; Stensheim, H.; Lähteenmäki, P.; Winther, J.F.; Ullenhag, G.J.; Lundberg, F.E. Cancer survival in women diagnosed with pregnancy-associated cancer: An overview using nationwide registry data in Sweden 1970–2018. Eur. J. Cancer 2021, 155, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Murgia, F.; Marinaccio, M.; Cormio, G.; Loizzi, V.; Cicinelli, R.; Bettocchi, S.; Cicinelli, E. Pregnancy related cancer in Apulia. A population based linkage study. Eur. J. Obstet. Gynecol. Reprod. Biol. X 2019, 3, 100025. [Google Scholar] [CrossRef] [PubMed]
- Parazzini, F.; Gadducci, A.; Cicinelli, E.; Maggino, T.; Peccatori, F.; Scarfone, G.; Roncella, E.; Scambia, G.; Zola, P.; Sartori, E. Pregnancy-associated cancers: Frequency and temporal trends in Italy. Int. J. Gynecol. Cancer 2020, 30, 241–244. [Google Scholar] [CrossRef]
- Guzzinati, S.; Battagello, J.; Bovo, E.; Baracco, M.; Baracco, S.; Carpin, E.; Dal Cin, A.; Fiore, A.R.; Greco, A.; Martin, G.; et al. Quality control on digital cancer registration. PLoS ONE 2022, 17, e0279415. [Google Scholar] [CrossRef]
- Certificato di Assistenza al Parto (CeDAP). Analisi dell’Evento Nascita—Anno 2021, A Cura di Direzione Generale della Digitalizzazione, del Sistema Informativo Sanitario e della Statistica—Ufficio di Statistica, Anno 2022. Available online: https://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=3264 (accessed on 14 June 2023).
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351, Erratum in Stat. Med. 2001, 20, 655. [Google Scholar] [CrossRef]
- Linkeviciute, A.; Canario, R.; Peccatori, F.A.; Dierickx, K. Guidelines for Cancer Treatment during Pregnancy: Ethics-Related Content Evolution and Implications for Clinicians. Cancers 2022, 14, 4325. [Google Scholar] [CrossRef]
- Galati, F.; Magri, V.; Arias-Cadena, P.A.; Moffa, G.; Rizzo, V.; Pasculli, M.; Botticelli, A.; Pediconi, F. Pregnancy-Associated Breast Cancer: A Diagnostic and Therapeutic Challenge. Diagnostics 2023, 13, 604. [Google Scholar] [CrossRef]
- Peccatori, F.A.; Azim, H.A., Jr.; Orecchia, R.; Hoekstra, H.J.; Pavlidis, N.; Kesic, V.; Pentheroudakis, G.; ESMO Guidelines Working Group. Cancer, pregnancy and fertility: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24 (Suppl. S6), VI160–VI170. [Google Scholar] [CrossRef] [PubMed]
- Paris, I.; Di Giorgio, D.; Carbognin, L.; Corrado, G.; Garganese, G.; Franceschini, G.; Sanchez, A.M.; De Vincenzo, R.P.; Accetta, C.; Terribile, D.A.; et al. Pregnancy-Associated Breast Cancer: A Multidisciplinary Approach. Clin. Breast Cancer 2021, 21, e120–e127. [Google Scholar] [CrossRef] [PubMed]
- McCormick, A.; Peterson, E. Cancer in Pregnancy. Obstet. Gynecol. Clin. N. Am. 2018, 45, 187–200. [Google Scholar] [CrossRef]
- Zemlickis, D.; Lishner, M.; Degendorfer, P.; Panzarella, T.; Burke, B.; Sutcliffe, S.B.; Koren, G. Maternal and fetal outcome after breast cancer in pregnancy. Am. J. Obstet. Gynecol. 1992, 166, 781–787. [Google Scholar] [CrossRef]
- Amant, F.; Deckers, S.; Van Calsteren, K.; Loibl, S.; Halaska, M.; Brepoels, L.; Beijnen, J.; Cardoso, F.; Gentilini, O.; Lagae, L.; et al. Breast cancer in pregnancy: Recommendations of an international consensus meeting. Eur. J. Cancer 2010, 46, 3158–3168. [Google Scholar] [CrossRef] [PubMed]
- Dal Maso, L.; Panato, C.; De Paoli, A.; Mattioli, V.; Serraino, D.; Elisei, R.; Zoppini, G.; Gobitti, C.; Borsatti, E.; Di Felice, E.; et al. Trends in thyroid function testing, neck ultrasound, thyroid fine needle aspiration, and thyroidectomies in North-eastern Italy. J. Endocrinol. Investig. 2021, 44, 1679–1688. [Google Scholar] [CrossRef]
- AIOM. I Numeri del Cancro 2019. Available online: https://www.aiom.it/wp-content/uploads/2019/09/2019_Numeri_Cancro-operatori-web.pdf (accessed on 14 June 2023).
- Di Tucci, C.; Galati, G.; Mattei, G.; Chinè, A.; Fracassi, A.; Muzii, L. Fertility after Cancer: Risks and Successes. Cancers 2022, 14, 2500. [Google Scholar] [CrossRef]
- Lawrenz, B.; Henes, M.; Neunhoeffer, E.; Fehm, T.; Huebner, S.; Kanz, L.; Marini, P.; Mayer, F. Pregnancy after successful cancer treatment: What needs to be considered? Onkologie 2012, 35, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Amant, F.; Lefrère, H.; Borges, V.F.; Cardonick, E.; Lambertini, M.; Loibl, S.; Peccatori, F.; Partridge, A.; Schedin, P. The definition of pregnancy-associated breast cancer is outdated and should no longer be used. Lancet Oncol. 2021, 22, 753–754. [Google Scholar] [CrossRef]
- Lee, Y.Y.; Roberts, C.L.; Young, J.; Dobbins, T. Using hospital discharge data to identify incident pregnancy-associated cancers: A validation study. BMC Pregnancy Childbirth 2013, 13, 37. [Google Scholar] [CrossRef]
- Lu, D.; Ludvigsson, J.F.; Smedby, K.E.; Fall, K.; Valdimarsdóttir, U.; Cnattingius, S.; Fang, F. Maternal Cancer During Pregnancy and Risks of Stillbirth and Infant Mortality. J. Clin. Oncol. 2017, 35, 1522–1529. [Google Scholar] [CrossRef] [PubMed]



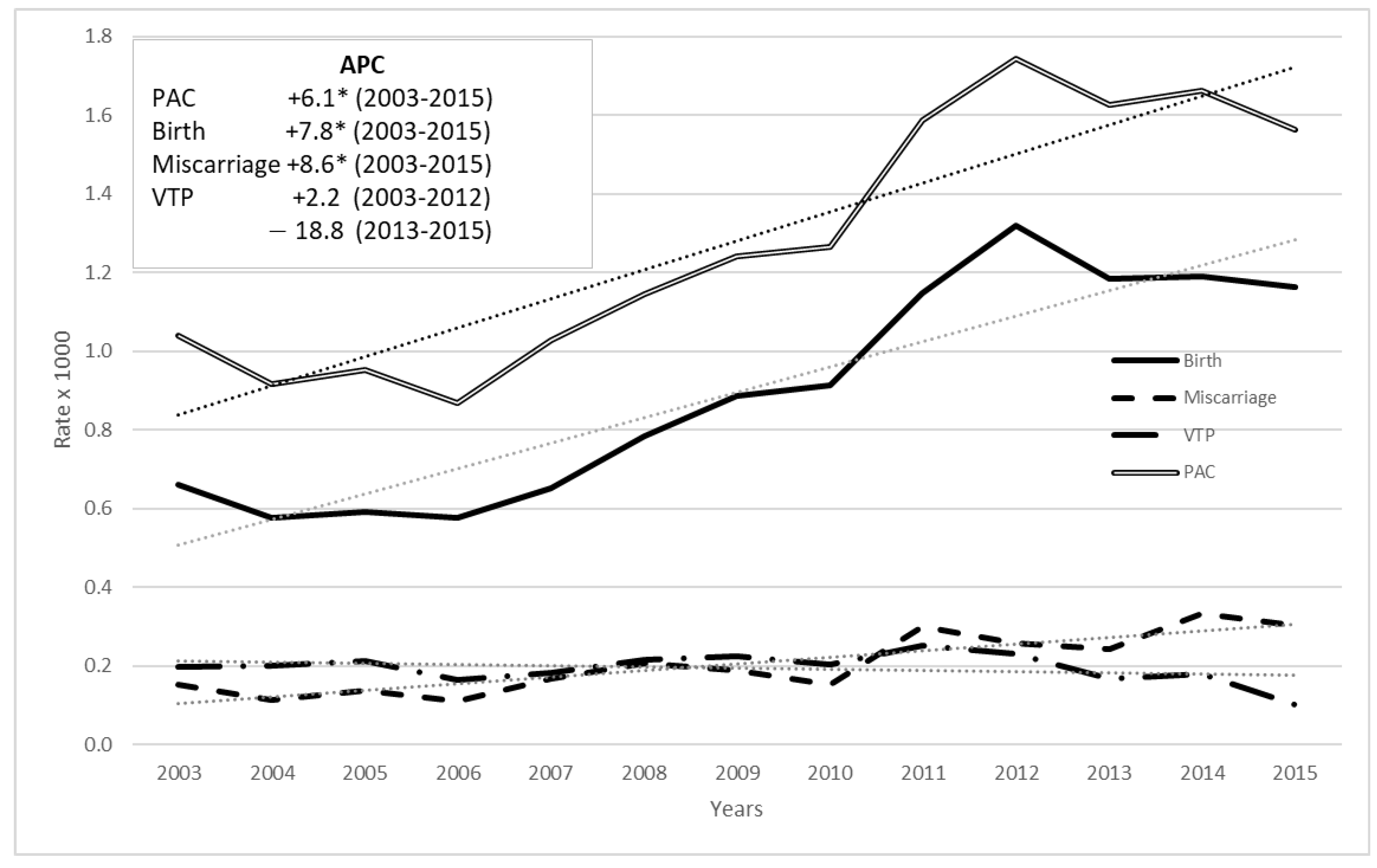
| Year of Cancer Incidence | Women with Cancer Diagnosis | Pregnancies | PAC | PAC/Pregnancies × 1000 |
|---|---|---|---|---|
| 2003 | 4158 | 221,037 | 230 | 1.04 |
| 2004 | 4266 | 228,901 | 210 | 0.92 |
| 2005 | 4488 | 226,995 | 216 | 0.95 |
| 2006 | 4742 | 238,192 | 207 | 0.87 |
| 2007 | 5586 | 262,382 | 270 | 1.03 |
| 2008 | 6306 | 260,398 | 298 | 1.14 |
| 2009 | 6736 | 264,171 | 328 | 1.24 |
| 2010 | 6663 | 260,548 | 330 | 1.27 |
| 2011 | 6166 | 179,601 | 285 | 1.59 |
| 2012 | 6149 | 169,922 | 296 | 1.74 |
| 2013 | 6734 | 201,822 | 328 | 1.63 |
| 2014 | 6393 | 182,407 | 303 | 1.66 |
| 2015 | 5778 | 165,061 | 258 | 1.56 |
| 2003–2015 | 74,165 | 2,861,437 | 3559 | 1.24 |
| Women 15–49 | Women with PAC 15–49 | ||||
|---|---|---|---|---|---|
| Topography * | N | % | N | % | p |
| Breast (C50) | 30,626 | 41.29 | 866 | 24.33 | 0.0000 |
| Thyroid and other endocrine glands (C73–C75) | 11,731 | 15.82 | 849 | 23.86 | 0.0000 |
| Femal genital organs (C51–C58) | 7626 | 10.28 | 350 | 9.83 | 0.3893 |
| Digestive organs (C15–C26) | 5755 | 7.76 | 212 | 5.96 | 0.0001 |
| Melanoma of the skin (C44 with morphology codes: 8720–8790) | 5254 | 7.08 | 510 | 14.33 | 0.0000 |
| Lymph nodes (C77) | 2937 | 3.96 | 200 | 5.62 | 0.0000 |
| Hematopoietic and reticuloendothelial systems (C42) | 2806 | 3.78 | 169 | 4.75 | 0.0034 |
| Respiratory system and intrathoracic organs (C30–C39) | 2292 | 3.09 | 97 | 2.73 | 0.2179 |
| Eye, brain, and other parts of central nervous system (C69–C72) | 1408 | 1.90 | 98 | 2.75 | 0.0003 |
| Urinary tract (C64–C68) | 1361 | 1.84 | 85 | 2.39 | 0.0170 |
| Lip, oral cavity, and pharynx (C00–C14) | 876 | 1.18 | 41 | 1.15 | 0.8750 |
| Connective, subcutaneous, and other soft tissues (C49) | 503 | 0.68 | 35 | 0.98 | 0.0319 |
| Unknown primary site (C80) | 364 | 0.49 | 21 | 0.59 | 0.4100 |
| Bones, joints, and articular cartilage of other and unspecified sites (C40–C41) | 301 | 0.41 | 15 | 0.42 | 0.8863 |
| Other and ill-defined sites (C76) | 157 | 0.21 | 6 | 0.17 | 0.5829 |
| Retroperitoneum and peritoneum (C48) | 136 | 0.18 | 4 | 0.11 | 0.3293 |
| Peripheral nerves and autonomic nervous system (C47) | 32 | 0.04 | 1 | 0.03 | 0.6703 |
| Total | 74,165 | 100.00 | 3559 | 100.00 | |
| All Cancers | ||||
|---|---|---|---|---|
| Pregnancy Outcome | One Year before Cancer Diagnosis | One Year after Cancer Diagnosis | Two Years after Cancer Diagnosis | Total |
| Birth | 59.7 (1477) | 20.0 (495) | 20.3 (502) | 53.1 (2474) |
| Miscarriage | 57.4 (323) | 19.7 (111) | 22.9 (129) | 12.1 (563) |
| Voluntary termination of pregnancy | 45.8 (257) | 36.0 (202) | 18.2 (102) | 12.0 (561) |
| Ectopic pregnancy and hydatidiform mole | 63.0 (46) | 13.7 (10) | 23.3 (17) | 1.6 (73) |
| Pregnancy not classifiable | 46.2 (456) | 35.5 (350) | 18.3 (180) | 21.2 (986) |
| Total | 54.9 (2559) | 25.1 (1168) | 20.0 (930) | 100.0 (4657) |
| Breast | ||||
| Pregnancy Outcome | One Year before Cancer Diagnosis | One Year after Cancer Diagnosis | Two Years after Cancer Diagnosis | Total |
| Birth | 75.4 (419) | 21.0 (117) | 3.6 (20) | 53.1 (556) |
| Miscarriage | 77.6 (118) | 17.1 (26) | 5.3 (8) | 14.5 (152) |
| Voluntary termination of pregnancy | 61.4 (97) | 28.5 (45) | 10.1 (16) | 15.1 (158) |
| Ectopic pregnancy and hydatidiform mole | 63.6 (7) | 9.1 (1) | 27.3 (3) | 1.1 (11) |
| Pregnancy not classifiable | 50.6 (86) | 44.1 (75) | 5.3 (9) | 16.2 (170) |
| Total | 69.4 (727) | 25.2 (264) | 5.4 (56) | 100.0 (1047) |
| Thyroid and Other Endocrine Glands Cancer | ||||
| Pregnancy Outcome | One Year before Cancer Diagnosis | One Year after Cancer Diagnosis | Two Years after Cancer Diagnosis | Total |
| Birth | 52.4 (326) | 16.9 (105) | 30.7 (191) | 56.6 (622) |
| Miscarriage | 45.1 (60) | 21.8 (29) | 33.1 (44) | 12.1 (133) |
| Voluntary termination of pregnancy | 36.3 (58) | 42.5 (68) | 21.2 (34) | 14.6 (160) |
| Ectopic pregnancy and hydatidiform mole | 66.7 (6) | 0.0 (0) | 33.3 (3) | 0.8 (9) |
| Pregnancy not classifiable | 39.7 (69) | 24.1 (42) | 36.2 (63) | 15.8 (174) |
| Total | 47.3 (519) | 22.2 (244) | 30.5 (335) | 100.0 (1098) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pierannunzio, D.; Maraschini, A.; Lopez, T.; Donati, S.; Amodio, R.; Bianconi, F.; Bruni, R.; Castaing, M.; Cirilli, C.; Fantaci, G.; et al. Cancer and Pregnancy: Estimates in Italy from Record-Linkage Procedures between Cancer Registries and the Hospital Discharge Database. Cancers 2023, 15, 4305. https://doi.org/10.3390/cancers15174305
Pierannunzio D, Maraschini A, Lopez T, Donati S, Amodio R, Bianconi F, Bruni R, Castaing M, Cirilli C, Fantaci G, et al. Cancer and Pregnancy: Estimates in Italy from Record-Linkage Procedures between Cancer Registries and the Hospital Discharge Database. Cancers. 2023; 15(17):4305. https://doi.org/10.3390/cancers15174305
Chicago/Turabian StylePierannunzio, Daniela, Alice Maraschini, Tania Lopez, Serena Donati, Rosalba Amodio, Fortunato Bianconi, Rossella Bruni, Marine Castaing, Claudia Cirilli, Giovanna Fantaci, and et al. 2023. "Cancer and Pregnancy: Estimates in Italy from Record-Linkage Procedures between Cancer Registries and the Hospital Discharge Database" Cancers 15, no. 17: 4305. https://doi.org/10.3390/cancers15174305