
Immunotherapy in Urothelial Cancer: Stop When Achieving a Response, Restart upon Disease Progression


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
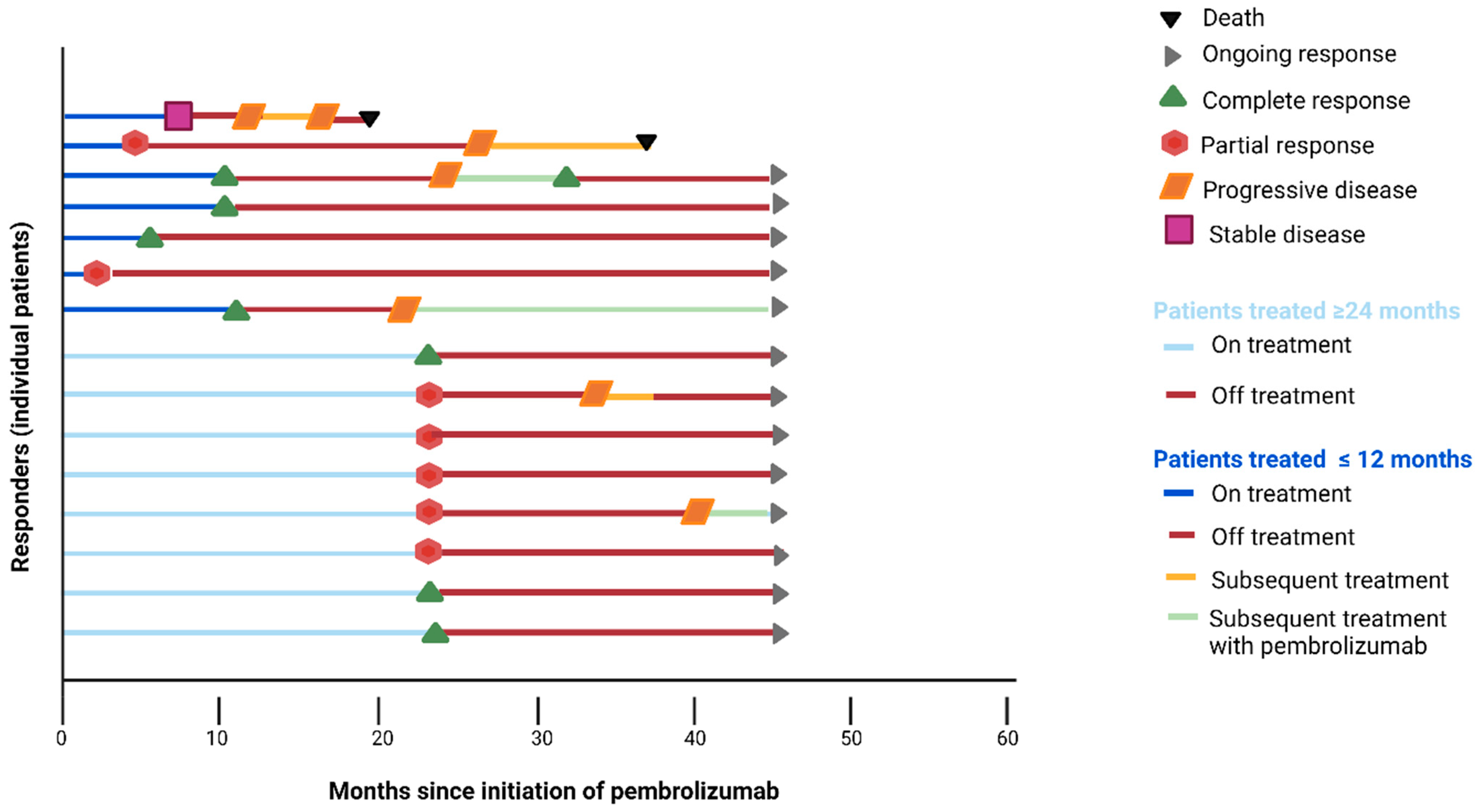
3. Results
3.1. Patients with Treatment Duration ≤ 12 Months
3.2. Patients with Treatment Duration > 12 to <24 Months
3.3. Patients with Treatment Duration of 24 Months
3.4. ctDNA-Based Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Rosenberg, J.E.; Hoffman-Censits, J.; Powles, T.; van der Heijden, M.S.; Balar, A.V.; Necchi, A.; Dawson, N.; O’Donnell, P.H.; Balmanoukian, A.; Loriot, Y.; et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: A single-arm, multicentre, phase 2 trial. Lancet 2016, 387, 1909–1920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, P.; Callahan, M.K.; Bono, P.; Kim, J.; Spiliopoulou, P.; Calvo, E.; Pillai, R.N.; Ott, P.A.; de Braud, F.; Morse, M.; et al. Nivolumab monotherapy in recurrent metastatic urothelial carcinoma (CheckMate 032): A multicentre, open-label, two-stage, multi-arm, phase 1/2 trial. Lancet Oncol. 2016, 17, 1590–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Vuky, J.; Powles, T.; Plimack, E.R.; Hahn, N.M.; de Wit, R.; Pang, L.; et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 1483–1492. [Google Scholar] [CrossRef]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. IMvigor210 Study Group. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2 trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. KEYNOTE-045 Investigators. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [Green Version]
- Powles, T.; Durán, I.; van der Heijden, M.S.; Loriot, Y.; Vogelzang, N.J.; De Giorgi, U.; Oudard, S.; Retz, M.M.; Castellano, D.; Bamias, A.; et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2018, 391, 748–757. [Google Scholar] [CrossRef]
- Mulder, E.E.A.P.; de Joode, K.; Litière, S.; Ten Tije, A.J.; Suijkerbuijk, K.P.M.; Boers-Sonderen, M.J.; Hospers, G.A.P.; de Groot, J.W.B.; van den Eertwegh, A.J.M.; Aarts, M.J.B.; et al. Early discontinuation of PD-1 blockade upon achieving a complete or partial response in patients with advanced melanoma: The multicentre prospective Safe Stop trial. BMC Cancer 2021, 21, 323. [Google Scholar] [CrossRef]
- Pokorny, R.; McPherson, J.P.; Haaland, B.; Grossmann, K.F.; Luckett, C.; Voorhies, B.N.; Sageser, D.S.; Wallentine, J.; Tolman, Z.; Hu-Lieskovan, S.; et al. Real-world experience with elective discontinuation of PD-1 inhibitors at 1 year in patients with metastatic melanoma. J. ImmunoTherapy Cancer 2021, 9, e001781. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef]
- Bilger, G.; Girard, N.; Doubre, H.; Levra, M.G.; Giroux-Leprieur, E.; Giraud, F.; Decroisette, C.; Carton, M.; Massiani, M.A. Discontinuation of immune checkpoint inhibitor (Ici) above 18 months of treatment in real-life patients with advanced non-small cell lung cancer (Nsclc): Intepi, a multicentric retrospective study. Cancer Immunol. Immunother. 2022, 71, 1719–1731. [Google Scholar] [CrossRef]
- Kim, H.; Kim, D.W.; Kim, M.; Lee, Y.; Ahn, H.K.; Cho, J.H.; Kim, I.H.; Lee, Y.-G.; Shin, S.-H.; Park, S.-E.; et al. Long-term outcomes in patients with advanced and/or metastatic non-small cell lung cancer who completed 2 years of immune checkpoint inhibitors or achieved a durable response after discontinuation without disease progression: Multicenter, real-world data (Kcsg Lu20-11). Cancer 2022, 128, 778–787. [Google Scholar] [PubMed]
- Daniel, E.C.; Balar, A.V.; Peter, H.; O’Donnell, P.G.; David, J.V.; Powles, T.; Vuky, J.; Lee, J.-L.; Fradet, Y.; Bellmunt, J.; et al. Post hoc analysis of the efficacy of pembrolizumab retreatment after progression of advanced urothelial carcinoma (UC) in KEYNOTE-045 and KEYNOTE. J. Clin. Oncol. 2022, 40, 512. [Google Scholar]
- Bernard-Tessier, A.; Baldini, C.; Martin, P.; Champiat, S.; Hollebecque, A.; Postel-Vinay, S.; Varga, A.; Bahleda, R.; Gazzah, A.; Michot, J.M.; et al. Outcomes of long-term responders to anti-programmed death 1 and anti-programmed death ligand 1 when being rechallenged with the same anti-programmed death 1 and anti-programmed death ligand 1 at progression. Eur. J. Cancer 2018, 101, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-related adverse events associated with immune checkpoint blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Belic, J.; Koch, M.; Ulz, P.; Auer, M.; Gerhalter, T.; Mohan, S.; Fischereder, K.; Petru, E.; Bauernhofer, T.; Geigl, J.B.; et al. Rapid Identification of Plasma DNA Samples with Increased ctDNA Levels by a Modified FAST-SeqS Approach. Clin. Chem. 2015, 61, 838–849. [Google Scholar] [CrossRef] [Green Version]
- Mendelaar, P.A.J.; Robbrecht, D.G.J.; Rijnders, M.; de Wit, R.; de Weerd, V.; Deger, T.; Westgeest, H.M.; Aarts, M.J.B.; Voortman, J.; Martens, J.W.M.; et al. Genome-wide aneuploidy detected by mFast-SeqS in circulating cell-free DNA is associated with poor response to pembrolizumab in patients with advanced urothelial cancer. Mol Oncol. 2022, 16, 2086–2097. [Google Scholar] [CrossRef]
- Valentin, J.; Ferté, T.; Dorizy-Vuong, V.; Dousset, L.; Prey, S.; Dutriaux, C.; Pham-Ledard, A.; Beylot-Barry, M.; Gérard, E. Real-world survival in patients with metastatic melanoma after discontinuation of anti-Pd-1 immunotherapy for objective response or adverse effects: A retrospective study. J. Oncol. 2021, 2021, 5524685. [Google Scholar] [CrossRef]
- Lasala, R.; Zovi, A.; Isgrò, V.; Romagnoli, A.; Musicco, F.; Santoleri, F. Time to treatment discontinuation in first-line non-small cell lung carcinoma: An overview. Curr. Med. Res. Opin. 2023, 1–10. [Google Scholar] [CrossRef]
- Waterhouse, D.M.; Garon, E.B.; Chandler, J.; McCleod, M.; Hussein, M.; Jotte, R.; Horn, L.; Daniel, D.B.; Keogh, G.; Creelan, B.; et al. Continuous versus 1-year fixed-duration nivolumab in previously treated advanced non-small-cell lung cancer: CheckMate 153. J. Clin. Oncol. 2020, 38, 3863–3873. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Schachter, J.; Arance, A.; Grob, J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.M.; Lotem, M.; et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): Post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019, 20, 1239–1251. [Google Scholar] [CrossRef]
- Jansen, Y.J.L.; Rozeman, E.A.; Mason, R.; Goldinger, S.M.; Foppen, M.H.G.; Hoejberg, L.; Schmidt, H.; van Thienen, J.V.; Haanen, J.B.A.G.; Tiainen, L.; et al. Discontinuation of anti-PD-1 antibody therapy in the absence of disease progression or treatment limiting toxicity: Clinical outcomes in advanced melanoma. Ann. Oncol. 2019, 30, 1154–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.; Weber, J.S.; et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE. Ann. Oncol. 2019, 30, 582–588. [Google Scholar] [CrossRef]
- Iivanainen, S.; Koivunen, J.P. Early PD-1 therapy discontinuation in responding metastatic cancer patients. Oncology 2019, 96, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Ribas, A.; Hamid, O.; Daud, A.; Wolchok, J.D.; Joshua, A.M.; Hwu, W.; Weber, J.S.; Gangadhar, T.C.; Joseph, R.W.; et al. Durable complete response after discontinuation of pembrolizumab in patients with metastatic melanoma. J. Clin. Oncol. 2018, 36, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Gauci, M.; Lanoy, E.; Champiat, S.; Caramella, C.; Ammari, S.; Aspeslagh, S.; Varga, A.; Baldini, C.; Bahleda, R.; Gazzah, A.; et al. Long-term survival in patients responding to Anti-PD-1/PD-L1 therapy and disease outcome upon treatment discontinuation. Clin. Cancer Res. 2019, 25, 946–956. [Google Scholar] [CrossRef] [Green Version]
- Tikkanen, A.; Iivanainen, S.; Koivunen, J.P. Treatment discontinuation and re-initiation of anti-PD-(L)1 agents in metastatic cancers. J. Cancer Res. Clin. Oncol. 2020, 146, 2153–2160. [Google Scholar] [CrossRef] [Green Version]
- Ladwa, R.; Atkinson, V. The cessation of anti-PD-1 antibodies of complete responders in metastatic melanoma. Melanoma Res. 2017, 27, 168–170. [Google Scholar] [CrossRef]
- Pons-Tostivint, E.; Latouche, A.; Vaflard, P.; Ricci, F.; Loirat, D.; Hescot, S.; Sablin, M.P.; Rouzier, R.; Kamal, M.; Morel, C.; et al. Comparative Analysis of Durable Responses on Immune Checkpoint Inhibitors Versus Other Systemic Therapies: A Pooled Analysis of Phase III Trials. JCO Precis Oncol. 2019, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Balar, A.V.; Castellano, D.E.; Grivas, P.; Vaughn, D.J.; Powles, T.; Vuky, J.; Fradet, Y.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; et al. Efficacy and safety of pembrolizumab in metastatic urothelial carcinoma: Results from KEYNOTE-045 and KEYNOTE-052 after up to 5 years of follow-up. Ann. Oncol. 2023, 34, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Vandekerkhove, G.; Todenhöfer, T.; Annala, M.; Struss, W.J.; Wong, A.; Beja, K.; Ritch, E.; Brahmbhatt, S.; Volik, S.V.; Hennenlotter, J.; et al. Circulating Tumor DNA Reveals Clinically Actionable Somatic Genome of Metastatic Bladder Cancer. Clin. Cancer Res. 2017, 23, 6487–6497. [Google Scholar] [CrossRef] [Green Version]
- Weiss, G.J.; Beck, J.; Braun, D.P.; Bornemann-Kolatzki, K.; Barilla, H.; Cubello, R.; Quan, W., Jr.; Sangal, A.; Khemka, V.; Waypa, J.; et al. Tumor Cell-Free DNA Copy Number Instability Predicts Therapeutic Response to Immunotherapy. Clin. Cancer Res. 2017, 23, 5074–5081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibby, A.C.; Torgerson, D.J.; Leach, S.; Lewis-White, H.; Maskell, N.A. Commentary: Considerations for using the ‘Trials within Cohorts’ design in a clinical trial of an investigational medicinal product. Trials 2018, 19, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, R.M.; Spiegelhalter, D.J.; Smith, G.C.; Thompson, S.G. Bias modelling in evidence synthesis. J. R. Stat. Soc. Ser. A Stat. Soc. 2009, 72, 21–47. [Google Scholar] [CrossRef] [Green Version]
- Ghadessi, M.; Tang, R.; Zhou, J.; Liu, R.; Wang, C.; Toyoizumi, K.; Mei, C.; Zhang, L.; Deng, C.Q.; Beckman, R.A. A roadmap to using historical controls in clinical trials—By Drug Information Association Adaptive Design Scientific Working Group (DIA-ADSWG). Orphanet. J. Rare Dis. 2020, 15, 69. [Google Scholar] [CrossRef] [Green Version]
- Basch, E.; Schrag, D.; Henson, S.; Jansen, J.; Ginos, B.; Stover, A.M.; Carr, P.; Spears, P.A.; Jonsson, M.; Deal, A.M.; et al. Effect of Electronic Symptom Monitoring on Patient-Reported Outcomes Among Patients with Metastatic Cancer: A Randomized Clinical Trial. JAMA 2022, 327, 2413–2422. [Google Scholar] [CrossRef] [PubMed]
- Battle, D. Aim for a Cure. 2023. Available online: https://kccure.org/2023/06/aim-for-a-cure-kidney-cancer-asco-2023-learn-more-kccure/ (accessed on 8 June 2023).
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Treatment Duration ≤ 12 Months (n = 7) | Treatment Duration 12–24 Months (n = 2) | Treatment Duration ≥ 24 Months (n = 8) |
|---|---|---|---|
| Age (median, years) | 63 | 71 | 71 |
| Gender | |||
| Male | 5 (71%) | 2 (100%) | 7 (88%) |
| Female | 2 (29%) | 0 (0%) | 1 (12%) |
| Visceral metastases * | |||
| No | 7 (100%) | 0 (0%) | 4 (50%) |
| Yes | 0 (0%) | 2 (100%) | 4 (50%) |
| WHO-status at baseline | |||
| 0 | 5 (71%) | 0 (0%) | 2 (25%) |
| 1 | 2 (29%) | 2 (100%) | 6 (75%) |
| Line of treatment | |||
| First line pembrolizumab | 3 (43%) | 0 (0%) | 2 (25%) |
| Second line pembrolizumab | 4 (57%) | 2 (100%) | 6 (75%) |
| Characteristic | Treatment Duration ≤ 12 Months (n = 7) | Treatment Duration 12–24 Months (n = 2) | Treatment Duration ≥ 24 Months (n = 8) |
|---|---|---|---|
| PD-L1 status ^ | |||
| Negative | 2 (29%) | 0 (0%) | 3 (38%) |
| Positive | 5 (71%) | 2 (100%) | 5 (62%) |
| mFast-SeqS aneuploidy score | |||
| at baseline # | |||
| High (≥5) | 0 (0%) | 0 (0%) | 1 (12%) |
| Low (<5) | 7 (100%) | 2 (100%) | 7 (88%) |
| mFast-SeqS aneuploidy score | |||
| prior to cycle 2 pembrolizumab # | |||
| High (≥5) | 0 (0%) | 0 (0%) | 1 (12%) b |
| Low (<5) | 6 (86%) a | 2 (100%) | 7 (88%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salhi, Y.; De Wit, R.; Robbrecht, D. Immunotherapy in Urothelial Cancer: Stop When Achieving a Response, Restart upon Disease Progression. Cancers 2023, 15, 3654. https://doi.org/10.3390/cancers15143654
Salhi Y, De Wit R, Robbrecht D. Immunotherapy in Urothelial Cancer: Stop When Achieving a Response, Restart upon Disease Progression. Cancers. 2023; 15(14):3654. https://doi.org/10.3390/cancers15143654
Chicago/Turabian StyleSalhi, Youssra, Ronald De Wit, and Debbie Robbrecht. 2023. "Immunotherapy in Urothelial Cancer: Stop When Achieving a Response, Restart upon Disease Progression" Cancers 15, no. 14: 3654. https://doi.org/10.3390/cancers15143654