
Efficacy of Immune Checkpoint Inhibitor (ICI) Rechallenge in Advanced Melanoma Patients’ Responders to a First Course of ICI: A Multicenter National Retrospective Study of the French Group of Skin Cancers (Groupe de Cancérologie Cutanée, GCC)

 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Patients
2.3. Objectives
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Patients
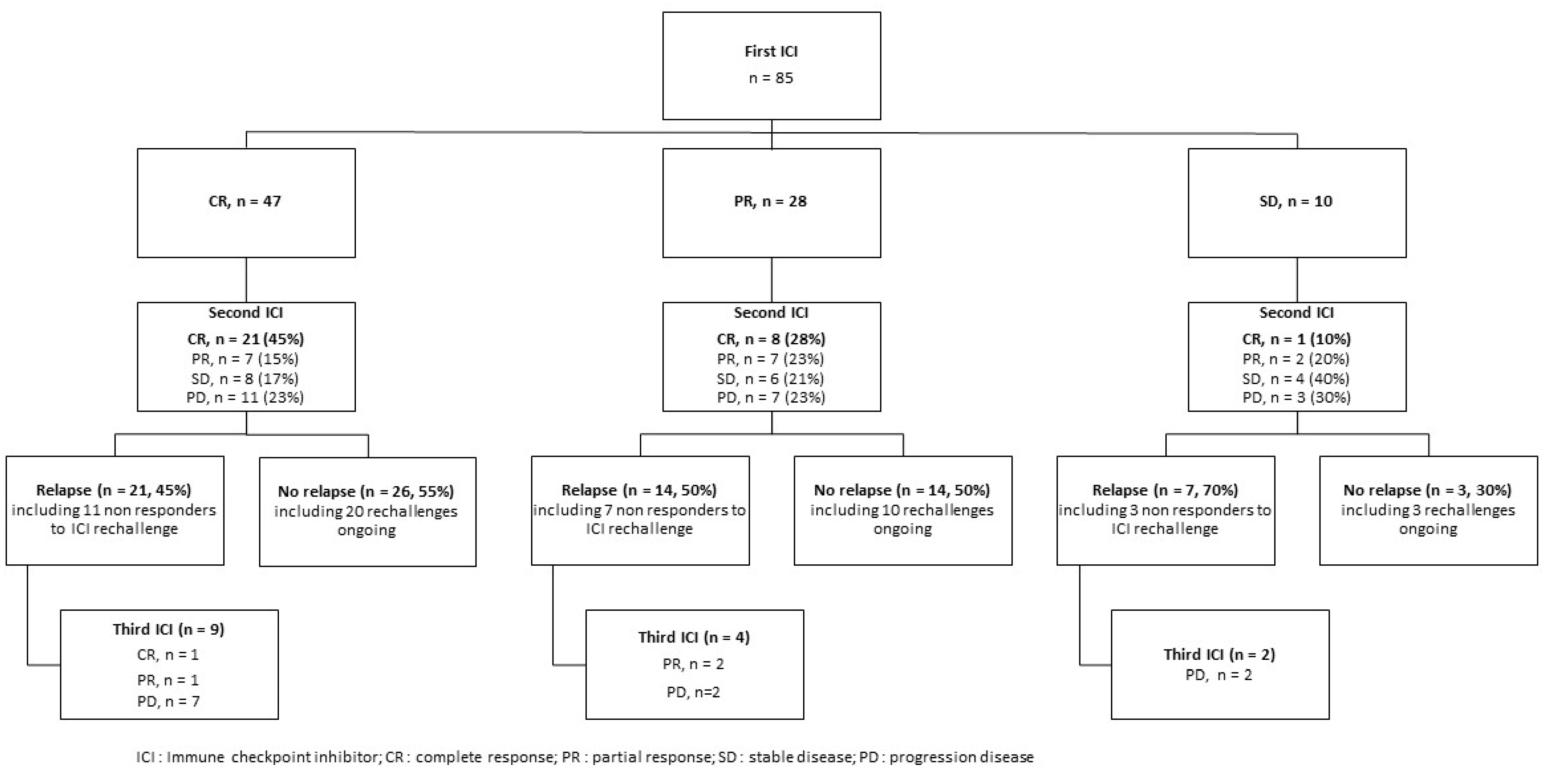
3.2. Response to ICI Rechallenge
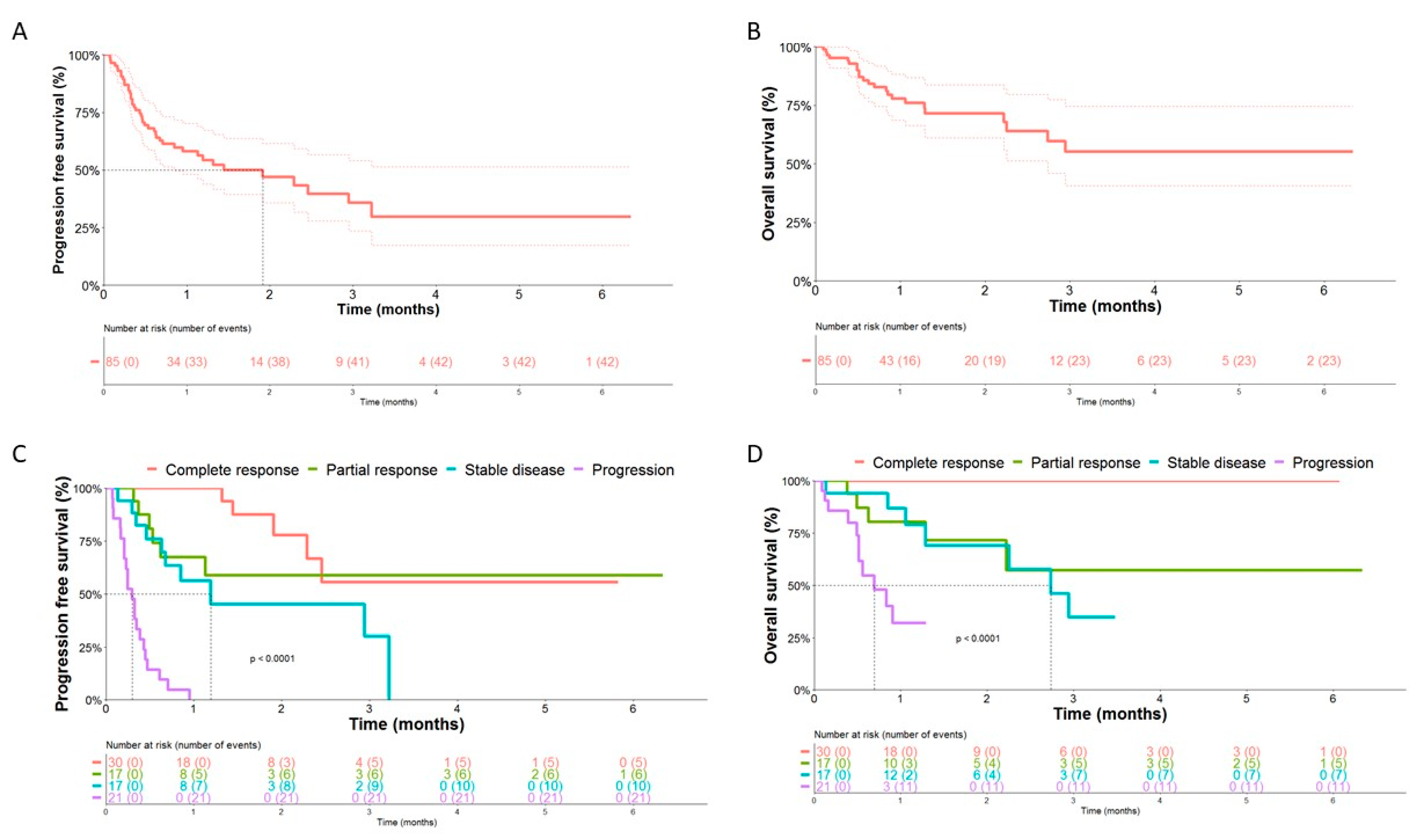
3.3. Progression-Free Survival and Overall Survival
3.4. Factors Associated with Response and Outcomes to ICI Rechallenge
3.5. Second Rechallenge with Immune Checkpoint Inhibitors
3.6. Safety of ICI Rechallenge
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keilholz, U.; Ascierto, P.A.; Dummer, R.; Robert, C.; Lorigan, P.; van Akkooi, A.; Arance, A.; Blank, C.U.; Chiarion Sileni, V.; Donia, M.; et al. ESMO consensus conference recommendations on the management of metastatic melanoma: Under the auspices of the ESMO Guidelines Committee. Ann. Oncol. 2020, 31, 1435–1448. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Hamid, O.; Daud, A.; Wolchok, J.D.; Joshua, A.M.; Hwu, W.J.; Weber, J.S.; Gangadhar, T.C.; Joseph, R.W.; et al. Durable Complete Response After Discontinuation of Pembrolizumab in Patients With Metastatic Melanoma. J. Clin. Oncol. 2018, 36, 1668–1674. [Google Scholar] [CrossRef]
- Robert, C.; Marabelle, A.; Herrscher, H.; Caramella, C.; Rouby, P.; Fizazi, K.; Besse, B. Immunotherapy discontinuation—How, and when? Data from melanoma as a paradigm. Nat. Rev. Clin. Oncol. 2020, 17, 707–715. [Google Scholar] [CrossRef]
- Lebbé, C.; Weber, J.S.; Maio, M.; Neyns, B.; Harmankaya, K.; Hamid, O.; O’Day, S.J.; Konto, C.; Cykowski, L.; McHenry, M.B.; et al. Survival follow-up and ipilimumab retreatment of patients with advanced melanoma who received ipilimumab in prior phase II studies. Ann. Oncol. 2014, 25, 2277–2284. [Google Scholar] [CrossRef] [PubMed]
- Chiarion-Sileni, V.; Pigozzo, J.; Ascierto, P.A.; Simeone, E.; Maio, M.; Calabrò, L.; Marchetti, P.; De Galitiis, F.; Testori, A.; Ferrucci, P.F.; et al. Ipilimumab retreatment in patients with pretreated advanced melanoma: The expanded access programme in Italy. Br. J. Cancer 2014, 110, 1721–1726. [Google Scholar] [CrossRef] [Green Version]
- Larkin, J.; Minor, D.; D’Angelo, S.; Neyns, B.; Smylie, M.; Miller WHJr Gutzmer, R.; Linette, G.; Chmielowski, B.; Lao, C.D.; Lorigan, P.; et al. Overall Survival in Patients With Advanced Melanoma Who Received Nivolumab Versus Investigator’s Choice Chemotherapy in CheckMate 037: A Randomized, Controlled, Open-Label Phase III Trial. J. Clin. Oncol. 2018, 36, 383–390. [Google Scholar] [CrossRef]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.; Weber, J.S.; et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE-001. Ann Oncol. 2019, 30, 582–588. [Google Scholar] [CrossRef]
- Pollack, M.H.; Betof, A.; Dearden, H.; Rapazzo, K.; Valentine, I.; Brohl, A.S.; Ancell, K.K.; Long, G.V.; Menzies, A.M.; Eroglu, Z.; et al. Safety of resuming anti-PD-1 in patients with immune-related adverse events (irAEs) during combined anti-CTLA-4 and anti-PD1 in metastatic melanoma. Ann. Oncol. 2018, 29, 250–255. [Google Scholar] [CrossRef]
- Spain, L.; Walls, G.; Messiou, C.; Turajlic, S.; Gore, M.; Larkin, J. Efficacy and toxicity of rechallenge with combination immune checkpoint blockade in metastatic melanoma: A case series. Cancer Immunol. Immunother. 2017, 66, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, L.; Apuri, S.; Eroglu, Z.; Kottschade, L.A.; Forschner, A.; Gutzmer, R.; Schlaak, M.; Heinzerling, L.; Krackhardt, A.M.; Loquai, C.; et al. Ipilimumab alone or in combination with nivolumab after progression on anti-PD-1 therapy in advanced melanoma. Eur. J. Cancer 2017, 75, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Brunot, A.; Grob, J.J.; Jeudy, G.; Grange, F.; Guillot, B.; Kramkimel, N.; Mortier, L.; Le Corre, Y.; Aubin, F.F.; Mansard, S.; et al. Association of Anti-Programmed Cell Death 1 Antibody Treatment With Risk of Recurrence of Toxic Effects After Immune-Related Adverse Events of Ipilimumab in Patients With Metastatic Melanoma. JAMA Dermatol. 2020, 156, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Schachter, J.; Ribas, A.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus ipilimumab for advanced melanoma: Final overall survival results of a multicentre, randomised, open-label phase 3 study (KEYNOTE-006). Lancet 2017, 390, 1853–1862. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Schachter, J.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.M.; Lotem, M.; et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): Post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019, 20, 1239–1251. [Google Scholar] [CrossRef] [PubMed]
- Jansen, Y.J.L.; Rozeman, E.A.; Mason, R.; Goldinger, S.M.; Geukes Foppen, M.H.; Hoejberg, L.; Schmidt, H.; van Thienen, J.V.; Haanen, J.B.A.G.; Tiainen, L.; et al. Discontinuation of anti-PD-1 antibody therapy in the absence of disease progression or treatment limiting toxicity: Clinical outcomes in advanced melanoma. Ann. Oncol. 2019, 30, 1154–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asher, N.; Israeli-Weller, N.; Shapira-Frommer, R.; Ben-Betzalel, G.; Schachter, J.; Meirson, T.; Markel, G. Immunotherapy Discontinuation in Metastatic Melanoma: Lessons from Real-Life Clinical Experience. Cancers 2021, 13, 3074. [Google Scholar] [CrossRef]
- Whitman, E.D.; Scherrer, E.; Ou, W.; Krepler, C. Outcomes of retreatment with anti-PD-1 monotherapy after response to first course in patients with cutaneous melanoma. Future Oncol. 2020, 16, 1441–1453. [Google Scholar] [CrossRef]
- Dutheil, A.; Belkadi, D.; Antigny, M.; Roy, S.; Lupu, J.; Vallet, A.; Routier, E.; Robert, C. Complete responders to checkpoint inhibitors in advanced melanoma: Relapse risk factors, and patients’ outcomes. J. Clin. Oncol. 2021, 39, 9550. [Google Scholar] [CrossRef]
- Van Zeijl, M.C.T.; van den Eertwegh, A.J.M.; Wouters, M.W.J.M.; de Wreede, L.C.; Aarts, M.J.B.; van den Berkmortel, F.W.P.J.; de Groot, J.B.; Hospers, G.A.P.; Kapiteijn, E.; Piersma, D.; et al. Discontinuation of anti-PD-1 monotherapy in advanced melanoma-Outcomes of daily clinical practice. Int. J. Cancer 2022, 150, 317–326. [Google Scholar] [CrossRef]
- Zaremba, A.; Eggermont, A.M.M.; Robert, C.; Dummer, R.; Ugurel, S.; Livingstone, E.; Ascierto, P.A.; Long, G.V.; Schadendorf, D.; Zimmer, L. The concepts of rechallenge and retreatment with immune checkpoint blockade in melanoma patients. Eur. J. Cancer 2021, 155, 268–280. [Google Scholar] [CrossRef] [PubMed]
- Betof Warner, A.; Palmer, J.S.; Shoushtari, A.N.; Goldman, D.A.; Panageas, K.S.; Hayes, S.A.; Bajwa, R.; Momtaz, P.; Callahan, M.K.; Wolchok, J.D.; et al. Long-Term Outcomes and Responses to Retreatment in Patients With Melanoma Treated With PD-1 Blockade. J. Clin. Oncol. 2020, 38, 1655–1663. [Google Scholar] [CrossRef]
- Pokorny, R.; McPherson, J.P.; Haaland, B.; Grossmann, K.F.; Luckett, C.; Voorhies, B.N.; Sageser, D.S.; Wallentine, J.; Tolman, Z.; Hu-Lieskovan, S.; et al. Real-world experience with elective discontinuation of PD-1 inhibitors at 1 year in patients with metastatic melanoma. J. Immunother. Cancer 2021, 9, e001781. [Google Scholar] [CrossRef] [PubMed]
- Nardin, C.; Jeand’heur, A.; Bouiller, K.; Valnet-Rabier, M.B.; Dresco, F.; Castagna, J.; Mareschal, A.; Carlet, C.; Nerich, V.; Limat, S.; et al. Vitiligo under anti-programmed cell death-1 therapy is associated with increased survival in melanoma patients. J. Am. Acad. Dermatol. 2020, 82, 770–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, C.; Mohr, P.; Bluhm, L.; Grimmelmann, I.; Gutzmer, R.; Meier, F.; Garzarolli, M.; Weichenthal, M.; Pfoehler, C.; Herbst, R.; et al. Impact of radiotherapy and sequencing of systemic therapy on survival outcomes in melanoma patients with previously untreated brain metastasis: A multicenter DeCOG study on 450 patients from the prospective skin cancer registry ADOREG. J. Immunother. Cancer 2022, 10, e004509. [Google Scholar] [CrossRef]
- Maugeais, M.; Péron, J.; Dalle, S.; Boespflug, A.; Duruissaux, M.; Corbaux, P.; Reverdy, T.; Sahin, G.; Rabier, A.; Lopez, J.; et al. Impact of Liver Metastases and Number of Metastatic Sites on Immune-Checkpoint Inhibitors Efficacy in Patients with Different Solid Tumors: A Retrospective Study. Biomedicines 2023, 11, 83. [Google Scholar] [CrossRef]
- Petrelli, F.; Signorelli, D.; Ghidini, M.; Ghidini, A.; Pizzutilo, E.G.; Ruggieri, L.; Cabiddu, M.; Borgonovo, K.; Dognini, G.; Brighenti, M.; et al. Association of Steroids use with Survival in Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Cancers 2020, 12, 546. [Google Scholar] [CrossRef] [Green Version]
- Reschke, R.; Ziemer, M. Rechallenge with checkpoint inhibitors in metastatic melanoma. J. Dtsch. Dermatol. Ges. 2020, 18, 429–436. [Google Scholar] [CrossRef] [Green Version]
- Alrabadi, N.N.; Abushukair, H.M.; Ababneh, O.E.; Syaj, S.S.; Al-Horani, S.S.; Qarqash, A.A.; Darabseh, O.A.; Al-Sous, M.M.; Al-Aomar, S.R.; Ahmed, Y.B.; et al. Systematic review and meta-analysis efficacy and safety of immune checkpoint inhibitors in advanced melanoma patients with anti-PD-1 progression: A systematic review and meta-analysis. Clin. Transl. Oncol. 2021, 23, 1885–1904. [Google Scholar] [CrossRef]
- Carlet, C.; Dalle, S.; Leccia, M.T.; Mortier, L.; Dalac-Rat, S.; Dutriaux, C.; Legoupil, D.; Montaudié, H.; Dereure, O.; De Quatrebarbes, J.; et al. Late-onset adverse events of anti-PD1 therapy in melanoma patients: An observational study from MELBASE, a nationwide prospective cohort. J. Am. Acad. Dermatol. 2022, 86, 345–352. [Google Scholar] [CrossRef]
- Das, S.; Johnson, D.B. Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 306. [Google Scholar] [CrossRef] [PubMed]
- Indini, A.; Di Guardo, L.; Cimminiello, C.; Prisciandaro, M.; Randon, G.; De Braud, F.; Del Vecchio, M. Immune-related adverse events correlate with improved survival in patients undergoing anti-PD1 immunotherapy for metastatic mela s undergoing anti-PD1 immunotherapy for metastatic melanoma. J. Cancer Res. Clin. Oncol. 2019, 145, 511–521. [Google Scholar] [CrossRef]
- Robert, C.; Schadendorf, D.; Messina, M.; Hodi, F.S.; O’Day, S.; MDX010-20 investigators. Efficacy and safety of retreatment with ipilimumab in patients with pretreated advanced melanoma who progressed after initially achieving disease control. Clin. Cancer Res. 2013, 19, 2232–2239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutros, C.; Tarhini, A.; Routier, E.; Lambotte, O.; Ladurie, F.L.; Carbonnel, F.; Izzeddine, H.; Marabelle, A.; Champiat, S.; Berdelou, A.; et al. Safety profiles of anti-CTLA-4 and anti-PD-1 antibodies alone and in combination. Nat. Rev. Clin. Oncol. 2016, 13, 473–486. [Google Scholar] [CrossRef] [PubMed]
- Haanen, J.; Ernstoff, M.; Wang, Y.; Menzies, A.; Puzanov, I.; Grivas, P.; Larkin, J.; Peters, S.; Thompson, J.; Obeid, M. Rechallenge patients with immune checkpoint inhibitors following severe immune-related adverse events: Review of the literature and suggested prophylactic strategy. J. Immunother. Cancer 2020, 8, e000604. [Google Scholar] [CrossRef]
- Gobbini, E.; Charles, J.; Toffart, A.C.; Leccia, M.T.; Moro-Sibilot, D.; Levra, M.G. Literature meta-analysis about the efficacy of re-challenge with PD-1 and PD-L1 inhibitors in cancer patients. Bull. Cancer 2020, 107, 1098–1107. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total, n = 85, 100% | |
|---|---|
| Age (years) | |
| Median (range) | 72 (30–89) |
| Gender | |
| Male (%) | 47 (55) |
| Female (%) | 38 (45) |
| ECOG performance status | |
| 0/1 (%) | 81 (95) |
| ≥2 (%) | 4 (5) |
| Autoimmune disease | |
| No (%) | 79 (93) |
| Yes (%) | 6 (7) |
| Type of primary melanoma | |
| Cutaneous (%) | 70 (82) |
| Mucosal (%) | 6 (7) |
| Uveal (%) | 3 (4) |
| Unknown (%) | 6 (7) |
| Breslow index (mm) | |
| Median range | 3.3 (0.5–25) |
| Unknown | 17 (20) |
| Ulceration | |
| No (%) | 33 (39) |
| Yes (%) | 28 (33) |
| Unknown (%) | 24 (28) |
| Mutation | |
| BRAF V600 E/K (%) | 19 (22) |
| BRAF no V600 (%) | 1 (1) |
| NRAS (%) | 27 (32) |
| CKIT (%) | 3 (4) |
| GNAQ (%) | 1 (1) |
| Unknown (%) | 34 (40) |
| AJCC stage | |
| IIIC (%) | 7 (8) |
| IIID (%) | 3 (4) |
| IV (%) | 75 (88) |
| Number of metastatic sites | |
| 3 (%) | 48 (57) |
| >3 (%) | 37 (43) |
| Localization of metastasis | |
| Cutaneous (%) | 34 (40) |
| Lymph node (%) | 33 (39) |
| Lung (%) | 17 (20) |
| Liver (%) | 11 (13) |
| Brain (%) | 22 (26) |
| Other (%) | 14 (16) |
| Elevated LDH level | |
| No (%) | 55 (65) |
| Yes (%) | 11 (13) |
| Unknown (%) | 19 (22) |
| Treatment between the two ICI courses | |
| Surgery (%) | 8 (9) |
| Radiotherapy (%) | 10 (12) |
| Targeted therapy (%) | 6 (7) |
| Chemotherapy (%) | 6 (7) |
| Protocol (%) | 5 (6) |
| Second course of ICI (ICI rechallenge) | |
| Rechallenge (%) | 73 (86) |
| Escalation (%) | 4 (5) |
| Switch (%) | 8 (9) |
| Univarious Model | Multivarious Model | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Age (years) | 0.99 | 0.95, 1.022 | 0.462 | |||
| Gender | 0.665 | |||||
| Male | 1 | — | ||||
| Female | 1.210 | 0.512, 2.889 | ||||
| ECOG performance status (ICI rechallenge) | 0.828 | |||||
| 0/1 | 1 | — | ||||
| ≥2 | 0.800 | 0.092, 6.933 | ||||
| Type of primitive tumor | 0.461 | |||||
| Other | 1 | — | ||||
| Cutaneous | 1.524 | 0.494, 4.797 | ||||
| BRAFV600 mutation | 0.436 | |||||
| No | 1 | — | ||||
| Yes | 1.518 | 0.541, 4.533 | ||||
| Response to 1st ICI | 0.100 | |||||
| Complete response + Partial response | 1 | — | ||||
| Stable disease | 0.302 | 0.061, 1.178 | ||||
| Duration of 1st ICI (months) | 0.98 | 0.946, 1.022 | 0.403 | |||
| Time to relapse after 1st ICI (months) | 0.725 | |||||
| ≤6 months | 1 | — | ||||
| >6 months | 1.188 | 0.451, 3.120 | ||||
| Systemic treatment between the ICI courses | 0.020 | 0.035 | ||||
| No | 1 | — | 1 | — | ||
| Yes | 0.228 | 0.058, 0.742 | 0.249 | 0.061, 0.860 | ||
| Local treatment between the ICI courses | 0.980 | |||||
| No | 1 | — | ||||
| Yes | 1.014 | 0.356, 2.960 | ||||
| Number of metastatic sites (ICI rechallenge) | 0.521 | |||||
| ˃3 | 1 | — | ||||
| ≤3 | 1.326 | 0.559, 3.165 | ||||
| Brain metastasis (ICI rechallenge) | 0.283 | |||||
| No | 1 | — | ||||
| Yes | 0.586 | 0.216, 1.554 | ||||
| Elevated LDH level (ICI rechallenge) | 0.036 | 0.061 | ||||
| No | 1 | — | 1 | — | ||
| Yes | 0.440 | 0.113, 1.641 | 0.392 | 0.098, 1.505 | ||
| Unknown | 0.244 | 0.075, 0.718 | 0.278 | 0.083, 0.858 | ||
| Corticosteroids (ICI rechallenge) | 0.174 | |||||
| No | 1 | — | ||||
| Yes | 0.364 | 0.072, 1.486 | ||||
| Second course of ICI (ICI rechallenge) Rechallenge Escalation Switch | 1 0.825 1.375 | — 0.095, 7.179 0.314, 7.104 | 0.896 | |||
| Toxicity (ICI rechallenge) | 0.890 | |||||
| No | 1 | — | ||||
| Yes | 1.071 | 0.409, 2.859 | ||||
| Study | Number of Patients | 1st ICI Antibodies | Response to 1st ICI | ICI Antibodies for Rechallenge | Response to ICI Rechallenge | Median Survival (Months) |
|---|---|---|---|---|---|---|
| Keynote-006 [15] | 13 | PB | BORR 92% DCR 100% | PB | BORR 54% DCR 77% | NA |
| Keynote-001 [9] | 4 | PB | BORR 100% | PB | BORR 25% DCR 50% | NA |
| Betof Warner et al. (2019) [22] | 41 | Anti-PD1 * | BORR 68% DCR 100% | Anti-PD1 63% IPI + NIVO 37% | Anti PD1: BORR 12% DCR NA IPI + NIVO: BORR 33% DCR NA | NA |
| Jansen et al. (2019) [16] | 19 | Anti-PD1 (PB 90%, NIVO 10%) | BORR 79% DCR 100% | Anti-PD1 (PB 79%, NIVO 21%) | BORR 32% DCR 58% | NA |
| Whitman et al. (2020) [18] | 21 | Anti-PD1 | BORR 67% DCR 100% | Anti-PD1 | BORR 48% DCR 62% | PFS: 9.9 OS: 30 |
| Pokorny et al. (2021) [23] | 8 | Anti-PD1 (PB 92% NIVO 8%) | BORR 79% DCR 100% | Anti-PD1 | BORR 50% DCR 87.5% | NA |
| Asher et al. (2021) [17] | 21 | Anti-PD1 81% IPI + NIVO 19% | No PD (DCR = 100%) | Anti-PD1 90% IPI + NIVO 5% IPI 5% | BORR 47% DCR 68% | NA |
| Dutheil et al. (2021) [19] | 13 | NA | BORR 100% | NA | BORR 38% DCR 46% | NA |
| Van Zeijl et al. (2022) [20] | 27 | Anti-PD1 | BORR 69% DCR 100% | Anti-PD1 | BORR 30% DCR 63% | NA |
| Nardin et al. (2022) [24] | 85 | Anti-PD1 80% (PB 48, NIVO 32%) IPI + NIVO 8% IPI 12% | BORR 88% DCR 100% | Anti-PD1 (93%) (PB 52%, NIVO 41%) IPI + NIVO 5% IPI 2% | BORR 54% DCR 75% | 1-yOS: 78% PFS: 21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nardin, C.; Hennemann, A.; Diallo, K.; Funck-Brentano, E.; Puzenat, E.; Heidelberger, V.; Jeudy, G.; Samimi, M.; Lesage, C.; Boussemart, L.; et al. Efficacy of Immune Checkpoint Inhibitor (ICI) Rechallenge in Advanced Melanoma Patients’ Responders to a First Course of ICI: A Multicenter National Retrospective Study of the French Group of Skin Cancers (Groupe de Cancérologie Cutanée, GCC). Cancers 2023, 15, 3564. https://doi.org/10.3390/cancers15143564
Nardin C, Hennemann A, Diallo K, Funck-Brentano E, Puzenat E, Heidelberger V, Jeudy G, Samimi M, Lesage C, Boussemart L, et al. Efficacy of Immune Checkpoint Inhibitor (ICI) Rechallenge in Advanced Melanoma Patients’ Responders to a First Course of ICI: A Multicenter National Retrospective Study of the French Group of Skin Cancers (Groupe de Cancérologie Cutanée, GCC). Cancers. 2023; 15(14):3564. https://doi.org/10.3390/cancers15143564
Chicago/Turabian StyleNardin, Charlée, Aymeric Hennemann, Kadiatou Diallo, Elisa Funck-Brentano, Eve Puzenat, Valentine Heidelberger, Géraldine Jeudy, Mahtab Samimi, Candice Lesage, Lise Boussemart, and et al. 2023. "Efficacy of Immune Checkpoint Inhibitor (ICI) Rechallenge in Advanced Melanoma Patients’ Responders to a First Course of ICI: A Multicenter National Retrospective Study of the French Group of Skin Cancers (Groupe de Cancérologie Cutanée, GCC)" Cancers 15, no. 14: 3564. https://doi.org/10.3390/cancers15143564