
Contrast-Enhanced Imaging in the Management of Intrahepatic Cholangiocarcinoma: State of Art and Future Perspectives
 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
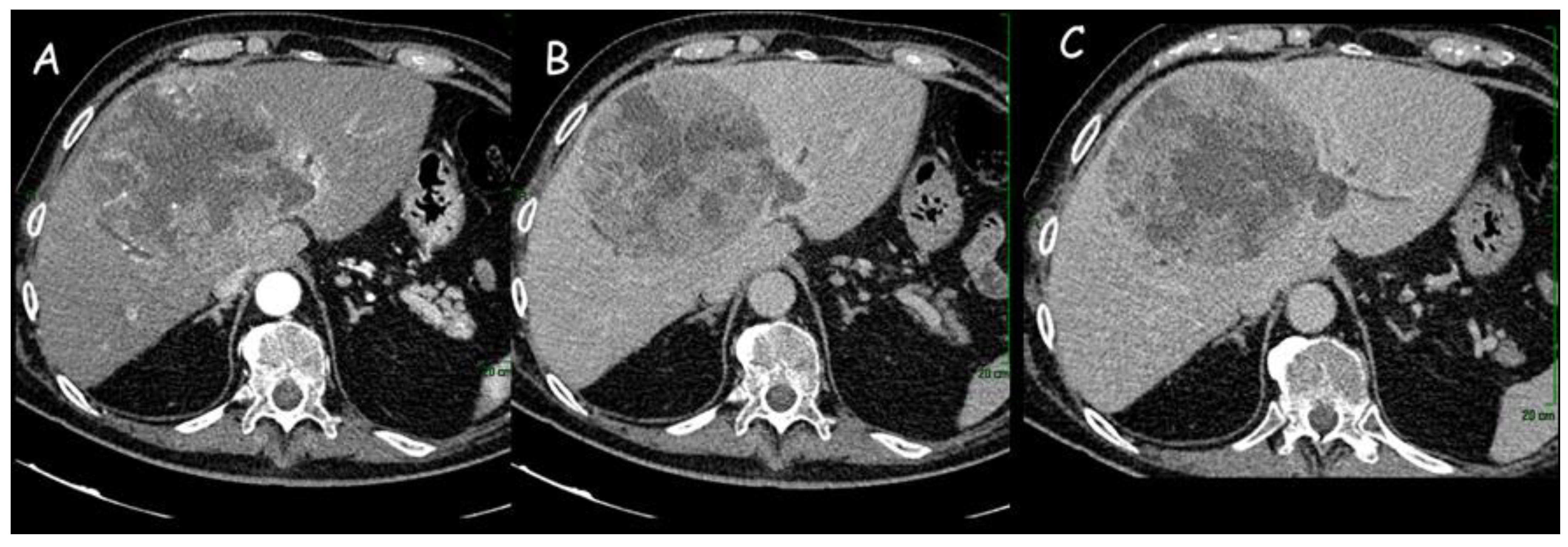
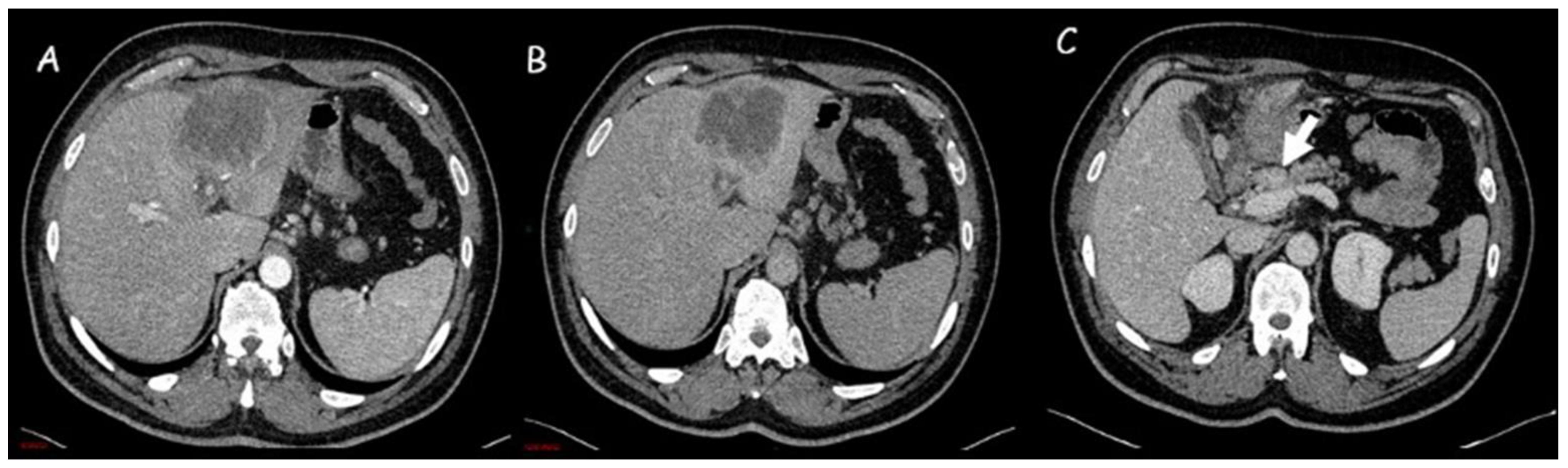
1.1. Computed Tomography
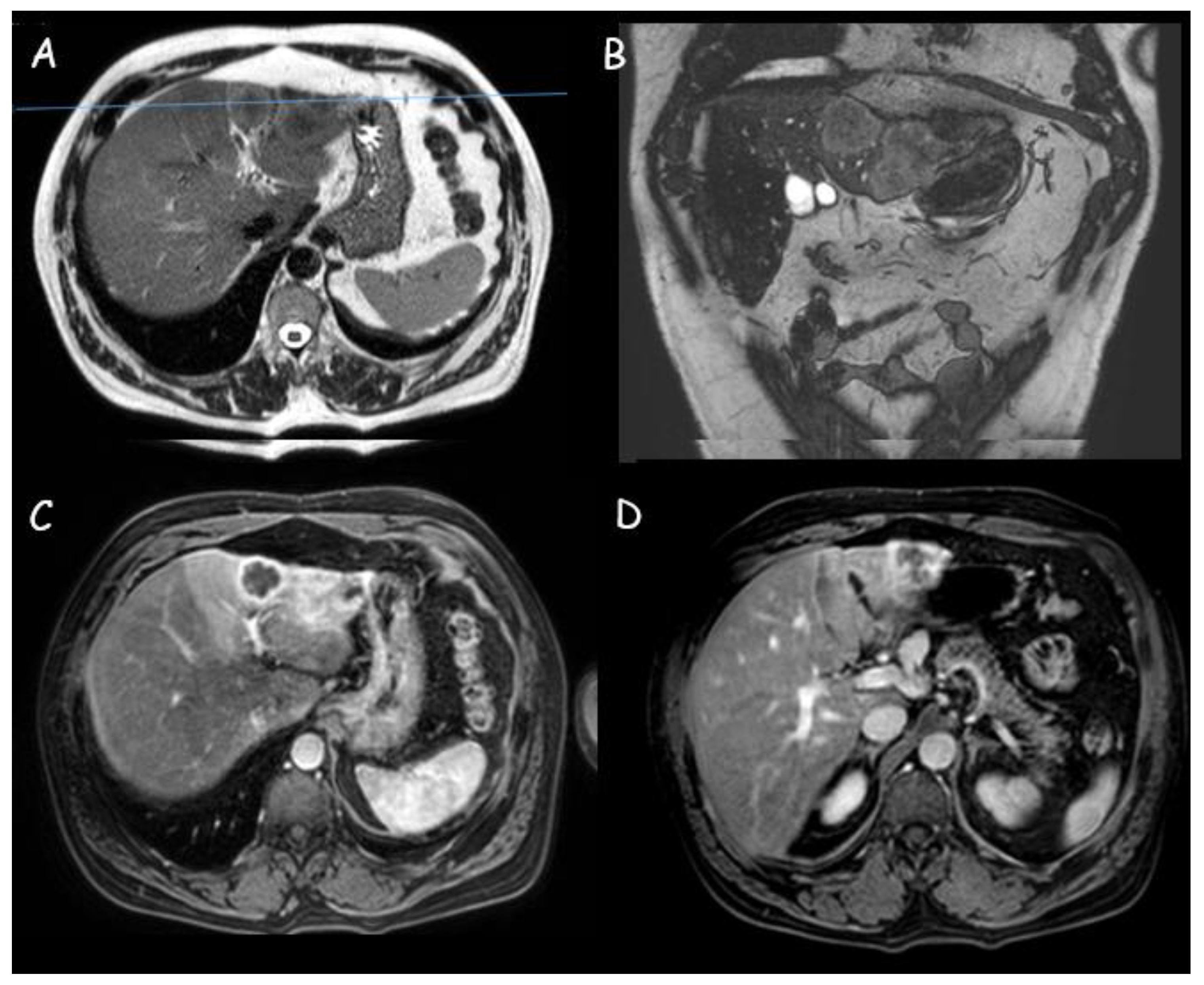
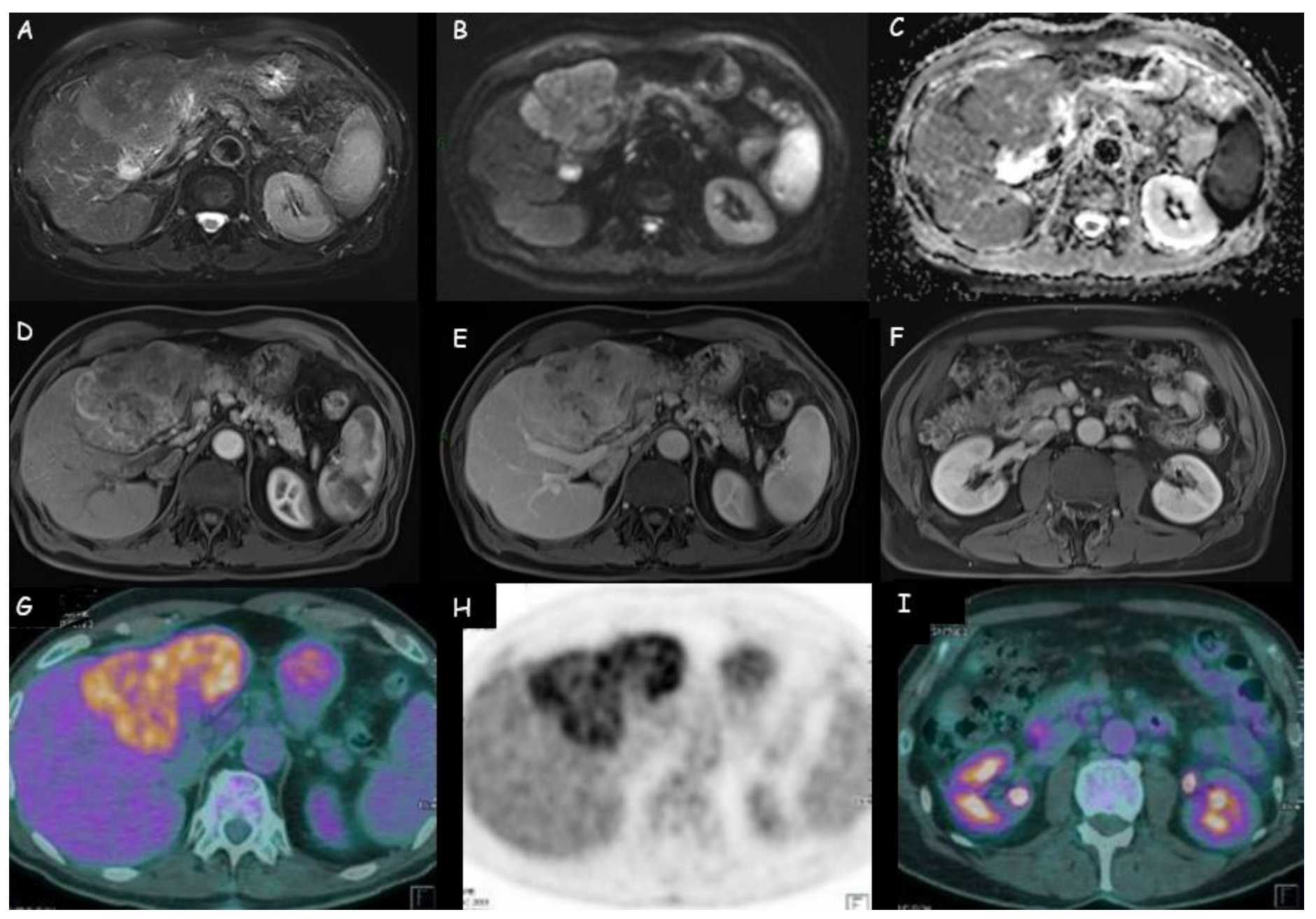
1.2. Magnetic Resonance Imaging
1.3. Positron Emission Tomography with Fluorodeoxyglucose
1.4. Contrast-Enhanced Ultrasound (CEUS)
1.5. Radiomics
2. Present Shadows and Future Perspectives

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Computed Tomography | Magnetic Resonance | Contrast-Enhanced Ultrasound |
|---|---|---|
|
|
|
| Number of Patients | Diagnostic Imaging | Primary iCCA | Metastatic Lymph Nodes | Distant Metastases | |
|---|---|---|---|---|---|
| Kim et al. [74] | 123 | 18FDG-PET/CT | Se = 84.0% Sp = 79.3% PPV = 92.9% NPV = 60.5% Accuracy = 82.9% | Accuracy = 75.9% | Accuracy = 88.3% |
| CT | - | Accuracy = 60.9% | Accuracy = 78.7% | ||
| Kim YY et al. [29] | 334 | MRI | Se = 91.0% (T1b), 89.1% (T2), 77.8% (T3 or T4) Sp = 53.9% (T1b), 39.8% (T2), 45.5% (T3 or T4) | Se = 65.4% Sp = 54.6% | Vascular invasion: Se = 73.8% Sp = 47.0% Visceral peritoneal invasion: Se = 77.2% Sp = 45.1% |
| CT | Se = 80.5% (T1b), 73.8% (T2), 58.0% (T3 or T4) Sp = 69.2% (T1b), 54.0% (T2), 63.2% (T3 or T4) | Se = 64.0% Sp = 36.4% | Vascular invasion: Se = 56.8% Sp = 60.3% Visceral peritoneal invasion: Se = 57.0% Sp = 62.38% | ||
| Park et al. [77] | 18 | CT | ND | Se = 20.0% Sp = 86.4% | ND |
| 18FDG-PET/CT | ND | Se = 80.0% Sp = 92.3% | ND | ||
| Lee et al. [114] | 99 | 18FDG-PET/CT | Se = 90.2% Sp = 70.6% PPV = 93.7% NPV = 60.0% Accuracy = 86.9% | PPV = 94.1% | Se = 94.7% |
| CT | Se = 84.2% Sp = 70.6% PPV = 93.2% NPV = 48.0% Accuracy = 81.8% | PPV = 77.5% | Se = 63.2% | ||
| Lin et al. [115] | 291 | PET-CT 18FDG-PET/CT | NA | Se = 83.0% Sp = 88.3% PPV = 81.6% NPV = 89.3% Accuracy = 86.3% | Se = 87.8% Sp = 95.4% PPV = 86.7% NPV = 95.8% Accuracy = 93.5% |
| Nishioka et al. [116] | 202 | CT | Se = 49% Sp = 100% PPV = 100% NPV = 75% Accuracy = 80% | Se = 40% Sp = 80% PPV = 63% NPV = 68% Accuracy = 67% | Macrovascular invasion: Se = 60% Sp = 89% PPV = 25% NPV = 97% Accuracy = 88% Bile duct invasion: Se = 17% Sp = 99% PPV = 25% NPV = 99% Accuracy = 93% |
| MRI | Se = 51% Sp = 97% PPV = 92% NPV = 76% Accuracy = 79% | Se = 56% Sp = 83% PPV = 74% NPV = 76% Accuracy = 76% | Macrovascular invasion: Se = 60% Sp = 94% PPV = 38% NPV = 98% Accuracy = 92% Bile duct invasion: Se = 50% Sp = 99% PPV = 50% NPV = 96% Accuracy = 93% | ||
| 18FDG-PET/CT | Se = 29% Sp = 100% PPV = 100% NPV = 71% Accuracy = 72% | Se = 84% Sp = 86% PPV = 91% NPV = 84% Accuracy = 86% | Macrovascular invasion: Se = 40% Sp = 98% PPV = 50% NPV = 97% Accuracy = 94% Bile duct invasion: Se = 17% Sp = 100% PPV = 94% NPV = 94% Accuracy = 93% | ||
| Petrowsky et al. [117] | 61 | CT | Se = 78% Sp = 80% PPV = 92% NPV = 57% Accuracy = 79% | Se = 24% Sp = 86% PPV = 50% NPV = 65% Accuracy = 62% | Se = 25% Sp = 100% PPV = 100% NPV = 84% Accuracy = 85% |
| PET-CT | Se = 93% Sp = 80% PPV = 93% NPV = 80% Accuracy = 89% | Se = 12% Sp = 96% PPV = 67% NPV = 64% Accuracy = 64% | Se = 100% Sp = 100% PPV = 100% NPV = 100% Accuracy = 100% | ||
| Vidili et al. [95] | 269 | CEUS (LiRADS-M) | Se = 91.3% SP = 96.7% PPV = 56.8% NPV = 96.5% Accuracy = 96.5% | NA | NA |
| Holzapfel et al. [67] | 24 | MRI (DWI + respiratory-triggered single-shot echo-planar imaging) | NA | Se = 83.3% Sp = 92.8% PPV = 66.7% NPV = 96.7% | NA |
| Lamarca et al. [73] | 198 | 18FDG-PET | Se = 37.5% Sp = 97.0% | Se = 37.5% Sp = 97.0% | NA |
3. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kelley, R.K.; Bridgewater, J.; Gores, G.J.; Zhu, A.X. Systemic therapies for intrahepatic cholangiocarcinoma. J. Hepatol. 2020, 72, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhi, H.; Gores, G.J. Cholangiocarcinoma: Modern advances in understanding a deadly old disease. J. Hepatol. 2006, 45, 856–867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vithayathil, M.; Khan, S.A. Current epidemiology of cholangiocarcinoma in Western countries. J. Hepatol. 2022, 77, 1690–1698. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Valery, P.C.; Laversanne, M.; Clark, P.J.; Petrick, J.L.; McGlynn, K.A.; Bray, F. Projections of primary liver cancer to 2030 in 30 countries worldwide. Hepatology 2018, 67, 600–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massarweh, N.N.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Cancer Control J. Moffitt Cancer Cent. 2017, 24, 1073274817729245. [Google Scholar] [CrossRef]
- Rizvi, S.; Khan, S.A.; Hallemeier, C.L.; Kelley, R.K.; Gores, G.J. Cholangiocarcinoma—Evolving concepts and therapeutic strategies. Nat. Rev. Clin. Oncol. 2018, 15, 95–111. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.M.; Parmar, A.D.; Geller, D.A. Intrahepatic Cholangiocarcinoma. Surg. Oncol. Clin. N. Am. 2014, 23, 231–246. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.J.; Chun, Y.S. Intrahepatic cholangiocarcinoma: The AJCC/UICC 8th edition updates. Chin. Clin. Oncol. 2018, 7, 52. [Google Scholar] [CrossRef]
- Hu, L.-S.; Zhang, X.-F.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Recurrence Patterns and Timing Courses Following Curative-Intent Resection for Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2019, 26, 2549–2557. [Google Scholar] [CrossRef]
- El-Diwany, R.; Pawlik, T.M.; Ejaz, A. Intrahepatic Cholangiocarcinoma. Surg. Oncol. Clin. N. Am. 2019, 28, 587–599. [Google Scholar] [CrossRef]
- Endo, I.; Gonen, M.; Yopp, A.C.; Dalal, K.M.; Zhou, Q.; Klimstra, D.; D’Angelica, M.; DeMatteo, R.P.; Fong, Y.; Schwartz, L.; et al. Intrahepatic Cholangiocarcinoma: Rising Frequency, Improved Survival, and Determinants of Outcome after Resection. Ann. Surg. 2008, 248, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.-H.; Chen, X.; Zhang, X.-H.; Zhang, E.-C.; Sun, C.-X. Clinicopathological characteristics and prognostic factors for intrahepatic cholangiocarcinoma: A population-based study. Sci. Rep. 2021, 11, 3990. [Google Scholar] [CrossRef] [PubMed]
- Mar, W.A.; Chan, H.K.; Trivedi, S.B.; Berggruen, S.M. Imaging of Intrahepatic Cholangiocarcinoma. Semin. Ultrasound CT MRI 2021, 42, 366–380. [Google Scholar] [CrossRef] [PubMed]
- Joo, I.; Lee, J.M.; Yoon, J.H. Imaging Diagnosis of Intrahepatic and Perihilar Cholangiocarcinoma: Recent Advances and Challenges. Radiology 2018, 288, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, I.S.; Kilcoyne, A.; Everett, J.M.; Mino-Kenudson, M.; Harisinghani, M.G.; Ganesan, K. Cholangiocarcinoma: Classification, diagnosis, staging, imaging features, and management. Abdom. Radiol. N. Y. 2017, 42, 1637–1649. [Google Scholar] [CrossRef]
- Alvaro, D.; Gores, G.J.; Walicki, J.; Hassan, C.; Sapisochin, G.; Komuta, M.; Forner, A.; Valle, J.W.; Laghi, A.; Ilyas, S.I.; et al. EASL-ILCA Clinical Practice Guidelines on the management of intrahepatic cholangiocarcinoma. J. Hepatol. 2023, 79, 181–208. [Google Scholar] [CrossRef]
- Kubo, S.; Shinkawa, H.; Asaoka, Y.; Ioka, T.; Igaki, H.; Izumi, N.; Itoi, T.; Unno, M.; Ohtsuka, M.; Okusaka, T.; et al. Liver Cancer Study Group of Japan Clinical Practice Guidelines for Intrahepatic Cholangiocarcinoma. Liver Cancer 2022, 11, 290–314. [Google Scholar] [CrossRef]
- Bowlus, C.L.; Arrivé, L.; Bergquist, A.; Deneau, M.; Forman, L.; Ilyas, S.I.; Lunsford, K.E.; Martinez, M.; Sapisochin, G.; Shroff, R.; et al. AASLD practice guidance on primary sclerosing cholangitis and cholangiocarcinoma. Hepatology 2023, 77, 659–702. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Imai, Y.; Murakami, T.; Nishikawa, M.; Kurokawa, M.; Yonezawa, T.; Tokunaga, K.; Fukushima, Y.; Wakasa, K.; Kim, T.; et al. Intrahepatic cholangiocarcinoma with marked hypervascularity. Abdom. Imaging 1999, 24, 66–68. [Google Scholar] [CrossRef]
- Kim, S.W.; Lee, J.M.; Han, J.K.; Kim, K.H.; Lee, J.Y.; Choi, B.I. Peripheral Mass–Forming Cholangiocarcinoma in Cirrhotic Liver. Am. J. Roentgenol. 2007, 189, 1428–1434. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Chen, B.; Zhan, C.; Yu, H.; Zheng, J.; Bao, W.; Deng, T.; Zheng, C.; Wu, L.; Yang, Y.; et al. A Novel Clinical-Radiomics Model Based on Sarcopenia and Radiomics for Predicting the Prognosis of Intrahepatic Cholangiocarcinoma After Radical Hepatectomy. Front. Oncol. 2021, 11, 744311. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.A.; Lee, J.M.; Lee, K.B.; Kim, S.H.; Yoon, S.H.; Han, J.K.; Choi, B.I. Intrahepatic Mass-forming Cholangiocarcinomas: Enhancement Patterns at Multiphasic CT, with Special Emphasis on Arterial Enhancement Pattern—Correlation with Clinicopathologic Findings. Radiology 2011, 260, 148–157. [Google Scholar] [CrossRef] [Green Version]
- Brown, Z.J.; Hewitt, D.B.; Pawlik, T.M. Biomarkers of intrahepatic cholangiocarcinoma: Diagnosis and response to therapy. Front. Biosci. Landmark Ed. 2022, 27, 85. [Google Scholar] [CrossRef] [PubMed]
- Iavarone, M.; Piscaglia, F.; Vavassori, S.; Galassi, M.; Sangiovanni, A.; Venerandi, L.; Forzenigo, L.V.; Golfieri, R.; Bolondi, L.; Colombo, M. Contrast enhanced CT-scan to diagnose intrahepatic cholangiocarcinoma in patients with cirrhosis. J. Hepatol. 2013, 58, 1188–1193. [Google Scholar] [CrossRef]
- Zhang, H.; Yang, T.; Wu, M.; Shen, F. Intrahepatic cholangiocarcinoma: Epidemiology, risk factors, diagnosis and surgical management. Cancer Lett. 2016, 379, 198–205. [Google Scholar] [CrossRef]
- Lee, H.Y.; Kim, S.H.; Lee, J.M.; Kim, S.-W.; Jang, J.-Y.; Han, J.K.; Choi, B.I. Preoperative Assessment of Resectability of Hepatic Hilar Cholangiocarcinoma: Combined CT and Cholangiography with Revised Criteria. Radiology 2006, 239, 113–121. [Google Scholar] [CrossRef]
- Aloia, T.A.; Charnsangavej, C.; Faria, S.; Ribero, D.; Abdalla, E.K.; Vauthey, J.N.; Curley, S.A. High-resolution computed tomography accurately predicts resectability in hilar cholangiocarcinoma. Am. J. Surg. 2007, 193, 702–706. [Google Scholar] [CrossRef]
- Kim, Y.; Yeom, S.; Shin, H.; Choi, S.H.; Rhee, H.; Park, J.H.; Cho, E.; Park, S.; Lee, S.S.; Park, M. Clinical Staging of Mass-Forming Intrahepatic Cholangiocarcinoma: Computed Tomography Versus Magnetic Resonance Imaging. Hepatol. Commun. 2021, 5, 2009–2018. [Google Scholar] [CrossRef]
- Park, H.M.; Jang, H.Y.; Lee, D.E.; Kang, M.J.; Han, S.-S.; Kim, S.-W.; Park, S.-J. Prognostic impact of tumor vascularity on CT in resectable intrahepatic cholangiocarcinoma. HPB 2022, 24, 359–369. [Google Scholar] [CrossRef]
- Zhang, Y.; Uchida, M.; Abe, T.; Nishimura, H.; Hayabuchi, N.; Nakashima, Y. Intrahepatic Peripheral Cholangiocarcinoma: Comparison of Dynamic CT and Dynamic MRI. J. Comput. Assist. Tomogr. 1999, 23, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Péporté, A.R.; Sommer, W.H.; Nikolaou, K.; Reiser, M.F.; Zech, C.J. Imaging features of intrahepatic cholangiocarcinoma in Gd-EOB-DTPA-enhanced MRI. Eur. J. Radiol. 2013, 82, e101–e106. [Google Scholar] [CrossRef]
- Kim, M.-J.; Choi, J.-Y.; Chung, Y.E. Evaluation of Biliary Malignancies Using Multidetector-Row Computed Tomography. J. Comput. Assist. Tomogr. 2010, 34, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Engelbrecht, M.R.; Katz, S.S.; van Gulik, T.M.; Laméris, J.S.; van Delden, O.M. Imaging of Perihilar Cholangiocarcinoma. Am. J. Roentgenol. 2015, 204, 782–791. [Google Scholar] [CrossRef]
- Kim, N.H.; Lee, S.R.; Kim, Y.H.; Kim, H.J. Diagnostic Performance and Prognostic Relevance of FDG Positron Emission Tomography/Computed Tomography for Patients with Extrahepatic Cholangiocarcinoma. Korean J. Radiol. 2020, 21, 1355–1366. [Google Scholar] [CrossRef]
- Noji, T.; Kondo, S.; Hirano, S.; Tanaka, E.; Ambo, Y.; Kawarada, Y.; Morikawa, T. CT evaluation of paraaortic lymph node metastasis in patients with biliary cancer. J. Gastroenterol. 2005, 40, 739–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartsch, F.; Hahn, F.; Müller, L.; Baumgart, J.; Hoppe-Lotichius, M.; Kloeckner, R.; Lang, H. Relevance of suspicious lymph nodes in preoperative imaging for resectability, recurrence and survival of intrahepatic cholangiocarcinoma. BMC Surg. 2020, 20, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Y.; Mao, Y.; Chen, J.; Qiu, Y.; Wang, Z.; He, J. Preoperative Computed Tomography Features of Intrahepatic Cholangiocarcinoma for Predicting Lymph Node Metastasis and Overall Survival. J. Comput. Assist. Tomogr. 2019, 43, 729–735. [Google Scholar] [CrossRef]
- Meng, Z.-W.; Lin, X.-Q.; Zhu, J.-H.; Han, S.-H.; Chen, Y.-L. A nomogram to predict lymph node metastasis before resection in intrahepatic cholangiocarcinoma. J. Surg. Res. 2018, 226, 56–63. [Google Scholar] [CrossRef]
- Wakiya, T.; Ishido, K.; Kimura, N.; Nagase, H.; Kanda, T.; Ichiyama, S.; Soma, K.; Matsuzaka, M.; Sasaki, Y.; Kubota, S.; et al. CT-based deep learning enables early postoperative recurrence prediction for intrahepatic cholangiocarcinoma. Sci. Rep. 2022, 12, 8428. [Google Scholar] [CrossRef]
- Jiao, C.Y.; Zhang, H.; Ji, G.W.; Xu, Q.; Lu, M.; Zhang, B.; Yang, Y.; Wang, X.H.; Li, X.C. CT-based clinico-radiological nomograms for prognosis prediction in patients with intrahepatic mass-forming cholangiocarcinoma: A multi-institutional study. Eur. Radiol. 2022, 32, 8326–8338. [Google Scholar] [CrossRef] [PubMed]
- Esnaola, N.F.; Meyer, J.E.; Karachristos, A.; Maranki, J.L.; Camp, E.R.; Denlinger, C.S. Evaluation and management of intrahepatic and extrahepatic cholangiocarcinoma. Cancer 2016, 122, 1349–1369. [Google Scholar] [CrossRef] [Green Version]
- Mar, W.A.; Shon, A.M.; Lu, Y.; Yu, J.H.; Berggruen, S.M.; Guzman, G.; Ray, C.E., Jr.; Miller, F. Imaging spectrum of cholangiocarcinoma: Role in diagnosis, staging, and posttreatment evaluation. Abdom. Radiol. N. Y. 2016, 41, 553–567. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Kim, S.H.; Jang, K.M.; Choi, S.-Y.; Lee, S.J.; Choi, D. The role of diffusion-weighted MR imaging for differentiating benign from malignant bile duct strictures. Eur. Radiol. 2014, 24, 947–958. [Google Scholar] [CrossRef] [PubMed]
- Murakami, T.; Nakamura, H.; Tsuda, K.; Ishida, T.; Tomoda, K.; Hori, S.; Monden, M.; Kanai, T.; Wakasa, K.; Sakurai, M.; et al. Contrast-enhanced MR imaging of intrahepatic cholangiocarcinoma: Pathologic correlation study. J. Magn. Reson. Imaging 1995, 5, 165–170. [Google Scholar] [CrossRef]
- Ciresa, M.; De Gaetano, A.M.; Pompili, M.; Saviano, A.; Infante, A.; Montagna, M.; Guerra, A.; Giuga, M.; Vellone, M.; Ardito, F.; et al. Enhancement patterns of intrahepatic mass-forming cholangiocarcinoma at multiphasic computed tomography and magnetic resonance imaging and correlation with clinicopathologic features. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2786–2797. [Google Scholar]
- Koh, J.; Chung, Y.E.; Nahm, J.H.; Kim, H.Y.; Kim, K.-S.; Park, Y.N.; Kim, M.-J.; Choi, J.-Y. Intrahepatic mass-forming cholangiocarcinoma: Prognostic value of preoperative gadoxetic acid-enhanced MRI. Eur. Radiol. 2016, 26, 407–416. [Google Scholar] [CrossRef]
- Kajiyama, K.M.; Maeda, T.M.; Takenaka, K.M.; Sugimachi, K.M.; Tsuneyoshi, M.M. The Significance of Stromal Desmoplasia in Intrahepatic Cholangiocarcinoma: A Special Reference of “scirrhous-Type” and “Nonscirrhous-Type” Growth. Am. J. Surg. Pathol. 1999, 23, 892–902. [Google Scholar] [CrossRef]
- Kang, Y.; Lee, J.M.; Kim, S.H.; Han, J.K.; Choi, B.I. Intrahepatic Mass-forming Cholangiocarcinoma: Enhancement Patterns on Gadoxetic Acid–enhanced MR Images. Radiology 2012, 264, 751–760. [Google Scholar] [CrossRef]
- Mamone, G.; Marrone, G.; Caruso, S.; Carollo, V.; Gentile, G.; Crino’, F.; Milazzo, M.; Gianluca, M. Intrahepatic mass-forming cholangiocarcinoma: Enhancement pattern on Gd-BOPTA-MRI with emphasis of hepatobiliary phase. Abdom. Imaging 2015, 40, 2313–2322. [Google Scholar] [CrossRef]
- Xing, L.-H.; Zhuo, L.-Y.; Wang, J.-N.; Zhang, Y.; Zhu, F.-Y.; Wang, C.; Yin, X.-P.; Gao, B.-L. Values of MRI Imaging Presentations in the Hepatobiliary Phase, DWI and T2WI Sequences in Predicting Pathological Grades of Intrahepatic Mass-Forming Cholangiocarcinoma. Front. Oncol. 2022, 12, 867702. [Google Scholar] [CrossRef] [PubMed]
- Asayama, Y.; Nishie, A.; Ishigami, K.; Ushijima, Y.; Takayama, Y.; Fujita, N.; Kubo, Y.; Aishima, S.; Shirabe, K.; Yoshiura, T.; et al. Distinguishing intrahepatic cholangiocarcinoma from poorly differentiated hepatocellular carcinoma using precontrast and gadoxetic acid-enhanced MRI. Diagn. Interv. Radiol. Ank. Turk. 2015, 21, 96–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.; Liang, Y.; Wang, Z.; Tan, C.; Yang, R.; Wei, X.; Jiang, X. Optimizing CT and MRI criteria for differentiating intrahepatic mass-forming cholangiocarcinoma and hepatocellular carcinoma. Acta Radiol. Stockh. Swed. 1987 2023, 64, 926–935. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Liu, L.; Fang, J.; Rao, S.; Lv, L.; Zeng, M.; Shi, Y.; Yang, C. MRI features predict microvascular invasion in intrahepatic cholangiocarcinoma. Cancer Imaging Off. Publ. Int. Cancer Imaging Soc. 2020, 20, 40. [Google Scholar] [CrossRef] [PubMed]
- Min, J.H.; Kim, Y.K.; Choi, S.-Y.; Kang, T.W.; Lee, S.J.; Kim, J.M.; Ahn, S.; Cho, H. Intrahepatic Mass-forming Cholangiocarcinoma: Arterial Enhancement Patterns at MRI and Prognosis. Radiology 2019, 290, 691–699. [Google Scholar] [CrossRef]
- Jin, K.-P.; Sheng, R.-F.; Yang, C.; Zeng, M.-S. Combined arterial and delayed enhancement patterns of MRI assist in prognostic prediction for intrahepatic mass-forming cholangiocarcinoma (IMCC). Abdom. Radiol. N. Y. 2022, 47, 640–650. [Google Scholar] [CrossRef]
- Huang, X.; Yang, J.; Li, J.; Xiong, Y. Comparison of magnetic resonance imaging and 18-fludeoxyglucose positron emission tomography/computed tomography in the diagnostic accuracy of staging in patients with cholangiocarcinoma: A Meta-Analysis. Medicine 2020, 99, e20932. [Google Scholar] [CrossRef]
- Sheng, R.; Huang, X.; Jin, K.; Gao, S.; Zeng, M.; Wu, D.; Shi, G. Contrast-enhanced MRI could predict response of systemic therapy in advanced intrahepatic cholangiocarcinoma. Eur. Radiol. 2022, 32, 5156–5165. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2021, 76, 681–693. [Google Scholar] [CrossRef]
- Choi, S.-Y.; Kim, Y.K.; Min, J.H.; Kang, T.W.; Jeong, W.K.; Ahn, S.; Won, H. Added value of ancillary imaging features for differentiating scirrhous hepatocellular carcinoma from intrahepatic cholangiocarcinoma on gadoxetic acid-enhanced MR imaging. Eur. Radiol. 2018, 28, 2549–2560. [Google Scholar] [CrossRef]
- Xing, L.-H.; Zhuo, L.-Y.; Zhang, Y.; Ma, X.; Ma, Z.-P.; Zhao, Y.-J.; Yin, X.-P.; Gao, B.-L. DWI Combined With Hepatobiliary-Phase Enhanced Imaging Can Better Differentiate Cholangiocarcinoma From Atypical Liver Abscesses. Front. Oncol. 2022, 12, 723089. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Tan, H.; Panje, C.M.; Yu, H.; Xiu, Y.; Shi, H. Role of 18F-FDG PET/CT Imaging in Intrahepatic Cholangiocarcinoma. Clin. Nucl. Med. 2016, 41, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.B.; Liao, J.; Xie, R.; Chen, G.L.; Chen, G. Discrimination of metastatic from hyperplastic pelvic lymph nodes in patients with cervical cancer by diffusion-weighted magnetic resonance imaging. Abdom. Imaging 2011, 36, 102–109. [Google Scholar] [CrossRef]
- Klerkx, W.M.; Mali, W.M.; Heintz, A.P.; de Kort, G.A.; Takahara, T.; Peeters, P.H. Observer variation of magnetic resonance imaging and diffusion weighted imaging in pelvic lymph node detection. Eur. J. Radiol. 2011, 78, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Takashima, S.; Takayama, F.; Kawakami, S.; Saito, A.; Matsushita, T.; Momose, M.; Ishiyama, T. Head and Neck Lesions: Characterization with Diffusion-weighted Echo-planar MR Imaging. Radiology 2001, 220, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Promsorn, J.; Eurboonyanun, K.; Chadbunchachai, P.; Apivatanasiri, C.; Wirasorn, K.; Chindaprasirt, J.; Sookprasert, A.; Harisinghani, M. Diffusion-weighted imaging as an imaging biomarker for assessing survival of patients with intrahepatic mass-forming cholangiocarcinoma. Abdom. Radiol. N. Y. 2022, 47, 2811–2821. [Google Scholar] [CrossRef]
- Holzapfel, K.; Gaa, J.; Schubert, E.C.; Eiber, M.; Kleeff, J.; Rummeny, E.J.; Loos, M. Value of diffusion-weighted MR imaging in the diagnosis of lymph node metastases in patients with cholangiocarcinoma. Abdom. Radiol. N. Y. 2016, 41, 1937–1941. [Google Scholar] [CrossRef]
- Promsorn, J.; Soontrapa, W.; Somsap, K.; Chamadol, N.; Limpawattana, P.; Harisinghani, M. Evaluation of the diagnostic performance of apparent diffusion coefficient (ADC) values on diffusion-weighted magnetic resonance imaging (DWI) in differentiating between benign and metastatic lymph nodes in cases of cholangiocarcinoma. Abdom. Radiol. N. Y. 2019, 44, 473–481. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, Z.; Zhao, J.; Liu, S.; Zhang, X.; Yuan, F.; Shi, Y.; Song, B. Intrahepatic cholangiocarcinoma: MRI texture signature as predictive biomarkers of immunophenotyping and survival. Eur. Radiol. 2021, 31, 3661–3672. [Google Scholar] [CrossRef]
- Renzulli, M.; Brandi, N.; Brocchi, S.; Balacchi, C.; Lanza, C.; Pettinari, I.; Stefanini, B.; Carrafiello, G.; Piscaglia, F.; Golfieri, R.; et al. Association between anatomic variations of extrahepatic and intrahepatic bile ducts: Do look up! J. Anat. 2023, 242, 683–694. [Google Scholar] [CrossRef]
- Jadvar, H.; Henderson, R.W.; Conti, P.S. [F-18]Fluorodeoxyglucose Positron Emission Tomography and Positron Emission Tomography: Computed Tomography in Recurrent and Metastatic Cholangiocarcinoma. J. Comput. Assist. Tomogr. 2007, 31, 223–228. [Google Scholar] [CrossRef]
- Songthamwat, M.; Chamadol, N.; Khuntikeo, N.; Thinkhamrop, J.; Koonmee, S.; Chaichaya, N.; Bethony, J.; Thinkhamrop, B. Evaluating a preoperative protocol that includes magnetic resonance imaging for lymph node metastasis in the Cholangiocarcinoma Screening and Care Program (CASCAP) in Thailand. World J. Surg. Oncol. 2017, 15, 176. [Google Scholar] [CrossRef] [Green Version]
- Lamarca, A.; Barriuso, J.; Chander, A.; McNamara, M.G.; Hubner, R.A.; Óreilly, D.; Manoharan, P.; Valle, J.W. 18F-fluorodeoxyglucose positron emission tomography (18FDG-PET) for patients with biliary tract cancer: Systematic review and meta-analysis. J. Hepatol. 2019, 71, 115–129. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Kim, M.-H.; Lee, T.Y.; Hwang, C.Y.; Kim, J.S.; Yun, S.-C.; Lee, S.S.; Seo, D.W.; Lee, S.K. Clinical Role of18F-FDG PET-CT in Suspected and Potentially Operable Cholangiocarcinoma: A Prospective Study Compared with Conventional Imaging. Am. J. Gastroenterol. 2008, 103, 1145–1151. [Google Scholar] [CrossRef]
- Lee, Y.; Yoo, I.R.; Boo, S.H.; Kim, H.; Park, H.L.; Hyun O, J. The Role of F-18 FDG PET/CT in Intrahepatic Cholangiocarcinoma. Nucl. Med. Mol. Imaging 2017, 51, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Mavros, M.N.; Economopoulos, K.P.; Alexiou, V.G.; Pawlik, T.M. Treatment and Prognosis for Patients with Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-Analysis. JAMA Surg. 2014, 149, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Park, T.G.; Yu, Y.-D.; Park, B.J.; Cheon, G.J.; Oh, S.Y.; Kim, D.-S.; Choe, J.-G. Implication of Lymph Node Metastasis Detected on 18F-FDG PET/CT for Surgical Planning in Patients with Peripheral Intrahepatic Cholangiocarcinoma. Clin. Nucl. Med. 2014, 39, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.R.; Burns, P.N.; Kono, Y. Contrast-Enhanced Ultrasound of Focal Liver Masses: A Success Story. Ultrasound Med. Biol. 2020, 46, 1059–1070. [Google Scholar] [CrossRef]
- Faccioli, N.; D’Onofrio, M.; Comai, A.; Cugini, C. Contrast-enhanced ultrasonography in the characterization of benign focal liver lesions: Activity-based cost analysis. Radiol. Med. 2007, 112, 810–820. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Nolsøe, C.P.; Barr, R.G.; Berzigotti, A.; Burns, P.N.; Cantisani, V.; Chammas, M.C.; Chaubal, N.; Choi, B.I.; Clevert, D.-A.; et al. Guidelines and Good Clinical Practice Recommendations for Contrast-Enhanced Ultrasound (CEUS) in the Liver–Update 2020 WFUMB in Cooperation with EFSUMB, AFSUMB, AIUM, and FLAUS. Ultrasound Med. Biol. 2020, 46, 2579–2604. [Google Scholar] [CrossRef] [PubMed]
- Galassi, M.; Iavarone, M.; Rossi, S.; Bota, S.; Vavassori, S.; Rosa, L.; Leoni, S.; Venerandi, L.; Marinelli, S.; Sangiovanni, A.; et al. Patterns of appearance and risk of misdiagnosis of intrahepatic cholangiocarcinoma in cirrhosis at contrast enhanced ultrasound. Liver Int. Off. J. Int. Assoc. Study Liver 2013, 33, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.X.; Li, R.; Zhang, X.H.; Tang, C.L.; Guo, Y.L.; Guo, D.Y.; Luo, M.K. Factors Affecting the Enhancement Patterns of Intrahepatic Cholangiocarcinoma (ICC) on Contrast-Enhanced Ultrasound (CEUS) and their Pathological Correlations in Patients with a Single Lesion. Ultraschall Med. Stuttg. Ger. 1980 2016, 37, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Li, R.; Zhang, Y.; Yang, L.; Zhang, X.; Tang, C.; Guo, D. Enhancement Patterns of Intrahepatic Cholangiocarcinoma on Contrast-Enhanced Ultrasound: Correlation with Clinicopathologic Findings and Prognosis. Ultrasound Med. Biol. 2019, 45, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Xue, L.-Y.; Wang, W.-P.; Huang, B.-J.; Li, C.-X. Dynamic enhancement pattern of intrahepatic cholangiocarcinoma on contrast-enhanced ultrasound: The correlation with cirrhosis and tumor size. Abdom. Imaging 2015, 40, 1558–1566. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.C.; Jang, H.-J.; Kim, T.K. Characterization of Indeterminate Liver Lesions on CT and MRI With Contrast-Enhanced Ultrasound: What Is the Evidence? Am. J. Roentgenol. 2020, 214, 1295–1304. [Google Scholar] [CrossRef]
- Wildner, D.; Pfeifer, L.; Goertz, R.S.; Bernatik, T.; Sturm, J.; Neurath, M.F.; Strobel, D. Dynamic Contrast-Enhanced Ultrasound (DCE-US) for the Characterization of Hepatocellular Carcinoma and Cholangiocellular Carcinoma. Ultraschall Med. Stuttg. Ger. 1980 2014, 35, 522–527. [Google Scholar] [CrossRef]
- Chen, Y.; Zhu, Y.; Chen, K.; Wang, H.; Zhang, W.; Bao, J.; Wang, W. Differentiation between hepatocellular carcinoma and intrahepatic cholangiocarcinoma using contrast-enhanced ultrasound: A systematic review and meta-analysis. Clin. Hemorheol. Microcirc. 2021, 79, 293–309. [Google Scholar] [CrossRef]
- Shin, S.K.; Choi, D.J.; Kim, J.H.; Kim, Y.S.; Kwon, O.S. Characteristics of contrast-enhanced ultrasound in distinguishing small (≤3 cm) hepatocellular carcinoma from intrahepatic cholangiocarcinoma. Medicine 2018, 97, e12781. [Google Scholar] [CrossRef]
- Xu, H.-X.; Chen, L.-D.; Liu, L.-N.; Zhang, Y.-F.; Guo, L.-H.; Liu, C. Contrast-enhanced ultrasound of intrahepatic cholangiocarcinoma: Correlation with pathological examination. Br. J. Radiol. 2012, 85, 1029–1037. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.; Chang, X.; Lv, K.; Wang, Y.; Fu, X.; Tan, L.; Gui, Y.; Zhou, T.; Chen, X.; Jiang, Y. Contrast-enhanced Ultrasound Features of Intrahepatic Cholangiocarcinoma: A New Perspective. Sci. Rep. 2019, 9, 19363. [Google Scholar] [CrossRef] [Green Version]
- Piscaglia, F.; Wilson, S.R.; Lyshchik, A.; Cosgrove, D.; Dietrich, C.F.; Jang, H.-J.; Kim, T.K.; Salvatore, V.; Willmann, J.K.; Sirlin, C.B.; et al. American College of Radiology Contrast Enhanced Ultrasound Liver Imaging Reporting and Data System (CEUS LI-RADS) for the diagnosis of Hepatocellular Carcinoma: A pictorial essay. Ultraschall Med. Stuttg. Ger. 1980 2017, 38, 320–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Zhang, X.; Ma, K.-S.; Li, X.-W.; Xia, F.; Zhong, H.; Tang, C.-L.; Guo, Y.; Yan, X.-C. Dynamic enhancing vascular pattern of intrahepatic peripheral cholangiocarcinoma on contrast-enhanced ultrasound: The influence of chronic hepatitis and cirrhosis. Abdom. Imaging 2013, 38, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.-J.; Wang, W.; Lu, M.-D.; Xie, X.-Y.; Xu, H.-X.; Xu, Z.-F.; Chen, L.-D.; Wang, Z.; Liang, J.-Y.; Huang, Y.; et al. Contrast-Enhanced Ultrasound for the Characterization of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Liver Cancer 2015, 4, 241–252. [Google Scholar] [CrossRef]
- Huang, J.-Y.; Li, J.-W.; Ling, W.-W.; Li, T.; Luo, Y.; Liu, J.-B.; Lu, Q. Can contrast enhanced ultrasound differentiate intrahepatic cholangiocarcinoma from hepatocellular carcinoma? World J. Gastroenterol. 2020, 26, 3938–3947. [Google Scholar] [CrossRef] [PubMed]
- Vidili, G.; Arru, M.; Solinas, G.; Calvisi, D.F.; Meloni, P.; Sauchella, A.; Turilli, D.; Fabio, C.; Cossu, A.; Madeddu, G.; et al. Contrast-enhanced ultrasound Liver Imaging Reporting and Data System: Lights and shadows in hepatocellular carcinoma and cholangiocellular carcinoma diagnosis. World J. Gastroenterol. 2022, 28, 3488–3502. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Li, Q.; Liu, Y.; Han, J.; Zheng, W.; Huang, Y.; Zheng, X.; Cao, L.; Zhou, J.-H. Distinguishing intrahepatic cholangiocarcinoma from hepatocellular carcinoma in patients with and without risks: The evaluation of the LR-M criteria of contrast-enhanced ultrasound liver imaging reporting and data system version 2017. Eur. Radiol. 2020, 30, 461–470. [Google Scholar] [CrossRef]
- Wildner, D.; Bernatik, T.; Greis, C.; Seitz, K.; Neurath, M.F.; Strobel, D. CEUS in Hepatocellular Carcinoma and Intrahepatic Cholangiocellular Carcinoma in 320 Patients—Early or Late Washout Matters: A Subanalysis of the DEGUM Multicenter Trial. Ultraschall Med. Stuttg. Ger. 1980 2015, 36, 132–139. [Google Scholar] [CrossRef]
- Chen, L.-D.; Ruan, S.; Liang, J.-Y.; Yang, Z.; Shen, S.-L.; Huang, Y.; Li, W.; Wang, Z.; Xie, X.-Y.; Lu, M.-D.; et al. Differentiation of intrahepatic cholangiocarcinoma from hepatocellular carcinoma in high-risk patients: A predictive model using contrast-enhanced ultrasound. World J. Gastroenterol. 2018, 24, 3786–3798. [Google Scholar] [CrossRef]
- Guo, H.; Zheng, X.; Cheng, M.; Zeng, D.; Huang, H.; Xie, X.; Lu, M.; Kuang, M.; Wang, W.; Xian, M.; et al. Contrast-Enhanced Ultrasound for Differentiation Between Poorly Differentiated Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2022, 41, 1213–1225. [Google Scholar] [CrossRef]
- Zeng, D.; Xu, M.; Liang, J.-Y.; Cheng, M.-Q.; Huang, H.; Pan, J.-M.; Huang, Y.; Tong, W.-J.; Xie, X.-Y.; Lu, M.-D.; et al. Using new criteria to improve the differentiation between HCC and non-HCC malignancies: Clinical practice and discussion in CEUS LI-RADS 2017. Radiol. Med. 2022, 127, 1–10. [Google Scholar] [CrossRef]
- Wang, X.; Liang, P.; Yu, J.; Yao, J.-D.; Fan, F.-Y.; Yu, X.; Cheng, Z.-G.; Han, Z.-Y.; Liu, F.-Y.; Dou, J.-P. Contrast-enhanced ultrasound features predict the prognosis of percutaneous microwave ablation of intrahepatic cholangiocarcinoma. Br. J. Radiol. 2022, 95, 20211379. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Belli, A.; Borzillo, V.; Palumbo, P.; Bruno, F.; Grassi, R.; Ottaiano, A.; Nasti, G.; Pilone, V.; et al. Correction: Conventional, functional and radiomics assessment for intrahepatic cholangiocarcinoma. Infect. Agents Cancer 2022, 17, 22. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Yang, Z.; Zhang, H.; Huang, G.; Li, Q.; Ning, P.; Yu, H. Personalized intrahepatic cholangiocarcinoma prognosis prediction using radiomics: Application and development trend. Front. Oncol. 2023, 13, 1133867. [Google Scholar] [CrossRef]
- Ji, G.-W.; Zhu, F.-P.; Zhang, Y.-D.; Liu, X.-S.; Wu, F.-Y.; Wang, K.; Xia, Y.-X.; Zhang, Y.-D.; Jiang, W.-J.; Li, X.-C.; et al. A radiomics approach to predict lymph node metastasis and clinical outcome of intrahepatic cholangiocarcinoma. Eur. Radiol. 2019, 29, 3725–3735. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Park, B.; Park, S.Y.; Choi, S.H.; Rhee, H.; Park, J.H.; Cho, E.-S.; Yeom, S.-K.; Park, S.; Park, M.-S.; et al. Preoperative prediction of postsurgical outcomes in mass-forming intrahepatic cholangiocarcinoma based on clinical, radiologic, and radiomics features. Eur. Radiol. 2021, 31, 8638–8648. [Google Scholar] [CrossRef]
- Qian, X.; Lu, X.; Ma, X.; Zhang, Y.; Zhou, C.; Wang, F.; Shi, Y.; Zeng, M. A Multi-Parametric Radiomics Nomogram for Preoperative Prediction of Microvascular Invasion Status in Intrahepatic Cholangiocarcinoma. Front. Oncol. 2022, 12, 838701. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhou, G.; Zhang, J.; Xu, C.; Wang, X.; Xu, P. Radiomics signature on dynamic contrast-enhanced MR images: A potential imaging biomarker for prediction of microvascular invasion in mass-forming intrahepatic cholangiocarcinoma. Eur. Radiol. 2021, 31, 6846–6855. [Google Scholar] [CrossRef]
- Fiz, F.; Masci, C.; Costa, G.; Sollini, M.; Chiti, A.; Ieva, F.; Torzilli, G.; Viganò, L. PET/CT-based radiomics of mass-forming intrahepatic cholangiocarcinoma improves prediction of pathology data and survival. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3387–3400. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Zhao, L.; Xin, B.; Ma, G.; Wang, X.; Song, S. 18F-FDG PET/CT radiomic analysis for classifying and predicting microvascular invasion in hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Quant. Imaging Med. Surg. 2022, 12, 4135–4150. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Yang, P.; Yen, E.A.; Wan, Y.; Jiang, Y.; Cao, Z.; Shen, X.; Wu, Y.; Wang, J.; Luo, C.; et al. A multi-organ cancer study of the classification performance using 2D and 3D image features in radiomics analysis. Phys. Med. Biol. 2019, 64, 215009. [Google Scholar] [CrossRef]
- Perrin, T.; Midya, A.; Yamashita, R.; Chakraborty, J.; Saidon, T.; Jarnagin, W.R.; Gonen, M.; Simpson, A.L.; Do, R.K.G. Short-term reproducibility of radiomic features in liver parenchyma and liver malignancies on contrast-enhanced CT imaging. Abdom. Radiol. N. Y. 2018, 43, 3271–3278. [Google Scholar] [CrossRef] [PubMed]
- Renzulli, M.; Pecorelli, A.; Brandi, N.; Brocchi, S.; Tovoli, F.; Granito, A.; Carrafiello, G.; Ierardi, A.M.; Golfieri, R. The Feasibility of Liver Biopsy for Undefined Nodules in Patients under Surveillance for Hepatocellular Carcinoma: Is Biopsy Really a Useful Tool? J. Clin. Med. 2022, 11, 4399. [Google Scholar] [CrossRef] [PubMed]
- Fong, Z.V.; Brownlee, S.A.; Qadan, M.; Tanabe, K.K. The Clinical Management of Cholangiocarcinoma in the United States and Europe: A Comprehensive and Evidence-Based Comparison of Guidelines. Ann. Surg. Oncol. 2021, 28, 2660–2674. [Google Scholar] [CrossRef]
- Lee, S.W.; Kim, H.J.; Park, J.H.; Park, D.I.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I. Clinical usefulness of 18F-FDG PET-CT for patients with gallbladder cancer and cholangiocarcinoma. J. Gastroenterol. 2010, 45, 560–566. [Google Scholar] [CrossRef]
- Lin, Y.; Chong, H.; Song, G.; Zhang, C.; Dong, L.; Aye, L.; Liang, F.; Yang, S.; Zeng, M.; Ding, G.; et al. The influence of 18F-fluorodeoxyglucose positron emission tomography/computed tomography on the N- and M-staging and subsequent clinical management of intrahepatic cholangiocarcinoma. HepatoBiliary Surg. Nutr. 2022, 11, 684–695. [Google Scholar] [CrossRef]
- Nishioka, E.; Tsurusaki, M.; Kozuki, R.; Im, S.-W.; Kono, A.; Kitajima, K.; Murakami, T.; Ishii, K. Comparison of Conventional Imaging and 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in the Diagnostic Accuracy of Staging in Patients with Intrahepatic Cholangiocarcinoma. Diagnostics 2022, 12, 2889. [Google Scholar] [CrossRef]
- Petrowsky, H.; Wildbrett, P.; Husarik, D.B.; Hany, T.F.; Tam, S.; Jochum, W.; Clavien, P.-A. Impact of integrated positron emission tomography and computed tomography on staging and management of gallbladder cancer and cholangiocarcinoma. J. Hepatol. 2010, 45, 43–50. [Google Scholar] [CrossRef] [PubMed]





| Study | Patients (n) | Arterial Phase (Hyperenhancement) | Portal/Late Phases | |
|---|---|---|---|---|
| Chen LD et al. [98] | 88 HCC 88 iCCA | 1.8% HCC 64.5% iCAA | Hyperenhancement: 98.2% HCC 88.7% iCCA Hypoenhancement: 11.3% HCC 1.8% iCCA | Early washout: 30.9% HCC 91.9% iCCA Marked washout: 1.3% HCC 61.3% iCCA |
| Chen T et al. [90] | 21 iCCA | 4.8% | Heterogeneous hyperenhancement: 61.9% Homogeneous hyperenhancement: 19.0% Isoenhancement: 4.8% Hypoenhancement: 4.8% | Rim-like venous hyperenhancement: 66.7% Hypoenhancement: 85.7% (portal–venous phase) 95.2% (late phase) |
| Guo et al. [99] | 56 iCCA 60 HCC | Irregular 62.5% iCCA 3.3% HCC | Hyperenhancement: 94.6% iCAA 100% HCC | Washout in late phase: 94.6% iCCA Marked washout: 67.9% iCCA 6.7% HCC |
| Huang et al. [94] | 99 iCCA 129 HCC | 50.5% iCCA 16.3% HCC | 15.2% iCCA 37.2% HCC | Early washout: 93.4% iCCA 96.1% HCC Marked washout: 23.2% iCCA 7.8% HCC |
| Li et al. [96] | With risk factors: 59 HCC 55 iCAA | 0% HCC 42.6% iCCA Risk factors: cirrhosis, chronic hepatitis | 100.0% HCC 50.0% iCCA | Early washout: 3.6% HCC 90.7% iCCA Marked washout: 3.4% HCC 79.6% iCCA |
| Without risk factors: 55 HCC 55 iCCA | 0% HCC 52.7% iCCA | 100.0% HCC 45.5% iCCA | Early washout: 5.6% HCC 92.7% iCCA Marked washout: 9.1% HCC 89.1% iCCA | |
| Wildner et al. [97] | 42 iCCA 278 HCC Cirrhosis: 16.7% iCCA 76.9% HCC | 85.7% iCCA 61% HCC | Center: 16.7% iCCA 60.3% HCC Periphery: 40.5% iCCA 75% HCC | Early washout (portal–venous phase): -Tumor center: 85.8% iCCA 49.8% HCC - Tumor periphery: 66.7% iCCA 32.6% HCC Washout in late phase: 92.9% iCCA 75% HCCs |
| Xu et al. [89] | 32 iCCA | 59.4% | Heterogeneous hyperenhancement: 18.8% Homogeneous hyperenhancement: 9.4% heterogeneous hypo-enhancement: 12.5% | Portal phase: -isoenhancement: 3.1% -hypoenhancement: 96.9% Late phase: hypoenhancement: 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerrito, L.; Ainora, M.E.; Borriello, R.; Piccirilli, G.; Garcovich, M.; Riccardi, L.; Pompili, M.; Gasbarrini, A.; Zocco, M.A. Contrast-Enhanced Imaging in the Management of Intrahepatic Cholangiocarcinoma: State of Art and Future Perspectives. Cancers 2023, 15, 3393. https://doi.org/10.3390/cancers15133393
Cerrito L, Ainora ME, Borriello R, Piccirilli G, Garcovich M, Riccardi L, Pompili M, Gasbarrini A, Zocco MA. Contrast-Enhanced Imaging in the Management of Intrahepatic Cholangiocarcinoma: State of Art and Future Perspectives. Cancers. 2023; 15(13):3393. https://doi.org/10.3390/cancers15133393
Chicago/Turabian StyleCerrito, Lucia, Maria Elena Ainora, Raffaele Borriello, Giulia Piccirilli, Matteo Garcovich, Laura Riccardi, Maurizio Pompili, Antonio Gasbarrini, and Maria Assunta Zocco. 2023. "Contrast-Enhanced Imaging in the Management of Intrahepatic Cholangiocarcinoma: State of Art and Future Perspectives" Cancers 15, no. 13: 3393. https://doi.org/10.3390/cancers15133393