
Caring for Adolescents and Young Adults (AYA) with Cancer: A Scoping Review into Caregiver Burdens and Needs
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
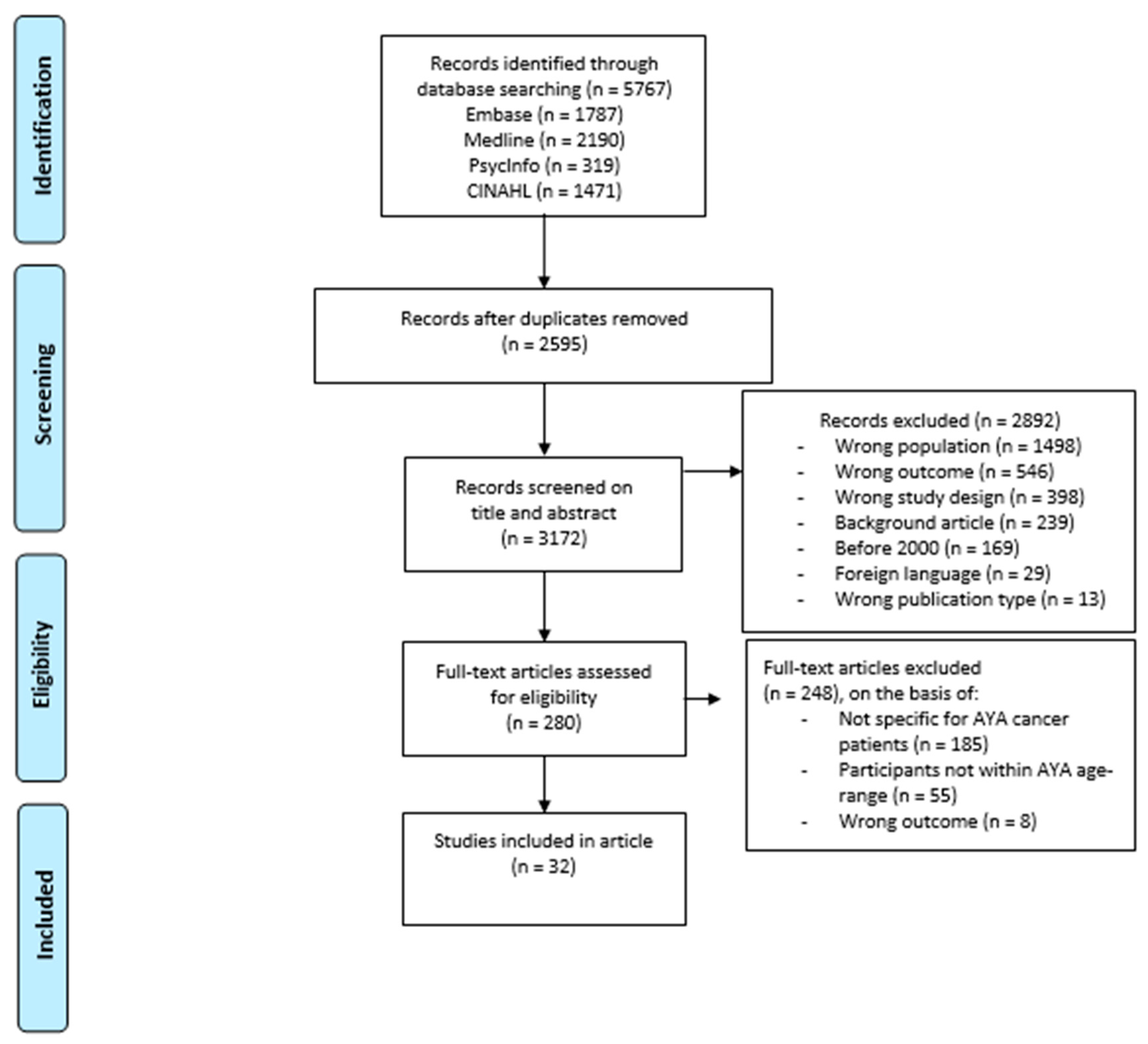
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
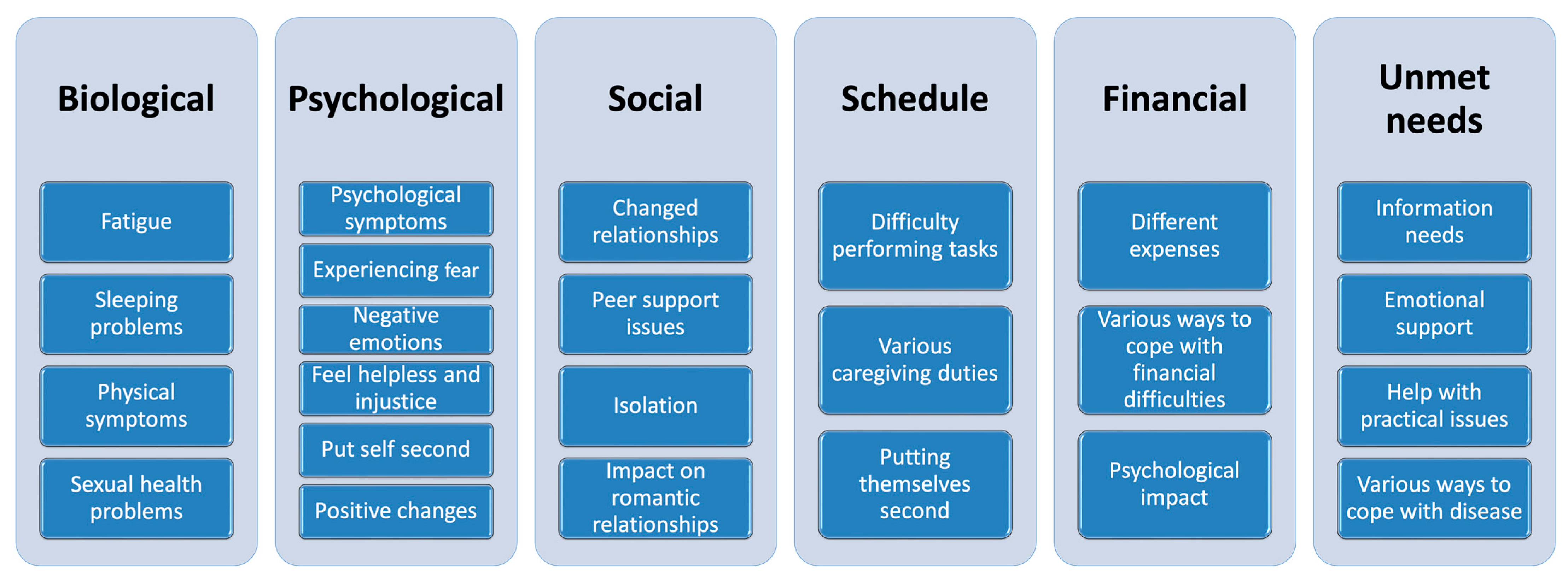
3. Results
3.1. Biological Impact

{kind=link}
{kind=link}
| First Author [Ref.] | Country, Year | Study Design | Participant Characteristics (Age of Patient at Diagnosis) | Outcome Measures | Summary of Findings |
|---|---|---|---|---|---|
| Borstelmann [25] | USA, 2022 | Cross-sectional | 289 partners of AYA cancer patients (22 to 40 years old) | Sexuality (GMSEX) | 20% of the participants reported sexual difficulties |
| Demiralp [18] | Turkey, 2010 | Qualitative | 2 spouses, 3 siblings, and 4 mothers of AYA cancer patients (16 to 38 years old) | Interviews to describe the personal experiences of family caregivers of patients with malignant tumors | Participants reported physical problems due to caregiving |
| Gorman [26] | USA, 2020 | Qualitative | 25 male partners of female AYA cancer patients (24 to 39 years old) | Interviews on how patients and partners appraise and manage their sexual health and intimate relationships after cancer | Participants reported a decrease in sexual health and different practices to improve this |
| Grinyer [24] | UK, 2006 | Qualitative | 9 mothers of AYA cancer patients (18 to 25 years old) | Interviews on the health of mothers and coping with these issues | Participants ignored their own physical health issues |
| Head [27] | USA, 2018 | Qualitative | 8 spouses, 5 mothers, 5 siblings, 2 partners, and 1 child of AYA cancer patients (18 to 36 years old) | Interviews to identify salient issues in relation to illness transformations for supporters | Participants report lifestyle changes and an altered attitude towards preventative healthcare |
| Iannarino [19] | USA, 2018 | Qualitative | 14 spouses, 6 siblings, 4 partners, and 1 ex-partner of AYA cancer survivors (18 to 39 years old) | Interview questions were designed to elicit narrative examples of participants’ experiences of biographical disruption, their attempts to navigate altered relationships, and their evaluations of others’ support attempts following biographical disruption | Participants were fatigued, which was caused by caregiving |
| Jeon [22] | Australia, 2020 | Qualitative | 3 caregivers of AYA cancer patients (aged 29 to 35 years old) | Explore sleep experiences of caregivers: perceptions of the nature and impact on sleep disturbances, potential ecological factors, and views on treatment options | Participants identified sleeping problems due to worrying and a lack of time to rest |
| Nolbris [23] | Sweden, 2014 | Qualitative | 9 siblings of AYA cancer patients (15 to 22 years old) | Interviews on the experiences of being a sibling of someone with cancer and narrating their memories and thoughts | Participants report difficulty sleeping during the night |
| Sanden [20] | Norway, 2008 | Qualitative | A partner of an AYA cancer patient (27 years old) | Described the impact of living in a disrupted situation as partner to a patient with testicular cancer | Participant felt drained, leaving no energy for being emotional |
| Sari [21] | Turkey, 2013 | Qualitative | 13 parents of AYA cancer patients (15 to 17 years old) | Experiences of parents giving home care to their child on chemotherapy | Participants dealt with physical problems and were being hygienic to keep out viruses |
| Stevens [17] | UK, 2018 | Mixed-methods | 14 parents, 4 partners, 7 friends, and 4 other caregivers of AYA cancer patients (16 to 24 years old) | Unmet needs in cancer services | Participants reported impact on physical well-being due to caregiving |
3.2. Psychological Impact
| First Author [Ref.] | Country, Year | Study Design | Participant Characteristics (Age Patient at Diagnosis) | Outcome Measures | Summary of Findings |
|---|---|---|---|---|---|
| Baum [28] | USA, 2022 | Cross-sectional | 9 parents, 21 spouses, and 3 other caregivers of AYA cancer patients (16 to 39 years old) | PTSS (IES-R) Subjective distress (Distress Thermometer, Problem List) HRQoL (FACT-GP) Anxiety and depressive symptoms (ASR) |
|
| Bogetz [35] | USA, 2020 | Qualitative | 22 parents of AYA cancer patients (14 to 25 years old) | Interviews on communication, worries, information sharing, strengths, and support | Participants report many negative emotions and want to protect their AYA. They have difficulty balancing autonomy and advocating |
| Bogetz [40] | USA, 2022 | Qualitative | 22 parents of AYA cancer patients (14 to 25 years old) | Interviews on the process by which parents adapt to child’s serious illness | Participants experience negative emotions. There are also oscillating experiences during the disease, which they want to share |
| Borstelmann [25] | USA, 2022 | Cross-sectional | 289 partners of AYA cancer patients (22 to 40 years old) | Quality of life (CQOLC) Coping (BRIEF-COPE) Concerns (PCQ) Anxiety and Depression (HADS) |
|
| Cheng [31] | China, 2022 | Cross-sectional | 150 partners, 91 parents, 41 other (siblings, children or other relatives) caregivers of AYA cancer patients (15 to 39 years old) | Anxiety (GAD-7) Depression (PHQ-9) Quality of life (Quality of Life Family Scale) |
|
| Davies [41] | UK, 2019 | Qualitative | 3 partners of AYA cancer patients (19 to 20 years old) | Interviews on experiences of supporting an AYA with cancer | Participants reported to put themselves second and give up own comfort for caregiving |
| Demiralp [18] | Turkey, 2010 | Qualitative | 2 spouses, 3 siblings, and 4 mothers of AYA cancer patients (16 to 38 years old) | Interviews to describe the personal experiences of family caregivers of patients with malignant tumors | Participants identified various positive and negative emotions related to caregiving |
| Friesen [42] | Canada, 2002 | Qualitative | 4 children, 1 mother, 1 sibling, and 2 partners of 3 AYA cancer patients (28 to 40 years old) | Interviews regarding the impact of the disease on the family and their responses | Participants report difficulty in disclosing information to the patient |
| Gorman [26] | USA, 2020 | Qualitative | 25 male partners of female AYA cancer patients (24 to 39 years old) | Interviews on how patients and partners appraise and manage their sexual health and intimate relationships after cancer | Participants had negative emotions regarding reduced intimacy with their partner |
| Grinyer [24] | UK, 2006 | Qualitative | 9 mothers of AYA cancer patients (18 to 25 years old) | Interviews on the health of mothers coping with these issues | Participants reported difficulty balancing their input during hospital visits while being sensitive to independence |
| Head [27] | USA, 2018 | Qualitative | 8 spouses, 5 mothers, 5 siblings, 2 partners, and 1 child of AYA cancer patients (18 to 36 years old) | Interviews to identify salient issues related to illness transformations for supporters | Participants showed a changed outlook on life due to the disease |
| Iannarino [19] | USA, 2018 | Qualitative | 14 spouses, 6 siblings, 4 partners, and 1 ex-partner of AYA cancer survivors (18 to 39 years old) | Interview questions were designed to elicit narrative examples of participants’ experience of biographical disruption, their attempts to navigate altered relationships, and their evaluations of others’ support attempts following biographical disruption | Participants showed many negative emotions due to the disease and tended not to share those with others |
| McCarthy [29] | Australia, 2016 | Cross-sectional | 204 parent caretakers of AYA cancer patients (15 to 25 years old) | PTSS (PCL-S) Distress (K10) Impact of cancer (Life Impact Scale) Life stress |
|
| Mikrut [32] | USA, 2017 | Cross-sectional | 66 parents of AYA cancer patients (17 to 39 years old) | Social constraints on emotional disclosure (Lopre, 1999) Cognitive processing (IES-R) Fear of cancer recurrence (Concerns about Recurrence Scale) Depressive symptoms (PHQ-9) |
|
| Mishra [30] | USA, 2018 | Qualitative | 5 partners, 1 parent, and 2 undefined caregivers of AYA cancer patients (20 to 39 years old) | Interviews to examine the experiences of cancer as an informal caregiver | Participants reported many negative psychological symptoms due to caregiving There were also positive changes in their outlook on life |
| Nam [34] | USA, 2016 | Cross-sectional | Parents and other family caregivers of AYA cancer patients (15 to 21 years old) | Distress (IES) Sociodemographic and clinical variables | 60.5% had a distress score of a clinically significant level (score above 26 on IES), which is an overall clinical concern for PTSD They had lower levels of intrusion compared to caregivers for younger patients (overall p = 0.02) |
| Nolbris [23] | Sweden, 2014 | Qualitative | 9 siblings of AYA cancer patients (15 to 22 years old) | Interviews on the experiences of being a sibling of someone with cancer, narrating their memories and thoughts | Participants experienced negative emotions because of the realization of mortality. They felt helpless and left out, and had to adjust to the situation |
| Palma [39] | USA, 2015 | Qualitative | 46 mothers of AYA patients (14 to 30 years old) | Identifying the daily maternal caregiver demands | Difficulty in letting the patient be independent during hospital visits, wanting to advocate |
| Sanden [20] | Norway, 2008 | Case study | A partner of an AYA cancer patient (27 years old) | Described the impact of living in a disrupted situation as partner to a patient with testicular cancer | Participant put self second and neglected own needs. She wanted to experience everything together, but also has a changed future |
| Schweitzer [36] | Australia, 2014 | Qualitative | 2 parents from AYA cancer patients (15 to 17 years old) | Identifying the experiences related to the diagnosis | Diagnosis was a shock and they realized their child could die. Also, positive change in outlook on life occurred |
| Van Schoors [37] | Belgium, 2019 | Qualitative | 4 parents and three siblings of AYA cancer patients (16 years old) | Interviews on the experiences of the diagnostic and treatment process, as well as perspectives on family relationships and functioning post diagnosis | Participants felt separated from family. They had negative emotions but had a hard time talking about them. Also, felt like a team to take care of the patient. |
3.3. Social Impact
| First Author [Ref.] | Country, Year | Study Design | Participant Characteristics (Age of Patient at Diagnosis) | Outcome Measures | Summary of Findings |
|---|---|---|---|---|---|
| Bogetz [40] | USA, 2022 | Qualitative | 22 parents of AYA cancer patients (14 to 25 years old) | Interviews on the process by which parents adapt to child’s serious illness | Support from others was perceived as helpful Participants also felt isolated |
| Borstelmann [25] | USA, 2022 | Cross-sectional | 289 partners of AYA cancer patients (22 to 40 years old) | Relationship strain (CARES) | 32% of all participants reported relationship strain |
| Demiralp [18] | Turkey, 2010 | Qualitative | 2 spouses, 3 siblings, and 4 mothers of AYA cancer patients (16 to 38 years old) | Interviews to describe the personal experiences of family caregivers of patients with malignant tumors | Participants experienced their family relationships as closer because of the disease |
| Gorman [26] | USA, 2020 | Qualitative | 25 male partners of female AYA cancer patients (24 to 39 years old) | Interviews on how patients and partners appraised and managed their sexual health and intimate relationships after cancer | Participants perceived a positive change in their relationship with their partner |
| Grinyer [24] | UK, 2006 | Qualitative | 9 mothers of AYA cancer patients (18 to 25 years old) | Interviews on the health of mothers coping with these issues | Participants felt lonely and experienced relationship strain due to different ways of coping Impaired social life |
| Iannarino [19] | USA, 2018 | Qualitative | 14 spouses, 6 siblings, 4 partners, and 1 ex-partner of AYA cancer survivors (18 to 39 years old) | Interview questions were designed to elicit narrative examples of participants’ experiences of biographical disruption, their attempts to navigate altered relationships, and their evaluations of others’ support attempts following biographical disruption | Participants experienced a lack of support from others. They also had difficult dynamics with other supporters |
| Mader [43] | Denmark, 2020 | Cohort | 2579 parents of AYA cancer patients (15 to 19 years old) | Separation, divorce, family planning, and sociodemographic and clinical data | Participants had a lower risk of divorce or separation compared to parents of younger children with cancer (HR > 1 for all age-groups below 15 years old) |
| Mishra [30] | USA, 2018 | Qualitative | 5 partners, 1 parent, and 2 undefined caregivers of AYA cancer patients (20 to 39 years old) | Interviews to examine the experiences of cancer for an informal caregiver | Participants identify stronger relationships to the patient due to the disease |
| Reblin [44] | USA, 2017 | Qualitative | 8 parents and 1 spouse of AYA cancer patients (19 to 29 years old) | Provided an insight into the expectations for types of psychosocial support using interviews | Participants identified that relationships became more meaningful Also, there were difficult dynamics between caregivers |
| Sanden [20] | Norway, 2008 | Case study | A partner of an AYA cancer patient (27 years old) | Described the impact of living in a disrupted situation as partner to a patient with testicular cancer | Participant reported feeling a lot of support from family, which was perceived as helpful |
| Sari [21] | Turkey, 2013 | Qualitative | 13 parents of AYA cancer patients (15 to 17 years old) | Experiences of parents giving home care to their child on chemotherapy | Participants felt isolated as they reduced visits from others |
| Stevens [17] | UK, 2018 | Mixed-method | 14 parents, 4 partners, 7 friends, and 4 other caregivers of AYA cancer patients (16 to 24 years old) | Unmet needs in cancer services | Participants identified a changed relationship to the patient |
| Syse [33] | Norway, 2010 | Cohort | Registry of all divorce rates in Norway with filter for AYA cancer patients (15 to 18 years old) | Divorce rates | Among participants there was no significant effect for divorce probability for being a parent of a child with or without cancer (OR 1.04, CI 0.95 to 1.13). Age of child with cancer did not have a significant effect (OR 1.01, CI 0.77 to 1.31) |
3.4. Schedule Impact
| First Author [Ref.] | Country, Year | Study Design | Participant Characteristics (Age of Patient at Diagnosis) | Outcome Measures | Summary of Findings |
|---|---|---|---|---|---|
| Bogetz [35] | USA, 2020 | Qualitative | 22 parents of AYA cancer patients (14 to 25 years old) | Interviews on communication, worries, information sharing, strengths, and support | Participants had difficulty with the role of being a parent. They also struggled with all roles and tasks they had to undertake |
| Davies [41] | UK, 2019 | Qualitative | 3 partners of AYA cancer patients (19 to 20 years old) | Interviews on experiences of supporting an AYA with cancer | Participants helped AYA to continue daily life. They worked more hours, moved closer to them and helped to make decisions |
| Demiralp [18] | Turkey, 2010 | Qualitative | 2 spouses, 3 siblings, and 4 mothers of AYA cancer patients (16 to 38 years old) | Interviews to describe the personal experiences of family caregivers of patients with malignant tumors | Participants helped the patient with their daily activities |
| Friesen [42] | Canada, 2002 | Qualitative | 4 children, 1 mother, 1 sibling, and 2 partners of 3 AYA cancer patients (28 to 40 years old) | Interviews regarding the impact of the disease on the family and their responses | Participants worked more hours to take care of AYA, took care of their families and helped them get back into society |
| Gorman [26] | USA, 2020 | Qualitative | 25 male partners of female AYA cancer patients (24 to 39 years old) | Interviews on how patients and partners appraise and manage their sexual health and intimate relationships after cancer | Participants joined AYA for hospital visits and advocated for them. Difficult to shift back to sexual partner |
| Grinyer [24] | UK, 2006 | Qualitative | 9 mothers of AYA cancer patients (18 to 25 years old) | Interviews on the health of mothers coping with these issues. | Caregivers reported many different roles and tasks |
| Iannarino [19] | USA, 2018 | Qualitative | 14 spouses, 6 siblings, 4 partners, and 1 ex-partner of AYA cancer survivors (18 to 39 years old) | Interview questions were designed to elicit narrative examples of participants’ experiences of biographical disruption, their attempts to navigate altered relationships, and their evaluations of others’ support attempts following biographical disruption | Caregivers took on many different roles and tasks in addition to their normative ones. Their own life plan was disrupted |
| Palma [39] | USA, 2015 | Qualitative | 46 mothers of AYA patients (14 to 30 years old) | Daily maternal caregiver demands | Participants had to manage all disease-related tasks and help with asking questions and making decisions. They advocated for them and helped them back into society |
| Reblin [44] | USA, 2017 | Qualitative | 8 parents and 1 spouse of AYA cancer patients (19 to 29 years old) | Provided insight into the expectations for types of psychosocial support using interviews | Participants were emotional support and assisted with travelling. Dividing roles were based on one’s characteristics, and it was difficult to undertake caregiving aside from normal activities |
| Sanden [20] | Norway, 2008 | Case study | A partner of an AYA cancer patient (27 years old) | Described the impact of living in a disrupted situation as partner to a patient with testicular cancer | Participant managed medical care and emotional support and participated during healthcare visits. They gave up their own free time |
| Sari [21] | Turkey, 2013 | Qualitative | 13 parents of AYA cancer patients (15 to 17 years old) | Experiences of parents giving home care to their child on chemotherapy | Participants changed their living situation. They offered practical support and try to stay a parent in the meantime |
| Schweitzer [36] | Australia, 2014 | Qualitative | 2 parents of AYA cancer patients (15 to 17 years old) | Identifying the experiences related to the diagnosis | Participants felt like life revolved completely around hospital visits and medical care |
| Stevens [17] | UK, 2018 | Mixed-method | 14 parents, 4 partners, 7 friends, and 4 other caregivers of AYA cancer patients (16 to 24 years old) | Unmet needs in cancer services | Participants provided many types of support (emotional, practical, Advice, physical care, financial). Also, it was difficult to manage their normative tasks |
| Van Schoors [37] | Belgium,2019 | Qualitative | 4 parents and 3 siblings of AYA cancer patients (16 years old) | Interviews on the experiences of the diagnostic and treatment processes, as well as perspectives on family relationships and functioning post diagnosis | Participants gave up their own free time to take care of AYAs |
3.5. Financial Impact
| First Author [Ref.] | Country, Year | Study Design | Participant Characteristics (Age of Patient at Diagnosis) | Outcome Measures | Summary of Findings |
|---|---|---|---|---|---|
| Baum [28] | USA, 2022 | Cross-sectional | 9 parents, 21 spouses, and 3 other caregivers of AYA cancer patients (16 to 39 years old) | Financial toxicity (Cost) | 43.9% of participants had financial toxicity |
| Borstelmann [25] | USA, 2022 | Cross-sectional | 289 partners of AYA cancer patients (22 to 40 years old) | Financial security (self-developed) | 29% of participants had financial insecurity |
| Davies [41] | UK, 2019 | Qualitative | 3 partners of AYA cancer patients (19 to 20 years old) | Interviews on experiences of supporting an AYA with cancer | Moving closer to the patient increased costs for participants |
| Friesen [42] | Canada, 2002 | Qualitative | 4 children, 1 mother, 1 sibling, and 2 partners of 3 AYA cancer patients (28 to 40 years old) | Interviews regarding the impact of the disease on the family, and their responses | Participants took on multiple jobs to increase income |
| Iannarino [19] | USA, 2018 | Qualitative | 14 spouses, 6 siblings, 4 partners, and 1 ex-partner of AYA cancer survivors (18 to 39 years old) | Interview questions were designed to elicit narrative examples of participants’ experience of biographical disruption, their attempts to navigate altered relationships, and their evaluations of others’ support attempts following biographical disruption | Participants moved closer to the patient, leading to additional costs |
| McCarthy [46] | Australia, 2018 | Cross-sectional | 204 parent caretakers of AYA cancer patients (15 to 25 years old) | Information needs | 47% of participants needed financial support after treatment |
| McNeil [45] | Finland, 2019 | Cross-sectional | 204 parent caretakers of AYA cancer patients (15 to 25 years old) | Self-developed questionnaire on financial impact Use of income support | 62% of participants had financial difficulties and 38% wanted support for this during treatment. 68% also wanted this after treatment. 32% had problems in receiving this support |
| Mishra [30] | USA, 2018 | Qualitative | 5 partners, 1 parent, and 2 undefined caregivers of AYA cancer patients (20 to 39 years old) | Interviews to examine the experiences of cancer as an informal caregiver | Participants reported financial burdens due to the disease |
| Nightingale [38] | USA, 2021 | Qualitative | 23 parents and 1 grandparent of AYA cancer patients (15 to 39 years old) | Interviews eliciting understanding and experiences of financial aspects of cancer | Participants reported many financial issues due to disease-related expenses. They shielded their AYA from this burden |
| Stevens [17] | UK, 2018 | Mixed-method | 14 parents, 4 partners, 7 friends, and 4 other caregivers of AYA cancer patients (16 to 24 years old) | Unmet needs in cancer services | Participants reported financial problems due to the disease |
3.6. Unmet Needs
| First Author [Ref.] | Country, Year | Study Design | Participant Characteristics (Age of Patient at Diagnosis) | Outcome Measures | Summary of Findings |
|---|---|---|---|---|---|
| Bogetz [35] | USA, 2020 | Qualitative | 22 parents of AYA cancer patients (14 to 25 years old) | Interviews on communication, worries, information sharing, strengths and support | Participants reported various ways to cope with the disease |
| Bogetz [40] | USA, 2022 | Qualitative | 22 parents of AYA cancer patients (14 to 25 years old) | Interviews on the processes by which parents adapted to child’s serious illness | Participants had preferences for support and felt the need to share their experience. They reported various ways of coping |
| Cheng [31] | China, 2022 | Cross-sectional | 150 partners, 91 parents, and 41 other (siblings, children, or other relatives) caregivers of AYA cancer patients (15 to 39 years old) | Unmet needs (SPUNS-SFC) | Of the participants, at least 98.9% had one unmet need. Needs were positively associated with anxiety and depression |
| Demiralp [18] | Turkey, 2010 | Qualitative | 2 spouses, 3 siblings, and 4 mothers of AYA cancer patients (16 to 38 years old) | Interviews to describe the personal experiences of family caregivers of patients with malignant tumors | Participants reported various ways to cope with the disease |
| Gorman [26] | USA, 2020 | Qualitative | 25 male partners of female AYA cancer patients (24 to 39 years old) | Interviews on how patients and partners appraised and managed their sexual health and intimate relationships after cancer | Participants reported a preference for support for their sexual health |
| Grinyer [24] | UK, 2006 | Qualitative | 9 mothers of AYA cancer patients (18 to 25 years old) | Interviews on the health of mothers coping with these issues | Participants wished for support on how to talk to the patient regarding sexuality |
| Hodgson [48] | USA, 2021 | Cross-sectional | 5 parents, 2 partners, 10 spouses, and two other family members of AYA cancer patients (18 to 41 years old) | Distress (Distress Thermometer) Patient problems (Patient Problems List) Coping (Coping Strategies Inventory—Short Forms) | In participants, adaptive coping was related to less distress (B = −0.137, p < 0.05). An engaging coping style from patients was related to fewer patient problems for caregivers (B = −0.489, p = 0.014) |
| Iannarino [19] | USA, 2018 | Qualitative | 14 spouses, 6 siblings, 4 partners, and 1 ex-partner of AYA cancer survivors (18 to 39 years old) | Interview questions were designed to elicit narrative examples of participants’ experiences of biographical disruption, their attempts to navigate altered relationships, and their evaluations of others’ support attempts following biographical disruption | Participants reported a need for understandable information for all ages and those not familiar with the healthcare system |
| Jeon [22] | Australia, 2020 | Qualitative | 3 caregivers of AYA cancer patients (aged 29 to 35 years old) | Explored sleep experiences of caregivers: perceptions of the nature and impact on sleep disturbances, potential ecological factors, and views on treatment options | Participants reported various ways to cope with the disease |
| McCarthy [46] | Australia, 2018 | Cross-sectional | 204 parent caretakers of AYA cancer patients (15 to 25 years old) | Information needs Patient activation (PAM) | 50% of participants had information needs in any domain. 30% had support needs for themselves and the patient. They wanted to be able to discuss with the patient what is happening |
| McNeil [45] | Finland, 2019 | Cross-sectional | 204 parent caretakers of AYA cancer patients (15 to 25 years old) | Self-developed questionnaire on financial impact Use of income support Education and work impact Demographics and clinical variables | 38% wanted income support during treatment. 68% of them also wanted this support after treatment completion. 32% had difficulty receiving financial support due to multiple reasons |
| Mishra [30] | USA, 2018 | Qualitative | 5 partners, 1 parent, and 2 undefined caregivers of AYA cancer patients (20 to 39 years old) | Interviews to examine the experiences of cancer for an informal caregiver | Participants reported various ways of coping. They had a need for information on multiple domains |
| Nightingale [38] | USA, 2021 | Qualitative | 23 parents and 1 grandparent of AYA cancer patients (15 to 39 years old) | Interviews eliciting understanding and experiences of financial aspects of cancer | Participants had a need for financial support and information. They had many ways to cope with the financial issues |
| Sawyer [47] | Australia, 2017 | Cross-sectional | 204 parents of AYA cancer patients (15 to 25 years old) | Service needed (AYA Hope/CNQ-PC) Post-traumatic stress (PCL-S) | Participants had a need to talk to a social worker, and wanted a peer support group and religious counselling |
| Stevens [17] | UK, 2018 | Mixed-method | 14 parents, 4 partners, 7 friends, and 4 other caregivers of AYA cancer patients (16 to 24 years old) | Unmet needs in cancer services | There was a need for support in all domains of life among these participants. They wanted face-to-face guidance from the hospital |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Husson, O.; Zebrack, B.J.; Block, R.; Embry, L.; Aguilar, C.; Hayes-Lattin, B.; Cole, S. Health-Related Quality of Life in Adolescent and Young Adult Patients with Cancer: A Longitudinal Study. J. Clin. Oncol. 2017, 35, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Patterson, P.; McDonald, F.E.; Zebrack, B.; Medlow, S. Emerging Issues Among Adolescent and Young Adult Cancer Survivors. Semin. Oncol. Nurs. 2015, 31, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Stark, D.; Peccatori, F.; Fern, L.; Laurence, V.; Gaspar, N.; Bozovic-Spasojevic, I.; Smith, O.; De Munter, J.; Derwich, K.; et al. Adolescents and young adults (AYA) with cancer: A position paper from the AYA Working Group of the European Society for Medical Oncology (ESMO) and the European Society for Paediatric Oncology (SIOPE). ESMO Open 2021, 6, 100096. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, N.M.; Penney, A.; Zebrack, B. Providing developmentally appropriate psychosocial care to adolescent and young adult cancer survivors. Cancer 2011, 117 (Suppl. 10), 2329–2334. [Google Scholar] [CrossRef] [Green Version]
- Cheung, C.K.; Zebrack, B. What do adolescents and young adults want from cancer resources? Insights from a Delphi panel of AYA patients. Support. Care Cancer 2017, 25, 119–126. [Google Scholar] [CrossRef]
- Zebrack, B.J. Psychological, social, and behavioral issues for young adults with cancer. Cancer 2011, 117 (Suppl. 10), 2289–2294. [Google Scholar] [CrossRef] [Green Version]
- Zebrack, B.; Isaacson, S. Psychosocial Care of Adolescent and Young Adult Patients with Cancer and Survivors. J. Clin. Oncol. 2012, 30, 1221–1226. [Google Scholar] [CrossRef] [Green Version]
- Alfano, C.M.; Leach, C.R.; Smith, T.G.; Miller, K.D.; Alcaraz, K.I.; Bs, R.S.C.; Wender, R.C.; Brawley, O.W. Equitably improving outcomes for cancer survivors and supporting caregivers: A blueprint for care delivery, research, education, and policy. CA Cancer J. Clin. 2019, 69, 35–49. [Google Scholar] [CrossRef] [Green Version]
- Molassiotis, A.; Wang, M. Understanding and Supporting Informal Cancer Caregivers. Curr. Treat. Options Oncol. 2022, 23, 494–513. [Google Scholar] [CrossRef]
- Hawkey, A.J.; Ussher, J.M.; Perz, J.; Parton, C.; Patterson, P.; Bateson, D.; Hobbs, K.; Kirsten, L. The impact of cancer-related fertility concerns on current and future couple relationships: People with cancer and partner perspectives. Eur. J. Cancer Care 2021, 30, e13348. [Google Scholar] [CrossRef]
- Thana, K.; Lehto, R.; Sikorskii, A.; Wyatt, G. Informal caregiver burden for solid tumour cancer patients: A review and future directions. Psychol. Health 2021, 36, 1514–1535. [Google Scholar] [CrossRef]
- Ma, H.S.; Krümpelmann, A.; Haun, M.W.; Friederich, H.-C.; Huber, J.; Thomas, M.; Winkler, E.C.; Herzog, W.; Ma, M.H. When do we need to care about the caregiver? Supportive care needs, anxiety, and depression among informal caregivers of patients with cancer and cancer survivors. Cancer 2015, 121, 1513–1519. [Google Scholar] [CrossRef]
- Hu, X.; Peng, X.; Su, Y.; Huang, W. Caregiver burden among Chinese family caregivers of patients with lung cancer: A cross-sectional survey. Eur. J. Oncol. Nurs. 2018, 37, 74–80. [Google Scholar] [CrossRef]
- Junkins, C.C.; Kent, E.; Litzelman, K.; Bevans, M.; Cannady, R.S.; Rosenberg, A.R. Cancer across the ages: A narrative review of caregiver burden for patients of all ages. J. Psychosoc. Oncol. 2020, 38, 782–798. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef]
- Stevens, M.C.; Beynon, P.; Cameron, A.; Cargill, J.; Cheshire, J.; Dolby, S.; Psychol, C. Understanding and Utilizing the Unmet Needs of Teenagers and Young Adults with Cancer to Determine Priorities for Service Development: The Macmillan on Target Programme. J. Adolesc. Young-Adult Oncol. 2018, 7, 652–659. [Google Scholar] [CrossRef]
- Demiralp, M.; Hatipoglu, S.; Iyigun, E.; Demiralp, B.; Cicek, E.I.; Basbozkurt, M. Living with a Malignant Musculoskeletal Tumor. Experiences of Family Caregivers. Orthop. Nurs. 2010, 29, 86–91. [Google Scholar] [CrossRef]
- Iannarino, N.T. “It’s My Job Now, I Guess”: Biographical disruption and communication work in supporters of young adult cancer survivors. Commun. Monogr. 2018, 85, 491–514. [Google Scholar] [CrossRef]
- Sandén, I.; Söderhamn, O. Experiences of Living in a Disrupted Situation as Partner to a Man with Testicular Cancer. Am. J. Men’s Health 2009, 3, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Sari, H.Y.; Yilmaz, M.; Ozsoy, S.; Kantar, M.; Çetingul, N. Experiences of Parents with the Physical Care Needs at Home of Children with Cancer: A qualitative study. Cancer Nurs. 2013, 36, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Jeon, M.S.; Agar, M.R.; Koh, E.-S.; Nowak, A.K.; Hovey, E.J.; Dhillon, H.M. Understanding sleep disturbance in the context of malignant brain tumors: A qualitative analysis. Neuro-Oncol. Pract. 2021, 8, 179–189. [Google Scholar] [CrossRef]
- Nolbris, M.J.; Enskär, K.; Hellström, A.-L. Grief Related to the Experience of Being the Sibling of a Child with Cancer. Cancer Nurs. 2014, 37, E1–E7. [Google Scholar] [CrossRef] [PubMed]
- Grinyer, A. Caring for a young adult with cancer: The impact on mothers’ health. Health Soc. Care Community 2006, 14, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Borstelmann, N.A.; Rosenberg, S.; Gelber, S.; Zheng, Y.; Meyer, M.; Ruddy, K.J.; Schapira, L.; Come, S.; Borges, V.; Cadet, T.; et al. Partners of young breast cancer survivors: A cross-sectional evaluation of psychosocial concerns, coping, and mental health. J. Psychosoc. Oncol. 2020, 38, 670–686. [Google Scholar] [CrossRef]
- Gorman, J.R.; Smith, E.; Drizin, J.H.; Lyons, K.S.; Harvey, S.M. Navigating sexual health in cancer survivorship: A dyadic perspective. Support. Care Cancer 2020, 28, 5429–5439. [Google Scholar] [CrossRef]
- Head, K.J.; Iannarino, N.T. “It Changed Our Outlook on How We Want to Live”: Cancer as a Transformative Health Experience for Young Adult Survivors and Their Family Members. Qual. Health Res. 2019, 29, 404–417. [Google Scholar] [CrossRef]
- Baum, L.V.; Koyama, T.; Schremp, E.A.; Zhang, K.; Rodweller, C.A.; Roth, M.C.; Compas, B.E.; Friedman, D.L. Posttraumatic stress symptoms and financial toxicity among adolescent and young adult oncology patients and their caregivers at cancer diagnosis. Cancer 2022, 128, 2005–2014. [Google Scholar] [CrossRef]
- McCarthy, M.C.; McNeil, R.; Drew, S.; Dunt, D.; Kosola, S.; Orme, L.; Sawyer, S.M. Psychological Distress and Posttraumatic Stress Symptoms in Adolescents and Young Adults with Cancer and Their Parents. J. Adolesc. Young-Adult Oncol. 2016, 5, 322–329. [Google Scholar] [CrossRef]
- Mishra, S.I.; Brakey, H.R.; Kano, M.; Nedjat-Haiem, F.R.; Sussman, A.L. Health related quality of life during cancer treatment: Perspectives of young adult (23–39 years) cancer survivors and primary informal caregivers. Eur. J. Oncol. Nurs. 2018, 32, 48–54. [Google Scholar] [CrossRef]
- Cheng, Q.; Ng, M.S.; Choi, K.C.; So, W.K. Unmet needs, anxiety, depression, and quality of life among caregivers of adolescents and young adults with cancer: A cross-sectional study. Asia-Pac. J. Oncol. Nurs. 2022, 9, 100108. [Google Scholar] [CrossRef]
- Mikrut, E.E.; Panjwani, A.A.; Cipollina, R.; Revenson, T.A. Emotional adjustment among parents of adolescents and young adults with cancer: The influence of social constraints on cognitive processing and fear of recurrence. J. Behav. Med. 2020, 43, 237–245. [Google Scholar] [CrossRef]
- Syse, A.; Loge, J.H.; Lyngstad, T.H. Does Childhood Cancer Affect Parental Divorce Rates? A Population-Based Study. J. Clin. Oncol. 2010, 28, 872–877. [Google Scholar] [CrossRef]
- Nam, G.E.; Warner, E.L.; Morreall, D.K.; Kirchhoff, A.C.; Kinney, A.Y.; Fluchel, M. Understanding psychological distress among pediatric cancer caregivers. Support. Care Cancer 2016, 24, 3147–3155. [Google Scholar] [CrossRef]
- Bogetz, J.F.; Trowbridge, A.; Kingsley, J.; Taylor, M.; Rosenberg, A.R.; Barton, K.S. “It’s My Job to Love Him”: Parenting Adolescents and Young Adults with Advanced Cancer. Pediatrics 2020, 146, e2020006353. [Google Scholar] [CrossRef]
- Schweitzer, R.; Griffiths, M.; Yates, P. Parental experience of childhood cancer using Interpretative Phenomenological Analysis. Psychol. Health 2012, 27, 704–720. [Google Scholar] [CrossRef] [Green Version]
- Van Schoors, M.; De Mol, J.; Verhofstadt, L.L.; Goubert, L.; Van Parys, H. The family practice of support-giving after a pediatric cancer diagnosis: A multi-family member interview analysis. Eur. J. Oncol. Nurs. 2020, 44, 101712. [Google Scholar] [CrossRef] [Green Version]
- Nightingale, C.L.; Canzona, M.R.; Danhauer, S.C.; Reeve, B.B.; Howard, D.S.; Tucker-Seeley, R.D.; Golden, S.L.S.; Little-Greene, D.; Roth, M.E.; Victorson, D.E.; et al. Financial burden for caregivers of adolescents and young adults with cancer. Psycho-Oncology 2022, 31, 1354–1364. [Google Scholar] [CrossRef]
- Palma, E.; Maldonado, L.; Hobbie, W.; Ogle, S.; Kobayashi, K. Maternal Caregiving Demands for Adolescent and Young Adult Survivors of Pediatric Brain Tumors. Oncol. Nurs. Forum 2015, 42, 222–229. [Google Scholar] [CrossRef]
- Bogetz, J.; Trowbridge, A.; Kingsley, J.; Taylor, M.; Wiener, L.; Rosenberg, A.R.; Barton, K.S. Stuck Moments and Silver-Linings: The Spectrum of Adaptation Among Non-Bereaved and Bereaved Parents of Adolescents and Young Adults with Advanced Cancer. J. Pain Symptom Manag. 2021, 62, 709–719. [Google Scholar] [CrossRef]
- Davies, J.; Hannigan, B.; Kelly, D. The experience of partners supporting adolescents and young adults with cancer. J. Adv. Nurs. 2019, 75, 2890–2898. [Google Scholar] [CrossRef] [PubMed]
- Friesen, P.; Pepler, C.; Hunter, P. Interactive Family Learning Following a Cancer Diagnosis. Oncol. Nurs. Forum 2002, 29, 981–987. [Google Scholar] [CrossRef] [Green Version]
- Mader, L.; Hargreave, M.; Frederiksen, L.E.; Bidstrup, P.E.; Dalton, S.O.; Kjær, S.K.; Nielsen, T.T.; Kroyer, A.; Winther, J.F.; Erdmann, F. The impact of childhood cancer on parental separation, divorce, and family planning in Denmark. Cancer 2020, 126, 3330–3340. [Google Scholar] [CrossRef] [PubMed]
- Reblin, M.; Stanley, N.; Galligan, A.; Reed, D.; Quinn, G.P. Family dynamics in young adult cancer caregiving: “It should be teamwork”. J. Psychosoc. Oncol. 2018, 37, 526–540. [Google Scholar] [CrossRef] [PubMed]
- McNeil, R.J.; McCarthy, M.; Dunt, D.; Thompson, K.; Kosola, S.; Orme, L.; Drew, S.; Sawyer, S. Financial Challenges of Cancer for Adolescents and Young Adults and Their Parent Caregivers. Soc. Work Res. 2019, 43, 17–30. [Google Scholar] [CrossRef]
- McCarthy, M.C.; McNeil, R.; Drew, S.; Orme, L.; Sawyer, S.M. Information needs of adolescent and young adult cancer patients and their parent-carers. Support. Care Cancer 2018, 26, 1655–1664. [Google Scholar] [CrossRef]
- Sawyer, S.M.; McNeil, R.; McCarthy, M.; Orme, L.; Thompson, K.; Drew, S.; Dunt, D. Unmet need for healthcare services in adolescents and young adults with cancer and their parent carers. Support. Care Cancer 2017, 25, 2229–2239. [Google Scholar] [CrossRef]
- Hodgson, J.; Lamson, A.; Kolobova, I.; Tucker, E.; Brimhall, A.; Lea, C.S.; Brinkley, J. The Experience of Distress and Coping Among Young Adults with Cancer and Their Caregivers. Contemp. Fam. Ther. 2022, 44, 199–209. [Google Scholar] [CrossRef]
- Essig, S.; Steiner, C.; Kuehni, C.E.; Weber, H.; Kiss, A. Improving Communication in Adolescent Cancer Care: A Multiperspective Study. Pediatr. Blood Cancer 2016, 63, 1423–1430. [Google Scholar] [CrossRef] [Green Version]
- Koumarianou, A.; Symeonidi, A.E.; Kattamis, A.; Linardatou, K.; Chrousos, G.P.; Darviri, C. A review of psychosocial interventions targeting families of children with cancer. Palliat. Support. Care 2021, 19, 103–118. [Google Scholar] [CrossRef]
- Hoellen, F.; Wagner, J.F.; Lüdders, D.W.; Rody, A.; Banz-Jansen, C. Anxiety in caregiving partners of breast cancer patients. Arch. Gynecol. Obstet. 2019, 300, 993–1005. [Google Scholar] [CrossRef]
- Jones, J.M.; Lewis, F.M.; Griffith, K.; Cheng, T.; Secord, S.; Walton, T.; Bernstein, L.J.; Maheu, C.; Catton, P. Helping Her Heal-Group: A pilot study to evaluate a group delivered educational intervention for male spouses of women with breast cancer. Psycho-Oncology 2013, 22, 2102–2109. [Google Scholar] [CrossRef]
- Sidhu, R.; Passmore, A.; Baker, D. The effectiveness of a peer support camp for siblings of children with cancer. Pediatr. Blood Cancer 2006, 47, 580–588. [Google Scholar] [CrossRef]
- Packman, W.; Greenhalgh, J.; Chesterman, B.; Shaffer, T.; Fine, J.; Vanzutphen, K.; Golan, R.; Amylon, M.D. Siblings of Pediatric Cancer Patients: The quantitative and qualitative nature of quality of life. J. Psychosoc. Oncol. 2005, 23, 87–108. [Google Scholar] [CrossRef]
- Gregory, D.; Van Puymbroeck, M.; Crowe, B.; Garst, B.; Amylon, M. The Lived Experience of Siblings of Children with Cancer Who Attended a Peer Support Camp in the United States. Qual. Health Res. 2022, 32, 1342–1355. [Google Scholar] [CrossRef]
- Northouse, L.L.; Katapodi, M.C.; Schafenacker, A.M.; Weiss, D. The Impact of Caregiving on the Psychological Well-Being of Family Caregivers and Cancer Patients. Semin. Oncol. Nurs. 2012, 28, 236–245. [Google Scholar] [CrossRef] [Green Version]
- Cohen, M.; Kuten, A. Cognitive–behavior group intervention for relatives of cancer patients: A controlled study. J. Psychosom. Res. 2006, 61, 187–196. [Google Scholar] [CrossRef]
- Bevan, J.L.; Pecchioni, L.L. Understanding the impact of family caregiver cancer literacy on patient health outcomes. Patient Educ. Couns. 2008, 71, 356–364. [Google Scholar] [CrossRef]
- Hu, Y.; Liu, T.; Li, F. Association between dyadic interventions and outcomes in cancer patients: A meta-analysis. Support. Care Cancer 2019, 27, 745–761. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reuvers, M.J.P.; Gedik, A.; Way, K.M.; Elbersen-van de Stadt, S.M.; van der Graaf, W.T.A.; Husson, O. Caring for Adolescents and Young Adults (AYA) with Cancer: A Scoping Review into Caregiver Burdens and Needs. Cancers 2023, 15, 3263. https://doi.org/10.3390/cancers15123263
Reuvers MJP, Gedik A, Way KM, Elbersen-van de Stadt SM, van der Graaf WTA, Husson O. Caring for Adolescents and Young Adults (AYA) with Cancer: A Scoping Review into Caregiver Burdens and Needs. Cancers. 2023; 15(12):3263. https://doi.org/10.3390/cancers15123263
Chicago/Turabian StyleReuvers, Milou J. P., Asiye Gedik, Kirsty M. Way, Sanne M. Elbersen-van de Stadt, Winette T. A. van der Graaf, and Olga Husson. 2023. "Caring for Adolescents and Young Adults (AYA) with Cancer: A Scoping Review into Caregiver Burdens and Needs" Cancers 15, no. 12: 3263. https://doi.org/10.3390/cancers15123263