

E-Cadherin Expression Varies Depending on the Location within the Primary Tumor and Is Higher in Colorectal Cancer with Lymphoid Follicles
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. CRC Tissue Samples
2.3. Tumor Budding Parameters
2.4. Lymphoid Follicles
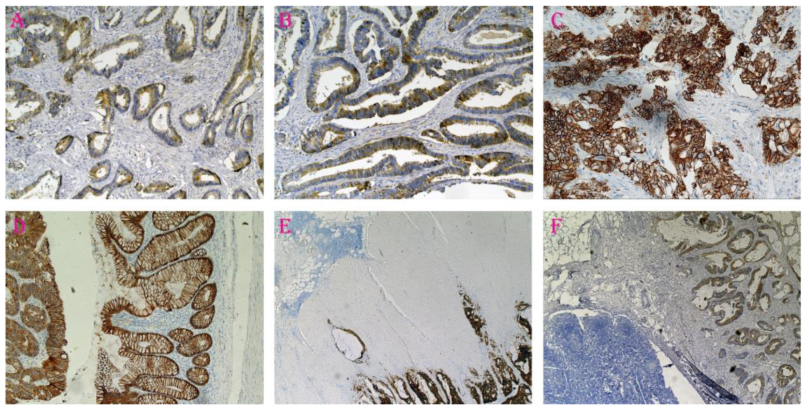
2.5. E-Cadherin Expression
2.6. Statistics
3. Results
3.1. Characteristics of the Population
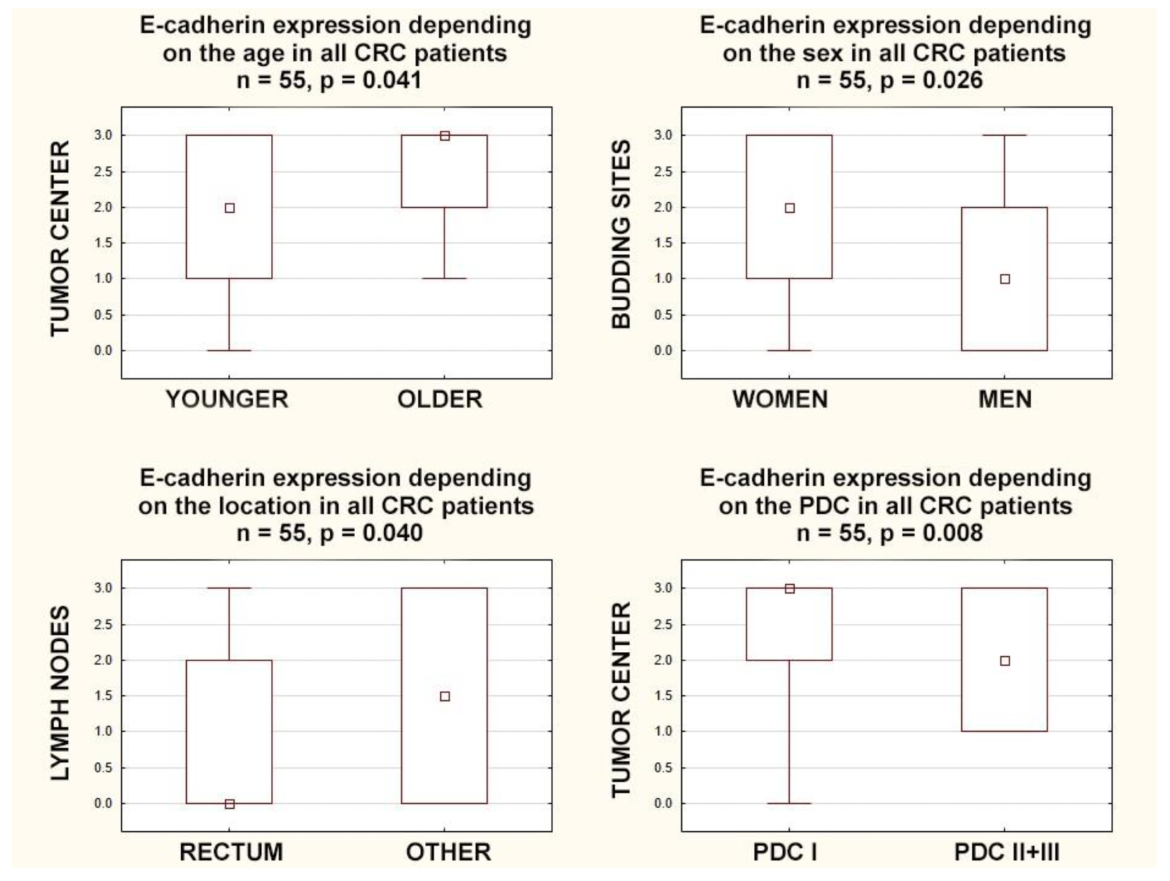
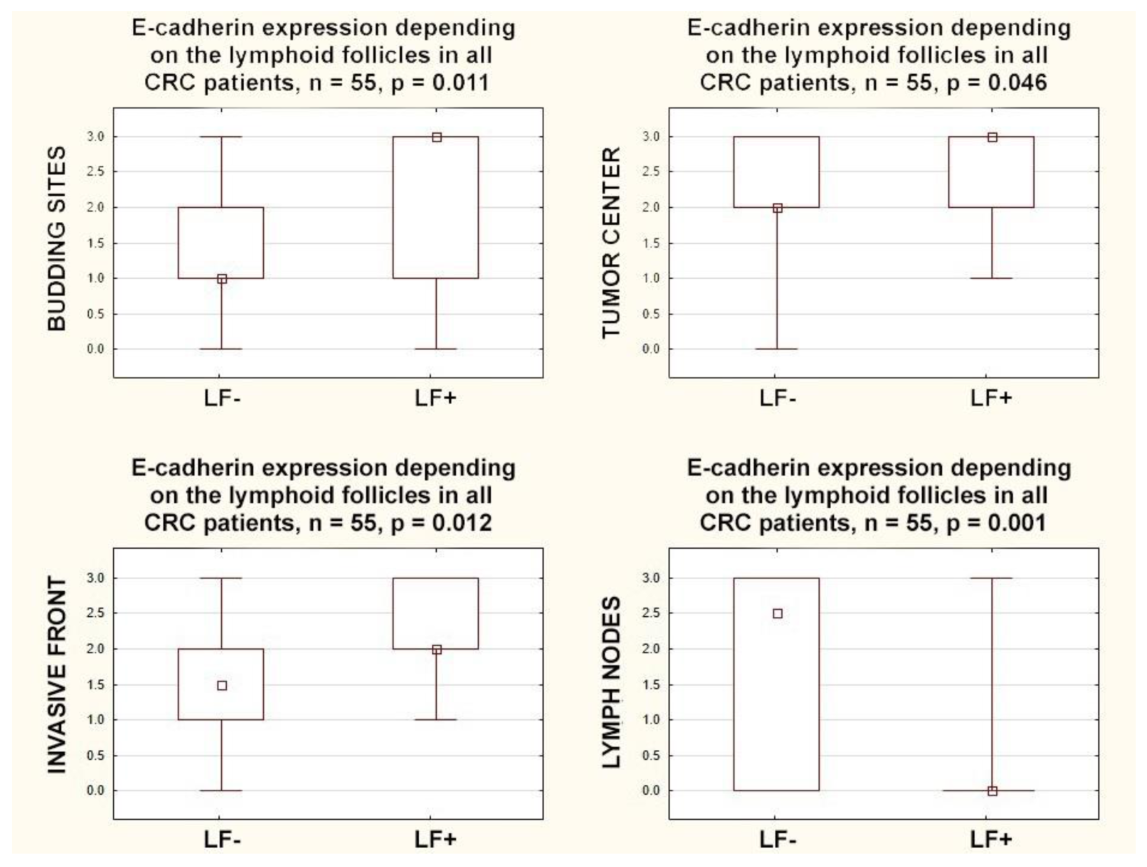
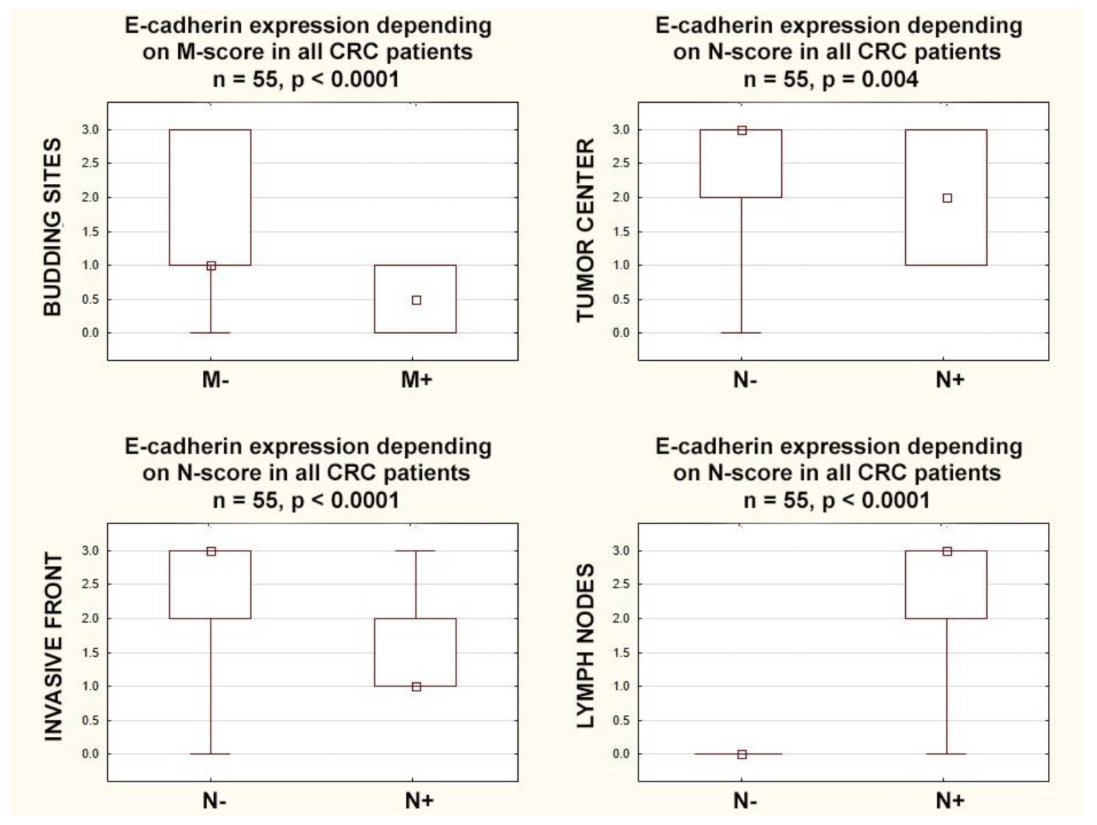
3.2. E-Cadherin Protein Expression
3.3. Lymphoid Follicles
3.4. Budding
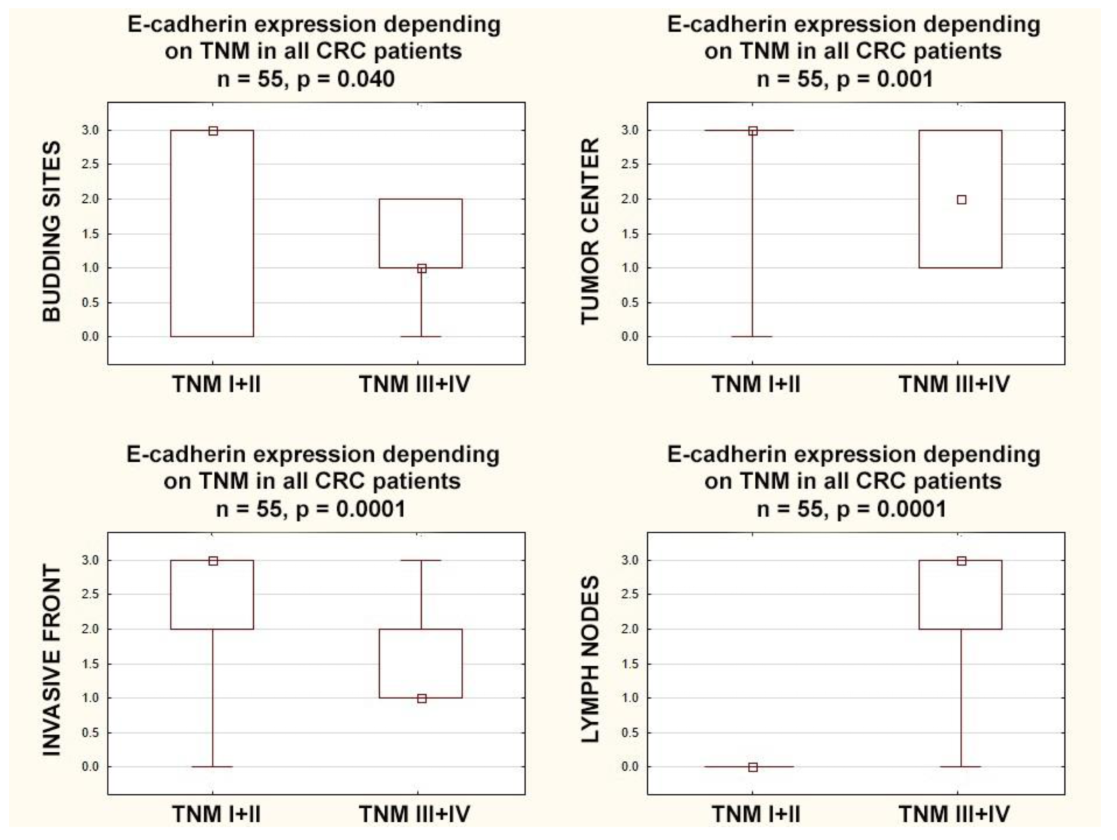
3.5. E-Cadherin Expression According to TNM Classification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, A.; Kumar, R.; Yadav, G.; Garg, P. Artificial intelligence in intestinal polyp and colorectal cancer prediction. Cancer Lett. 2023, 565, 216238. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal Cancer Statistics, 2023. CA Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef]
- Novikov, N.M.; Zolotaryova, S.Y.; Alexis, M.; Gautreau, A.M.; Denisov, E.V. Mutational drivers of cancer cell migration and invasion. Br. J. Cancer 2021, 124, 102–114. [Google Scholar] [CrossRef] [PubMed]
- Tunuguntla, A.; Suresh, T.N.; Pn, S. Association Between the Immunohistochemistry Expression of E-cadherin, Beta-Catenin, and CD44 in Colorectal Adenocarcinoma. Cureus 2023, 15, e35686. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Jin, J.; Zhou, Z.; Wang, Y.; Min, K.; Zuo, X.; Jiang, J.; Zhou, Y.; Shi, J. Snail inhibits metastasis via regulation of E-cadherin and is associated with prognosis in colorectal cancer. Oncol. Lett. 2023, 25, 271. [Google Scholar] [CrossRef] [PubMed]
- Markowski, A.R.; Błachnio-Zabielska, A.U.; Guzińska-Ustymowicz, K.; Markowska, A.; Pogodzińska, K.; Roszczyc, K.; Zińczuk, J.; Zabielski, P. Ceramides Profile Identifies Patients with More Advanced Stages of Colorectal Cancer. Biomolecules 2020, 10, 632. [Google Scholar] [CrossRef] [Green Version]
- Van den Berg, I.; Coebergh van den Braak, R.R.J.; van Vugt, J.L.A.; Ijzermans, J.N.M.; Buettner, S. Actual survival after resection of primary colorectal cancer: Results from a prospective multicenter study. World J. Surg. Onc. 2021, 19, 96. [Google Scholar] [CrossRef]
- American Joint Committee on Cancer. AJCC Cancer Staging Manual, 8th ed.; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Markowski, A.R.; Markowska, A.J.; Ustymowicz, W.; Pryczynicz, A.; Guzińska-Ustymowicz, K. Simultaneous analysis of tumor infiltrating immune cells density, tumor budding status, and presence of lymphoid follicles in CRC tissue. Sci. Rep. 2022, 12, 21732. [Google Scholar] [CrossRef]
- Carrie, A.; Duckworth, C.A. Identifying key regulators of the intestinal stem cell niche. Biochem. Soc. Trans. 2021, 49, 2163–2176. [Google Scholar]
- Burandt, E.; Lübbersmeyer, F.; Gorbokon, N.; Büscheck, F.; Luebke, A.M.; Menz, A.; Kluth, M.; Hube-Magg, C.; Hinsch, A.; Höflmayer, D.; et al. E-cadherin expression in human tumors: A tissue microarray study on 10,851 tumors. Biomark. Res. 2021, 9, 44. [Google Scholar] [CrossRef]
- Debnath, P.; Huirem, R.S.; Dutta, P.; Palchaudhuri, S. Epithelial–mesenchymal transition and its transcription factors. Biosci. Rep. 2022, 42, BSR20211754. [Google Scholar] [CrossRef] [PubMed]
- Loh, C.Y.; Chai, J.Y.; Tang, T.F.; Wong, W.F.; Sethi, G.; Shanmugam, M.K.; Chong, P.P.; Looi, C.Y. The E-Cadherin and N-Cadherin Switch in Epithelial-to-Mesenchymal Transition: Signaling, Therapeutic Implications, and Challenges. Cells 2019, 8, 1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zlobec, I.; Berger, M.D.; Lugli, A. Tumour budding and its clinical implications in gastrointestinal cancers. Br. J. Cancer. 2020, 123, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Choi, S.Y.; Kim, W.J.; Ji, M.; Lee, T.G.; Son, B.R.; Yoon, S.M.; Sung, R.; Lee, E.J.; Youn, S.J.; et al. Combined aberrant expression of E-cadherin and S100A4, but not β catenin is associated with disease free survival and overall survival in colorectal cancer patients. Diagn Pathol. 2013, 8, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.C.; Roh, S.A.; Kim, H.C.; Koo, K.H.; Cho, Y.K.; Yu, C.S.; Kwon, Y.M.; Kim, J.S. Coexpression of carcinoembryonic antigen and E-cadherin in colorectal adenocarcinoma with liver metastasis. J. Gastrointest Surg. 2003, 7, 931–938. [Google Scholar] [CrossRef]
- Bendardaf, R.; Sharif-Askari, F.S.; Sharif-Askari, N.S.; Syrjänen, K.; Pyrhönen, S. Cytoplasmic E-cadherin Expression Is Associated With Higher Tumour Level of VEGFA, Lower Response Rate to Irinotecan-based Treatment and Poorer Prognosis in Patients With Metastatic Colorectal Cancer. Anticancer Res. 2019, 39, 1953–1957. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.A.; Inamura, K.; Yamauchi, M.; Nishihara, R.; Mima, K.; Sukawa, Y.; Li, T.; Yasunari, M.; Morikawa, T.; Fitzgerald, K.C.; et al. Loss of CDH1 (E-cadherin) expression is associated with infiltrative tumour growth and lymph node metastasis. Br. J. Cancer 2016, 114, 199–206. [Google Scholar] [CrossRef] [Green Version]
- Tóth, L.; András, C.; Molnár, C.; Tanyi, M.; Csiki, Z.; Molnár, P.; Szántó, J. Investigation of β catenin and E-cadherin expression in Dukes B2 stage colorectal cancer with tissue microarray method. Is it a marker of metastatic potential in rectal cancer? Pathol. Oncol. Res. 2012, 18, 429–437. [Google Scholar] [CrossRef]
- Zhao, Y.; Yu, T.; Zhang, N.; Chen, J.; Zhang, P.; Li, S.; Luo, L.; Cui, Z.; Qin, Y.; Liu, F. Nuclear E-cadherin acetylation promotes colorectal tumorigenesis via enhancing β-catenin activity. Mol. Cancer Res. 2019, 17, 655–665. [Google Scholar] [CrossRef] [Green Version]
- Sipos, F.; Műzes, G. Isolated lymphoid follicles in colon: Switch points between inflammation and colorectal cancer? World J. Gastroenterol. 2011, 17, 1666–1673. [Google Scholar] [CrossRef]
- Fu, K.-I.; Sano, Y.; Kato, S.; Fujii, T.; Koba, I.; Yoshino, T.; Ochiai, A.; Yoshida, S.; Fujimori, T. Incidence and localization of lymphoid follicles in early colorectal neoplasms. World J. Gastroenterol. 2005, 11, 6863–6866. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.M.; Min, B.W.; Lee, J.H.; Choi, J.S.; Lee, S.I.; Park, S.S.; Kim, J.; Um, J.W.; Kim, S.H.; Moon, H.Y. The prognostic significance of E-cadherin and liver intestinE-cadherin expression in colorectal cancer. Dis. Colon. Rectum. 2007, 50, 1873–1880. [Google Scholar] [CrossRef]
- Lugli, A.; Zlobec, I.; Minoo, P.; Baker, K.; Tornillo, L.; Terracciano, L.; Jass, J.R. Prognostic significance of the wnt signalling pathway molecules APC, beta-catenin and E-cadherin in colorectal cancer: A tissue microarray-based analysis. Histopathology 2007, 50, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Karamitopoulou, E.; Zlobec, I.; Patsouris, E.; Peros, G.; Lugli, A. Loss of E-cadherin independently predicts the lymph node status in colorectal cancer. Pathology 2011, 43, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Ozgüven, B.Y.; Karacetin, D.; Kabukcuoğlu, F.; Taskin, T.; Yener, S. Immunohistochemical study of E-cadherin and β-catenin expression in colorectal carcinomas. Pol. J. Pathol. 2011, 62, 19–24. [Google Scholar]
- Mohri, Y. Prognostic significance of E-cadherin expression in human colorectal cancer tissue. Surg. Today 1997, 27, 606–612. [Google Scholar] [CrossRef]
- Hong, M.; Kim, J.W.; Shin, M.K.; Kim, B.C. Poorly Differentiated Clusters in Colorectal Adenocarcinomas Share Biological Similarities with Micropapillary Patterns as well as Tumor Buds. Korean Med. Sci. 2017, 32, 1595–1602. [Google Scholar] [CrossRef]
- Khoursheed, M.A.; Mathew, T.C.; Makar, R.R.; Louis, S.; Asfar, S.K.; Al Sayer, H.M.; Dashti, H.M.; Al Bader, A. Expression of E-cadherin in human colorectal cancer. Surgeon 2003, 1, 86–91. [Google Scholar] [CrossRef]
- Elzagheid, A.; Algars, A.; Bendardaf, R.; Lamlum, H.; Ristamaki, R.; Collan, Y.; Syrjanen, K.; Pyrhonen, S. E-cadherin expression pattern in primary colorectal carcinomas and their metastases reflects disease outcome. World J. Gastroenterol. 2006, 12, 4304–4309. [Google Scholar] [CrossRef]
- Miladi Abdennadher, I.; Abdelmaksoud Dammak, R.; Ayed Guerfali, D.B.; Ayadi, L.; Khabir, A.; Amouri, A.; Frikha, F.; Tahri, N.; Ellouz, S.; Frikha, M.; et al. Expression of COX 2 and E-cadherin in Tunisian patients with colorectal adenocarci¬noma. Acta Histochem. 2012, 114, 577–581. [Google Scholar] [CrossRef]
- El Gehani, K.; Aljafil, R.; El Hasadi, I.; Al-Ammari, S.; Said, W.; Adim, A.; Hasouna, A.B. Loss of E-cadherin Expression in Colorectal Carcinoma and its Prognostic Significance. Acta Sci. Gastroint. Dis. 2019, 2, 3–8. [Google Scholar]
- Dorudi, S.; Sheffield, J.P.; Poulsom, R.; Northover, J.M.; Hart, I.R. E-cadherin expression in colorectal cancer. An immunocy-tochemical and in situ hybridization study. Am. J. Pathol. 1993, 142, 981–986. [Google Scholar] [PubMed]
- Elzagheid, A.; Buhmeida, A.; Laato, M.; El Faitori, O.; Syrjänen, K.; Collan, Y.; Pyrhönen, S. Loss of E-cadherin expression predicts disease recurrence and shorter survival in colorectal carcinoma. APMIS 2012, 120, 539–548. [Google Scholar] [CrossRef]
- Yun, J.A.; Kim, S.H.; Hong, H.K.; Yun, S.H.; Kim, H.C.; Chun, H.K.; Cho, Y.B.; Lee, W.Y. Loss of E-cadherin expression is associated with a poor prognosis in stage III colorectal cancer. Oncology 2014, 86, 318–328. [Google Scholar] [CrossRef]
- Ikeguchi, M.; Taniguchi, T.; Makino, M.; Kaibara, N. Reduced E-cadherin expression and enlargement of cancer nuclei strongly correlate with hematogenic metastasis in colorectal adenocarcinoma. Scand J. Gastroenterol. 2000, 35, 839–846. [Google Scholar]
- Bhangu, A.; Wood, G.; Brown, G.; Darzi, A.; Tekkis, P.; Goldin, R. The role of epithelial mesenchymal transition and resistance to neoadjuvant therapy in locally advanced rectal cancer. Colorectal Dis. 2014, 16, O133–O143. [Google Scholar] [CrossRef]
- Jurčić, P.; Radulović, P.; Balja, M.P.; Milošević, M.; Krušlin, B. E-cadherin and NEDD9 expression in primary colorectal cancer, metastatic lymph nodes and liver metastases. Oncol. Lett. 2019, 17, 2881–2889. [Google Scholar] [CrossRef] [Green Version]
- Ikeguchi, M.; Makino, M.; Kaibara, N. Clinical significance of Ecadherin-catenin complex expression in metastatic foci of colorectal carcinoma. J. Surg. Oncol. 2001, 77, 201–207. [Google Scholar] [CrossRef]
- Palaghia, M.; Mihai, C.; Lozneanu, L.; Ciobanu, D.; Trofin, A.M.; Rotariu, A.; Târcoveanu, F.; Cijevschi Prelipcean, C. E-cadherin expression in primary colorectal cancer and metastatic lymph nodes. Rom. J. Morphol. Embryol. 2016, 57, 205–209. [Google Scholar] [PubMed]
- Masaki, T.; Goto, A.; Sugiyama, M.; Matsuoka, H.; Abe, N.; Sakamoto, A.; Atomi, Y. Possible contribution of CD44 variant 6 and nuclear beta-catenin expression to the formation of budding tumor cells in patients with T1 colorectal carcinoma. Cancer 2001, 92, 2539–2546. [Google Scholar] [CrossRef] [PubMed]
- Fujiyoshia, K.; Vayrynena, J.P.; Borowskya, J.; Papke, D.J., Jr.; Arimaa, K.; Harukia, K.; Kishikawaa, J.; Akimotoa, N.; Ugaia, T.; Laua, M.C.; et al. Tumour budding, poorly differentiated clusters, and T-cell response in colorectal cancer. EBioMedicine 2020, 57, 102860. [Google Scholar] [CrossRef] [PubMed]
- Jang, T.J. Expression of E-cadherin and b-catenin is Altered at Tumor Budding Sites, Whose Number is Associated with the Progression of Colorectal Carcinoma. Korean J. Pathol. 2009, 43, 523–527. [Google Scholar] [CrossRef] [Green Version]
- Zlobec, I.; Lugli, A.; Baker, K.; Roth, S.; Minoo, P.; Hayashi, S.; Terracciano, L.; Jass, J.R. Role of APAF-1, and peritumoral lymphocytic infiltration in tumour budding in colorectal cancer. J. Pathol. 2007, 212, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.; Jiang, L.; Sun, Y.; Li, H. Effect of E-cadherin on Prognosis of Colorectal Cancer: A Meta-Analysis. Mol. Diagn Ther. 2022, 26, 397–409. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender |
| Male, n = 27 (49.09%) |
| Female, n = 28 (50.91%) |
| Age |
| <60, n = 11 (20.00%) |
| 60–69, n = 18 (32.73%) |
| 70–79, n = 21 (38.18%) |
| ≥80, n = 5 (9.09%) |
| Primary tumor location |
| Rectum, n = 23 (41.82%) |
| Colon, n = 32 (58.18%) |
| Histologic type |
| Adenocarcinoma, n = 54 (98.18%) |
| Mucinous adenocarcinoma, n = 1 (1.82%) |
| T stage, Depth of tumor invasion |
| T1, submucosa, n = 0 |
| T2, muscularis propria, n = 3 (5.45%) |
| T3, subserosa, n = 52 (94.55%) |
| T4, serosa or other organs, n = 0 |
| N stage, Lymph node metastases |
| N0, absent, n = 29 (52.73%) |
| N1, present, n = 26 (47.27%) |
| M stage, Distant metastases |
| M0 absent, n = 49 (89.09%) |
| M1 present, n = 6 (10.91%) |
| TNM stage |
| TNM-I, n = 3 (5.45%) |
| TNM-II, n = 23 (41.82%) |
| TNM-III, n = 23 (41.82%) |
| TNM-IV, n = 6 (10.91%) |
| Lymphovascular invasion (LVI) |
| LVI-0, absent, n = 20 (36.36%) |
| LVI-1, present, n = 35 (63.64%) |
| Perineural invasion (PNI) |
| PNI-0, absent, n = 51 (92.73%) |
| PNI-1, present, n = 4 (7.27%) |
| E-cadherin expression pattern in the tumor center (ECD-TC) |
| ECD-TC-0, n = 1 (1.82%) |
| ECD-TC-1, n = 9 (16.36%) |
| ECD-TC-2, n = 16 (29.09%) |
| ECD-TC-3, n = 29 (52.73%) |
| E-cadherin expression pattern in the invasive front (ECD-IF) |
| ECD-IF-0, n = 1 (1.82%) |
| ECD-IF-1, n = 18 (32.73%) |
| ECD-IF-2, n = 20 (36.36%) |
| ECD-IF-3, n = 16 (29.09%) |
| E-cadherin expression pattern in tumor budding sites (ECD-BS) |
| ECD-BS-0, n = 13 (23.63%) |
| ECD-BS-1, n = 18 (32.73%) |
| ECD-BS-2, n = 8 (14.55%) |
| ECD-BS-3, n = 16 (29.09%) |
| E-cadherin expression pattern in regional lymph nodes (ECD-LN) |
| ECD-LN-0, n = 31 (56.36%) |
| ECD-LN-1, n = 2 (3.64%) |
| ECD-LN-2, n = 3 (5.45%) |
| ECD-LN-3, n = 19 (34.55%) |
| Tumor budding foci in colorectal cancer tissue (TBF) |
| TBF-1, n = 51 (92.73%) |
| TBF-2, n = 3 (5.45%) |
| TBF-3, n = 1 (1.82%) |
| Poorly differentiated clusters in colorectal cancer tissue (PDC) |
| PDC-1, n = 34 (61.82%) |
| PDC-2, n = 14 (25.45%) |
| PDC-3, n = 7 (12.73%) |
| Areas of poorly differentiated components in colorectal cancer tissue (POR) |
| POR-1, n = 36 (65.45%) |
| POR-2, n = 12 (21.82%) |
| POR-3, n = 7 (12.73%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markowski, A.R.; Ustymowicz, K.; Markowska, A.J.; Romańczyk, W.; Guzińska-Ustymowicz, K. E-Cadherin Expression Varies Depending on the Location within the Primary Tumor and Is Higher in Colorectal Cancer with Lymphoid Follicles. Cancers 2023, 15, 3260. https://doi.org/10.3390/cancers15123260
Markowski AR, Ustymowicz K, Markowska AJ, Romańczyk W, Guzińska-Ustymowicz K. E-Cadherin Expression Varies Depending on the Location within the Primary Tumor and Is Higher in Colorectal Cancer with Lymphoid Follicles. Cancers. 2023; 15(12):3260. https://doi.org/10.3390/cancers15123260
Chicago/Turabian StyleMarkowski, Adam R., Konstancja Ustymowicz, Anna J. Markowska, Wiktoria Romańczyk, and Katarzyna Guzińska-Ustymowicz. 2023. "E-Cadherin Expression Varies Depending on the Location within the Primary Tumor and Is Higher in Colorectal Cancer with Lymphoid Follicles" Cancers 15, no. 12: 3260. https://doi.org/10.3390/cancers15123260