

The SAlzburg PEritoneal SUrface CAlculator (SAPESUCA): The First Web-Based Application for Peritoneal Surface Area Quantification
 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
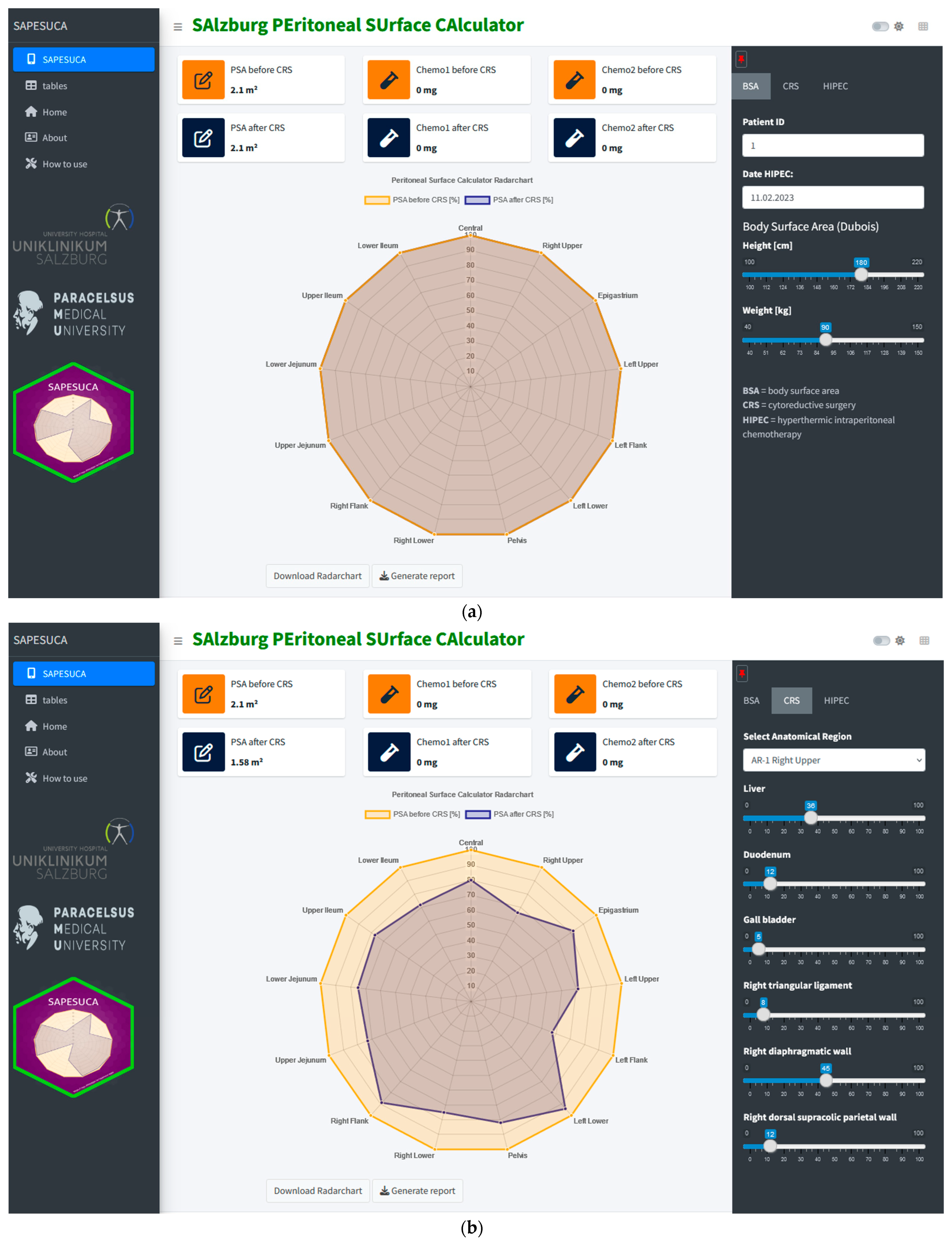
2.1. SAPESUCA R Shiny Application
2.2. SAPESUCA Calculation Algorithm
2.3. SAPESUCA Simulation Validation
2.4. Patients’ Selection Criteria
2.5. Cytoreductive Surgery
2.6. HIPEC Procedure
2.7. Postoperative Systemic Therapy and Follow-Up
2.8. Statistical Analysis
3. Results
3.1. Patients’ Baseline Characteristics
3.2. Quantification of the Peritoneal Surface Area before and after Cytoreductive Surgery with the SAPESUCA Application
3.3. Quantification of the Peritonectomy Extent with the SAPESUCA Application
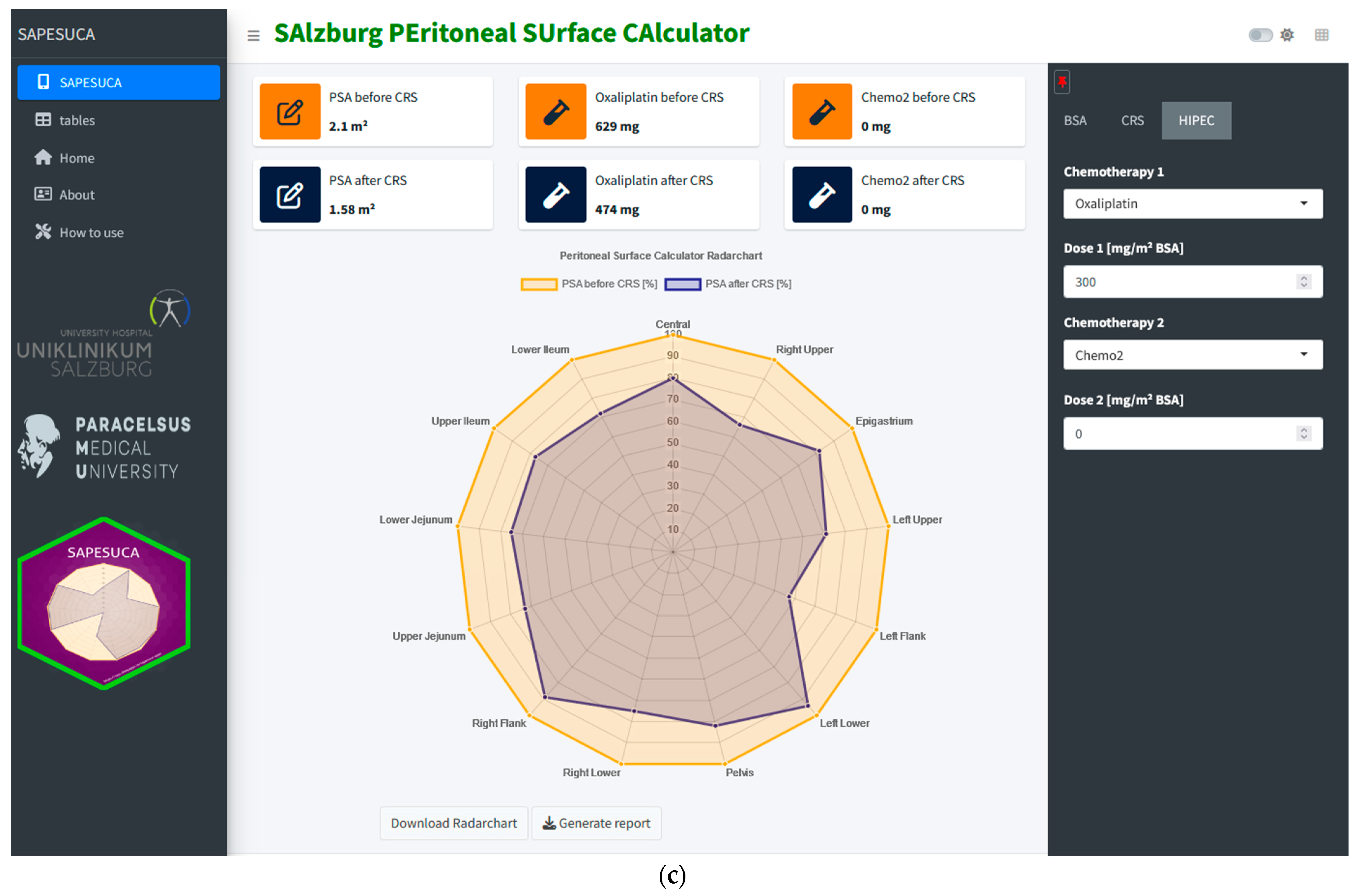
3.4. Individual Quantification of the Peritoneal Surface Area before and after CRS
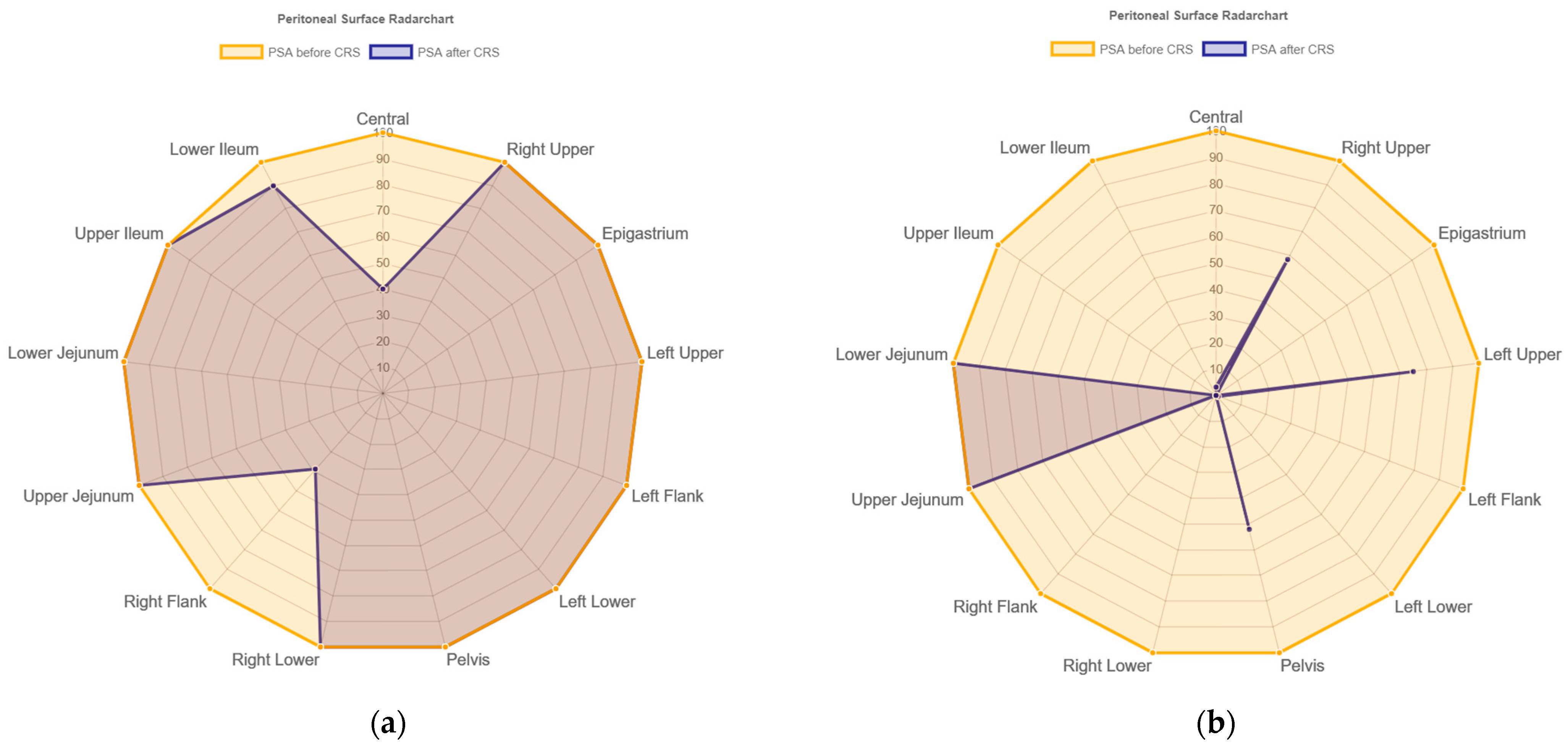
3.5. Correlation of Peritonectomy Extent and PCI Score
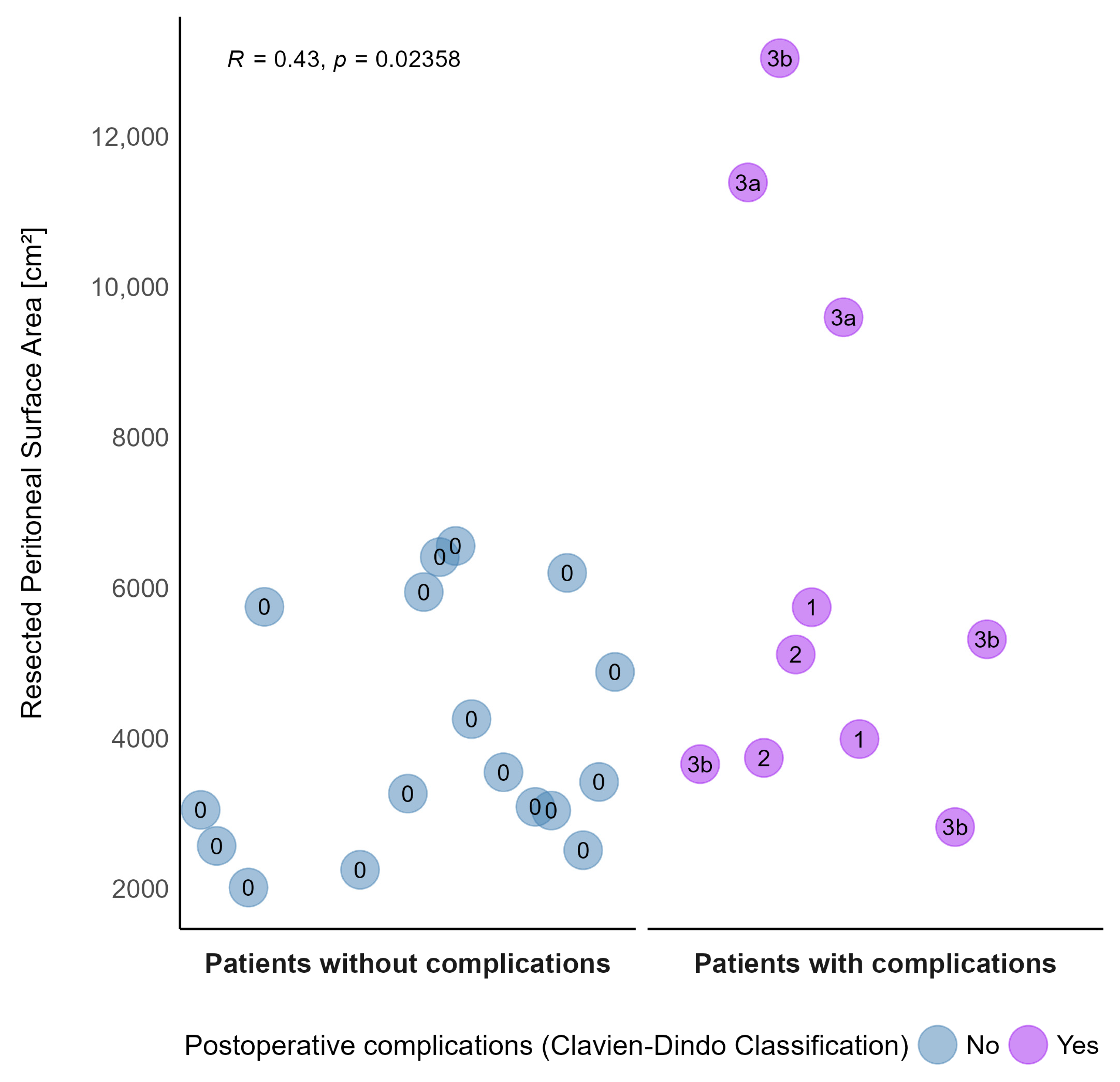
3.6. Correlation of Peritonectomy Extent and Morbidity
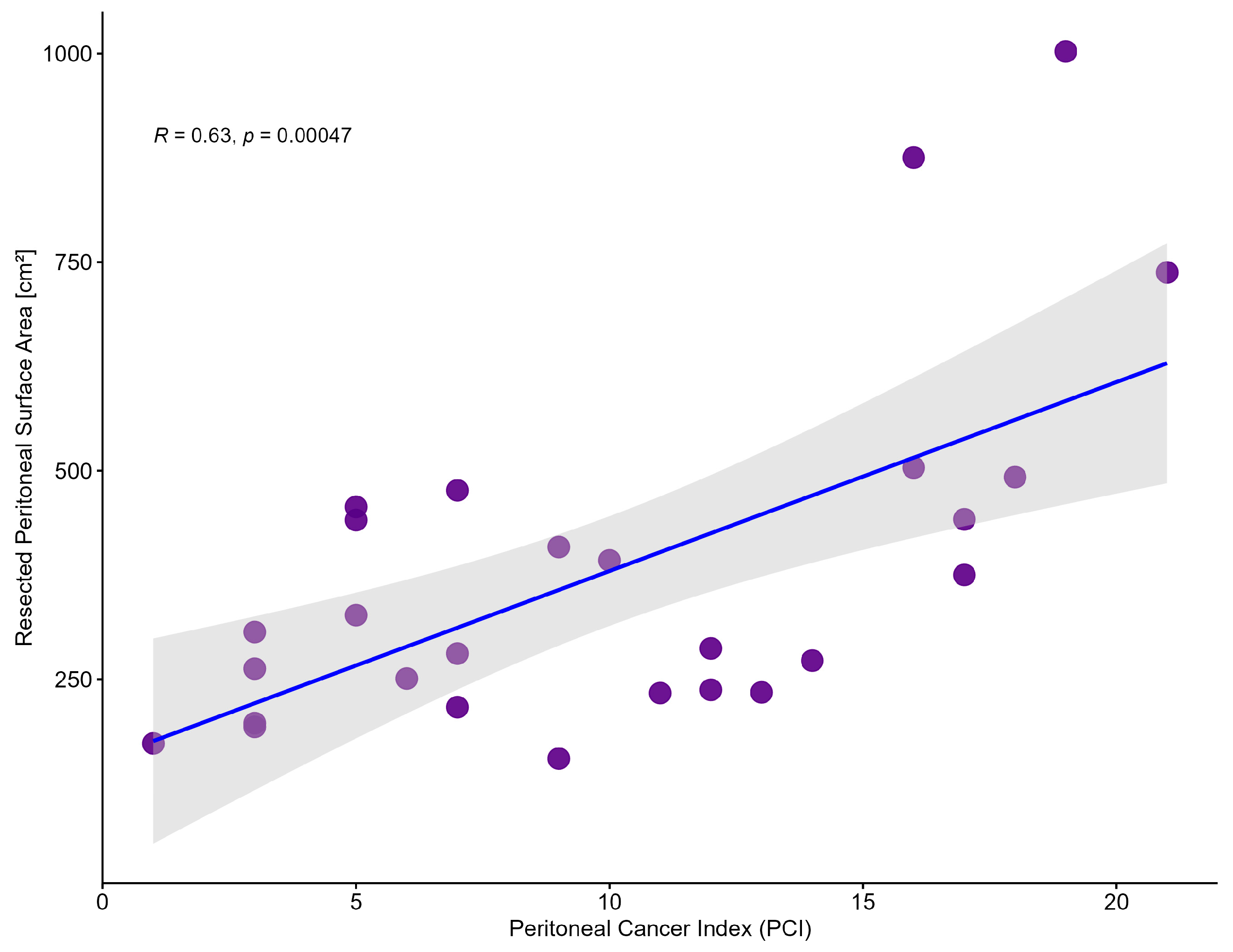
3.7. Simulation of the Chemotherapeutic Dose Adjustment by SAPESUCA Based on the Remaining PSA after CRS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SAPESUCA | SAlzburg PEritoneal SUrface CAlculator |
| HIPEC | Hyperthermic Intraperitoneal Chemotherapy |
| CRS | Cytoreductive Surgery |
| PSA | Peritoneal Surface Area |
| PCI | Peritoneal Cancer Index |
| SPCI | Simplified Peritoneal Cancer Index |
| CC | Completeness of Cytoreduction |
| PSS | Prior Surgical Score |
| PESUCA | PEritoneal SUrface CAlculator |
| BSA | Body Surface Area |
| KPI | Key Performance Indicator |
| GUI | Graphical User Interface |
| CT | Computed Tomography |
References
- Segelman, J.; Granath, F.; Holm, T.; Machado, M.; Mahteme, H.; Martling, A. Incidence, prevalence and risk factors for peritoneal carcinomatosis from colorectal cancer. Br. J. Surg. 2012, 99, 699–705. [Google Scholar] [CrossRef]
- van Gestel, Y.R.; de Hingh, I.H.; van Herk-Sukel, M.P.; van Erning, F.N.; Beerepoot, L.V.; Wijsman, J.H.; Slooter, G.D.; Rutten, H.J.; Creemers, G.J.; Lemmens, V.E. Patterns of metachronous metastases after curative treatment of colorectal cancer. Cancer Epidemiol. 2014, 38, 448–454. [Google Scholar] [CrossRef]
- Franko, J.; Shi, Q.; Goldman, C.D.; Pockaj, B.A.; Nelson, G.D.; Goldberg, R.M.; Pitot, H.C.; Grothey, A.; Alberts, S.R.; Sargent, D.J. Treatment of colorectal peritoneal carcinomatosis with systemic chemotherapy: A pooled analysis of north central cancer treatment group phase III trials N9741 and N9841. J. Clin. Oncol. 2012, 30, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Franko, J.; Shi, Q.; Meyers, J.P.; Maughan, T.S.; Adams, R.A.; Seymour, M.T.; Saltz, L.; Punt, C.J.A.; Koopman, M.; Tournigand, C.; et al. Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: An analysis of individual patient data from prospective randomised trials from the Analysis and Research in Cancers of the Digestive System (ARCAD) database. Lancet Oncol. 2016, 17, 1709–1719. [Google Scholar] [CrossRef] [PubMed]
- Klaver, C.E.L.; Wisselink, D.D.; Punt, C.J.A.; Snaebjornsson, P.; Crezee, J.; Aalbers, A.G.J.; Brandt, A.; Bremers, A.J.A.; Burger, J.W.A.; Fabry, H.F.J.; et al. Adjuvant hyperthermic intraperitoneal chemotherapy in patients with locally advanced colon cancer (COLOPEC): A multicentre, open-label, randomised trial. Lancet Gastroenterol. Hepatol. 2019, 4, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Goéré, D.; Glehen, O.; Quenet, F.; Guilloit, J.M.; Bereder, J.M.; Lorimier, G.; Thibaudeau, E.; Ghouti, L.; Pinto, A.; Tuech, J.J.; et al. Second-look surgery plus hyperthermic intraperitoneal chemotherapy versus surveillance in patients at high risk of developing colorectal peritoneal metastases (PROPHYLOCHIP-PRODIGE 15): A randomised, phase 3 study. Lancet Oncol. 2020, 21, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Quénet, F.; Elias, D.; Roca, L.; Goéré, D.; Ghouti, L.; Pocard, M.; Facy, O.; Arvieux, C.; Lorimier, G.; Pezet, D.; et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 256–266. [Google Scholar] [CrossRef]
- Kusamura, S.; Dominique, E.; Baratti, D.; Younan, R.; Deraco, M. Drugs, carrier solutions and temperature in hyperthermic intraperitoneal chemotherapy. J. Surg. Oncol. 2008, 98, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Helderman, R.; Loke, D.R.; Kok, H.P.; Oei, A.L.; Tanis, P.J.; Franken, N.; Crezee, J. Variation in Clinical Application of Hyperthermic Intraperitoneal Chemotherapy: A Review. Cancers 2019, 11, 78. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, A.; de Hingh, I.; Van Der Speeten, K.; Hubner, M.; Deraco, M.; Bakrin, N.; Villeneuve, L.; Kusamura, S.; Glehen, O. HIPEC Methodology and Regimens: The Need for an Expert Consensus. Ann. Surg. Oncol. 2021, 28, 9098–9113. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat. Res. 1996, 82, 359–374. [Google Scholar]
- Verwaal, V.J.; van Tinteren, H.; van Ruth, S.; Zoetmulder, F.A. Predicting the survival of patients with peritoneal carcinomatosis of colorectal origin treated by aggressive cytoreduction and hyperthermic intraperitoneal chemotherapy. Br. J. Surg. 2004, 91, 739–746. [Google Scholar] [CrossRef]
- Gilly, F.N.; Carry, P.Y.; Sayag, A.C.; Brachet, A.; Panteix, G.; Salle, B.; Bienvenu, J.; Burgard, G.; Guibert, B.; Banssillon, V.; et al. Regional chemotherapy (with mitomycin C) and intra-operative hyperthermia for digestive cancers with peritoneal carcinomatosis. Hepatogastroenterology 1994, 41, 124–129. [Google Scholar]
- Verwaal, V.J.; van Ruth, S.; de Bree, E.; van Sloothen, G.W.; van Tinteren, H.; Boot, H.; Zoetmulder, F.A. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J. Clin. Oncol. 2003, 21, 3737–3743. [Google Scholar] [CrossRef]
- Ahmad, S.A.; Kim, J.; Sussman, J.J.; Soldano, D.A.; Pennington, L.J.; James, L.E.; Lowy, A.M. Reduced morbidity following cytoreductive surgery and intraperitoneal hyperthermic chemoperfusion. Ann. Surg. Oncol. 2004, 11, 387–392. [Google Scholar] [CrossRef]
- Shen, P.; Hawksworth, J.; Lovato, J.; Loggie, B.W.; Geisinger, K.R.; Fleming, R.A.; Levine, E.A. Cytoreductive surgery and intraperitoneal hyperthermic chemotherapy with mitomycin C for peritoneal carcinomatosis from nonappendiceal colorectal carcinoma. Ann. Surg. Oncol. 2004, 11, 178–186. [Google Scholar] [CrossRef]
- Younan, R.; Kusamura, S.; Baratti, D.; Oliva, G.D.; Costanzo, P.; Favaro, M.; Gavazzi, C.; Deraco, M. Bowel complications in 203 cases of peritoneal surface malignancies treated with peritonectomy and closed-technique intraperitoneal hyperthermic perfusion. Ann. Surg. Oncol. 2005, 12, 910–918. [Google Scholar] [CrossRef] [PubMed]
- Harmon, R.L.; Sugarbaker, P.H. Prognostic indicators in peritoneal carcinomatosis from gastrointestinal cancer. Int. Semin. Surg. Oncol. 2005, 2, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 5 January 2023).
- Shinyapps.io by Posit. Available online: https://www.shinyapps.io/ (accessed on 24 January 2023).
- Schredl, P.; Ramspott, J.P.; Neureiter, D.; Emmanuel, K.; Jäger, T. The PEritoneal SUrface CAlculator (PESUCA): A new tool to quantify the resected peritoneal surface area after cytoreductive surgery. Pleura Peritoneum 2020, 5, 20190031. [Google Scholar] [CrossRef] [Green Version]
- Albanese, A.M.; Albanese, E.F.; Mino, J.H.; Gomez, E.; Gomez, M.; Zandomeni, M.; Merlo, A.B. Peritoneal surface area: Measurements of 40 structures covered by peritoneum: Correlation between total peritoneal surface area and the surface calculated by formulas. Surg. Radiol. Anat. 2009, 31, 369–377. [Google Scholar] [CrossRef] [PubMed]
- DuBois, D. A formula to estimate the approximate surface area if height and body mass be known. Arch. Intern. Med. 1916, 17, 863–871. [Google Scholar] [CrossRef] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Elias, D.; Bonnay, M.; Puizillou, J.M.; Antoun, S.; Demirdjian, S.; El, O.A.; Pignon, J.P.; Drouard-Troalen, L.; Ouellet, J.F.; Ducreux, M. Heated intra-operative intraperitoneal oxaliplatin after complete resection of peritoneal carcinomatosis: Pharmacokinetics and tissue distribution. Ann. Oncol. 2002, 13, 267–272. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology, Mesothelioma: Peritoneal, Version 1.2023—15 December 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/meso_peritoneal.pdf (accessed on 4 January 2023).
- Sugarbaker, P.H.; Chang, D. Long-term regional chemotherapy for patients with epithelial malignant peritoneal mesothelioma results in improved survival. Eur. J. Surg. Oncol. 2017, 43, 1228–1235. [Google Scholar] [CrossRef]
- Kusamura, S.; Kepenekian, V.; Villeneuve, L.; Lurvink, R.J.; Govaerts, K.; De Hingh, I.; Moran, B.J.; Van der Speeten, K.; Deraco, M.; Glehen, O. Peritoneal mesothelioma: PSOGI/EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Eur. J. Surg. Oncol. 2021, 47, 36–59. [Google Scholar] [CrossRef]
- Lin, Y.L.; Xu, D.Z.; Li, X.B.; Yan, F.C.; Xu, H.B.; Peng, Z.; Li, Y. Consensuses and controversies on pseudomyxoma peritonei: A review of the published consensus statements and guidelines. Orphanet J. Rare Dis. 2021, 16, 85. [Google Scholar] [CrossRef]
- Stephens, A.D.; Alderman, R.; Chang, D.; Edwards, G.D.; Esquivel, J.; Sebbag, G.; Steves, M.A.; Sugarbaker, P.H. Morbidity and mortality analysis of 200 treatments with cytoreductive surgery and hyperthermic intraoperative intraperitoneal chemotherapy using the coliseum technique. Ann. Surg. Oncol. 1999, 6, 790–796. [Google Scholar] [CrossRef]
- Glehen, O.; Osinsky, D.; Cotte, E.; Kwiatkowski, F.; Freyer, G.; Isaac, S.; Trillet-Lenoir, V.; Sayag-Beaujard, A.C.; François, Y.; Vignal, J.; et al. Intraperitoneal chemohyperthermia using a closed abdominal procedure and cytoreductive surgery for the treatment of peritoneal carcinomatosis: Morbidity and mortality analysis of 216 consecutive procedures. Ann. Surg. Oncol. 2003, 10, 863–869. [Google Scholar] [CrossRef]
- Kusamura, S.; Younan, R.; Baratti, D.; Costanzo, P.; Favaro, M.; Gavazzi, C.; Deraco, M. Cytoreductive surgery followed by intraperitoneal hyperthermic perfusion: Analysis of morbidity and mortality in 209 peritoneal surface malignancies treated with closed abdomen technique. Cancer 2006, 106, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Cavaliere, F.; De Simone, M.; Virzì, S.; Deraco, M.; Rossi, C.R.; Garofalo, A.; Di Filippo, F.; Giannarelli, D.; Vaira, M.; Valle, M.; et al. Prognostic factors and oncologic outcome in 146 patients with colorectal peritoneal carcinomatosis treated with cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy: Italian multicenter study S.I.T.I.L.O. Eur. J. Surg. Oncol. 2011, 37, 148–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.S.; Gelli, M.; Agarwal, D.; Goéré, D. Complications of Cytoreductive Surgery and HIPEC in the Treatment of Peritoneal Metastases. Indian J. Surg. Oncol. 2016, 7, 225–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceelen, W. HIPEC with oxaliplatin for colorectal peritoneal metastasis: The end of the road? Eur. J. Surg. Oncol. 2019, 45, 400–402. [Google Scholar] [CrossRef] [PubMed]
- Dedrick, R.L.; Myers, C.E.; Bungay, P.M.; DeVita, V.T. Pharmacokinetic rationale for peritoneal drug administration in the treatment of ovarian cancer. Cancer Treat. Rep. 1978, 62, 1–11. [Google Scholar] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | N = 27 (100%) | ||
|---|---|---|---|
| Median age [years] (range) | 56 (22–75) | ||
| Median BMI [kg/m2] (range) | 25.7 (15.2–31.2) | ||
| Sex | Male | 16 (59%) | |
| Tumor histology | Adenocarcinoma Mucinous Signet ring cell | 12 (44%) 12 (44%) 3 (11%) | |
| Tumor localization | Right colon Transverse colon Left colon Sigmoid colon | 8 (30%) 5 (18%) 4 (15%) 10 (37%) | |
| Previous abdominal surgery for colon cancer | Yes | 18 (67%) | |
| Previous chemotherapy | Yes | 18 (67%) | |
| Median PCI (range) | 9 (1–21) | ||
| Median operative time [min] (range) | 352 (190–632) | ||
| CC-score | 0 1 | 26 (96%) 1 (4%) | |
| Cytoreduction | Greater omentum Liver metastasis Gallbladder Lesser omentum Stomach Spleen Pancreas Small bowel Colon Rectum Bladder Uterus Ovaries Other organs | 20/27 (74%) 5/27 (19%) 7/27 (26%) 11/27 (41%) 0/27 (0%) 5/27 (19%) 2/27 (7%) 15/27 (56%) 21/27 (78%) 12/27 (44%) 1/27 (4%) 8/27 (30%) 9/27 (33%) 9/27 (33%) | |
| Stoma creation | Yes | 14 (52%) | |
| 30-day complication | Yes | 10 (37%) | |
| Clavien-Dindo complication rate | 0 I II IIIa IIIb | 17 (63%) 2 (7%) 2 (7%) 2 (7%) 4 (15%) | |
| Median length of hospital stay (days) (range) | 14 (7–61) | ||
| Median length of ICU stay (days) (range) | 2 (1–9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jäger, T.; Schredl, P.; Neureiter, D.; Presl, J.; Tschann, P.; Königsrainer, I.; Pascher, A.; Emmanuel, K.; Regenbogen, S.; Ramspott, J.P. The SAlzburg PEritoneal SUrface CAlculator (SAPESUCA): The First Web-Based Application for Peritoneal Surface Area Quantification. Cancers 2023, 15, 3134. https://doi.org/10.3390/cancers15123134
Jäger T, Schredl P, Neureiter D, Presl J, Tschann P, Königsrainer I, Pascher A, Emmanuel K, Regenbogen S, Ramspott JP. The SAlzburg PEritoneal SUrface CAlculator (SAPESUCA): The First Web-Based Application for Peritoneal Surface Area Quantification. Cancers. 2023; 15(12):3134. https://doi.org/10.3390/cancers15123134
Chicago/Turabian StyleJäger, Tarkan, Philipp Schredl, Daniel Neureiter, Jaroslav Presl, Peter Tschann, Ingmar Königsrainer, Andreas Pascher, Klaus Emmanuel, Stephan Regenbogen, and Jan Philipp Ramspott. 2023. "The SAlzburg PEritoneal SUrface CAlculator (SAPESUCA): The First Web-Based Application for Peritoneal Surface Area Quantification" Cancers 15, no. 12: 3134. https://doi.org/10.3390/cancers15123134