
Plasma Metabolomics Predicts Chemotherapy Response in Advanced Pancreatic Cancer
 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Populations
2.2. Study Design
2.3. Metabolic Analysis (dMRM; Dynamic Multiple-Reaction Monitoring)
2.4. Statistical Analysis
3. Results
3.1. Patients and Clinical Characteristics
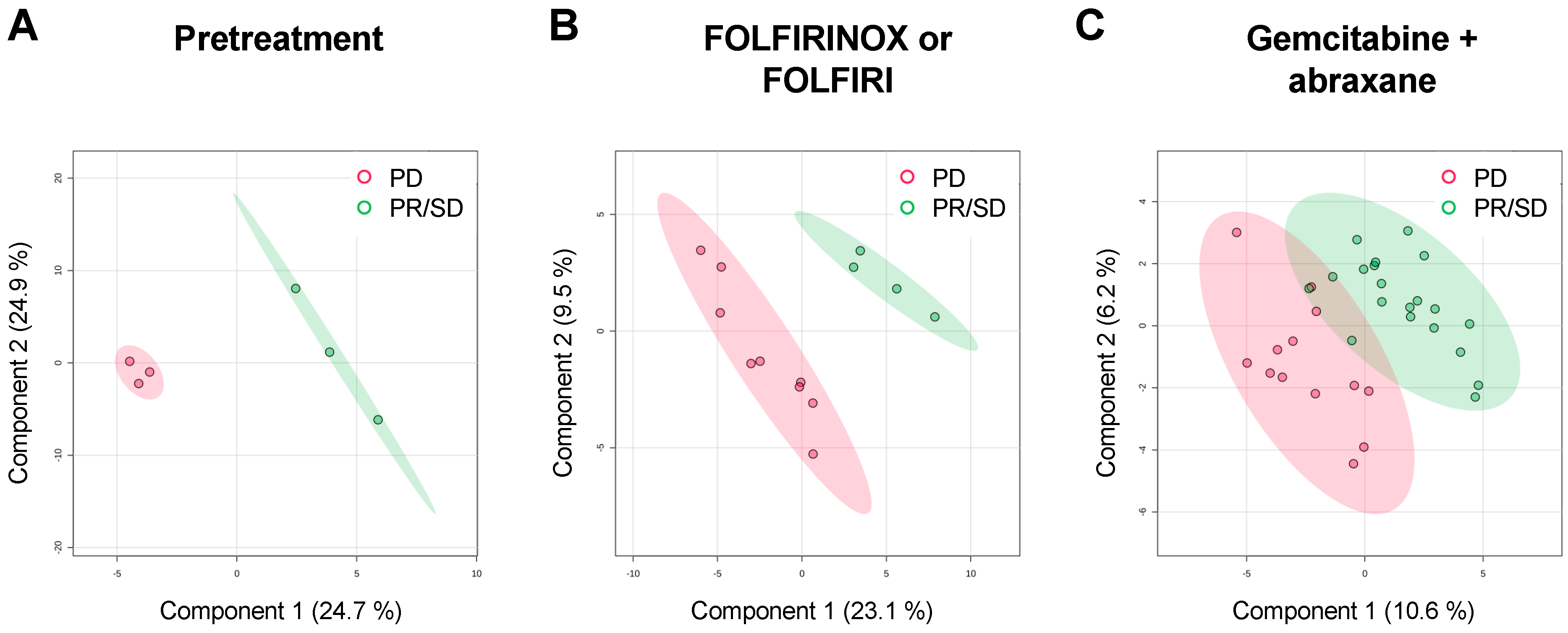
3.2. Plasma Metabolomic Profiles from APC Patients with Different Overall Response to Standard Chemotherapy Regimen
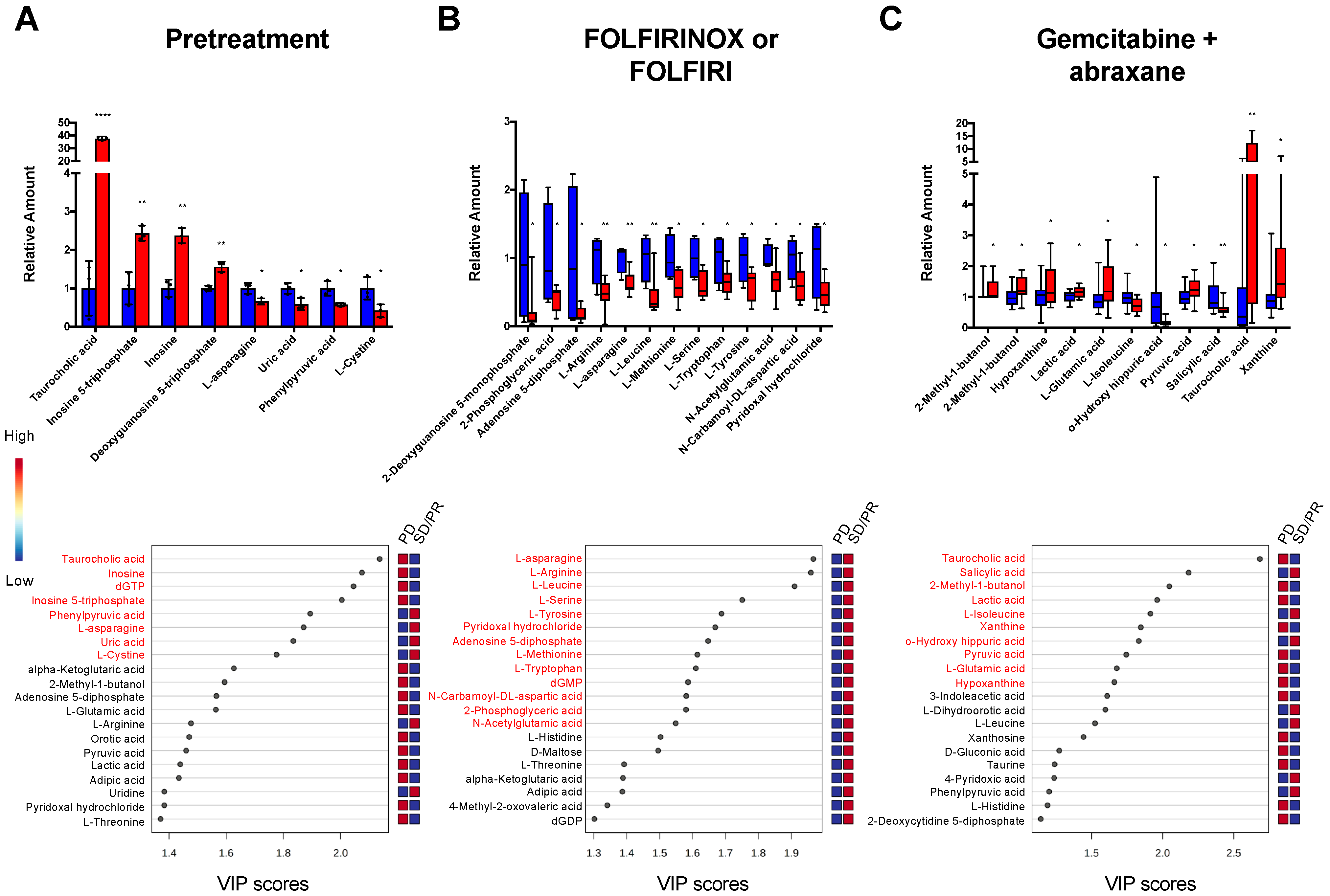
3.3. The Discovery and Identification of Metabolic Biomarkers
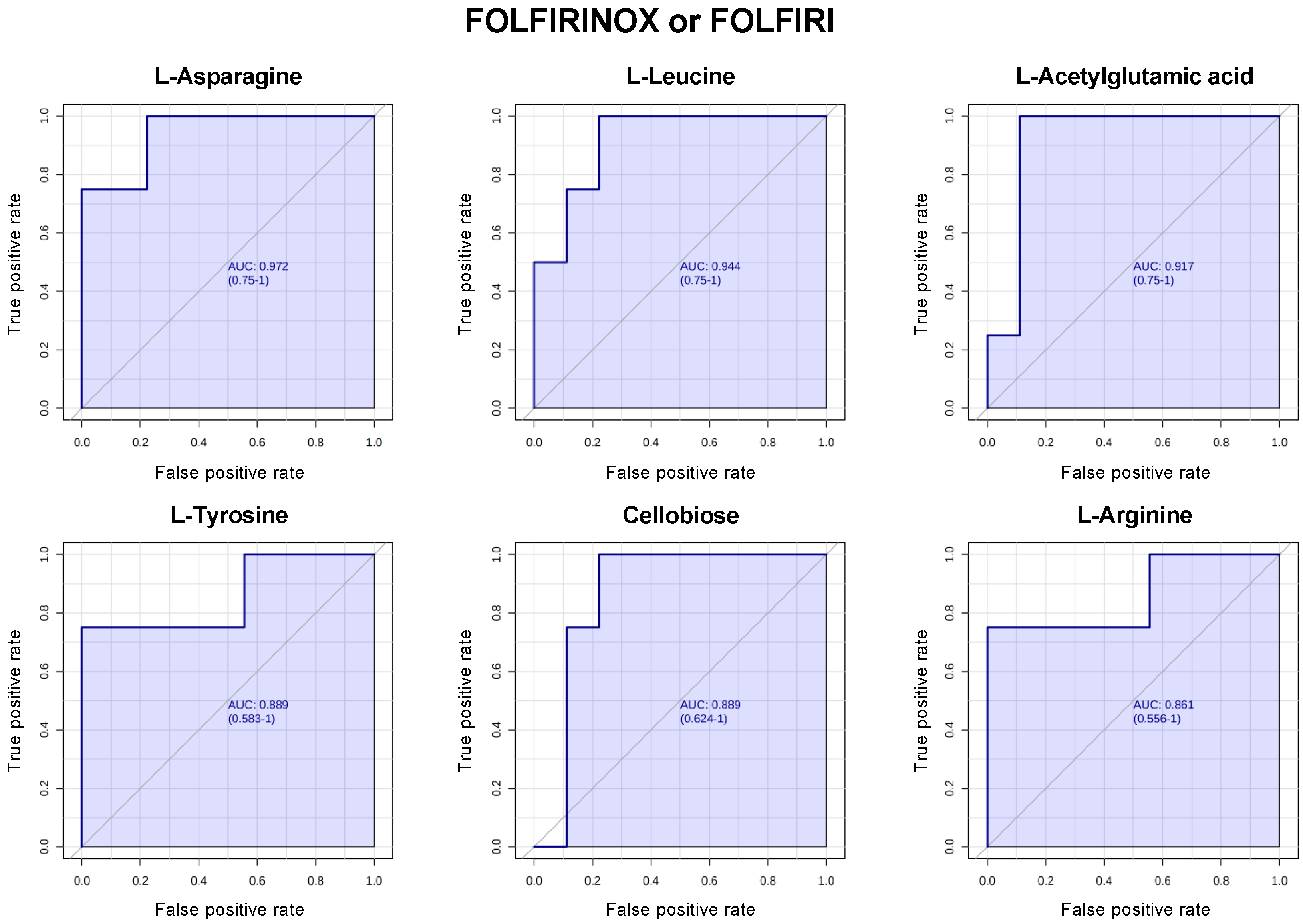
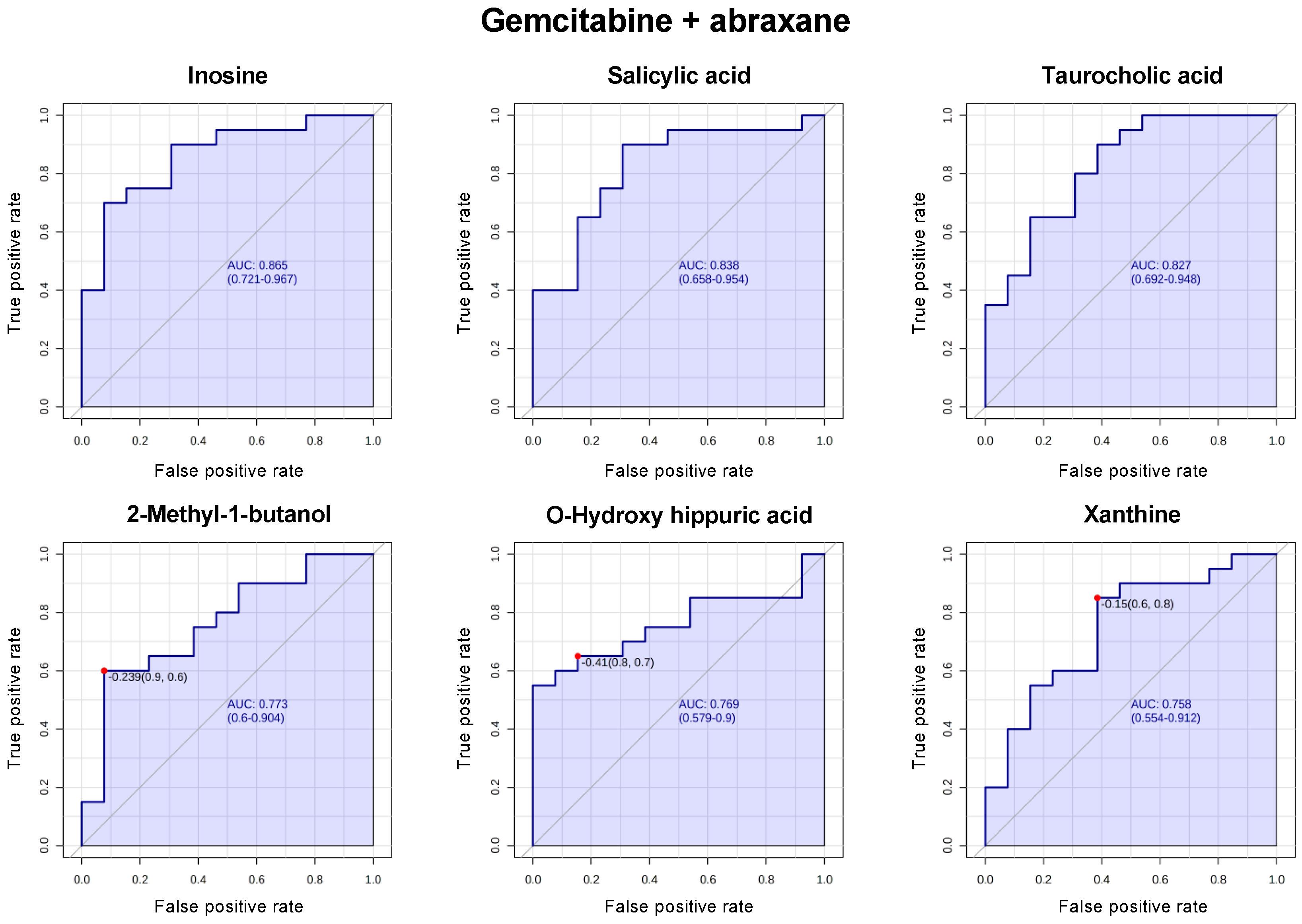
3.4. Biomarkers for the Prediction of a Response to Chemotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Samaan, J.S.; Abboud, Y.; Oh, J.; Jiang, Y.; Watson, R.; Park, K.; Liu, Q.; Atkins, K.; Hendifar, A.; Gong, J.; et al. Pancreatic Cancer Incidence Trends by Race, Ethnicity, Age and Sex in the United States: A Population-Based Study, 2000–2018. Cancers 2023, 15, 870. [Google Scholar] [CrossRef]
- Gong, J.; Tuli, R.; Shinde, A.; Hendifar, A.E. Meta-Analyses of Treatment Standards for Pancreatic Cancer. Mol. Clin. Oncol. 2016, 4, 315–325. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer Statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Hendifar, A.E.; Petzel, M.Q.B.; Zimmers, T.A.; Denlinger, C.S.; Matrisian, L.M.; Picozzi, V.J.; Rahib, L.; Hendifar, A.; Tuli, R.; Wolpin, B.; et al. Pancreas Cancer-Associated Weight Loss. Oncologist 2019, 24, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Aprile, G.; Negri, F.V.; Giuliani, F.; Carlo, E.D.; Melisi, D.; Simionato, F.; Silvestris, N.; Brunetti, O.; Leone, F.; Marino, D.; et al. Second-Line Chemotherapy for Advanced Pancreatic Cancer: Which Is the Best Option? Crit. Rev. Oncol. Hemat. 2017, 115, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D.S. Metabolomics for Investigating Physiological and Pathophysiological Processes. Physiol. Rev. 2019, 99, 1819–1875. [Google Scholar] [CrossRef]
- Qiu, S.; Cai, Y.; Yao, H.; Lin, C.; Xie, Y.; Tang, S.; Zhang, A. Small Molecule Metabolites: Discovery of Biomarkers and Therapeutic Targets. Signal Transduct. Target. Ther. 2023, 8, 132. [Google Scholar] [CrossRef]
- Letertre, M.P.M.; Giraudeau, P.; de Tullio, P. Nuclear Magnetic Resonance Spectroscopy in Clinical Metabolomics and Personalized Medicine: Current Challenges and Perspectives. Front. Mol. Biosci. 2021, 8, 698337. [Google Scholar] [CrossRef]
- Gowda, G.N.; Zhang, S.; Gu, H.; Asiago, V.; Shanaiah, N.; Raftery, D. Metabolomics-Based Methods for Early Disease Diagnostics. Expert Rev. Mol. Diagn. 2008, 8, 617–633. [Google Scholar] [CrossRef]
- Gonzalez-Covarrubias, V.; Martínez-Martínez, E.; del Bosque-Plata, L. The Potential of Metabolomics in Biomedical Applications. Metabolites 2022, 12, 194. [Google Scholar] [CrossRef] [PubMed]
- Clayton, T.A.; Lindon, J.C.; Cloarec, O.; Antti, H.; Charuel, C.; Hanton, G.; Provost, J.-P.; Net, J.-L.L.; Baker, D.; Walley, R.J.; et al. Pharmaco-Metabonomic Phenotyping and Personalized Drug Treatment. Nature 2006, 440, 1073–1077. [Google Scholar] [CrossRef] [PubMed]
- Spratlin, J.L.; Serkova, N.J.; Eckhardt, S.G. Clinical Applications of Metabolomics in Oncology: A Review. Clin. Cancer Res. 2009, 15, 431–440. [Google Scholar] [CrossRef]
- Kamphorst, J.J.; Nofal, M.; Commisso, C.; Hackett, S.R.; Lu, W.; Grabocka, E.; Heiden, M.G.V.; Miller, G.; Drebin, J.A.; Bar-Sagi, D.; et al. Human Pancreatic Cancer Tumors Are Nutrient Poor and Tumor Cells Actively Scavenge Extracellular Protein. Cancer Res. 2015, 75, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Battini, S.; Faitot, F.; Imperiale, A.; Cicek, A.E.; Heimburger, C.; Averous, G.; Bachellier, P.; Namer, I.J. Metabolomics Approaches in Pancreatic Adenocarcinoma: Tumor Metabolism Profiling Predicts Clinical Outcome of Patients. BMC Med. 2017, 15, 56. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Qin, H.; Liu, H.; Wei, T.; Wu, Z.; Shang, M.; Liu, H.; Wang, A.; Liu, J.; Shang, D.; et al. Tissue Metabolomics Identified New Biomarkers for the Diagnosis and Prognosis Prediction of Pancreatic Cancer. Front. Oncol. 2022, 12, 991051. [Google Scholar] [CrossRef]
- Napoli, C.; Sperandio, N.; Lawlor, R.T.; Scarpa, A.; Molinari, H.; Assfalg, M. Urine Metabolic Signature of Pancreatic Ductal Adenocarcinoma by 1H Nuclear Magnetic Resonance: Identification, Mapping, and Evolution. J. Proteome Res. 2012, 11, 1274–1283. [Google Scholar] [CrossRef]
- Davis, V.W.; Schiller, D.E.; Eurich, D.; Bathe, O.F.; Sawyer, M.B. Pancreatic Ductal Adenocarcinoma Is Associated with a Distinct Urinary Metabolomic Signature. Ann. Surg. Oncol. 2013, 20, 415–423. [Google Scholar] [CrossRef]
- Hipperson, L.; Hadden, W.J.; Nahm, C.B.; Gill, A.J.; Samra, J.S.; Dona, A.; Mittal, A.; Sahni, S. Urinary Metabolite Prognostic Biomarker Panel for Pancreatic Ductal Adenocarcinomas. Biochim. Biophys. Acta BBA Gen. Subj. 2021, 1865, 129966. [Google Scholar] [CrossRef]
- Bathe, O.F.; Shaykhutdinov, R.; Kopciuk, K.; Weljie, A.M.; McKay, A.; Sutherland, F.R.; Dixon, E.; Dunse, N.; Sotiropoulos, D.; Vogel, H.J. Feasibility of Identifying Pancreatic Cancer Based on Serum Metabolomics. Cancer Epidemiol. Prev. Biomark. 2011, 20, 140–147. [Google Scholar] [CrossRef]
- Kobayashi, T.; Nishiumi, S.; Ikeda, A.; Yoshie, T.; Sakai, A.; Matsubara, A.; Izumi, Y.; Tsumura, H.; Tsuda, M.; Nishisaki, H.; et al. A Novel Serum Metabolomics-Based Diagnostic Approach to Pancreatic Cancer. Cancer Epidemiol. Prev. Biomark. 2013, 22, 571–579. [Google Scholar] [CrossRef]
- He, X.; Zhong, J.; Wang, S.; Zhou, Y.; Wang, L.; Zhang, Y.; Yuan, Y. Serum Metabolomics Differentiating Pancreatic Cancer from New-Onset Diabetes. Oncotarget 2017, 8, 29116–29124. [Google Scholar] [CrossRef] [PubMed]
- Fest, J.; Vijfhuizen, L.S.; Goeman, J.J.; Veth, O.; Joensuu, A.; Perola, M.; Männistö, S.; Ness-Jensen, E.; Hveem, K.; Haller, T.; et al. Search for Early Pancreatic Cancer Blood Biomarkers in Five European Prospective Population Biobanks Using Metabolomics. Endocrinology 2019, 160, 1731–1742. [Google Scholar] [CrossRef] [PubMed]
- Jiao, L.; Maity, S.; Coarfa, C.; Rajapakshe, K.; Chen, L.; Jin, F.; Putluri, V.; Tinker, L.F.; Mo, Q.; Chen, F.; et al. A Prospective Targeted Serum Metabolomics Study of Pancreatic Cancer in Postmenopausal Women. Cancer Prev. Res. 2019, 12, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Martín-Blázquez, A.; Jiménez-Luna, C.; Díaz, C.; Martínez-Galán, J.; Prados, J.; Vicente, F.; Melguizo, C.; Genilloud, O.; del Palacio, J.P.; Caba, O. Discovery of Pancreatic Adenocarcinoma Biomarkers by Untargeted Metabolomics. Cancers 2020, 12, 1002. [Google Scholar] [CrossRef]
- Xie, G.; Lu, L.; Qiu, Y.; Ni, Q.; Zhang, W.; Gao, Y.-T.; Risch, H.A.; Yu, H.; Jia, W. Plasma Metabolite Biomarkers for the Detection of Pancreatic Cancer. J. Proteome Res. 2015, 14, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Gaiser, R.A.; Pessia, A.; Ateeb, Z.; Davanian, H.; Moro, C.F.; Alkharaan, H.; Healy, K.; Ghazi, S.; Arnelo, U.; Valente, R.; et al. Integrated Targeted Metabolomic and Lipidomic Analysis: A Novel Approach to Classifying Early Cystic Precursors to Invasive Pancreatic Cancer. Sci. Rep.-UK 2019, 9, 10208. [Google Scholar] [CrossRef]
- Mehta, K.Y.; Wu, H.-J.; Menon, S.S.; Fallah, Y.; Zhong, X.; Rizk, N.; Unger, K.; Mapstone, M.; Fiandaca, M.S.; Federoff, H.J.; et al. Metabolomic Biomarkers of Pancreatic Cancer: A Meta-Analysis Study. Oncotarget 2017, 8, 68899–68915. [Google Scholar] [CrossRef]
- Mahajan, U.M.; Alnatsha, A.; Li, Q.; Oehrle, B.; Weiss, F.-U.; Sendler, M.; Distler, M.; Uhl, W.; Fahlbusch, T.; Goni, E.; et al. Plasma Metabolome Profiling Identifies Metabolic Subtypes of Pancreatic Ductal Adenocarcinoma. Cells 2021, 10, 1821. [Google Scholar] [CrossRef]
- Urayama, S. Pancreatic Cancer Early Detection: Expanding Higher-Risk Group with Clinical and Metabolomics Parameters. World J. Gastroenterol. 2015, 21, 1707–1717. [Google Scholar] [CrossRef]
- Tumas, J.; Kvederaviciute, K.; Petrulionis, M.; Kurlinkus, B.; Rimkus, A.; Sakalauskaite, G.; Cicenas, J.; Sileikis, A. Metabolomics in Pancreatic Cancer Biomarkers Research. Med. Oncol. 2016, 33, 133. [Google Scholar] [CrossRef]
- Gu, W.; Tong, Z. Clinical Application of Metabolomics in Pancreatic Diseases: A Mini-Review. Lab. Med. 2019, 51, 116–121. [Google Scholar] [CrossRef]
- Gresham, G.; Placencio-Hickok, V.R.; Lauzon, M.; Nguyen, T.; Kim, H.; Mehta, S.; Paski, S.; Pandol, S.J.; Osipov, A.; Gong, J.; et al. Feasibility and Efficacy of Enteral Tube Feeding on Weight Stability, Lean Body Mass, and Patient-reported Outcomes in Pancreatic Cancer Cachexia. J. Cachexia Sarcopenia Muscle 2021, 12, 1959–1968. [Google Scholar] [CrossRef]
- Gong, J.; Osipov, A.; Lorber, J.; Tighiouart, M.; Kwan, A.K.; Muranaka, H.; Akinsola, R.; Billet, S.; Levi, A.; Abbas, A.; et al. Combination l-Glutamine with Gemcitabine and Nab-Paclitaxel in Treatment-Naïve Advanced Pancreatic Cancer: The Phase I GlutaPanc Study Protocol. Biomedicines 2023, 11, 1392. [Google Scholar] [CrossRef] [PubMed]
- Encarnación-Rosado, J.; Kimmelman, A.C. Harnessing Metabolic Dependencies in Pancreatic Cancers. Nat. Rev. Gastroenterol. 2021, 18, 482–492. [Google Scholar] [CrossRef]
- Trottier, J.; Białek, A.; Caron, P.; Straka, R.J.; Milkiewicz, P.; Barbier, O. Profiling Circulating and Urinary Bile Acids in Patients with Biliary Obstruction before and after Biliary Stenting. PLoS ONE 2011, 6, e22094. [Google Scholar] [CrossRef]
- Gál, E.; Veréb, Z.; Kemény, L.; Rakk, D.; Szekeres, A.; Becskeházi, E.; Tiszlavicz, L.; Takács, T.; Czakó, L.; Hegyi, P.; et al. Bile Accelerates Carcinogenic Processes in Pancreatic Ductal Adenocarcinoma Cells through the Overexpression of MUC4. Sci. Rep.-UK 2020, 10, 22088. [Google Scholar] [CrossRef] [PubMed]
- Santana-Codina, N.; Roeth, A.A.; Zhang, Y.; Yang, A.; Mashadova, O.; Asara, J.M.; Wang, X.; Bronson, R.T.; Lyssiotis, C.A.; Ying, H.; et al. Oncogenic KRAS Supports Pancreatic Cancer through Regulation of Nucleotide Synthesis. Nat. Commun. 2018, 9, 4945. [Google Scholar] [CrossRef]
- Xu, R.; Yang, J.; Ren, B.; Wang, H.; Yang, G.; Chen, Y.; You, L.; Zhao, Y. Reprogramming of Amino Acid Metabolism in Pancreatic Cancer: Recent Advances and Therapeutic Strategies. Front. Oncol. 2020, 10, 572722. [Google Scholar] [CrossRef] [PubMed]
- Dufour, E.; Gay, F.; Aguera, K.; Scoazec, J.-Y.; Horand, F.; Lorenzi, P.L.; Godfrin, Y. Pancreatic Tumor Sensitivity to Plasma l-Asparagine Starvation. Pancreas 2012, 41, 940–948. [Google Scholar] [CrossRef]
- Ragni, M.; Fornelli, C.; Nisoli, E.; Penna, F. Amino Acids in Cancer and Cachexia: An Integrated View. Cancers 2022, 14, 5691. [Google Scholar] [CrossRef]
- Ying, H.; Kimmelman, A.C.; Lyssiotis, C.A.; Hua, S.; Chu, G.C.; Fletcher-Sananikone, E.; Locasale, J.W.; Son, J.; Zhang, H.; Coloff, J.L.; et al. Oncogenic Kras Maintains Pancreatic Tumors through Regulation of Anabolic Glucose Metabolism. Cell 2012, 149, 656–670. [Google Scholar] [CrossRef] [PubMed]
- Bryant, K.L.; Mancias, J.D.; Kimmelman, A.C.; Der, C.J. KRAS: Feeding Pancreatic Cancer Proliferation. Trends Biochem. Sci. 2014, 39, 91–100. [Google Scholar] [CrossRef]
- Petruzzelli, M.; Wagner, E.F. Mechanisms of Metabolic Dysfunction in Cancer-Associated Cachexia. Gene Dev. 2016, 30, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Soom, T.V.; Bakkali, S.E.; Gebruers, N.; Verbelen, H.; Tjalma, W.; van Breda, E. The Effects of Chemotherapy on Energy Metabolic Aspects in Cancer Patients: A Systematic Review. Clin. Nutr. 2020, 39, 1863–1877. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N (%) or Mean |
|---|---|
| Total patients | 31 |
| Age | 67.1 years old |
| Gender | |
| Male | 12 (38.7) |
| Female | 19 (61.3) |
| Race/ethnicity * | |
| Non-Hispanic White | 19 (61.3) |
| African American | 2 (6.4) |
| Asian/Pacific Islander | 7 (22.6) |
| Hispanic/Latino | 7 (22.6) |
| Other | 2 (6.4) |
| Not reported | 1 (3.2) |
| Line of treatment | |
| First | 22 (71.0) |
| Second | 8 (25.8) |
| Third | 1 (3.2) |
| CTX regimen | |
| None | 4 (12.9) |
| Gemcitabine-based | 19 (61.3) |
| Gemcitabine + abraxane | 17 (54.8) |
| Gemcitabine + abraxane + peg-hyaluronidase | 1 (3.2) |
| Gemcitabine | 1 (3.2) |
| 5-fluorouracil-based | 8 (25.8) |
| FOLFIRINOX | 2 (6.4) |
| FOLFRI | 4 (12.9) |
| 5-FU + Oniyvde + anti-Ilα | 2 (6.4) |
| Best response to CTX | |
| N/A | 4 (12.9) |
| PR | 2 (6.4) |
| SD | 10 (35.3) |
| PD | 15 (48.4) |
| Median OS | 6.53 months |
| None | 4.75 months |
| Gemcitabine-based | 8.83 months |
| 5-fluorouracil-based | 5.48 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muranaka, H.; Hendifar, A.; Osipov, A.; Moshayedi, N.; Placencio-Hickok, V.; Tatonetti, N.; Stotland, A.; Parker, S.; Van Eyk, J.; Pandol, S.J.; et al. Plasma Metabolomics Predicts Chemotherapy Response in Advanced Pancreatic Cancer. Cancers 2023, 15, 3020. https://doi.org/10.3390/cancers15113020
Muranaka H, Hendifar A, Osipov A, Moshayedi N, Placencio-Hickok V, Tatonetti N, Stotland A, Parker S, Van Eyk J, Pandol SJ, et al. Plasma Metabolomics Predicts Chemotherapy Response in Advanced Pancreatic Cancer. Cancers. 2023; 15(11):3020. https://doi.org/10.3390/cancers15113020
Chicago/Turabian StyleMuranaka, Hayato, Andrew Hendifar, Arsen Osipov, Natalie Moshayedi, Veronica Placencio-Hickok, Nicholas Tatonetti, Aleksandr Stotland, Sarah Parker, Jennifer Van Eyk, Stephen J. Pandol, and et al. 2023. "Plasma Metabolomics Predicts Chemotherapy Response in Advanced Pancreatic Cancer" Cancers 15, no. 11: 3020. https://doi.org/10.3390/cancers15113020