

Efficacy of Tango Argentino for Cancer-Associated Fatigue and Quality of Life in Breast Cancer Survivors: A Randomized Controlled Trial
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
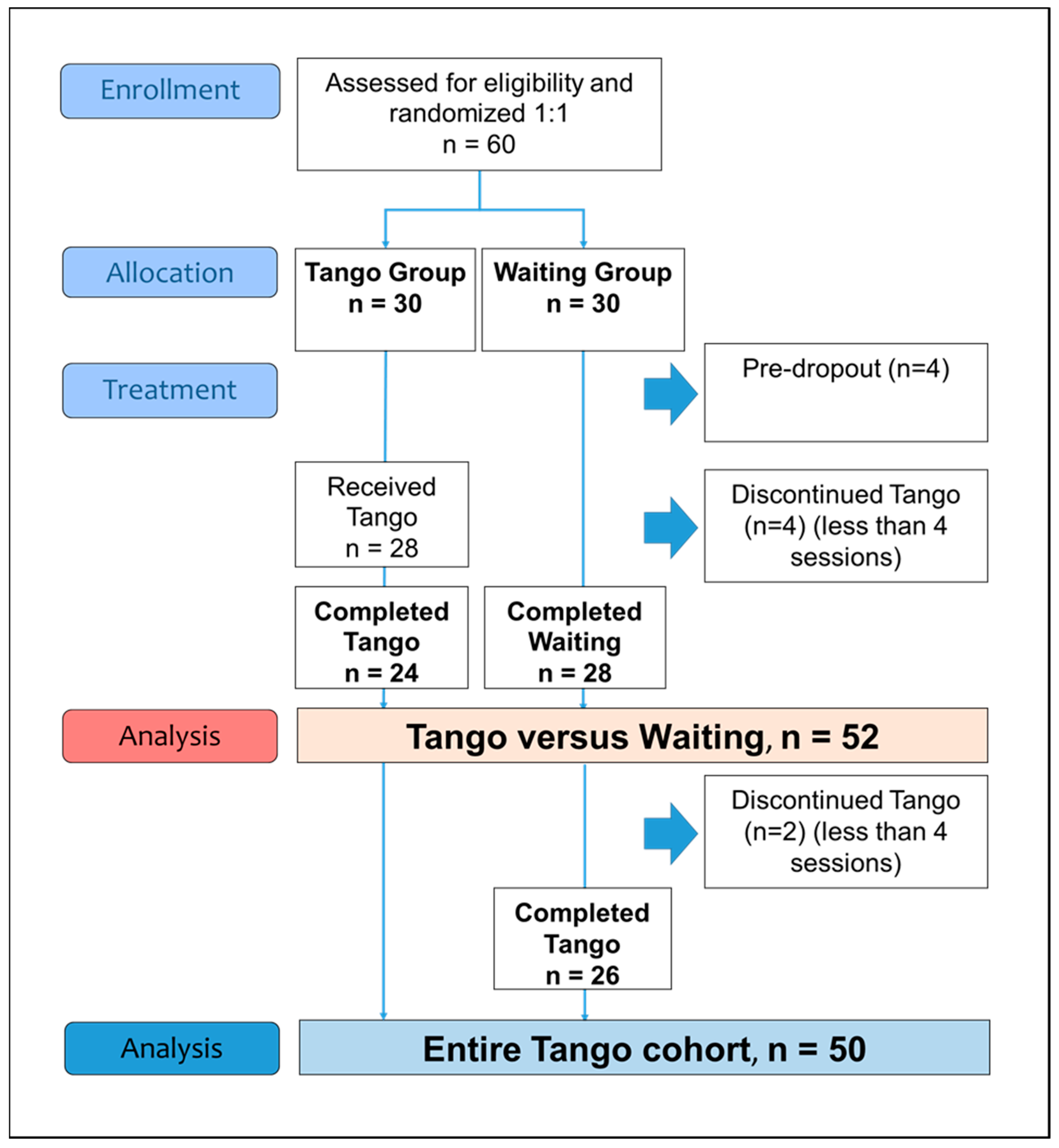
2.1. Participants, Study Design, and Procedure
2.2. Intervention
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
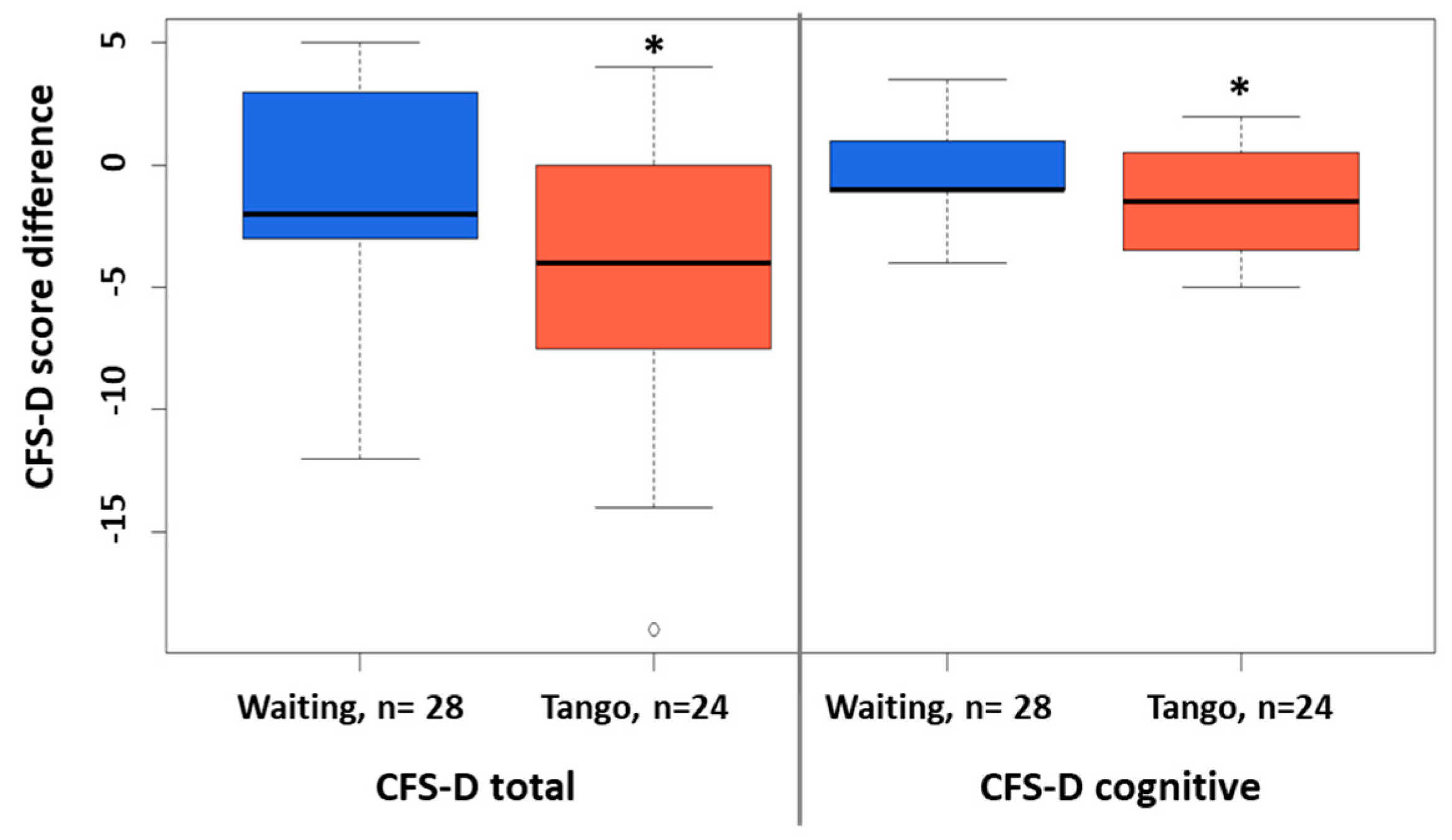
3.1. Group Comparisons
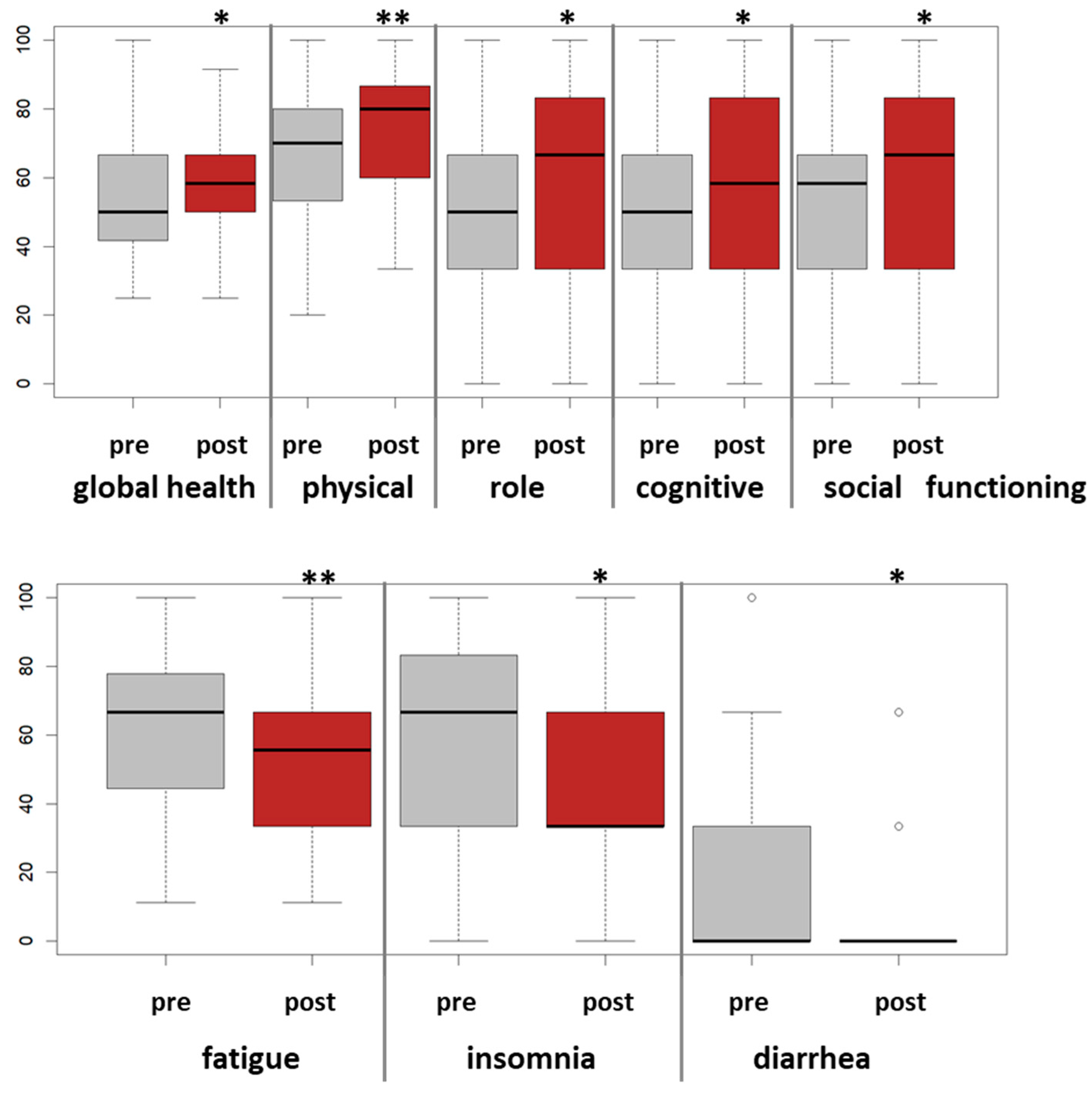
3.2. Pre-Postanalyses
3.3. Safety and Dropout
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Bower, J.E.; Ganz, P.A.; Desmond, K.A.; Bernaards, C.; Rowland, J.H.; Meyerowitz, B.E.; Belin, T.R. Fatigue in long-term breast carcinoma survivors: A longitudinal investigation. Cancer 2006, 106, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Fabi, A.; Falcicchio, C.; Giannarelli, D.; Maggi, G.; Cognetti, F.; Pugliese, P. The course of cancer related fatigue up to ten years in early breast cancer patients: What impact in clinical practice? Breast 2017, 34, 44–52. [Google Scholar] [CrossRef]
- Cella, D.; Peterman, A.; Passik, S.; Jacobsen, P.; Breitbart, W. Progress toward guidelines for the management of fatigue. Oncology 1998, 12, 369–377. [Google Scholar] [PubMed]
- Bower, J.E. Cancer-related fatigue—Mechanisms, risk factors, and treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef]
- Abrahams, H.J.G.; Gielissen, M.F.M.; Schmits, I.C.; Verhagen, C.; Rovers, M.M.; Knoop, H. Risk factors, prevalence, and course of severe fatigue after breast cancer treatment: A meta-analysis involving 12 327 breast cancer survivors. Ann. Oncol. 2016, 27, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Carmichael, A.R. Physical activity for women with breast cancer after adjuvant therapy. Cochrane Database Syst. Rev. 2018, 1, CD011292. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari-Hessari, P.; Montazeri, A. Health-related quality of life in breast cancer patients: Review of reviews from 2008 to 2018. Health Qual. Life Outcomes 2020, 18, 338. [Google Scholar] [CrossRef]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef]
- Torres, D.M.; Koifman, R.J.; Santos, S.D.S. Impact on fatigue of different types of physical exercise during adjuvant chemotherapy and radiotherapy in breast cancer: Systematic review and meta-analysis. Support. Care Cancer Care Cancer 2022, 30, 4651–4662. [Google Scholar] [CrossRef]
- Greenlee, H.; DuPont-Reyes, M.J.; Rn, L.G.B.; Carlson, L.E.; Cohen, M.R.; Deng, G.; Johnson, J.A.; Mumber, M.; Seely, D.; Zick, S.M.; et al. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J. Clin. 2017, 67, 194–232. [Google Scholar] [CrossRef]
- Bradt, J.; Dileo, C.; Magill, L.; Teague, A. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst. Rev. 2016, 8, CD006911. [Google Scholar] [CrossRef] [PubMed]
- Sturm, I.; Baak, J.; Storek, B.; Traore, A.; Thuss-Patience, P. Effect of dance on cancer-related fatigue and quality of life. Support. Care Cancer 2014, 22, 2241–2249. [Google Scholar] [CrossRef]
- Cillessen, L.; Johannsen, M.; Speckens, A.E.; Zachariae, R. Mindfulness-based interventions for psychological and physical health outcomes in cancer patients and survivors: A systematic review and meta-analysis of randomized controlled trials. Psycho-Oncology 2019, 28, 2257–2269. [Google Scholar] [CrossRef]
- Sun, H.; Huang, H.; Ji, S.; Chen, X.; Xu, Y.; Zhu, F.; Wu, J. The Efficacy of Cognitive Behavioral Therapy to Treat Depression and Anxiety and Improve Quality of Life Among Early-Stage Breast Cancer Patients. Integr. Cancer Ther. 2019, 18, 1534735419829573. [Google Scholar] [CrossRef] [PubMed]
- Xunlin, N.; Lau, Y.; Klainin-Yobas, P. The effectiveness of mindfulness-based interventions among cancer patients and survivors: A systematic review and meta-analysis. Support. Care Cancer 2020, 28, 1563–1578. [Google Scholar] [CrossRef] [PubMed]
- Kaltsatou, A.; Mameletzi, D.; Douka, S. Physical and psychological benefits of a 24-week traditional dance program in breast cancer survivors. J. Bodyw. Mov. Ther. 2011, 15, 162–167. [Google Scholar] [CrossRef]
- Koch, S.C.; Riege, R.F.F.; Tisborn, K.; Biondo, J.; Martin, L.; Beelmann, A. Effects of Dance Movement Therapy and Dance on Health-Related Psychological Outcomes. A Meta-Analysis Update. Front. Psychol. 2019, 10, 1806. [Google Scholar] [CrossRef]
- Frikkel, J.; Götte, M.; Beckmann, M.; Kasper, S.; Hense, J.; Teufel, M.; Schuler, M.; Tewes, M. Fatigue, barriers to physical activity and predictors for motivation to exercise in advanced Cancer patients. BMC Palliat. Care 2020, 19, 43. [Google Scholar] [CrossRef]
- Hohmann, L.; Bradt, J.; Stegemann, T.; Koelsch, S. Effects of music therapy and music-based interventions in the treatment of substance use disorders: A systematic review. PLoS ONE 2017, 12, e0187363. [Google Scholar] [CrossRef]
- Karkou, V.; Dudley-Swarbrick, I.; Starkey, J.; Parsons, A.; Aithal, S.; Omylinska-Thurston, J.; Verkooijen, H.M.; Boogaard, R.v.D.; Dochevska, Y.; Djobova, S.; et al. Dancing with Health: Quality of Life and Physical Improvements from an EU Collaborative Dance Programme with Women Following Breast Cancer Treatment. Front. Psychol. 2021, 12, 635578. [Google Scholar] [CrossRef] [PubMed]
- Lötzke, D.; Ostermann, T.; Büssing, A. Argentine tango in Parkinson disease—A systematic review and meta-analysis. BMC Neurol. 2015, 15, 226. [Google Scholar] [CrossRef] [PubMed]
- Worthen-Chaudhari, L.; Lamantia, M.; Monfort, S.; Mysiw, W.; Chaudhari, A.; Lustberg, M. Partnered, adapted argentine tango dance for cancer survivors: A feasibility study and pilot study of efficacy. Clin. Biomech. 2019, 70, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Oei, S.L.; Rieser, T.; Becker, S.; Groß, J.; Matthes, H.; Schad, F.; Thronicke, A. TANGO: Effect of tango Argentino on cancer-associated fatigue in breast cancer patients—Study protocol for a randomized controlled trial. Trials 2021, 22, 866. [Google Scholar] [CrossRef]
- Kröz, M.; Zerm, R.; Reif, M.; VON Laue, H.; Schad, F.; Büssing, A.; Bartsch, C.; Feder, G.; Girke, M. Validation of the German version of the Cancer Fatigue Scale (CFS-D). Eur. J. Cancer Care 2008, 17, 33–41. [Google Scholar] [CrossRef]
- Twomey, R.; Yeung, S.T.; Wrightson, J.G.; Millet, G.Y.; Culos-Reed, S.N. Post-exertional Malaise in People with Chronic Cancer-Related Fatigue. J. Pain Symptom Manag. 2020, 60, 407–416. [Google Scholar] [CrossRef]
- Hackney, M.E.; Earhart, G.M. Recommendations for Implementing Tango Classes for Persons with Parkinson Disease. Am. J. Dance Ther. 2010, 32, 41–52. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; De Haes, J.C.J.M.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. JNCI J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Twomey, R.; Yeung, S.; Wrightson, J.G.; Sung, L.; Robinson, P.D.; Millet, G.Y.; Culos-Reed, S.N. Physical Activity in Adults With Fatigue After Cancer Treatment. Commun. Kinesiol. 2021, 1, 1–20. [Google Scholar] [CrossRef]
- Van Vulpen, J.K.; Sweegers, M.G.; Peeters, P.H.M.; Courneya, K.S.; Newton, R.U.; Aaronson, N.K.; Jacobsen, P.B.; Galvão, D.A.; Chinapaw, M.J.; Steindorf, K.; et al. Moderators of Exercise Effects on Cancer-related Fatigue: A Meta-analysis of Individual Patient Data. Med. Sci. Sports Exerc. 2020, 52, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Savard, J.; Simard, S.; Ivers, H.; Morin, C.M. Randomized Study on the Efficacy of Cognitive-Behavioral Therapy for Insomnia Secondary to Breast Cancer, Part I: Sleep and Psychological Effects. J. Clin. Oncol. 2005, 23, 6083–6096. [Google Scholar] [CrossRef] [PubMed]
- Boing, L.; Fretta, T.D.B.; Lynch, B.M.; Dias, M.; da Rosa, L.M.; Baptista, F.; Bergmann, A.; Fausto, D.Y.; Martins, J.B.B.; Guimarães, A.C.D.A. Mat Pilates and belly dance: Effects on patient-reported outcomes among breast cancer survivors receiving hormone therapy and adherence to exercise. Complement. Ther. Clin. Pr. 2023, 50, 101683. [Google Scholar] [CrossRef]
- Cruz, E.I.d.S.; Cruz, A.H.D.S.; Ventura, J.A.; Marques, R.A.S.; Santos, R.D.S.; Reis, A.A.D.S. The impact of dance as a non-pharmacological adjuvant therapy cancer survivors: A clinical trial. Res. Soc. Dev. 2022, 11, e14411729714. [Google Scholar] [CrossRef]
- Peterson, L.L.; Ligibel, J.A. Physical Activity and Breast Cancer: An Opportunity to Improve Outcomes. Curr. Oncol. Rep. 2018, 20, 50. [Google Scholar] [CrossRef] [PubMed]
- Van Dijck, S.; Nelissen, P.; Verbelen, H.; Tjalma, W.; Gebruers, N. The effects of physical self-management on quality of life in breast cancer patients: A systematic review. Breast 2016, 28, 20–28. [Google Scholar] [CrossRef]
- Lipsett, A.; Barrett, S.; Haruna, F.; Mustian, K.; O’Donovan, A. The impact of exercise during adjuvant radiotherapy for breast cancer on fatigue and quality of life: A systematic review and meta-analysis. Breast 2017, 32, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Fabi, A.; Bhargava, R.; Fatigoni, S.; Guglielmo, M.; Horneber, M.; Roila, F.; Weis, J.; Jordan, K.; Ripamonti, C. Cancer-related fatigue: ESMO Clinical Practice Guidelines for diagnosis and treatment. Ann. Oncol. 2020, 31, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Greenlee, H.; Bohlke, K.; Bao, T.; DeMichele, A.M.; Deng, G.E.; Fouladbakhsh, J.M.; Gil, B.; Hershman, D.L.; Mansfield, S.; et al. Integrative Therapies During and After Breast Cancer Treatment: ASCO Endorsement of the SIO Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 2647–2655. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.; Pan, H.; Godwin, J.; Gray, R.; Arriagada, R.; Raina, V.; Abraham, M.; Medeiros Alencar, V.H.; Badran, A.; Bonfill, X.; et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013, 381, 805–816. [Google Scholar] [CrossRef]
- Mausbach, B.T.; Schwab, R.B.; Irwin, S.A. Depression as a predictor of adherence to adjuvant endocrine therapy (AET) in women with breast cancer: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2015, 152, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Schilder, C.M.T.; Seynaeve, C.; Linn, S.C.; Boogerd, W.; Beex, L.V.A.M.; Gundy, C.M.; Nortier, J.W.R.; Van De Velde, C.J.H.; Van Dam, F.S.A.M.; Schagen, S.B. Self-reported cognitive functioning in postmenopausal breast cancer patients before and during endocrine treatment: Findings from the neuropsychological TEAM side-study. Psycho-Oncology 2012, 21, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Haggstrom, L.R.; Vardy, J.L.; Carson, E.-K.; Segara, D.; Lim, E.; Kiely, B.E. Effects of Endocrine Therapy on Cognitive Function in Patients with Breast Cancer: A Comprehensive Review. Cancers 2022, 14, 920. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Shao, T.; Kushi, L.H.; Buono, D.; Tsai, W.Y.; Fehrenbacher, L.; Kwan, M.; Gomez, S.L.; Neugut, A.I. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res. Treat. 2011, 126, 529–537. [Google Scholar] [CrossRef]
- Joly, F.; Lange, M.; Dos Santos, M.; Vaz-Luis, I.; Di Meglio, A. Long-Term Fatigue and Cognitive Disorders in Breast Cancer Survivors. Cancers 2019, 11, 1896. [Google Scholar] [CrossRef]
- Oberste, M.; Schaffrath, N.; Schmidt, K.; Bloch, W.; Jäger, E.; Steindorf, K.; Hartig, P.; Joisten, N.; Zimmer, P. Protocol for the “Chemobrain in Motion—Study” (CIM—Study): A randomized placebo-controlled trial of the impact of a high-intensity interval endurance training on cancer related cognitive impairments in women with breast cancer receiving first-line chemotherapy. BMC Cancer 2018, 18, 1071. [Google Scholar] [CrossRef]
- Lange, M.; Joly, F.; Vardy, J.; Ahles, T.; Dubois, M.; Tron, L.; Winocur, G.; De Ruiter, M.; Castel, H. Cancer-related cognitive impairment: An update on state of the art, detection, and management strategies in cancer survivors. Ann. Oncol. 2019, 30, 1925–1940. [Google Scholar] [CrossRef]
- Oei, S.L.; Thronicke, A.; Kröz, M.; von Trott, P.; Schad, F.; Matthes, H. Impact of Oncological Therapy and Viscum album L Treatment on Cancer-Related Fatigue and Internal Coherence in Nonmetastasized Breast Cancer Patients. Integr. Cancer Ther. 2020, 19, 1534735420917211. [Google Scholar] [CrossRef]
- Witkoś, J.; Hartman-Petrycka, M. Implications of Argentine Tango for Health Promotion, Physical Well-Being as Well as Emotional, Personal and Social Life on a Group of Women Who Dance. Int. J. Environ. Res. Public Health 2021, 18, 5894. [Google Scholar] [CrossRef]
- Sodergren, S.C.; Copson, E.; White, A.; Efficace, F.; Sprangers, M.; Fitzsimmons, D.; Bottomley, A.; Johnson, C.D. Systematic Review of the Side Effects Associated with Anti-HER2-Targeted Therapies Used in the Treatment of Breast Cancer, on Behalf of the EORTC Quality of Life Group. Target. Oncol. 2016, 11, 277–292. [Google Scholar] [CrossRef]
- McKee, K.E.; Hackney, M.E. The Effects of Adapted Tango on Spatial Cognition and Disease Severity in Parkinson’s Disease. J. Mot. Behav. 2013, 45, 519–529. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total | Waiting | Tango | p-Value | |
|---|---|---|---|---|
| Number of patients, n (%) | 60 (100) | 30 (100) | 30 (100) | |
| Age, years, mean (SD) | 60.5 (10.3) | 59.3 (11.0) | 61.7 (9.4) | 0.377 |
| Body mass index (BMI) | ||||
| Normal (18.5 ≤ BMI < 25) | 39 (65) | 21 (70) | 18 (60) | |
| Overweight (25 ≤ BMI < 30) | 13 (22) | 6 (20) | 7 (23) | 0.668 |
| Obese (BMI ≥ 30) | 8 (13) | 3 (10) | 5 (17) | |
| Currently employed, n (%) | 23 (38) | 12 (40) | 11 (37) | 1 |
| Living in partnership, n (%) | 39 (65) | 19 (63) | 20 (67) | 1 |
| Years since first diagnosis: mean (SD) | 1.7 (0.7) | 1.7 (0.7) | 1.6 (0.6) | 0.614 |
| UICC stages, n (%) | ||||
| I | 28 (47) | 12 (40) | 16 (53) | |
| II | 23 (38) | 14 (47) | 9 (30) | 0.413 |
| III | 9 (15) | 4 (13) | 5 (17) | |
| Hormonal status, n (%) | ||||
| Premenopausal | 3 (5) | 3 (10) | 0 | |
| Postmenopausal | 57 (95) | 27 (90) | 30 (100) | 0.236 |
| Triple-negative status, n (%) | 6 (10) | 2 (7) | 4 (13) | 0.667 |
| Oncological Interventions, n (%) | ||||
| Surgery | 60 (100) | 30 (100) | 30 (100) | 1 |
| Radiation | 52 (87) | 25 (83) | 27 (90) | 0.704 |
| Endocrine therapy | 39 (65) | 21 (70) | 18 (60) | 0.588 |
| Chemotherapy | 31 (52) | 16 (53) | 15 (50) | 1 |
| Immunotherapy | 6 (10) | 3 (10) | 3 (10) | 1 |
| Sportive activities, n (%) | ||||
| No | 9 (15) | 5 (17) | 4 (13) | |
| Occasionally | 13 (22) | 4 (13) | 9 (30) | 0.293 |
| Regularly | 38 (64) | 21 (70) | 17 (57) | |
| Dance experience, n (%) | ||||
| No | 19 (32) | 12 (40) | 7 (23) | |
| Yes, in the past | 38 (63) | 16 (53) | 22 (73) | 0.273 |
| Yes, current | 3 (5) | 2 (7) | 1 (3) | |
| CFS-D | ||||
| Total fatigue score, mean (SD) | 32.2 (9.0) | 33.7 (7.6) | 30.6 (10.0) | 0.195 |
| Physical fatigue, mean (SD) | 14.1 (4.1) | 14.9 (3.8) | 13.3 (4.2) | 0.109 |
| Affective fatigue, mean (SD) | 6.9 (2.6) | 7.3 (2.2) | 6.4 (2.8) | 0.196 |
| Cognitive fatigue, mean (SD) | 11.2 (3.5) | 11.4 (3.0) | 10.9 (4.0) | 0.605 |
| Tango, n = 24 | Waiting, n = 28 | Tango vs. Waiting | ||||
|---|---|---|---|---|---|---|
| dmean (SD) | p-Value | dmean (SD) | p-Value | p-Value | d [95% CI] | |
| CFS-D-total | −4.4 (5.4) | 0.001 * | −1.3 (4.4) | 0.14 | 0.03 * | −0.64 [−1.2; −0.08] |
| Physical fatigue | −1.9 (2.5) | 0.002 * | −0.78 (2.6) | 0.14 | 0.13 | −0.43 [−1.0; 0.12] |
| Affective fatigue | −1.0 (2.4) | 0.052 | −0.3 (1.3) | 0.32 | 0.15 | −0.42 [−1.0; 0.14] |
| Cognitive fatigue | −1.5 (2.2) | 0.004 * | −0.3 (1.8) | 0.44 | 0.03 * | −0.62 [−1.2; −0.06] |
| PSQI-total | −0.8 (2.5) | 0.16 | −0.8 (2.3) | 0.08 | 0.96 | 0.02 [−0.54; 0.57] |
| Sleep latency | −0.3 (0.8) | 0.04 * | −0.1 (0.8) | 0.36 | 0.39 | −0.25 [−0.79; 0.30] |
| Daytime sleepiness | −0.3 (0.5) | 0.03 * | −0.04 (0.6) | 0.75 | 0.16 | −0.41 [−0.97; 0.15] |
| EORTC QLQ C30 | ||||||
| Global health | 4.7 (16.2) | 0.18 | −1.9 (11.0) | 0.40 | 0.10 | 0.48 [−0.08; 1.03] |
| Physical functioning | 3.3 (12.3) | 0.21 | −4.1 (17.8) | 0.25 | 0.09 | 0.48 [−0.08; 1.03] |
| Cognitive functioning | 6.9 (17.3) | 0.07 | 0.6 (20.7) | 0.88 | 0.25 | 0.33 [−0.22; 0.88] |
| Social functioning | 14.9 (27.0) | 0.01 * | 3.6 (28.3) | 0.52 | 0.16 | 0.41 [−0.14; 0.96] |
| Appetite loss | 0.0 (16.7) | 1 | 8.3 (21.1) | 0.05 * | 0.13 | −0.43 [−0.98; −0.12] |
| Diarrhea | −8.3 (19.8) | 0.06 | 7.1 (24.2) | 0.14 | 0.02 * | −0.69 [−1.25; −0.13] |
| n = 50 | dmean | SD | p-Value |
|---|---|---|---|
| CFS-D-total | −3.6 | 5.8 | 0.01 * |
| Physical fatigue | −1.6 | 2.8 | 0.02 * |
| Affective fatigue | −1.0 | 2.3 | 0.06 * |
| Cognitive fatigue | −1.1 | 2.3 | 0.002 * |
| PSQI-total | −0.9 | 2.7 | 0.03 * |
| Daytime sleepiness | −0.2 | 0.6 | 0.02 * |
| EORTC QLQ-C30 | |||
| Global health status | 5.7 | 15.6 | 0.02 * |
| Physical functioning | 6.9 | 14.3 | 0.001 * |
| Role functioning | 8.2 | 25.9 | 0.03 * |
| Cognitive functioning | 6.3 | 19.7 | 0.03 * |
| Social functioning | 9.2 | 27.6 | 0.02 * |
| Fatigue | −9.8 | 17.5 | 0.0003 * |
| Insomnia | −10.2 | 25.6 | 0.008 * |
| Diarrhea | −8.7 | 23.9 | 0.01 * |
| CFS-D, n = 50 | Total | Physical Fatigue | Cognitive Fatigue | Affective Fatigue | |
|---|---|---|---|---|---|
| Adjusted for | age, cancer stage, T0-value, and menopausal status | ||||
| Endocrine therapy | −6.825 * | −7.725 * | −6.513 | −7.119 + | |
| Reference BMI normal | |||||
| BMI overweight | 2.350 | 0.900 | 3.159 | 5.239 | |
| BMI obese | −7.391 | −12.882 * | −5.695 | −6.478 | |
| Sports | −3.711 * | −4.732 * | −3.760 + | −3.234 | |
| Dance experience | 6.781 * | 6.890 * | 6.390+ | 6.930+ | |
| EORTC QLQ C30, n = 50 | QL | PF | EF | CF | FA |
| Adjusted for | age, cancer stage, T0-value, and menopausal status | ||||
| Endocrine therapy | −2.847 | −1.894 | 3.242 | 3.315 | −2.367 |
| Reference BMI normal | |||||
| BMI overweight | −0.940 | 0.624 | 5.318 | 8.703 | 5.516 |
| BMI obese | 3.106 | 12.775 + | 27.671 ** | 14.755 | −6.873 |
| Sports | 4.353 + | 0.941 | 3.609 | 8.44 0 ** | −5.485 * |
| Dance experience | −5.071 | 1.091 | −9.575+ | −15.511 ** | 13.107 ** |
| n = 56 | Completed Tango (89%) | Discontinued Tango (11%) | p-Value |
|---|---|---|---|
| Number of patients, n (%) | 50 (100) | 6 (100) | |
| Age, years, mean (SD) | 61.3 (9.9) | 60.5 (12.2) | 0.855 |
| Body mass index (BMI) | |||
| Normal (18.5 ≤ BMI < 25) | 36 (72) | 2 (33) | |
| Overweight (25 ≤ BMI < 30) | 10 (20) | 1 (17) | 0.012 * |
| Obese (BMI ≥ 30) | 4 (8) | 3 (50) | |
| Living in partnership, n (%) | 31 (62) | 5 (83) | 0.562 |
| Years since first diagnosis: mean (SD) | 1.7 (0.7) | 1.4 (0.1) | 0.328 |
| UICC stages, n (%) | |||
| I | 23 (46) | 2 (33) | |
| II | 20 (40) | 2 (33) | 0.473 |
| III | 7 (14) | 2 (33) | |
| Hormonal status, n (%) | |||
| Premenopausal | 2 (4) | 0 | |
| Postmenopausal | 48 (96) | 6 (100) | 1 |
| Triple-negative status, n (%) | 4 (8) | 2 (33) | 0.231 |
| Interventions, n (%) | |||
| Surgery | 50 (100) | 6 (100) | 1 |
| Radiation | 46 (92) | 5 (83) | 1 |
| Endocrine therapy | 34 (68) | 4 (67) | 1 |
| Chemotherapy | 24 (48) | 6 (100) | 0.048 * |
| Immunotherapy | 6 (12) | 0 | 0.841 |
| Sport activities, n (%) | |||
| No | 8 (16) | 1 (17) | |
| Occasionally | 11 (22) | 1 (17) | 0.955 |
| Regularly | 31 (62) | 4 (67) | |
| Dance experience, n (%) | |||
| No | 16 (32) | 1 (17) | |
| Yes, in the past | 32 (64) | 4 (67) | 0.363 |
| Yes, current | 2 (4) | 1 (17) | |
| QoL assessment at baseline | |||
| CFS-D total, mean (SD) | 31.01 (9.26) | 37.00 (5.23) | 0.133 |
| PSQI total, mean (SD) | 9.55 (3.43) | 11.50 (4.99) | 0.229 |
| EORTC QLQ C30 Global health, mean (SD) | 54.42 (16.84) | 51.67 (20.00) | 0.739 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schad, F.; Rieser, T.; Becker, S.; Groß, J.; Matthes, H.; Oei, S.L.; Thronicke, A. Efficacy of Tango Argentino for Cancer-Associated Fatigue and Quality of Life in Breast Cancer Survivors: A Randomized Controlled Trial. Cancers 2023, 15, 2920. https://doi.org/10.3390/cancers15112920
Schad F, Rieser T, Becker S, Groß J, Matthes H, Oei SL, Thronicke A. Efficacy of Tango Argentino for Cancer-Associated Fatigue and Quality of Life in Breast Cancer Survivors: A Randomized Controlled Trial. Cancers. 2023; 15(11):2920. https://doi.org/10.3390/cancers15112920
Chicago/Turabian StyleSchad, Friedemann, Thomas Rieser, Sarah Becker, Jessica Groß, Harald Matthes, Shiao Li Oei, and Anja Thronicke. 2023. "Efficacy of Tango Argentino for Cancer-Associated Fatigue and Quality of Life in Breast Cancer Survivors: A Randomized Controlled Trial" Cancers 15, no. 11: 2920. https://doi.org/10.3390/cancers15112920