
The Lack of Standardized Outcomes for Surgical Salvage of HPV-Positive Recurrent Oropharyngeal Squamous Cell Carcinoma: A Systematic Scoping Review

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Identify the Research Question
2.2. Identify Relevant Literature
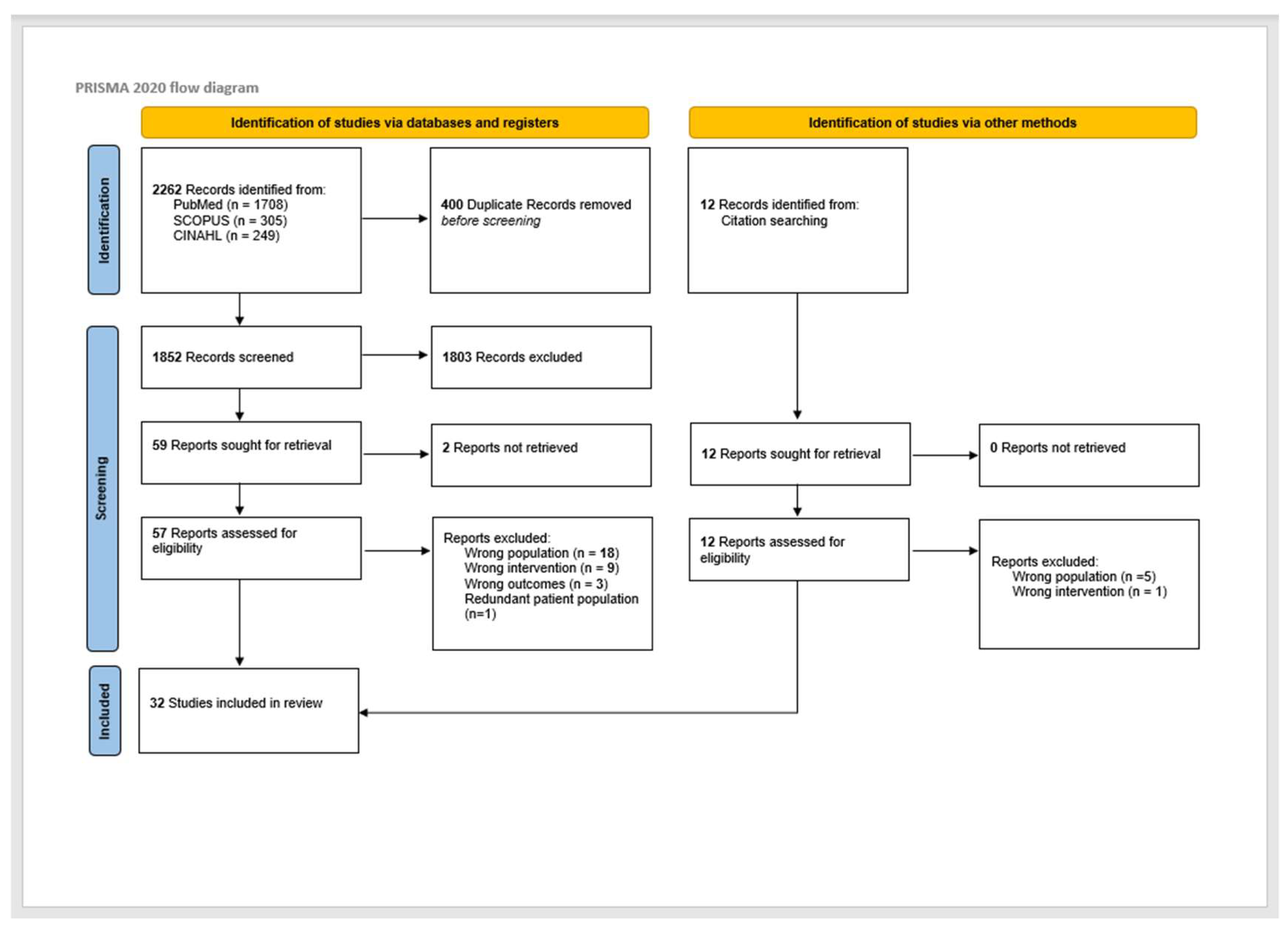
2.3. Study Selection
Search Process
2.4. Charting the Data
2.4.1. Data Extraction
2.4.2. Level of Evidence and Risk of Bias
2.5. Collating, Summarizing, and Reporting Results
2.6. Definitions
2.7. Statistical Analysis
3. Results
3.1. Publication Characteristics
3.2. Patient Attributes
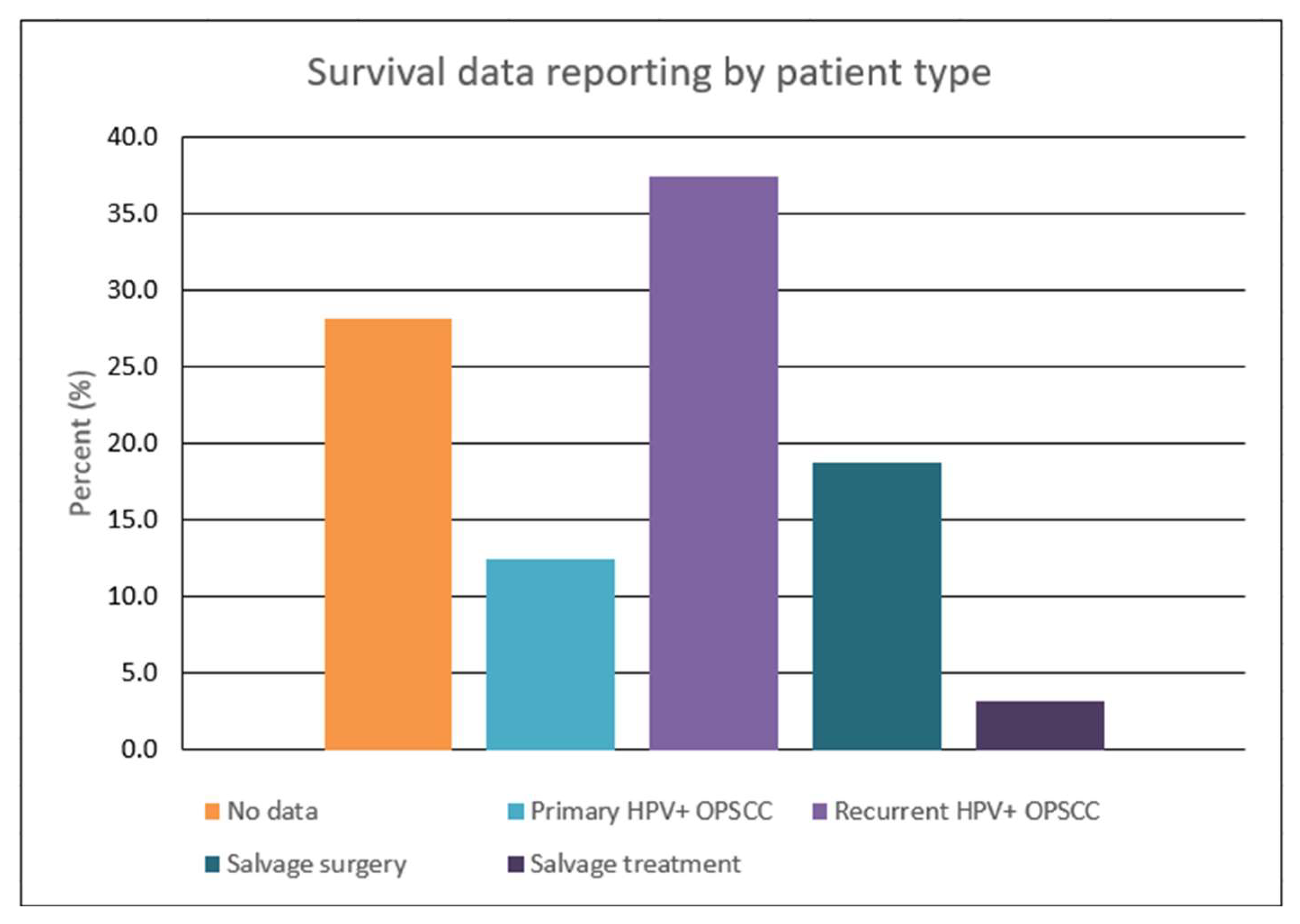
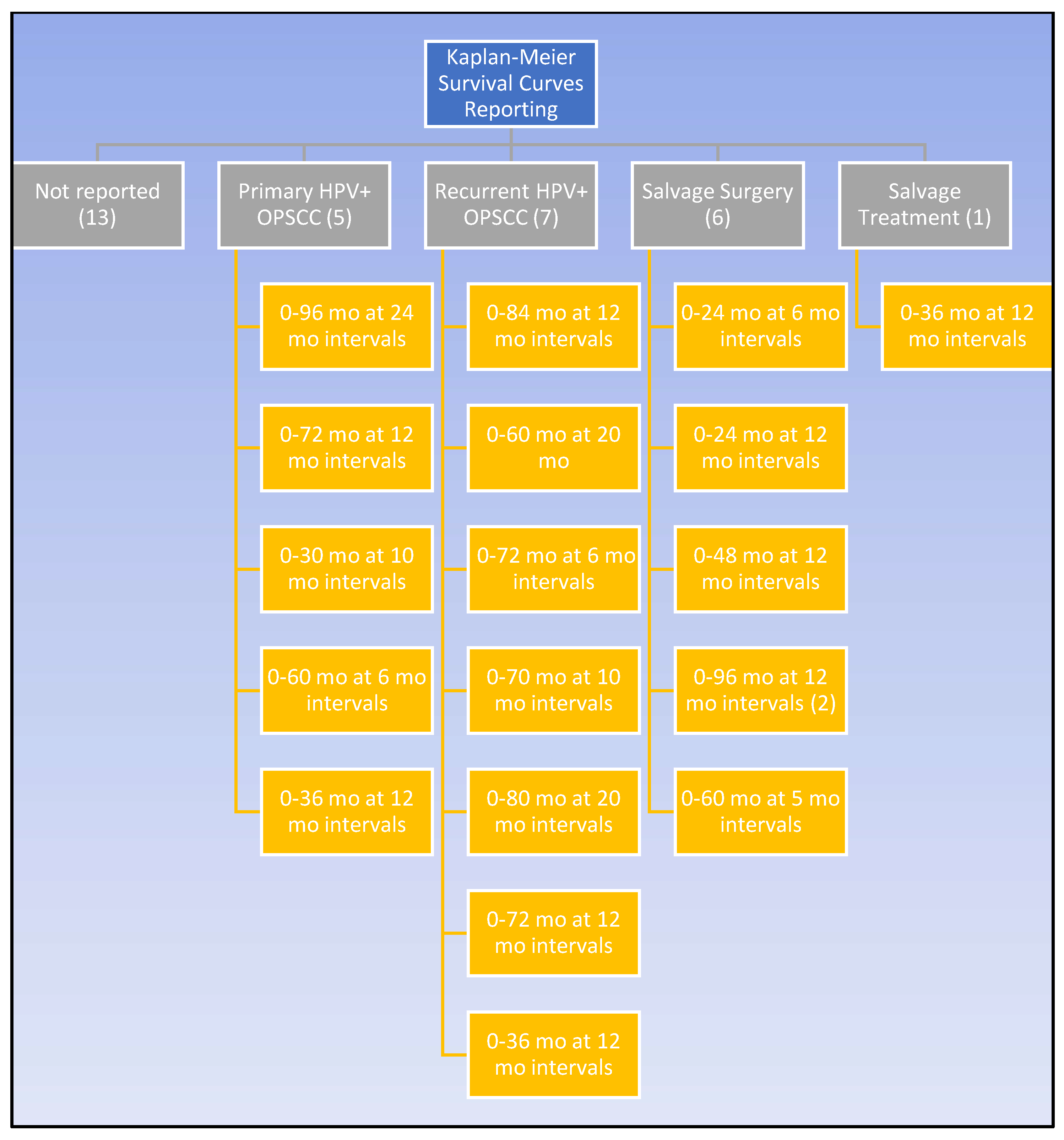
3.3. Survival Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Abbreviation | Definition |
| HPV | Human papillomavirus |
| OPSCC | Oropharyngeal squamous cell carcinoma |
| SS | Salvage surgery |
| OS | overall survival |
| PRS | post-recurrence survival |
| CSS | cancer-specific survival |
| DFS | disease-free survival |
| PFS | progression-free survival |
| K-M | Kaplan–Meier |
| DSS | disease-specific survival |
| RFS | relapse-free survival |
| LRR | Locoregional recurrence |
| ND | Neck dissection |
| TORS | Transoral robotic surgery |
| TLM | Transoral laser microsurgery |
| CACI | Charlson Age Comorbidity Index |
| HNSCC | Head and neck squamous cell carcinoma |
| QoL | Quality of life |
| PEG | Percutaneous endoscopic gastrostomy |
References
- Jemal, A.; Simard, E.P.; Dorell, C.; Noone, A.M.; Markowitz, L.E.; Kohler, B.; Eheman, C.; Saraiya, M.; Bandi, P.; Saslow, D.; et al. Annual Report to the Nation on the Status of Cancer, 1975–2009, featuring the burden and trends in human papillomavirus (HPV)-associated cancers and HPV vaccination coverage levels. J. Natl. Cancer Inst. 2013, 105, 175–201. [Google Scholar] [CrossRef]
- Nomura, F.; Sugimoto, T.; Kitagaki, K.; Ito, T.; Kawachi, H.; Eishi, Y.; Watanabe, K.; Igaue, M.; Shimizu, N.; Tomita, M.; et al. Clinical characteristics of Japanese oropharyngeal squamous cell carcinoma positive for human papillomavirus infection. Acta Otolaryngol. 2014, 134, 1265–1274. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Kang, S.Y.; Cohen, E.E.W. Current perspectives on recurrent HPV-mediated oropharyngeal cancer. Front. Oncol. 2022, 12, 966899. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Flamand, Y.; Weinstein, G.S.; Li, S.; Quon, H.; Mehra, R.; Garcia, J.J.; Chung, C.H.; Gillison, M.L.; Duvvuri, U.; et al. Transoral robotic surgical resection followed by randomization to low- or standard-dose IMRT in resectable p16+ locally advanced oropharynx cancer: A trial of the ECOG-ACRIN Cancer Research Group (E3311). J. Clin. Oncol. 2020, 38 (Suppl. 15), 6500. [Google Scholar] [CrossRef]
- Goodwin, W.J., Jr. Salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract: When do the ends justify the means? Laryngoscope 2000, 110 (Suppl. 93), 1–18. [Google Scholar] [CrossRef]
- Kao, S.S.; Micklem, J.; Ofo, E.; Edwards, S.; Dhatrak, D.; Foreman, A.; Krishnan, S.; Hodge, J.C. A comparison of oncological outcomes between transoral surgical and non-surgical treatment protocols in the management of oropharyngeal squamous cell carcinoma. J. Laryngol. Otol. 2018, 132, 349–355. [Google Scholar] [CrossRef]
- Zafereo, M.E.; Hanasono, M.M.; Rosenthal, D.I.; Sturgis, E.M.; Lewin, J.S.; Roberts, D.B.; Weber, R.S. The role of salvage surgery in patients with recurrent squamous cell carcinoma of the oropharynx. Cancer 2009, 115, 5723–5733. [Google Scholar] [CrossRef]
- Hamoir, M.; Schmitz, S.; Suarez, C.; Strojan, P.; Hutcheson, K.A.; Rodrigo, J.P.; Mendenhall, W.M.; Simo, R.; Saba, N.F.; D’Cruz, A.K.; et al. The Current Role of Salvage Surgery in Recurrent Head and Neck Squamous Cell Carcinoma. Cancers 2018, 10, 267. [Google Scholar] [CrossRef]
- Mclean, T.; Fitzgerald, C.; Boyle, J.O. Therapeutic strategies: Surgery for human papillomavirus-associated oropharyngeal carcinoma. J. Surg. Oncol. 2021, 124, 935–944. [Google Scholar] [CrossRef]
- Van Weert, S.; Leemans, C.R. Salvage surgery in head and neck cancer. Oral Dis. 2021, 27, 117–124. [Google Scholar] [CrossRef]
- Fakhry, C.; Zhang, Q.; Nguyen-Tan, P.F.; Rosenthal, D.; El-Naggar, A.; Garden, A.S.; Soulieres, D.; Trotti, A.; Avizonis, V.; Ridge, J.A.; et al. Human papillomavirus and overall survival after progression of oropharyngeal squamous cell carcinoma. J. Clin. Oncol. 2014, 32, 3365–3373. [Google Scholar] [CrossRef]
- Guo, T.; Qualliotine, J.R.; Ha, P.K.; Califano, J.A.; Kim, Y.; Saunders, J.R.; Blanco, R.G.; D’Souza, G.; Zhang, Z.; Chung, C.H.; et al. Surgical salvage improves overall survival for patients with HPV-positive and HPV-negative recurrent locoregional and distant metastatic oropharyngeal cancer. Cancer 2015, 121, 1977–1984. [Google Scholar] [CrossRef]
- Sweeny, L.; Rosenthal, E.L.; Clemons, L.; Stevens, T.M.; Cook McIntosh, E.R.; Carroll, W.R. Outcomes after surgical salvage for recurrent oropharyngeal squamous cell carcinoma. Oral Oncol. 2016, 60, 118–124. [Google Scholar] [CrossRef]
- Patel, T.R.; Lee, S.; Tajudeen, B.A.; Stenson, K.; Bhayani, M.; Al-Khudari, S. Association of HPV status with survival after surgical salvage of oropharyngeal cancers. Am. J. Otolaryngol. 2022, 43, 103491. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsely, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Henegan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H.; Goddard, O.; et al. The Oxford Levels of Evidence 2. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 24 October 2022).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Cochrane. 2022. Available online: www.training.cochrane.org/handbook (accessed on 24 October 2022).
- NCI Dictionary of Cancer Terms. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/ (accessed on 13 December 2022).
- Tsai, P.-C.; Chien, H.-C.; Hsu, P.-K.; Hung, J.-J.; Huang, C.-S.; Hsu, W.-H.; Hsu, H.-S. Post-recurrence survival analysis in patients with oligo-recurrence after curative esophagectomy. BMC Cancer 2022, 22, 637. [Google Scholar] [CrossRef]
- Freeman, M.F.; Turkey, J.W. Transformations related to the angular and the square root. Ann. Math. Stat. 1950, 21, 607–611.605. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Bigelow, E.O.; Harris, J.; Fakhry, C.; Gillison, M.L.; Nguyen-Tan, P.F.; Rosenthal, D.I.; Frank, S.J.; Nair, S.G.; Bahig, H.; Ridge, J.A.; et al. Risk stratification after recurrence of human papillomavirus (HPV)-related and non-HPV-related oropharyngeal cancer: Secondary analysis of NRG Oncology RTOG 0129 and 0522. Head Neck 2022, 44, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Carey, R.M.; Shimunov, D.; Weinstein, G.S.; Cannady, S.B.; Lukens, J.N.; Lin, A.; Swisher-McClure, S.; Bauml, J.M.; Aggarwal, C.; Cohen, R.B.; et al. Increased rate of recurrence and high rate of salvage in patients with human papillomavirus-associated oropharyngeal squamous cell carcinoma with adverse features treated with primary surgery without recommended adjuvant therapy. Head Neck 2021, 43, 1128–1141. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Sinha, P.; Last, A.; Ettyreddy, A.; Kallogjeri, D.; Pipkorn, P.; Rich, J.T.; Zevallos, J.P.; Paniello, R.; Puram, S.V.; et al. Outcomes of Patients with Single-Node Metastasis of Human Papillomavirus-Related Oropharyngeal Cancer Treated with Transoral Surgery. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Christopherson, K.M.; Moreno, A.C.; Elgohari, B.; Gross, N.; Ferrarotto, R.; Mohamed, A.S.R.; Brandon Gunn, G.; Goepfert, R.P.; Mott, F.E.; Shah, S.J.; et al. Outcomes after salvage for HPV-positive recurrent oropharyngeal cancer treated with primary radiation. Oral Oncol. 2021, 113, 105125. [Google Scholar] [CrossRef] [PubMed]
- Culié, D.; Lisan, Q.; Leroy, C.; Modesto, A.; Schiappa, R.; Chamorey, E.; Dassonville, O.; Poissonnet, G.; Guelfucci, B.; Bizeau, A.; et al. Oropharyngeal cancer: First relapse description and prognostic factor of salvage treatment according to p16 status, a GETTEC multicentric study. Eur. J. Cancer 2021, 143, 168–177. [Google Scholar] [CrossRef]
- Daniels, C.P.; Liu, H.Y.; Bernard, A.; Williams, C.; Foote, M.C.; Ladwa, R.; McGrath, M.; Panizza, B.J.; Porceddu, S.V. The declining role of post-treatment neck dissection in human papillomavirus-associated oropharyngeal cancer. Radiother. Oncol. 2020, 151, 242–248. [Google Scholar] [CrossRef]
- De Felice, F.; Bird, T.; Michaelidou, A.; Jeannon, J.P.; Simo, R.; Oakley, R.; Lyons, A.; Fry, A.; Cascarini, L.; Asit, A.; et al. Clinical outcomes in relapsed oropharyngeal cancer after definitive (chemo) radiotherapy. Oral Dis. 2021, 29, 595–603. [Google Scholar] [CrossRef]
- Galloway, T.J.; Zhang, Q.; Nguyen-Tan, P.F.; Rosenthal, D.I.; Soulieres, D.; Fortin, A.; Silverman, C.L.; Daly, M.E.; Ridge, J.A.; Hammond, J.A.; et al. Prognostic Value of p16 Status on the Development of a Complete Response in Involved Oropharynx Cancer Neck Nodes after Cisplatin-Based Chemoradiation: A Secondary Analysis of NRG Oncology RTOG 0129. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 362–371. [Google Scholar] [CrossRef]
- Joseph, A.W.; Guo, T.; Hur, K.; Xie, Y.; Yin, L.; Califano, J.A.; Ha, P.K.; Quon, H.; Richmon, J.D.; Eisele, D.W.; et al. Disease-free survival after salvage therapy for recurrent oropharyngeal squamous cell carcinoma. Head Neck 2016, 38 (Suppl. S1), E1501–E1509. [Google Scholar] [CrossRef]
- Landin, D.; Näsman, A.; Jara, S.J.; Hammarstedt-Nordenvall, L.; Munck-Wikland, E.; Dalianis, T.; Marklund, L. Post-Treatment Neck Dissection of Tonsillar and Base of Tongue Squamous Cell Carcinoma in the Era of PET-CT, HPV, and p16. Viruses 2022, 14, 1693. [Google Scholar] [CrossRef]
- Lee, N.C.J.; Kelly, J.R.; Park, H.S.; An, Y.; Judson, B.L.; Burtness, B.A.; Husain, Z.A. Patterns of failure in high-metastatic node number human papillomavirus-positive oropharyngeal carcinoma. Oral Oncol. 2018, 85, 35–39. [Google Scholar] [CrossRef]
- Masroor, F.; Corpman, D.; Carpenter, D.M.; Ritterman Weintraub, M.; Cheung, K.H.N.; Wang, K.H. Association of NCCN-Recommended Posttreatment Surveillance with Outcomes in Patients with HPV-Associated Oropharyngeal Squamous Cell Carcinoma. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 903–908. [Google Scholar] [CrossRef]
- Mueller, S.K.; Mantsopoulos, K.; Semrau, S.; Agaimy, A.; Eckstein, M.; Traxdorf, M.; Gostian, A.O.; Goncalves, M.; Sievert, M.; Haderlein, M.; et al. Influence of p16 status on indication and outcome of salvage neck dissection in oropharyngeal cancer. Acta Otolaryngol. 2021, 141, 187–192. [Google Scholar] [CrossRef]
- Patel, S.N.; Cohen, M.A.; Givi, B.; Dixon, B.J.; Gilbert, R.W.; Gullane, P.J.; Brown, D.H.; Irish, J.C.; de Almeida, J.R.; Higgins, K.M.; et al. Salvage surgery for locally recurrent oropharyngeal cancer. Head Neck 2016, 38 (Suppl. S1), E658–E664. [Google Scholar] [CrossRef]
- Pipkorn, P.; Sinha, P.; Kallogjeri, D.; Adkins, D.; Thorstad, W.T.; Rich, J.T.; Jackson, R.S. Outcomes of relapsed human papillomavirus-related oropharyngeal squamous cell carcinoma treated with curative intent. Head Neck 2019, 41, 1312–1319. [Google Scholar] [CrossRef]
- Routman, D.M.; Funk, R.K.; Tangsriwong, K.; Lin, A.; Keeney, M.G.; Garcia, J.J.; Zarka, M.A.; Lewis, J.T.; Stoddard, D.G.; Moore, E.J.; et al. Relapse Rates with Surgery Alone in Human Papillomavirus-Related Intermediate- and High-Risk Group Oropharynx Squamous Cell Cancer: A Multi-Institutional Review. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 938–946. [Google Scholar] [CrossRef]
- Ryan, W.R.; Xu, M.J.; Ochoa, E.; Plonowska-Hirschfeld, K.A.; Zebolsky, A.L.; Ha, P.K.; Bewley, A.F.; Mallen-St Clair, J.; Joshi, A.S.; Coffey, C.S.; et al. Oncologic outcomes of human papillomavirus-associated oropharynx carcinoma treated with surgery alone: A 12-institution study of 344 patients. Cancer 2021, 127, 3092–3106. [Google Scholar] [CrossRef]
- Sims, J.R.; Van Abel, K.; Martin, E.J.; Lohse, C.M.; Price, D.L.; Olsen, K.D.; Moore, E.J. Management of Recurrent and Metastatic HPV-Positive Oropharyngeal Squamous Cell Carcinoma after Transoral Robotic Surgery. Otolaryngol. Head Neck Surg. 2017, 157, 69–76. [Google Scholar] [CrossRef]
- Su, W.; Rajeev-Kumar, G.; Kang, M.; Posner, M.; Liu, J.T.; Westra, W.; Miles, B.A.; Gupta, V.; Sharma, S.; Misiukiewicz, K. Long-term outcomes in patients with recurrent human papillomavirus-positive oropharyngeal cancer after upfront transoral robotic surgery. Head Neck 2020, 42, 3490–3496. [Google Scholar] [CrossRef]
- Williamson, A.; Haywood, M.; Awad, Z. Feasibility of Free Flap Reconstruction Following Salvage Robotic-Assisted Resection of Recurrent and Residual Oropharyngeal Cancer in 3 Patients. Ear Nose Throat J. 2021, 100, 1113s–1118s. [Google Scholar] [CrossRef]
- Wotman, M.; Ghaly, M.; Massaro, L.; Tham, T.; Seetharamu, N.; Kamdar, D.; Frank, D.; Kraus, D.; Teckie, S. Management of the neck after definitive chemoradiation in patients with HPV-associated oropharyngeal cancer: An institutional experience. Am. J. Otolaryngol. 2019, 40, 684–690. [Google Scholar] [CrossRef]
- Yokota, T.; Onitsuka, T.; Hamauchi, S.; Shirasu, H.; Onozawa, Y.; Iida, Y.; Kamijo, T.; Mukaigawa, T.; Okada, S.; Irifune, Y.; et al. Triplet induction chemotherapy followed by less invasive surgery without reconstruction for human papillomavirus-associated oropharyngeal cancers: Why is it successful or unsuccessful? Int. J. Clin. Oncol. 2021, 26, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Dave, E.; Ozbek, U.; Gupta, V.; Genden, E.; Miles, B.; Teng, M.; Posner, M.; Misiukiewicz, K.; Bakst, R.L. The prognostic impact of human papillomavirus status following treatment failure in oropharyngeal cancer. PLoS ONE 2017, 12, e0181108. [Google Scholar] [CrossRef] [PubMed]
- Garden, A.S.; Gunn, G.B.; Hessel, A.; Beadle, B.M.; Ahmed, S.; El-Naggar, A.K.; Fuller, C.D.; Byers, L.A.; Phan, J.; Frank, S.J. Management of the lymph node-positive neck in the patient with human papillomavirus-associated oropharyngeal cancer. Cancer 2014, 120, 3082–3088. [Google Scholar] [CrossRef] [PubMed]
- Billfalk-Kelly, A.; Yu, E.; Su, J.; O’Sullivan, B.; Waldron, J.; Ringash, J.; Bartlett, E.; Perez-Ordonez, B.; Weinreb, I.; Bayley, A.; et al. Radiologic Extranodal Extension Portends Worse Outcome in cN+ TNM-8 Stage I Human Papillomavirus-Mediated Oropharyngeal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1017–1027. [Google Scholar] [CrossRef]
- Bledsoe, T.J.; Noble, A.R.; Hunter, G.K.; Rybicki, L.A.; Hoschar, A.; Chute, D.J.; Saxton, J.P.; Greskovich, J.F.; Adelstein, D.J.; Koyfman, S.A. Oropharyngeal squamous cell carcinoma with known human papillomavirus status treated with definitive chemoradiotherapy: Patterns of failure and toxicity outcomes. Radiat. Oncol. 2013, 8, 174. [Google Scholar] [CrossRef]
- Jackson, R.S.; Sinha, P.; Zenga, J.; Kallogjeri, D.; Suko, J.; Martin, E.; Moore, E.J.; Haughey, B.H. Transoral Resection of Human Papillomavirus (HPV)-Positive Squamous Cell Carcinoma of the Oropharynx: Outcomes with and Without Adjuvant Therapy. Ann. Surg. Oncol. 2017, 24, 3494–3501. [Google Scholar] [CrossRef]
- Chen, A.M.; Felix, C.; Wang, P.C.; Hsu, S.; Basehart, V.; Garst, J.; Beron, P.; Wong, D.; Rosove, M.H.; Rao, S.; et al. Reduced-dose radiotherapy for human papillomavirus-associated squamous-cell carcinoma of the oropharynx: A single-arm, phase 2 study. Lancet Oncol. 2017, 18, 803–811. [Google Scholar] [CrossRef]
- Carey, R.M.; Brody, R.M.; Shimunov, D.; Shinn, J.R.; Mady, L.J.; Rajasekaran, K.; Cannady, S.B.; Lin, A.; Lukens, J.N.; Bauml, J.M.; et al. Locoregional Recurrence in p16-Positive Oropharyngeal Squamous Cell Carcinoma after TORS. Laryngoscope 2021, 131, E2865–E2873. [Google Scholar] [CrossRef]
- Gross, N.D.; Hanna, E.Y. The Role of Surgery in the Management of Recurrent Oropharyngeal Cancer. Recent Results Cancer Res. 2017, 206, 197–205. [Google Scholar] [CrossRef]
- Kim, J.; Kim, S.; Albergotti, W.G.; Choi, P.A.; Kaplan, D.J.; Abberbock, S.; Johnson, J.T.; Gildener-Leapman, N. Selection of Ideal Candidates for Surgical Salvage of Head and Neck Squamous Cell Carcinoma: Effect of the Charlson-Age Comorbidity Index and Oncologic Characteristics on 1-Year Survival and Hospital Course. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 1059–1065. [Google Scholar] [CrossRef]
- Lang, K.; ElShafie, R.A.; Akbaba, S.; Koschny, R.; Bougatf, N.; Bernhardt, D.; Adeberg, S.; Hafner, M.; Kargus, S. Percutaneous Endoscopic Gastrostomy Tube Placement in Patients with Head and Neck Cancer Treated with Radiotherapy. Cancer Manag. Res. 2020, 12, 127–136. [Google Scholar] [CrossRef]
- Bulbul, M.G.; Genovese, T.J.; Hagan, K.; Rege, S.; Qureshi, A.; Varvares, M.A. Salvage surgery for recurrent squamous cell carcinoma of the head and neck: Systematic review and meta-analysis. Head Neck 2022, 44, 275–285. [Google Scholar] [CrossRef]
- Rich, J.T.; Neely, J.G.; Paniello, R.C.; Voelker, C.C.; Nussenbaum, B.; Wang, E.W. A practical guide to understanding Kaplan-Meier curves. Otolaryngol. Head Neck Surg. 2010, 143, 331–336. [Google Scholar] [CrossRef]
- Hung, J.J.; Hsu, W.H.; Hsieh, C.C.; Huang, B.S.; Huang, M.H.; Liu, J.S.; Wu, Y.C. Post-recurrence survival in completely resected stage I non-small cell lung cancer with local recurrence. Thorax 2009, 64, 192–196. [Google Scholar] [CrossRef]
- Mariotto, A.B.; Noone, A.M.; Howlader, N.; Cho, H.; Keel, G.E.; Garshell, J.; Woloshin, S.; Schwarts, L.M. Cancer survival: An overview of measures, uses, and interpretation. J. Natl. Cancer Inst. Monogr. 2014, 2014, 145–186. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | LRR 1 | SS 2 | SS + adj 3 |
|---|---|---|---|
| Bigelow 2022 [24] | 51 | 21 | 0 |
| Billfalk-Kelly 2019 [48] | 11 | 4 | 0 |
| Bledsoe 2013 [49] | 3 | 3 | 0 |
| Carey 2020 [25] | 32 | 11 | 3 |
| Chen 2017 [51] | 3 | 3 | 0 |
| Chen 2021 [26] | 11 | 9 | 2 |
| Christopherson 2021 [27] | 69 | 32 | 17 |
| Culié 2021 [28] | 55 | 38 | 0 |
| Daniels 2020 [29] | 36 | 19 | 0 |
| Dave 2017 [46] | 5 | 1 | 1 |
| DeFelice 2021 [30] | 10 | 6 | 0 |
| Fakhry 2014 [11] | 57 | 29 | 0 |
| Galloway 2016 [31] | 199 | 69 | 0 |
| Garden 2014 [47] | 20 | 14 | 0 |
| Guo 2015 [12] | 51 | 46 | 0 |
| Jackson 2017 [50] | 26 | 5 | 8 |
| Joseph 2016 [32] | 43 | 33 | 0 |
| Landin 2022 [33] | 26 | 5 | 8 |
| Lee 2018 [34] | 7 | 2 | 0 |
| Masroor 2019 [35] | 5 | 3 | 0 |
| Mueller 2021 [36] | 17 | 17 | 0 |
| Patel 2016 [37] | 19 | 19 | 0 |
| Patel 2022 [14] | 99 | 99 | 0 |
| Pipkorn 2019 [38] | 21 | 1 | 11 |
| Routman 2017 [39] | 12 | 0 | 5 |
| Ryan 2021 [40] | 22 | 8 | 1 |
| Sims 2017 [41] | 19 | 7 | 0 |
| Su 2020 [42] | 26 | 0 | 8 |
| Sweeny 2016 [13] | 9 | 9 | 0 |
| Williamson 2021 [43] | 3 | 3 | 0 |
| Wotman 2019 [44] | 20 | 6 | 0 |
| Yokota 2021 [45] | 2 | 0 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taniguchi, A.N.; Sutton, S.R.; Nguyen, S.A.; Kejner, A.E.; Albergotti, W.G. The Lack of Standardized Outcomes for Surgical Salvage of HPV-Positive Recurrent Oropharyngeal Squamous Cell Carcinoma: A Systematic Scoping Review. Cancers 2023, 15, 2832. https://doi.org/10.3390/cancers15102832
Taniguchi AN, Sutton SR, Nguyen SA, Kejner AE, Albergotti WG. The Lack of Standardized Outcomes for Surgical Salvage of HPV-Positive Recurrent Oropharyngeal Squamous Cell Carcinoma: A Systematic Scoping Review. Cancers. 2023; 15(10):2832. https://doi.org/10.3390/cancers15102832
Chicago/Turabian StyleTaniguchi, April N., Sarah R. Sutton, Shaun A. Nguyen, Alexandra E. Kejner, and William G. Albergotti. 2023. "The Lack of Standardized Outcomes for Surgical Salvage of HPV-Positive Recurrent Oropharyngeal Squamous Cell Carcinoma: A Systematic Scoping Review" Cancers 15, no. 10: 2832. https://doi.org/10.3390/cancers15102832