
A Review of the Use of Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Malignancy in Pediatric Patients
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
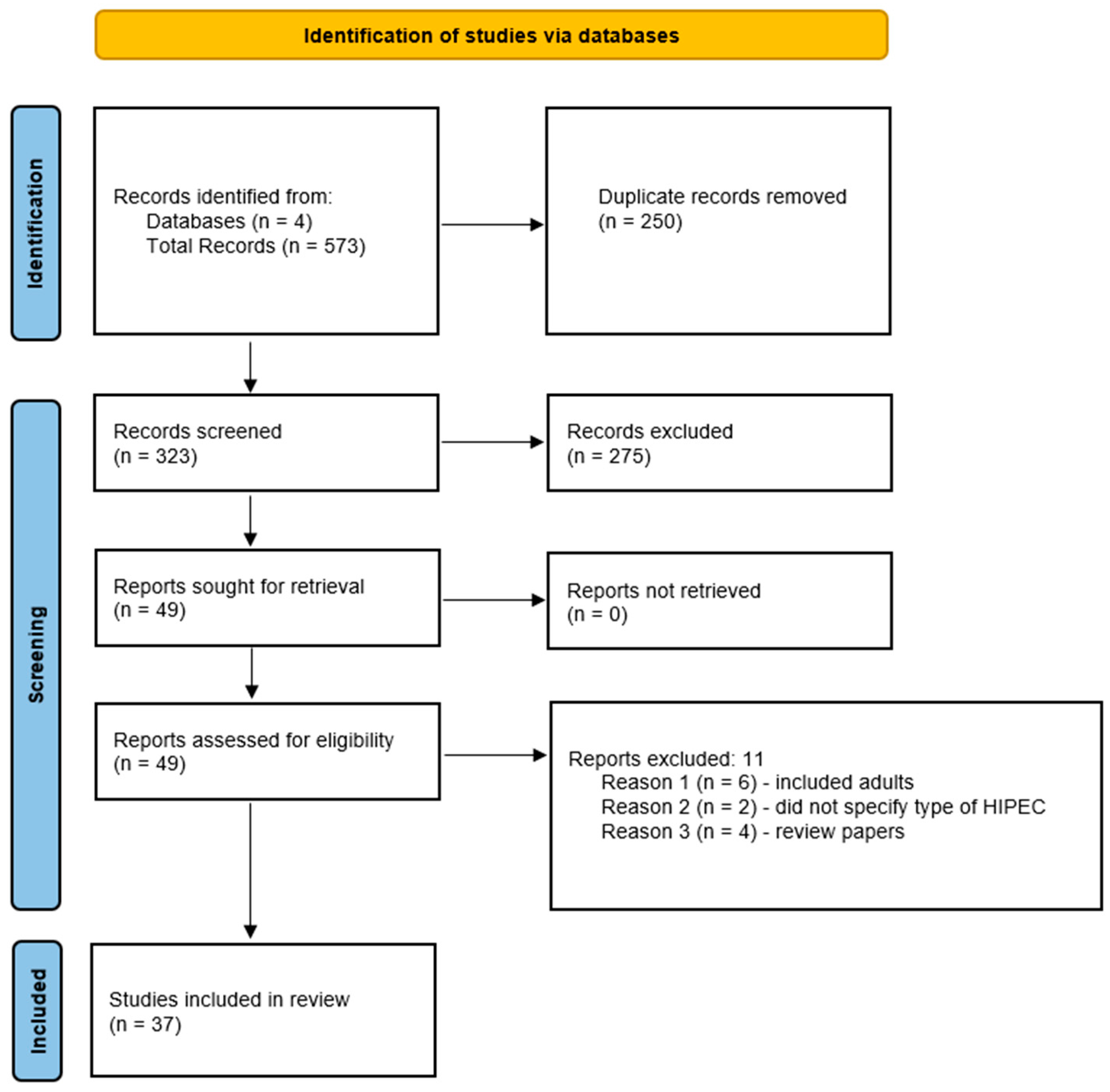
2. Methods
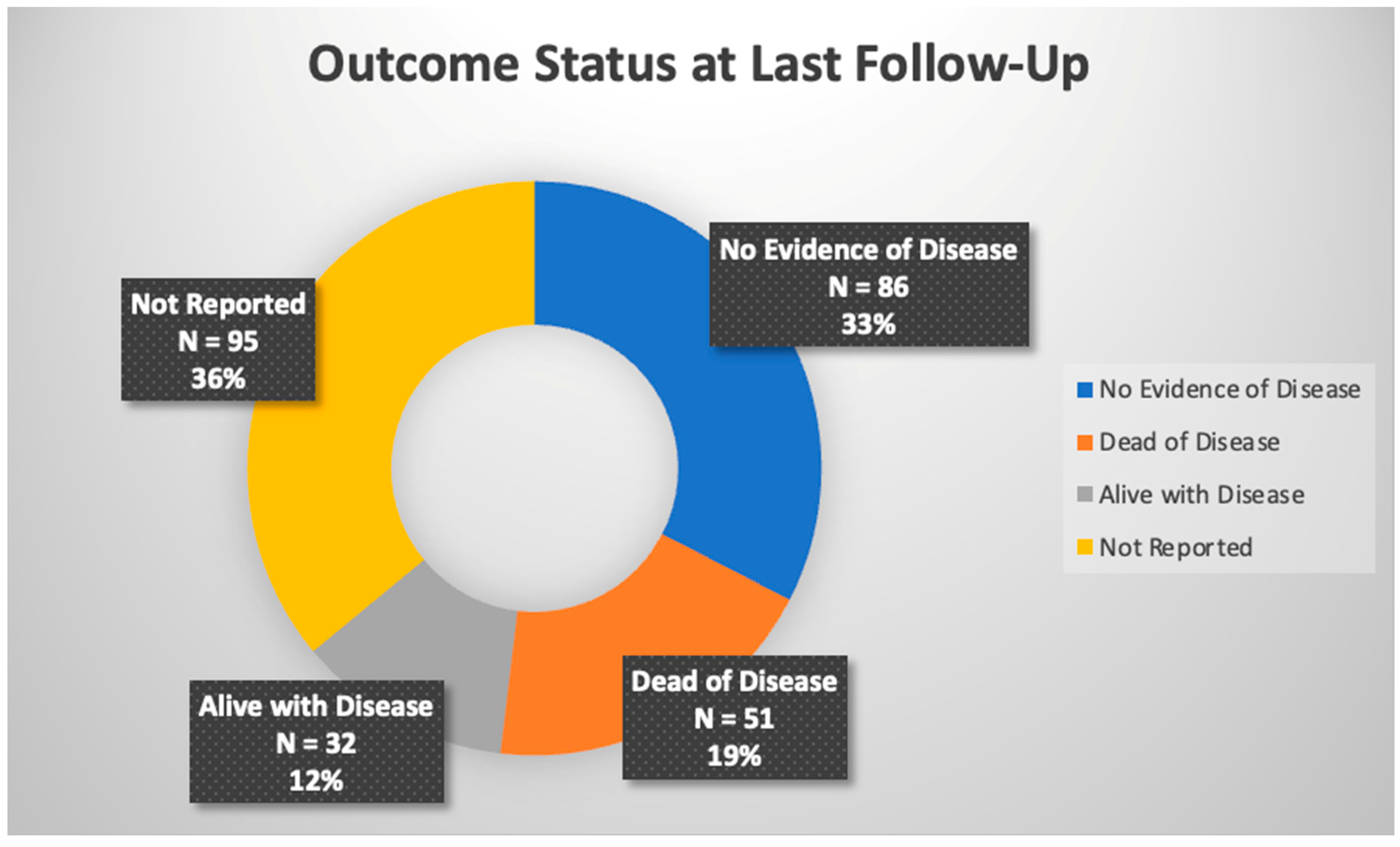
3. Results
4. Discussion
4.1. Cytoreductive Surgery and HIPEC Technique
4.2. Mitigating Agent and Reported Toxicities
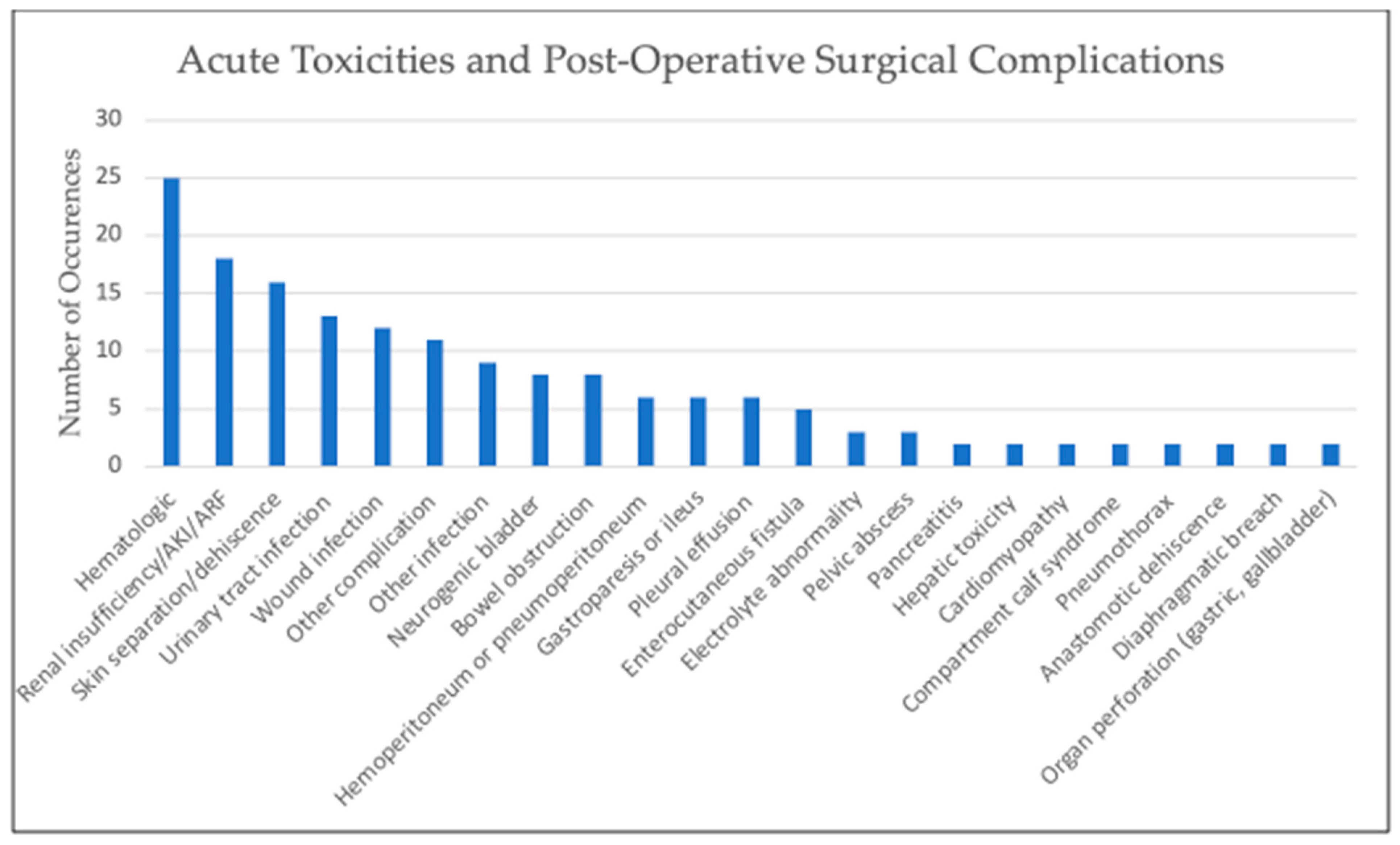
4.3. Known Toxicities and Complications
4.4. Pediatric Applications of HIPEC
4.4.1. Desmoplastic Small-Round-Cell Tumor (DSRCT)
4.4.2. Rhabdomyosarcoma (RMS)
4.4.3. Angiosarcoma
4.4.4. Colorectal Carcinoma
4.4.5. Primary Disseminated Ovarian Tumors
4.4.6. Mesothelioma
4.4.7. Wilms Tumor
4.4.8. Undifferentiated Sarcoma
4.4.9. Melanoma
4.4.10. Inflammatory Myofibroblastic Tumor (IMT)
4.4.11. Epithelioid Inflammatory Myofibroblastic Sarcoma (EIMS)
4.4.12. Histiocytic Sarcoma
4.4.13. Others
5. Future Directions
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dedrick, R.L.; Myers, C.E.; Bungay, P.M.; DeVita, V.T., Jr. Pharmacokinetic rationale for peritoneal drug administration in the treatment of ovarian cancer. Cancer Treat. Rep. 1978, 62, 1–11. [Google Scholar] [PubMed]
- Van Driel, W.J.; Koole, S.N.; Sikorska, K.; Schagen van Leeuwen, J.H.; Schreuder, H.W.R.; Hermans, R.H.M.; de Hingh, I.; Van der Velden, J.; Arts, H.J.; Massuger, L.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N. Engl. J. Med. 2018, 378, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Verwaal, V.J.; van Ruth, S.; de Bree, E.; van Sloothen, G.W.; van Tinteren, H.; Boot, H.; Zoetmulder, F.A. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J. Clin. Oncol. 2003, 21, 3737–3743. [Google Scholar] [CrossRef] [PubMed]
- Auer, R.C.; Sivajohanathan, D.; Biagi, J.; Conner, J.; Kennedy, E.; May, T. Indications for hyperthermic intraperitoneal chemotherapy with cytoreductive surgery: A systematic review. Eur. J. Cancer. 2020, 127, 76–95. [Google Scholar] [CrossRef] [PubMed]
- Bushati, M.; Rovers, K.P.; Sommariva, A.; Sugarbaker, P.H.; Morris, D.L.; Yonemura, Y.; Quadros, C.A.; Somashekhar, S.P.; Ceelen, W.; Dube, P.; et al. The current practice of cytoreductive surgery and HIPEC for colorectal peritoneal metastases: Results of a worldwide web-based survey of the Peritoneal Surface Oncology Group International (PSOGI). Eur. J. Surg. Oncol. 2018, 44, 1942–1948. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Bautista, F.; Elias, D.; Pasqualini, C.; Valteau-Couanet, D.; Brugieres, L. Hyperthermic intraperitoneal chemotherapy after cytoreductive surgery for the treatment of peritoneal carcinomatosis in pediatric solid malignancies: A single institution experience. J. Pediatr. Surg. 2014, 49, 1276–1279. [Google Scholar] [CrossRef]
- Gesche, J.; Beckert, S.; Neunhoeffer, F.; Kachanov, D.; Konigsrainer, A.; Seitz, G.; Fuchs, J. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: A safe treatment option for intraperitoneal rhabdomyosarcoma in children below 5 years of age. Pediatr. Blood Cancer 2019, 66, e27517. [Google Scholar] [CrossRef]
- Hayes-Jordan, A.; Green, H.; Fitzgerald, N.; Xiao, L.; Anderson, P. Novel treatment for desmoplastic small round cell tumor: Hyperthermic intraperitoneal perfusion. J. Pediatr. Surg. 2010, 45, 1000–1006. [Google Scholar] [CrossRef]
- Hayes-Jordan, A.; Green, H.; Lin, H.; Owusu-Agyemang, P.; Mejia, R.; Okhuysen-Cawley, R.; Cortes, J.; Fitzgerald, N.E.; McAleer, M.F.; Herzog, C.; et al. Cytoreductive surgery and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for children, adolescents, and young adults: The first 50 cases. Ann. Surg. Oncol. 2015, 22, 1726–1732. [Google Scholar] [CrossRef]
- Hayes-Jordan, A.; Green, H.; Prieto, V.; Wolff, J.E. Unusual cases: Melanomatosis and nephroblastomatosis treated with hyperthermic intraperitoneal chemotherapy. J. Pediatr. Surg. 2012, 47, 782–787. [Google Scholar] [CrossRef]
- Hayes-Jordan, A.; Green, H.; Ludwig, J.; Anderson, P. Toxicity of hyperthermic intraperitoneal chemotherapy (HIPEC) in pediatric patients with sarcomatosis/carcinomatosis: Early experience and phase 1 results. Pediatr. Blood Cancer 2012, 59, 395–397. [Google Scholar] [CrossRef]
- Hayes-Jordan, A.; Lopez, C.; Green, H.L.; Xiao, L.C.; Huh, W.; Herzog, C.E. Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) in pediatric ovarian tumors: A novel treatment approach. Pediatr. Surg. Int. 2016, 32, 71–73. [Google Scholar] [CrossRef]
- Hayes-Jordan, A.A.; Coakley, B.A.; Green, H.L.; Xiao, L.; Fournier, K.F.; Herzog, C.E.; Ludwig, J.A.; McAleer, M.F.; Anderson, P.M.; Huh, W.W. Desmoplastic Small Round Cell Tumor Treated with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy: Results of a Phase 2 Trial. Ann. Surg. Oncol. 2018, 25, 872–877. [Google Scholar] [CrossRef]
- Pariury, H.; Golden, C.; Huh, W.W.; Cham, E.; Chung, T.; Hayes-Jordan, A. Pediatric ovarian angiosarcoma treated with systemic chemotherapy and cytoreductive surgery with heated intraperitoneal chemotherapy: Case report and review of therapy. Pediatr. Blood Cancer 2019, 66, e27753. [Google Scholar] [CrossRef]
- Sorrentino, L.; Serra, F.; Cabry, F.; De Julis, S.; Barbieri, E.; Girardis, M.; Ceccarelli, P.L.; Gelmini, R. Cytoreductive surgery and HIPEC in a 14 years old patient with peritoneal recurrence of adenocarcinoma of the right colon. Int. J. Surg. Case Rep. 2019, 57, 118–121. [Google Scholar] [CrossRef]
- Winer, L.; Macedo, F.I.; Alfawaz, A.; Sommariva, A.; Cecchetto, G.; Podda, A.; Neville, H.L.; Möller, M.G. Novel Therapy for Pediatric Angiosarcoma with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. J. Pediatr. Hematol. Oncol. 2018, 40, e505–e510. [Google Scholar] [CrossRef]
- Zmora, O.; Hayes-Jordan, A.; Nissan, A.; Kventsel, I.; Newmann, Y.; Itskovsky, K.; Ash, S.; Levy-Mendelovich, S.; Shinhar, D.; Ben-Yaakov, A.; et al. Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) for disseminated intra-abdominal malignancies in children-a single-institution experience. J. Pediatr. Surg. 2018, 53, 1381–1386. [Google Scholar] [CrossRef]
- Malekzadeh, P.; Good, M.; Hughes, M.S. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) with cisplatin in pediatric patients with peritoneal mesothelioma: A single institution experience and long term follow up. Int. J. Hyperth. 2021, 38, 326–331. [Google Scholar] [CrossRef]
- Reingruber, B.; Boettcher, M.I.; Klein, P.; Hohenberger, W.; Pelz, J.O. Hyperthermic intraperitoneal chemoperfusion is an option for treatment of peritoneal carcinomatosis in children. J. Pediatr. Surg. 2007, 42, E17–E21. [Google Scholar] [CrossRef]
- Whitlock, R.S.; Malik, T.; Smith, V.; Mahajan, P.; Hayes-Jordan, A.; Vasudevan, S.A. Sclerosing Encapsulating Peritonitis in a Pediatric Patient Treated with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. J. Pediatr. Hematol. Oncol. 2021, 43, e685–e688. [Google Scholar] [CrossRef] [PubMed]
- Stiles, Z.E.; Murphy, A.J.; Anghelescu, D.L.; Brown, C.L.; Davidoff, A.M.; Dickson, P.V.; Glazer, E.S.; Bishop, M.W.; Furman, W.L.; Pappo, A.S.; et al. Desmoplastic Small Round Cell Tumor: Long-Term Complications After Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy. Ann. Surg. Oncol. 2020, 27, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Findlay, B.L.; Gargollo, P.C.; Granberg, C.F. Use of Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Pediatric Sarcoma for Maximal Oncologic Control. Urology 2020, 141, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Kazi, M.; Qureshi, S.S. Primary Peritoneal Rhabdomyosarcomatosis in a 2-Year-Old Child Treated with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy—Case Report and Review of Literature. Indian J. Surg. Oncol. 2021, 12, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Scalabre, A.; Philippe-Chomette, P.; Passot, G.; Orbach, D.; Elias, D.; Corradini, N.; Brugieres, L.; Msika, S.; Leclair, M.D.; Joseph, S.; et al. Cytoreductive surgery and hyperthermic intraperitoneal perfusion with chemotherapy in children with peritoneal tumor spread: A French nationwide study over 14 years. Pediatr. Blood. Cancer 2018, 65. [Google Scholar] [CrossRef]
- Sjoberg Bexelius, T.; Chisholm, J.C.; Okoye, B.; Cecil, T.; Angelini, P.; Dayal, S. Hyperthermic intraperitoneal chemotherapy (HIPEC) as another treatment modality for desmoplastic round cell tumour patients: First paediatric experience from UK. BMJ Case Rep. 2021, 14, e234876. [Google Scholar] [CrossRef]
- Zhu, Z.; Chang, X.; Wang, J.; Yang, S.; Qin, H.; Yang, W.; Cheng, H.; Meng, D.; Wang, H. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal malignant tumors in children: Initial experience in a single institution. Front. Surg. 2022, 9, 1078039. [Google Scholar] [CrossRef]
- Doctor, J.R.; Solanki, S.L.; Jain, A.R.; Patil, V.P. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in a 2-YearOld Child with Abdominopelvic Rhabdomyosarcoma: A Case Report of Anaesthetic Concerns. Turk. J. Anaesthesiol. Reanim. 2022, 50, 68–71. [Google Scholar] [CrossRef]
- Xiao, J.; Browning, M.B.; Boyd, K.P.; Suchi, M.; Turaga, K.K.; Firat, S.Y.; Mortland, L.J.; Lal, D.R. Multimodal Therapy Including Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy Can Result in Long-term Disease-free Survival in Pediatric Desmoplastic Small Round Cell Tumor with Extraperitoneal Disease. J. Pediatr. Hematol. Oncol. 2021, 43, 228–231. [Google Scholar] [CrossRef]
- Kartal, İ.; Topgül, K.; Aslan, M.K.; Dağdemir, A.; Özyürek, E.; Sarıkaya, Ş. Addition of hyperthermic intraperitoneal chemotherapy (HIPEC) after complete cytoreductive surgery in a child with desmoplastic small round cell tumour. J. Exp. Clin. Med. 2020, 36, 131–135. [Google Scholar]
- Fan, H.S.; I’Ons, B.; McConnell, R.; Kumar, V.; Alzahrani, S.; Morris, D.L. Peritonectomy and hyperthermic intraperitoneal chemotherapy as treatment for desmoplastic small round cell tumour. Int. J. Surg. Case Rep. 2015, 7, 85–88. [Google Scholar] [CrossRef]
- Oyeniyi, J.; Wu, J.; Liu, D.; Yao, J.C.; Green, H.; Albritton, K.; Huh, W.; Hayes-Jordan, A. Treatment of carcinomatosis using cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in adolescents and young adults. Am. J. Surg. 2015, 209, 610–615. [Google Scholar] [CrossRef]
- Orbach, D.; Andre, N.; Brecht, I.B.; Lopez Almaraz, R.; Ben-Ami, T.; Vermersch, S.; Carton, M.; Virgone, C.; Bisogno, G.; Schneider, D.T.; et al. Mesothelioma in children and adolescents: The European Cooperative Study Group for Pediatric Rare Tumors (EXPeRT) contribution. Eur. J. Cancer 2020, 140, 63–70. [Google Scholar] [CrossRef]
- Siddiqui, A.; Pinto, N.; Applebaum, M.A.; Mak, G.Z.; Cunningham, J.M.; LaBelle, J.L.; Nassin, M.L. The addition of autologous stem cell transplantation to neoadjuvant chemotherapy, radiation, and HIPEC for patients with unresectable desmoplastic small round cell tumor: A single center case series. Int. J. Surg. Oncol. 2020, 5, e95. [Google Scholar] [CrossRef]
- Cacciotti, C.; Samji, N.; Cox, S.; Yikilmaz, A.; Hann, C.; Marin, J.A.; Fowler, J.; VanHouwelingen, L.; Athale, U. Desmoplastic Small Round Cell Tumor with Ascending Intraspinal Metastasis at Recurrence: Case Report and Review of the Literature. J. Pediatr. Hematol.Oncol. 2022, 44, e561–e566. [Google Scholar] [CrossRef]
- Lamm, A.W.; Hayes, A.; Sutherland, R. Pediatric Patient Diagnosed with Testicular and Peritoneal Mesothelioma Undergoing Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy: From a Father’s Asbestos Exposure? J. Pediatr. Surg. Nurs. 2022, 11, 116–120. [Google Scholar] [CrossRef]
- Msika, S.; Gruden, E.; Sarnacki, S.; Orbach, D.; Philippe-Chomette, P.; Castel, B.; Sabate, J.M.; Flamant, Y.; Kianmanesh, R. Cytoreductive surgery associated to hyperthermic intraperitoneal chemoperfusion for desmoplastic round small cell tumor with peritoneal carcinomatosis in young patients. J. Pediatr. Surg. 2010, 45, 1617–1621. [Google Scholar] [CrossRef]
- Vermersch, S.; Arnaud, A.; Orbach, D.; Andre, N.; Berger, C.; Kepenekian, V.; Brigand, C.; Fresneau, B.; Poli-Merol, M.L.; Habougit, C.; et al. Multicystic and diffuse malignant peritoneal mesothelioma in children. Pediatr. Blood. Cancer. 2020, 67, e28286. [Google Scholar] [CrossRef]
- Sandler, G.; Franklin, A.; Hayes-Jordan, A. Histiocytic sarcoma in a child-successful management and long-term survival with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Pediatr. Blood Cancer 2018, 65, e27054. [Google Scholar] [CrossRef]
- Brecht, I.B.; Agaimy, A.; Besendorfer, M.; Carbon, R.; Thiel, F.C.; Rompel, O.; Osinski, D.; Langer, T.; Metzler, M.; Holter, W. Malignant peritoneal mesothelioma in a 16-year-old girl: Presentation of a rare disease. Klin. Padiatr. 2012, 224, 170–173. [Google Scholar] [CrossRef]
- El-Sharkawy, F.; Delgado, P.I.; Podda, A.; Neville, H.L.; Rojas, C.P. Angiosarcoma of the Pelvis in a 13-Year-Old Girl. Pediatr. Dev. Pathol. 2017, 20, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Vaz, J.A.; Katebi Kashi, P.; Movahedi-Lankarani, S.; Piguet, N.B.; Zeligs, K.P.; Bijelic, L.; Rao, U.N.M.; Conrads, T.P.; Maxwell, G.L.; Darcy, K.M.; et al. Sixteen year-old with leiomyosarcoma in a prior benign myomectomy site. Gynecol. Oncol. Rep. 2019, 29, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Garnier, H.; Murawski, M.; Jastrzebski, T.; Pawinska-Wasikowska, K.; Balwierz, W.; Sinacka, K.; Gorecki, W.; Izycka-Swieszewska, E.; Czauderna, P. Case Report: Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy Application in Intraperitoneally Disseminated Inflammatory Myofibroblastic Tumor and in the Youngest Patient in the World: New Indication and Modification of Technique. Front. Surg. 2021, 8, 746700. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, P.H. Management of peritoneal-surface malignancy: The surgeon’s role. Langenbeck’s Arch. Surg. 1999, 384, 576–587. [Google Scholar] [CrossRef]
- Rodríguez Silva, C.; Moreno Ruiz, F.J.; Bellido Estévez, I.; Carrasco Campos, J.; Titos García, A.; Ruiz López, M.; González Poveda, I.; Toval Mata, J.A.; Mera Velasco, S.; Santoyo Santoyo, J. Are there intra-operative hemodynamic differences between the Coliseum and closed HIPEC techniques in the treatment of peritoneal metastasis? A retrospective cohort study. World J. Surg. Oncol. 2017, 15, 51. [Google Scholar] [CrossRef]
- Lotti, M.; Capponi, M.G.; Piazzalunga, D.; Poiasina, E.; Pisano, M.; Manfredi, R.; Ansaloni, L. Laparoscopic HIPEC: A bridge between open and closed-techniques. J. Minimal Access Surg. 2016, 12, 86–89. [Google Scholar] [CrossRef]
- Cho, H.-K.; Lush, R.M.; Bartlett, D.L.; Alexander, H.R.; Wu, P.C.; Libutti, S.K.; Lee, K.B.; Venzon, D.J.; Bauer, K.S.; Reed, E.; et al. Pharmacokinetics of Cisplatin Administered by Continuous Hyperthermic Peritoneal Perfusion (CHPP) to Patients with Peritoneal Carcinomatosis. J. Clin. Pharmacol. 1999, 39, 394–401. [Google Scholar] [CrossRef]
- Goodman, M.D.; McPartland, S.; Detelich, D.; Saif, M.W. Chemotherapy for intraperitoneal use: A review of hyperthermic intraperitoneal chemotherapy and early post-operative intraperitoneal chemotherapy. J. Gastrointest. Oncol. 2016, 7, 45–57. [Google Scholar] [CrossRef]
- Freyer, D.R.; Chen, L.; Krailo, M.D.; Knight, K.; Villaluna, D.; Bliss, B.; Pollock, B.H.; Ramdas, J.; Lange, B.; Van Hoff, D.; et al. Effects of sodium thiosulfate versus observation on development of cisplatin-induced hearing loss in children with cancer (ACCL0431): A multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 63–74. [Google Scholar] [CrossRef]
- Howell, S.B.; Pfeifle, C.L.; Wung, W.E.; Olshen, R.A.; Lucas, W.E.; Yon, J.L.; Green, M. Intraperitoneal cisplatin with systemic thiosulfate protection. Ann. Intern. Med. 1982, 97, 845–851. [Google Scholar] [CrossRef]
- Laplace, N.; Kepenekian, V.; Friggeri, A.; Vassal, O.; Ranchon, F.; Rioufol, C.; Gertych, W.; Villeneuve, L.; Glehen, O.; Bakrin, N. Sodium thiosulfate protects from renal impairement following hyperthermic intraperitoneal chemotherapy (HIPEC) with Cisplatin. Int. J. Hyperth. 2020, 37, 897–902. [Google Scholar] [CrossRef]
- Hubner, M.; Kusamura, S.; Villeneuve, L.; Al-Niaimi, A.; Alyami, M.; Balonov, K.; Bell, J.; Bristow, R.; Guiral, D.C.; Fagotti, A.; et al. Guidelines for Perioperative Care in Cytoreductive Surgery (CRS) with or without hyperthermic IntraPEritoneal chemotherapy (HIPEC): Enhanced Recovery After Surgery (ERAS(R)) Society Recommendations—Part II: Postoperative management and special considerations. Eur. J. Surg. Oncol. 2020, 46, 2311–2323. [Google Scholar] [CrossRef]
- Piso, P.; Nedelcut, S.D.; Rau, B.; Konigsrainer, A.; Glockzin, G.; Strohlein, M.A.; Horbelt, R.; Pelz, J. Morbidity and Mortality Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy: Data from the DGAV StuDoQ Registry with 2149 Consecutive Patients. Ann. Surg. Oncol. 2019, 26, 148–154. [Google Scholar] [CrossRef]
- Bekhor, E.; Carr, J.; Hofstedt, M.; Sullivan, B.; Solomon, D.; Leigh, N.; Bolton, N.; Golas, B.; Sarpel, U.; Labow, D.; et al. The Safety of Iterative Cytoreductive Surgery and HIPEC for Peritoneal Carcinomatosis: A High Volume Center Prospectively Maintained Database Analysis. Ann. Surg. Oncol. 2020, 27, 1448–1455. [Google Scholar] [CrossRef]
- Sugarbaker, P.H.; Alderman, R.; Edwards, G.; Marquardt, C.E.; Gushchin, V.; Esquivel, J.; Chang, D. Prospective morbidity and mortality assessment of cytoreductive surgery plus perioperative intraperitoneal chemotherapy to treat peritoneal dissemination of appendiceal mucinous malignancy. Ann. Surg. Oncol. 2006, 13, 635–644. [Google Scholar] [CrossRef]
- Bent, M.A.; Padilla, B.E.; Goldsby, R.E.; DuBois, S.G. Clinical Characteristics and Outcomes of Pediatric Patients with Desmoplastic Small Round Cell Tumor. Rare Tumors 2016, 8, 6145. [Google Scholar] [CrossRef]
- Subbiah, V.; Lamhamedi-Cherradi, S.E.; Cuglievan, B.; Menegaz, B.A.; Camacho, P.; Huh, W.; Ramamoorthy, V.; Anderson, P.M.; Pollock, R.E.; Lev, D.C.; et al. Multimodality Treatment of Desmoplastic Small Round Cell Tumor: Chemotherapy and Complete Cytoreductive Surgery Improve Patient Survival. Clin. Cancer Res. 2018, 24, 4865–4873. [Google Scholar] [CrossRef]
- Honore, C.; Delhorme, J.B.; Nassif, E.; Faron, M.; Ferron, G.; Bompas, E.; Glehen, O.; Italiano, A.; Bertucci, F.; Orbach, D.; et al. Can we cure patients with abdominal Desmoplastic Small Round Cell Tumor? Results of a retrospective multicentric study on 100 patients. Surg. Oncol. 2019, 29, 107–112. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef]
- Quenet, F.; Elias, D.; Roca, L.; Goere, D.; Ghouti, L.; Pocard, M.; Facy, O.; Arvieux, C.; Lorimier, G.; Pezet, D.; et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 256–266. [Google Scholar] [CrossRef]
- van de Vlasakker, V.C.J.; Lurvink, R.J.; Cashin, P.H.; Ceelen, W.; Deraco, M.; Goere, D.; Gonzalez-Moreno, S.; Lehmann, K.; Li, Y.; Moran, B.; et al. The impact of PRODIGE 7 on the current worldwide practice of CRS-HIPEC for colorectal peritoneal metastases: A web-based survey and 2021 statement by Peritoneal Surface Oncology Group International (PSOGI). Eur. J. Surg. Oncol. 2021, 47, 2888–2892. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, L.; Serra, F.; Cabry, F.; Cauteroq, N.; Zmora, O.; Gelmini, R. Peritoneal carcinomatosis from colorectal cancer in the pediatric population: Cytoreductive surgery and HIPEC. A systematic review. Eur. J. Surg. Oncol. 2021, 47, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Yee, F.Z.Y.; Tan, G.H.C.; Chia, C.S.; Soo, K.C.; Teo, M.C.C. Uncommon indications for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Pleura Peritoneum 2017, 2, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Helderman, R.; Loke, D.R.; Kok, H.P.; Oei, A.L.; Tanis, P.J.; Franken, N.; Crezee, J. Variation in Clinical Application of Hyperthermic Intraperitoneal Chemotherapy: A Review. Cancers 2019, 11. [Google Scholar] [CrossRef]
- Seyfried, N.; Yurttas, C.; Burkard, M.; Oswald, B.; Tolios, A.; Herster, F.; Kauer, J.; Jager, T.; Konigsrainer, I.; Thiel, K.; et al. Prolonged Exposure to Oxaliplatin during HIPEC Improves Effectiveness in a Preclinical Micrometastasis Model. Cancers 2022, 14, 1158. [Google Scholar] [CrossRef]
- Wagner, B.R.; Adamus, A.L.; Sonnecken, D.; Vahdad, R.; Jank, P.; Denkert, C.; Mahnken, A.H.; Seitz, G. Establishment of a new valid animal model for the evaluation of hyperthermic intraperitoneal chemotherapy (HIPEC) in pediatric rhabdomyosarcoma. Pediatr. Blood Cancer 2021, 68, e29202. [Google Scholar] [CrossRef]
- Wagner, B.R.; Adamus, A.L.; Hempfling, L.; Vahdad, R.; Haap-Hoff, A.; Heinrich, B.; Vazquez, O.; Jank, P.; Denkert, C.; Seitz, G. Increasing the efficiency of hyperthermic intraperitoneal chemotherapy (HIPEC) by combination with a photosensitive drug in pediatric rhabdomyosarcoma in an animal model. Pediatr. Blood Cancer 2022, 69, e29864. [Google Scholar] [CrossRef]
- Ubink, I.; Bolhaqueiro, A.C.F.; Elias, S.G.; Raats, D.A.E.; Constantinides, A.; Peters, N.A.; Wassenaar, E.C.E.; de Hingh, I.; Rovers, K.P.; van Grevenstein, W.M.U.; et al. Organoids from colorectal peritoneal metastases as a platform for improving hyperthermic intraperitoneal chemotherapy. Br. J. Surg. 2019, 106, 1404–1414. [Google Scholar] [CrossRef]
- Kong, X.X.; Jiang, S.; Liu, T.; Liu, G.F.; Dong, M. Paclitaxel increases sensitivity of SKOV3 cells to hyperthermia by inhibiting heat shock protein 27. Biomed. Pharmacother. 2020, 132, 110907. [Google Scholar] [CrossRef]
- Katschinski, D.M.; Jacobson, E.L.; Wiedemann, G.J.; Robins, H.I. Modulation of VP-16 cytotoxicity by carboplatin and 41.8 degrees C hyperthermia. J. Cancer Res. Clin. Oncol. 2001, 127, 425–432. [Google Scholar] [CrossRef]
- Winslow, T.B.; Eranki, A.; Ullas, S.; Singh, A.K.; Repasky, E.A.; Sen, A. A pilot study of the effects of mild systemic heating on human head and neck tumour xenografts: Analysis of tumour perfusion, interstitial fluid pressure, hypoxia and efficacy of radiation therapy. Int. J. Hyperth. 2015, 31, 693–701. [Google Scholar] [CrossRef]
- Pelz, J.O.; Vetterlein, M.; Grimmig, T.; Kerscher, A.G.; Moll, E.; Lazariotou, M.; Matthes, N.; Faber, M.; Germer, C.T.; Waaga-Gasser, A.M.; et al. Hyperthermic intraperitoneal chemotherapy in patients with peritoneal carcinomatosis: Role of heat shock proteins and dissecting effects of hyperthermia. Ann. Surg. Oncol. 2013, 20, 1105–1113. [Google Scholar] [CrossRef]
- Siddiqui, F.; Avery, P.R.; Li, C.Y.; Zhang, X.; LaRue, S.M.; Dewhirst, M.W.; Ullrich, R.L. Induction of the human heat shock promoter HSP70B by nutritional stress: Implications for cancer gene therapy. Cancer Investig. 2008, 26, 553–561. [Google Scholar] [CrossRef]
- Zhang, Y.; Gu, Y.; Guo, T.; Li, Y.; Cai, H. Perioperative immunonutrition for gastrointestinal cancer: A systematic review of randomized controlled trials. Surg. Oncol. 2012, 21, e87–e95. [Google Scholar] [CrossRef]
- Tan, G.H.C.; Chia, C.S.; Wong, J.S.M.; Ong, W.S.; Zhu, H.Y.; Ong, C.J.; Teo, M.C.C. Randomized Controlled Trial Investigating Perioperative Immunonutrition for Patients Undergoing Cytoreductive Surgery (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC). Ann. Surg. Oncol. 2023, 30, 777–789. [Google Scholar] [CrossRef]
- Evers, D.J.; Verwaal, V.J. Indication for oophorectomy during cytoreduction for intraperitoneal metastatic spread of colorectal or appendiceal origin. Br. J. Surg. 2011, 98, 287–292. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Paper Referenced | Type of Malignancy | Type of HIPEC * | Temperature and Duration of HIPEC |
|---|---|---|---|
| Bautista et al. [7] | Ovarian tumors (3), mesothelioma (2), fibrolamellar hepatocellular carcinoma (2), other types (2) | Oxaliplatin 300 mg/m2 + Irinotecan 200 mg/m2 | 43 °C, 30 min |
| Gesche et al. [8] | RMS (6) | Cisplatin 37.5–75 mg/m2 (6) Doxorubicin 15 mg/m2 (4) | 42.5 °C, 60 min |
| Hayes-Jordan et al. 2010 [9] | DSRCT (8) | Cisplatin 100–150 mg/m2 (8) + Mitoxantrone (1) | 40–41 °C, 90 min |
| Hayes-Jordan et al. 2015 [10] | DSRCT (21), RMS (7), mesothelioma (4), other (18) | Cisplatin 100 mg/m2 | 41 °C, time unspecified |
| Hayes-Jordan et al. 2012 [11] | Melanoma (1), Wilms tumor (1) | Cisplatin 100 mg/m2 | 41 °C, 90 min |
| Hayes-Jordan et al. 2012 [12] | DSRCT (13), mesothelioma (5), RMS (2), Wilms tumor (2), other (5) | Cisplatin 150 mg/m2 | 40.5–41 °C, 90 min |
| Hayes-Jordan et al. 2016 [13] | Ovarian tumors (8) | Cisplatin 100 mg/m2 | 41 °C, 90 min |
| Hayes-Jordan et al. 2018 [14] | DSRCT (14), RMS (2), undifferentiated sarcoma (2), other (2) | Cisplatin 100 mg/m2 | 41°C, 90 min |
| Pariury et al. [15] | Angiosarcoma (1) | Paclitaxel 40 mg/m2 | 41.5 °C, 90 min |
| Sorrentino et al. [16] | Colon adenocarcinoma (1) | Mitomycin C | 42 °C, 60 min |
| Winer et al. [17] | Angiosarcoma (2) | Mitomycin C 18 mg/m2 then 9 mg/m2 × 2 (1) Cisplatin 30 mg/m2 + Doxorubicin 100 mg/m2 (1) | 41.5–42 °C 60–90 min |
| Zmora et al. [18] | RMS (3), mesothelioma (2), other (4) | Cisplatin 100 mg/m2 (7), Doxorubicin 20 mg/m2 (1), Mitomycin C (1) | 41 °C, 90 min |
| Malekzadeh et al. [19] | Peritoneal mesothelioma (7) | Cisplatin 250 mg/m2 (7) + Paclitaxel 125 mg/m2 and 5-FU (3) | 41.1–43 °C time unspecified |
| Reingruber et al. [20] | Colon adenocarcinoma (1) | Mitomycin C 30 mg/m2 | 41.2 °C, 90 min |
| Whitlock et al. [21] | DSRCT (1) | Cisplatin 100 mg/m2 | 40.0 °C, 90 min |
| Stiles et al. [22] | DSRCT (10) | Cisplatin 100 mg/m2 (8), Mitomycin-C (1), Melphalan (1) | 42 °C, 60–90 min |
| Findlay et al. [23] | Undifferentiated sarcoma (1) | Cisplatin 100 mg/m2 | 42.5 °C, 90 min |
| Kazi et al. [24] | RMS (1) | Cisplatin 100 mg/m2 | 41.5–42°C, 90 min |
| Scalabre et al. [25] | Mesothelioma (7), DSRCT (7), RMS (1), ovarian tumors (2), other types (5) | Oxaliplatin 300 mg/m2 + Irinotecan 200 mg/m2 (7), Cisplatin + Doxorubicin (2), Oxaliplatin (2), Mitomycin + Cisplatin (9), Cisplatin + Ametycin (1), Cisplatin 200 mg/m2 (1) | 41–44 °C, 30–90 min |
| Bexelius et al. [26] | DSRCT (1) | Cisplatin 100 mg/m2 | 41 °C, 90 min |
| Zhu et al. [27] | RMS (7), Wilms tumor (2), clear cell sarcoma of kidney (2), sarcoma (2), other types (6) | Doxorubicin 15 mg/m2 + Ifosfamide 1 g/m2 (11), Doxorubicin 15 mg/m2 + Cisplatin 50 mg/m2 (5), Cisplatin 50 mg/m2 (3) | 40.5–41.5 °C, 60 min |
| Doctor et al. [28] | RMS (1) | Cisplatin | 41.5–42.0°C, 60 min |
| Xiao et al. [29] | DSRCT (1) | Cisplatin | 40.5 °C, 90 min |
| Kartal et al. [30] | DSRCT (1) | Irinotecan 200 mg/m2 + Oxaliplatin 300 mg/m2 | 41.0 °C, 60 min |
| Fan et al. [31] | DSRCT (2) | Cisplatin | 41.5 °C, 90 min |
| Oyeniyi et al. [32] | Colon carcinoma (5) | Mitomycin C (3), Oxaliplatin (2) | NR |
| Orbach et al. [33] | Mesothelioma (27) | Cisplatin + Doxorubicin (9), Cisplatin + Mitomycin (5), Cisplatin (3), Oxaliplatin + Irinotecan (2), Cisplatin + Paclitaxel (1), unspecified (3) | NR |
| Siddiqui et al. [34] | DSRCT (3) | Cisplatin 100 mg/m2 | Temperature unspecified, 90 min |
| Cacciotti et al. [35] | DSRCT (1) | Cisplatin | NR |
| Lamm et al. [36] | Mesothelioma (1) | Cisplatin | NR |
| Msika et al. [37] | DSRCT (3) | Cisplatin 75 mg/m2 + Mitomycin C | 41.0–43.0°C, 30 min |
| Vermersch et al. [38] | Mesothelioma (9) | Cisplatin + Mitomycin (4), Oxaliplatin + Irinotecan (2), Cisplatin + Doxorubicin (2), Methotrexate (1) | 42.0–43.0 °C, 30–60 min |
| Sandler et al. [39] | Histiocytic sarcoma (1) | Cisplatin | NR |
| Brecht et al. [40] | Mesothelioma (1) | Cisplatin | 41.0°C, 60 min |
| El-Sharkawy et al. [41] | Angiosarcoma (1) | Mitomycin C | Temperature unspecified, 90 min |
| Vaz et al. [42] | Leiomyosarcoma (1) | Cisplatin + Doxorubicin | 42.0°C, 60 min |
| Garnier et al. [43] | Inflammatory myofibroblastic tumor (1) | Doxorubicin | Temperature unspecified, 30 min |
| Paper Referenced | Peritoneal Cancer Index | Degree of Cytoreduction | Morbidity Rate | Survival Status at Last Follow-Up (Median Follow-Up) * | NED |
|---|---|---|---|---|---|
| Bautista et al. [7] | NR | CCR0 | 7 out of 9 | 4 out of 9 (58.8 mos) | 3 out of 9 |
| Gesche et al. [8] | 4–21 | CCR0 | 2 out of 6 | 6 out of 6 (12 mos) | 6 out of 6 |
| Hayes-Jordan et al. 2010 [9] | 3–33 | CCR0 | 3 out of 8 | 5 out of 8 (36.3 mos) | 1 out of 8 |
| Hayes-Jordan et al. 2015 [10] | 16 (reported median) | CCR0–CCR2 | 28 out of 50 | Statistic not reported (21.9 mos) | NR |
| Hayes-Jordan et al. 2012 [11] | 12 | CCR0 | 1 out of 2 | 2 out of 2 (9.5 mos) | 0 out of 2 |
| Hayes-Jordan et al. 2012 [12] | NR | CCR0 | 16 out of 23 | NR | 26% |
| Hayes-Jordan et al. 2016 [13] | 0–16 | CCR0 (6), CCR1 (2) | 2 out of 8 | 5 out of 8 (32 mos) | 5 out of 8 |
| Hayes-Jordan et al. 2018 [14] | 15 (reported median) | CCR0–CCR1 | NR | 79% survival at 3 years in group with DSRCT | NR |
| Pariury et al. [15] | NR | NR | 0 out of 1 | 1 out of 1 (43 mos) | 1 out of 1 |
| Sorrentino et al. [16] | 3 | CCR0 | 0 out of 1 | 1 out of 1 (11 mos) | 1 out of 1 |
| Winer et al. [17] | 16–17 | CCR0 | NR | 2 out of 2 (12 mos) | 1 out of 2 |
| Zmora et al. [18] | NR | CCR0 | 4 out of 9 | 7 out of 9 (28 mos) | 4 out of 9 |
| Malekzadeh et al. [19] | 6–25 | CCR0 (4), CCR1 (2), CCR2 (1) | 4 out of 7 | 5 out of 7 (104 mos) | 1 out of 7 |
| Reingruber et al. [20] | NR | NR | 1 out of 1 | 0 out of 1 (Death at 30 mos) | 0 out of 1 |
| Whitlock et al. [21] | NR | NR | 0 out of 1 | 1 out of 1 (13 mos) | 0 out of 1 |
| Stiles et al. [22] | 5–20 | CCR0 (5), CCR1 (4), CCR2 (1) | 9 out of 9 | 2 out of 9 (34 mos) | 1 out of 9 |
| Findlay et al. [23] | NR | CCR0 | 1 out of 1 | 1 out of 1 (14 mos) | 1 out of 1 |
| Kazi et al. [24] | 8 | NR | 0 out of 1 | 1 out of 1 (10 mos) | 1 out of 1 |
| Scalabre et al. [25] | NR | CCR0 (16), CCR1 (4), CCR2 (2) | 14 out of 22 | 13 out of 22 (57.5 mos) | 6 out of 22 |
| Bexelius et al. [26] | NR | NR | 0 out of 1 | 1 out of 1 (26 mos) | 1 out of 1 |
| Zhu et al. [27] | 2–21 | CCR0 (13), CCR1 (6) | 2 out of 19 | 14 out of 19 (14 mos) | 13 out of 19 |
| Doctor et al. [28] | 6 | NR | 0 out of 1 | NR | NR |
| Xiao et al. [29] | 21 | CCR0 | 1 out of 1 | 1 out of 1 (72 mos) | 1 out of 1 |
| Kartal et al. [30] | NR | NR | 0 out of 1 | 0 out of 1 (8 mos) | 0 out of 1 |
| Fan et al. [31] | 5, 12 | NR | 2 out of 2 | 2 out of 2 (22 mos) | 0 out of 2 |
| Oyeniyi et al. [32] | NR | CCR0 | NR | 3 out of 5 (10 mos) | 3 out of 5 |
| Orbach et al. [33] | NR | CCR0 11), CCR1 (4), CCR2 (2), remaining unspecified | NR | 20 out of 27 (80.4 mos) | 17 out of 27 |
| Siddiqui et al. [34] | 22–27 | NR | 0 out of 3 | 0 out of 3 (37.5 mos) | 0 out of 3 |
| Cacciotti et al. [35] | NR | NR | 1 out of 1 | 0 out of 1 (38 mos) | 0 out of 1 |
| Lamm et al. [36] | NR | NR | 1 out of 1 | NR | NR |
| Msika et al. [37] | NR | CCR0 (2), CCR2 (1) | 1 out of 3 | 1 out of 3 (10 mos) | 1 out of 3 |
| Vermersch et al. [38] | >10 for 4, unknown for others | CCR0 (5), CCR2 (3), unspecified (1) | 3 out of 9 | 9 out of 9 (7 mos) | 6 out of 9 |
| Sandler et al. [39] | NR | NR | NR | 1 out of 1 (72 mos) | 1 out of 1 |
| Brecht et al. [40] | NR | NR | 0 out of 1 | 1 out of 1 (17 mos) | 1 out of 1 |
| El-Sharkawy et al. [41] | NR | NR | NR | 1 out of 1 (12 mos) | 1 out of 1 |
| Vaz et al. [42] | NR | NR | 0 out of 1 | NR | NR |
| Garnier et al. [43] | NR | CCR0 | NR | 1 out of 1 (12 mos) | 1 out of 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byrwa, D.J.; Twist, C.J.; Skitzki, J.; Repasky, E.; Ham, P.B., III; Gupta, A. A Review of the Use of Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Malignancy in Pediatric Patients. Cancers 2023, 15, 2815. https://doi.org/10.3390/cancers15102815
Byrwa DJ, Twist CJ, Skitzki J, Repasky E, Ham PB III, Gupta A. A Review of the Use of Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Malignancy in Pediatric Patients. Cancers. 2023; 15(10):2815. https://doi.org/10.3390/cancers15102815
Chicago/Turabian StyleByrwa, David J., Clare J. Twist, Joseph Skitzki, Elizabeth Repasky, P. Ben Ham, III, and Ajay Gupta. 2023. "A Review of the Use of Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Malignancy in Pediatric Patients" Cancers 15, no. 10: 2815. https://doi.org/10.3390/cancers15102815