
Immunodeficiencies Push Readmissions in Malignant Tumor Patients: A Retrospective Cohort Study Based on the Nationwide Readmission Database
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
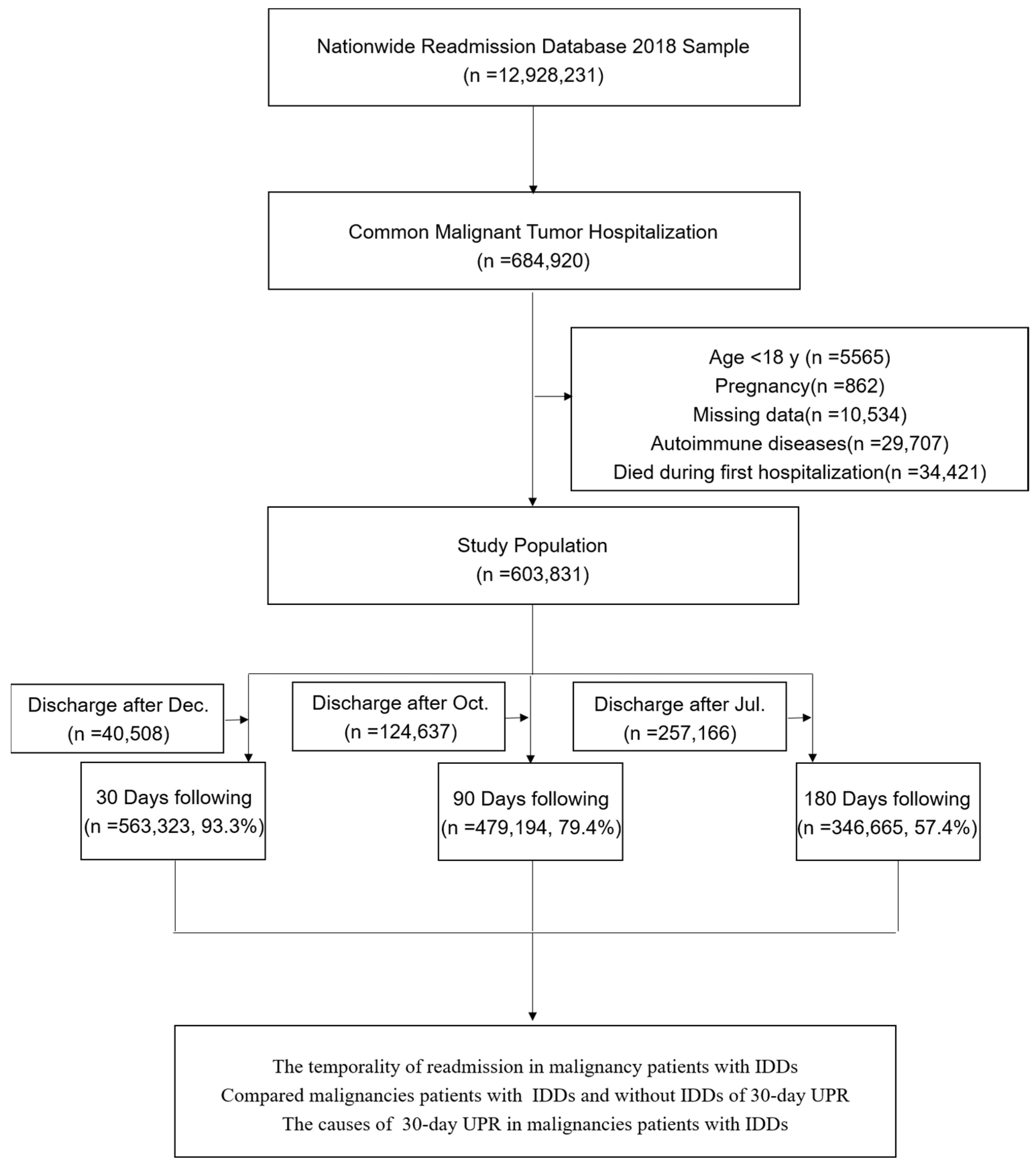
2.2. Study Population
2.3. Outcomes
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
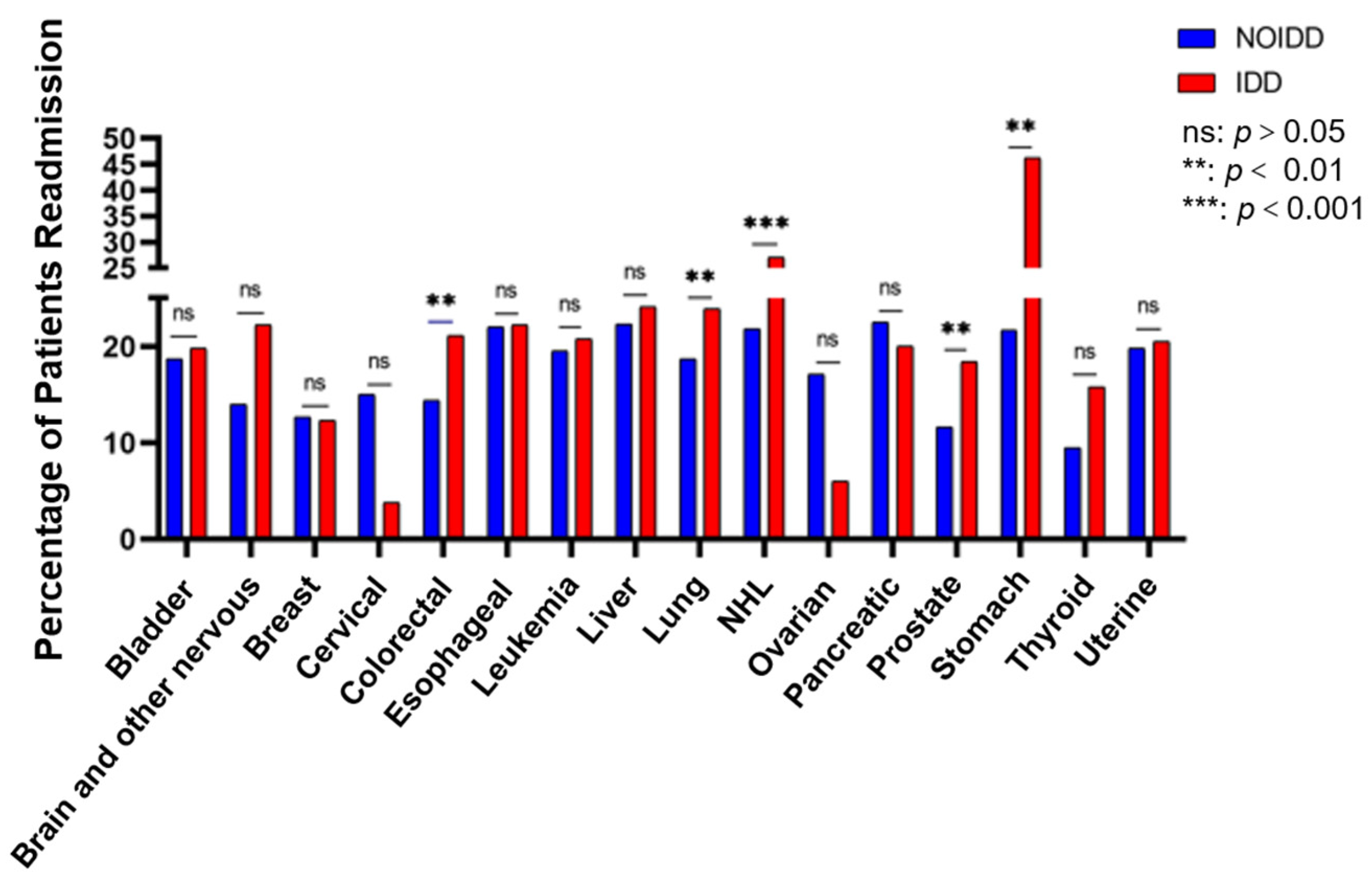
3.2. Readmission Risk of Malignancy for Patients Diagnosed with or without IDDs
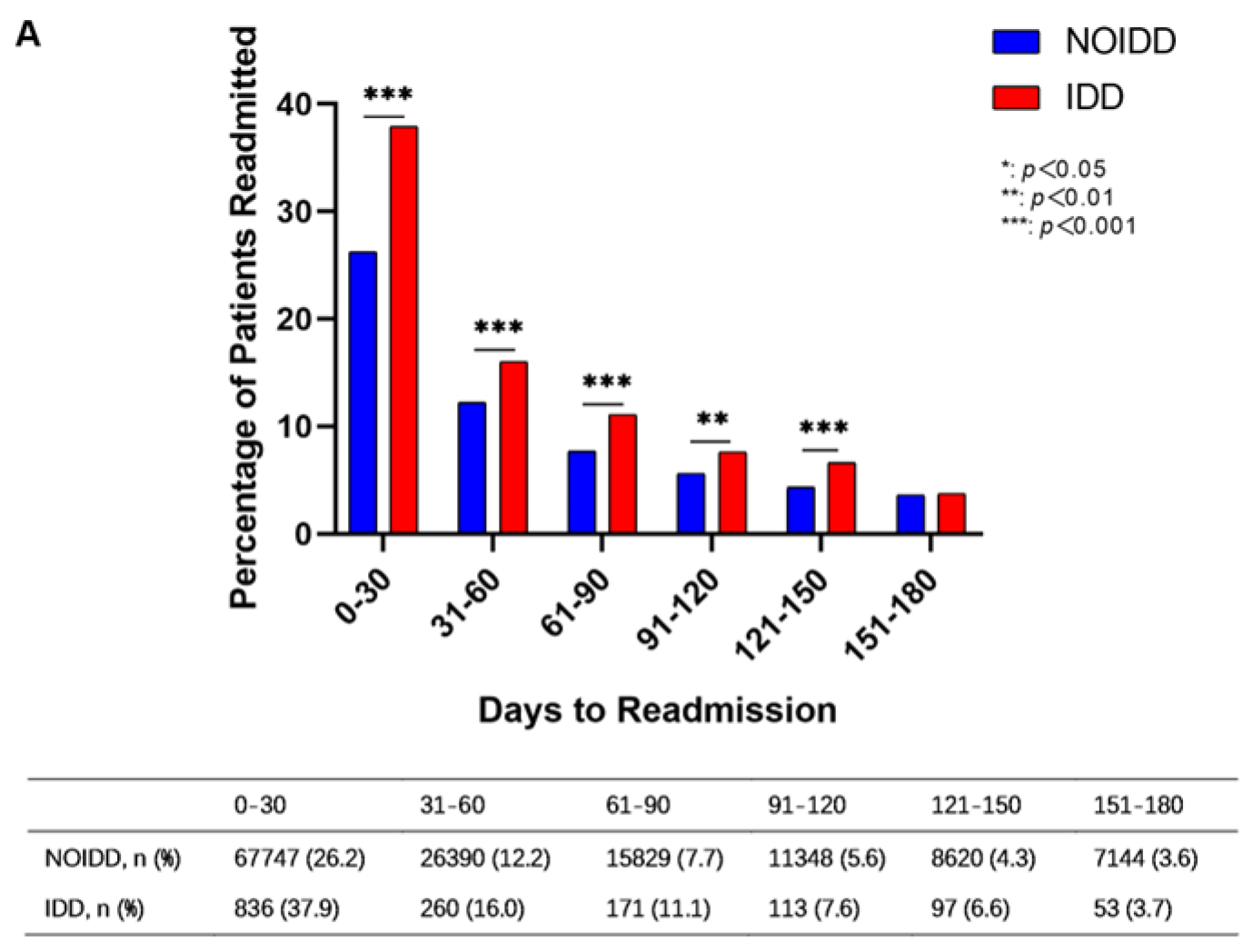
3.3. The Temporality and the Category of Readmissions
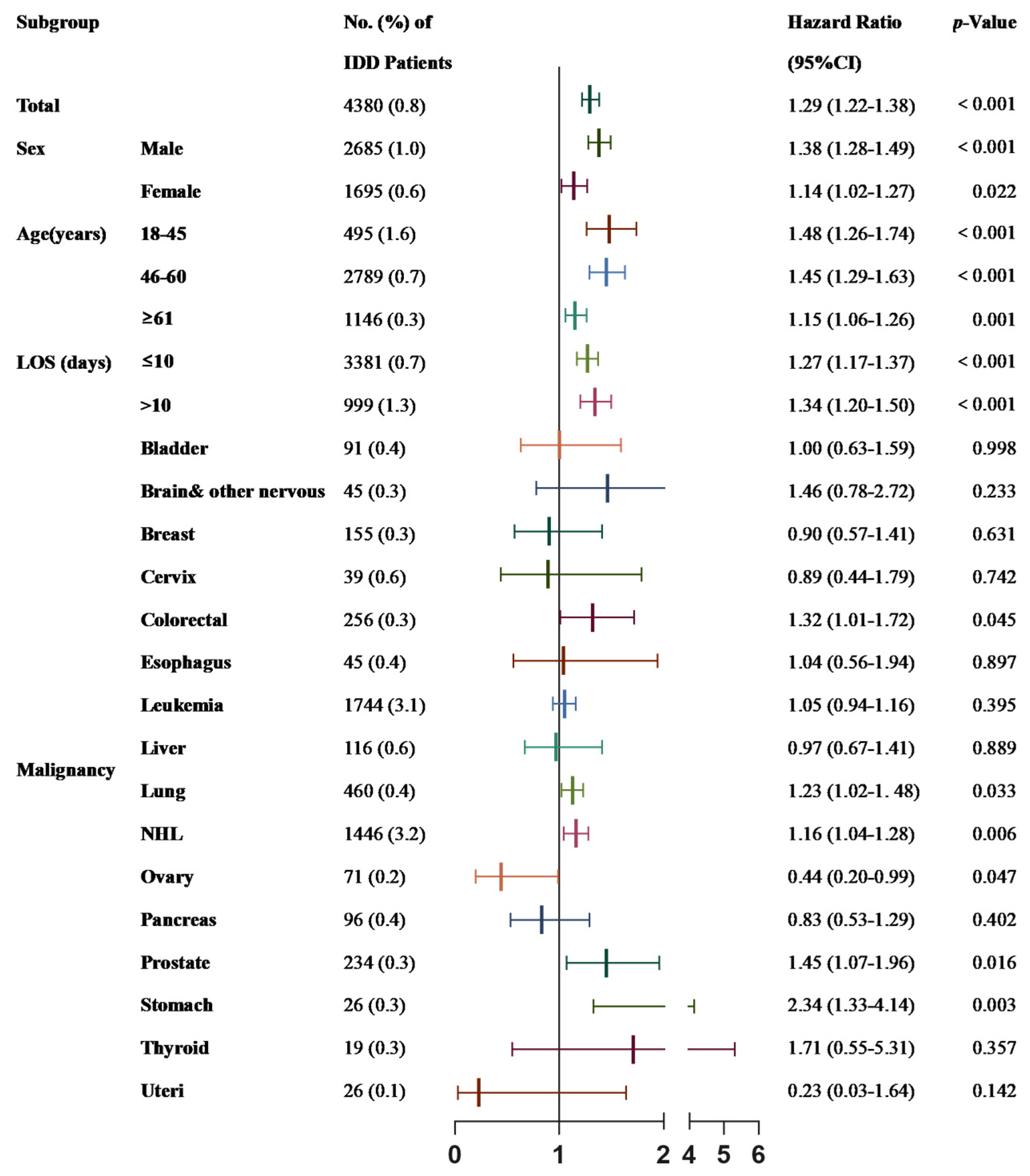
3.4. Subgroup Analysis of 30-Day Unplanned Readmission
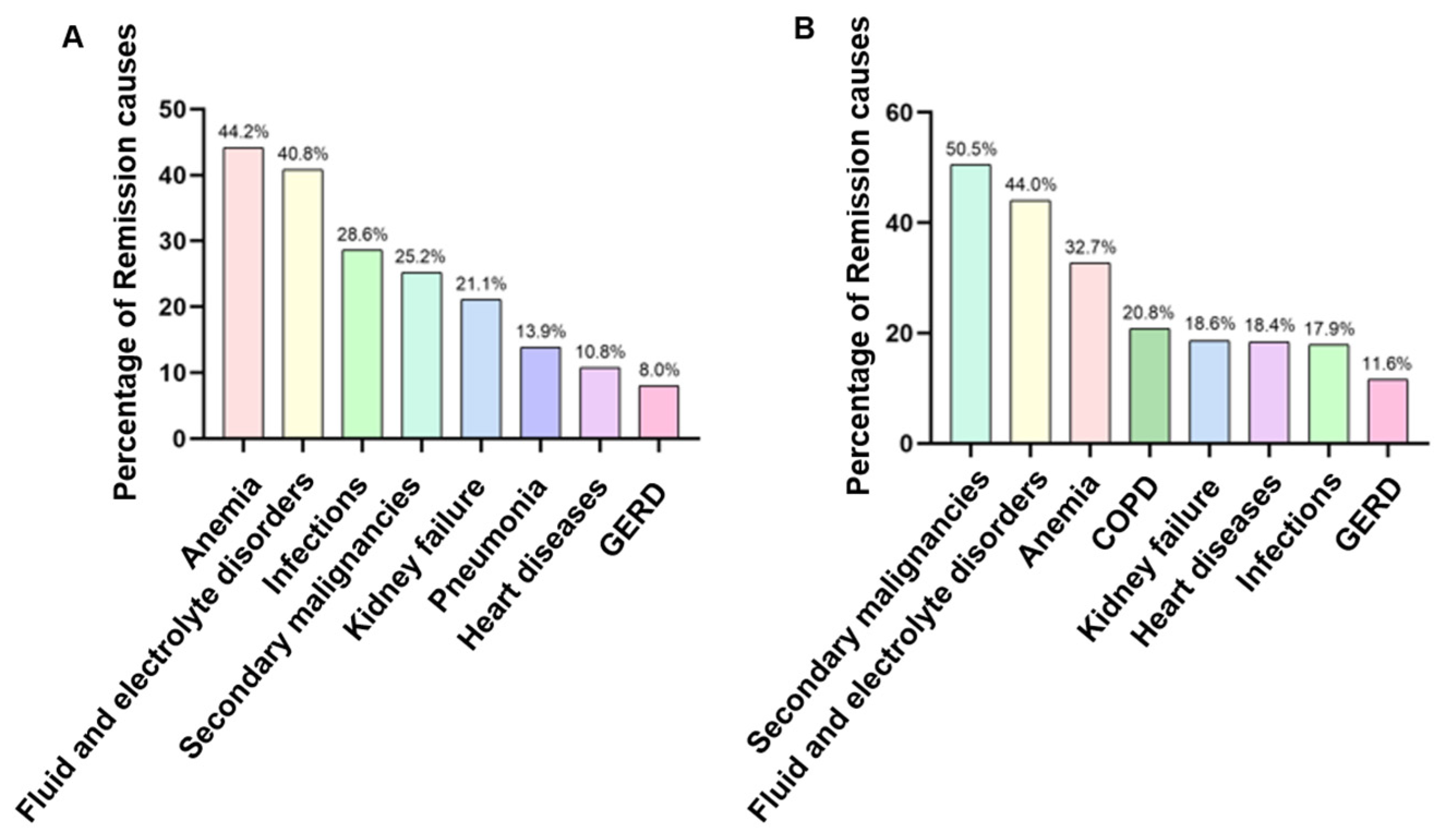
3.5. The Causes of 30-Day Unplanned Readmissions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stratton, M.R.; Campbell, P.J.; Futreal, P.A. The cancer genome. Nature 2009, 458, 719–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Jiménez, F.; Muiños, F.; Sentís, I.; Deu-Pons, J.; Reyes-Salazar, I.; Arnedo-Pac, C.; Lopez-Bigas, N. A compendium of mutational cancer driver genes. Nat. Rev. Cancer 2020, 20, 555–572. [Google Scholar] [CrossRef] [PubMed]
- Coulie, P.G.; Van den Eynde, B.J.; van der Bruggen, P.; Boon, T. Tumour antigens recognized by T lymphocytes: At the core of cancer immunotherapy. Nat. Rev. Cancer 2014, 14, 135–146. [Google Scholar] [CrossRef]
- Jhunjhunwala, S.; Hammer, C.; Delamarre, L. Antigen presentation in cancer: Insights into tumour immunogenicity and immune evasion. Nat. Rev. Cancer 2021, 21, 298–312. [Google Scholar] [CrossRef] [PubMed]
- Lang, F.; Schrörs, B.; Löwer, M.; Türeci, Ö.; Sahin, U. Identification of neoantigens for individualized therapeutic cancer vaccines. Nat. Rev. Drug Discov. 2022, 21, 261–282. [Google Scholar] [CrossRef]
- Chan, T.A.; Wolchok, J.D.; Snyder, A. Genetic Basis for Clinical Response to CTLA-4 Blockade in Melanoma. N. Engl. J. Med. 2015, 373, 1984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leidner, R.; Sanjuan Silva, N.; Huang, H.; Sprott, D.; Zheng, C.; Shih, Y.P.; Tran, E. Neoantigen T-Cell Receptor Gene Therapy in Pancreatic Cancer. N. Engl. J. Med. 2022, 386, 2112–2119. [Google Scholar] [CrossRef] [PubMed]
- Jaillon, S.; Ponzetta, A.; Di Mitri, D.; Santoni, A.; Bonecchi, R.; Mantovani, A. Neutrophil diversity and plasticity in tumour progression and therapy. Nat. Rev. Cancer 2020, 20, 485–503. [Google Scholar] [CrossRef]
- Vitale, I.; Manic, G.; Coussens, L.M.; Kroemer, G.; Galluzzi, L. Macrophages and Metabolism in the Tumor Microenvironment. Cell Metab. 2019, 30, 36–50. [Google Scholar] [CrossRef]
- Wolf, N.K.; Kissiov, D.U.; Raulet, D.H. Roles of natural killer cells in immunity to cancer, and applications to immunotherapy. Nat. Rev. Immunol. 2022; ahead of print. [Google Scholar] [CrossRef]
- Sun, J.M.; Shen, L.; Shah, M.A.; Enzinger, P.; Adenis, A.; Doi, T.; KEYNOTE-590 Investigators. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): A randomised, placebo-controlled, phase 3 study. Lancet 2021, 398, 759–771. [Google Scholar] [CrossRef] [PubMed]
- Forde, P.M.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Girard, N. Neoadjuvant Nivolumab Plus Chemotherapy in Resectable Lung Cancer. N. Engl. J. Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef] [PubMed]
- Theelen, W.S.; Chen, D.; Verma, V.; Hobbs, B.P.; Peulen, H.M.; Aerts, J.G.; Welsh, J.W. Pembrolizumab with or without radiotherapy for metastatic non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet Respir. Med. 2021, 9, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Park, M.A.; Li, J.T.; Hagan, J.B.; Maddox, D.E.; Abraham, R.S. Common variable immunodeficiency: A new look at an old disease. Lancet 2008, 372, 489–502. [Google Scholar] [CrossRef] [PubMed]
- Gathmann, B.; Grimbacher, B.; Beauté, J.; Dudoit, Y.; Mahlaoui, N.; Fischer, A.; Kindle, G. The European internet-based patient and research database for primary immunodeficiencies: Results 2004–06. Clin. Exp. Immunol. 2007, 147, 306–312. [Google Scholar]
- Kinlen, L.J.; Webster AD, B.; Bird, A.G.; Haile, R.; Peto, J.; Soothill, J.F.; Thompson, R.A. Prospective study of cancer in patients with hypogammaglobulinaemia. Lancet 1985, 1, 263–266. [Google Scholar] [CrossRef]
- Kralickova, P.; Milota, T.; Litzman, J.; Malkusova, I.; Jilek, D.; Petanova, J.; Sediva, A. CVID-Associated Tumors: Czech Nationwide Study Focused on Epidemiology, Immunology, and Genetic Background in a Cohort of Patients With CVID. Front. Immunol. 2018, 9, 3135. [Google Scholar] [CrossRef] [Green Version]
- Smit, M.; Brinkman, K.; Geerlings, S.; Smit, C.; Thyagarajan, K.; van Sighem, A.; Hallett, T.B. Future challenges for clinical care of an ageing population infected with HIV: A modelling study. Lancet Infect. Dis. 2015, 15, 810–818. [Google Scholar] [CrossRef] [Green Version]
- Yarchoan, R.; Uldrick, T.S. HIV-Associated Cancers and Related Diseases. N. Engl. J. Med. 2018, 378, 1029–1041. [Google Scholar] [CrossRef]
- Morlat, P.; Roussillon, C.; Henard, S.; Salmon, D.; Bonnet, F.; Cacoub, P.; ANRS EN20 Mortalité 2010 Study Group. Causes of death among HIV-infected patients in France in 2010 (national survey): Trends since 2000. Aids 2014, 28, 1181–1191. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Ramírez, R.U.; Shiels, M.S.; Dubrow, R.; Engels, E.A. Cancer risk in HIV-infected people in the USA from 1996 to 2012: A population-based, registry-linkage study. Lancet HIV 2017, 4, e495–e504. [Google Scholar] [CrossRef] [PubMed]
- AHRQ. Introduction to the HCUP Nationwide Readmissions Database(NRD) 2010–2018. 2020. Available online: https://datasetdirectory.disabilitystatistics.org/show/43 (accessed on 21 November 2022).
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Tangye, S.G.; Al-Herz, W.; Bousfiha, A.; Chatila, T.; Cunningham-Rundles, C.; Etzioni, A.; Sullivan, K.E. Human Inborn Errors of Immunity: 2019 Update on the Classification from the International Union of Immunological Societies Expert Committee. J. Clin. Immunol. 2020, 40, 24–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tangye, S.G.; Al-Herz, W.; Bousfiha, A.; Cunningham-Rundles, C.; Franco, J.L.; Holland, S.M.; Meyts, I. The Ever-Increasing Array of Novel Inborn Errors of Immunity: An Interim Update by the IUIS Committee. J. Clin. Immunol. 2021, 41, 666–679. [Google Scholar] [CrossRef]
- Nagata, N.; Nishijima, T.; Niikura, R.; Yokoyama, T.; Matsushita, Y.; Watanabe, K.; Gatanaga, H. Increased risk of non-AIDS-defining cancers in Asian HIV-infected patients: A long-term cohort study. BMC Cancer 2018, 18, 1066. [Google Scholar] [CrossRef] [Green Version]
- Quinti, I.; Agostini, C.; Tabolli, S.; Brunetti, G.; Cinetto, F.; Pecoraro, A.; Spadaro, G. Malignancies are the major cause of death in patients with adult onset common variable immunodeficiency. Blood 2012, 120, 1953–1954. [Google Scholar] [CrossRef]
- Jencks, S.F.; Williams, M.V.; Coleman, E.A. Rehospitalizations among patients in the Medicare fee-for-service program. N. Engl. J. Med. 2009, 360, 1418–1428. [Google Scholar] [CrossRef]
- Nipp, R.D.; Horick, N.K.; Qian, C.L.; Knight, H.P.; Kaslow-Zieve, E.R.; Azoba, C.C.; Temel, J.S. Effect of a Symptom Monitoring Intervention for Patients Hospitalized With Advanced Cancer: A Randomized Clinical Trial. JAMA Oncol. 2022, 8, 571–578. [Google Scholar] [CrossRef]
- McHugh, M.D.; Aiken, L.H.; Sloane, D.M.; Windsor, C.; Douglas, C.; Yates, P. Effects of nurse-to-patient ratio legislation on nurse staffing and patient mortality, readmissions, and length of stay: A prospective study in a panel of hospitals. Lancet 2021, 397, 1905–1913. [Google Scholar] [CrossRef]
- Bonilla, F.A.; Barlan, I.; Chapel, H.; Costa-Carvalho, B.T.; Cunningham-Rundles, C.; de la Morena, M.T.; Warnatz, K. International Consensus Document (ICON): Common Variable Immunodeficiency Disorders. J. Allergy Clin. Immunol. Pract. 2016, 4, 38–59. [Google Scholar] [CrossRef] [Green Version]
- Cunningham-Rundles, C.; Bodian, C. Common variable immunodeficiency: Clinical and immunological features of 248 patients. Clin. Immunol. 1999, 92, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Klocperk, A.; Friedmann, D.; Schlaak, A.E.; Unger, S.; Parackova, Z.; Goldacker, S.; Warnatz, K. Distinct CD8 T Cell Populations with Differential Exhaustion Profiles Associate with Secondary Complications in Common Variable Immunodeficiency. J. Clin. Immunol 2022, 42, 1254–1269. [Google Scholar] [CrossRef] [PubMed]
- Ueckermann, V.; Janse van Rensburg, L.; Pannell, N.; Ehlers, M. Characteristics and outcomes of patients admitted to a tertiary academic hospital in Pretoria with HIV and severe pneumonia: A retrospective cohort study. BMC Infect. Dis. 2022, 22, 548. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.D. Human immunodeficiency virus infection, anemia, and survival. Clin. Infect. Dis. 1999, 29, 44–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volberding, P.A.; Levine, A.M.; Dieterich, D.; Mildvan, D.; Mitsuyasu, R.; Saag, M. Anemia in HIV infection: Clinical impact and evidence-based management strategies. Clin. Infect. Dis. 2004, 38, 1454–1463. [Google Scholar] [CrossRef] [Green Version]
- Seidel, M.G. Autoimmune and other cytopenias in primary immunodeficiencies: Pathomechanisms, novel differential diagnoses, and treatment. Blood 2014, 124, 2337–2344. [Google Scholar] [CrossRef] [Green Version]
- Cunningham-Rundles, C. Hematologic complications of primary immune deficiencies. Blood Rev. 2002, 16, 61–64. [Google Scholar] [CrossRef]
- Knight, K.; Wade, S.; Balducci, L. Prevalence and outcomes of anemia in cancer: A systematic review of the literature. Am. J. Med. 2004, 116, 11s–26s. [Google Scholar] [CrossRef]
- Ludwig, H.; Van Belle, S.; Barrett-Lee, P.; Birgegård, G.; Bokemeyer, C.; Gascón, P.; Schrijvers, D. The European Cancer Anaemia Survey (ECAS): A large, multinational, prospective survey defining the prevalence, incidence, and treatment of anaemia in cancer patients. Eur. J. Cancer 2004, 40, 2293–2306. [Google Scholar] [CrossRef]
- Fischl, M.; Galpin, J.E.; Levine, J.D.; Groopman, J.E.; Henry, D.H.; Kennedy, P.; Rudnick, S.A. Recombinant human erythropoietin for patients with AIDS treated with zidovudine. N. Engl. J. Med. 1990, 322, 1488–1493. [Google Scholar] [CrossRef]
- Cunningham-Rundles, C. Common variable immune deficiency: Case studies. Blood 2019, 134, 1787–1795. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Mayer, L. Diagnosis and treatment of gastrointestinal disorders in patients with primary immunodeficiency. Clin. Gastroenterol. Hepatol. 2013, 11, 1050–1063. [Google Scholar] [CrossRef] [Green Version]
- Weiss, G.; Ganz, T.; Goodnough, L.T. Anemia of inflammation. Blood 2019, 133, 40–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gobert, D.; Bussel, J.B.; Cunningham-Rundles, C.; Galicier, L.; Dechartres, A.; Berezne, A.; Michel, M. Efficacy and safety of rituximab in common variable immunodeficiency-associated immune cytopenias: A retrospective multicentre study on 33 patients. Br. J. Haematol. 2011, 155, 498–508. [Google Scholar] [CrossRef] [Green Version]
- Treleaven, J.; Gennery, A.; Marsh, J.; Norfolk, D.; Page, L.; Parker, A.; Webb, D. Guidelines on the use of irradiated blood components prepared by the British Committee for Standards in Haematology blood transfusion task force. Br. J. Haematol. 2011, 152, 35–51. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | IDD | NOIDD | p-Value |
|---|---|---|---|
| No. of cases, n | 4852 | 598,979 | |
| Male, n (%) | 2993 (61.7) | 304,906 (50.9) | <0.001 |
| Age(years), n (%) | <0.001 | ||
| 1. 18–45 | 595 (12.3) | 34,847 (5.8) | |
| 2. 46–60 | 1231 (25.4) | 125,740 (21.0) | |
| 3. ≥61 | 3026 (62.4) | 438,392 (73.2) | |
| Hypertension, n (%) | 2620 (54.0) | 364,731 (60.9) | <0.001 |
| Diabetes, n (%) | 1232 (25.4) | 164,874 (27.5) | 0.001 |
| Hyperlipidemia, n (%) | 1541 (31.8) | 222,625 (37.2) | <0.001 |
| BMI ≥ 25.0, n (%) | 381 (7.9) | 65,897 (11.0) | <0.001 |
| Illness severity, n (%) | <0.001 | ||
| 1. Unclassified, minor and moderate | 972 (20.0) | 276,825 (46.2) | |
| 2. Major and extreme | 3880 (80.0) | 322,154 (53.8) | |
| Mortality risk, n (%) | <0.001 | ||
| 1. Unclassified, minor and moderate | 1894 (39.0) | 314,526 (52.5) | |
| 2. Major and extreme | 2958 (61.0) | 284,453 (47.5) | |
| LOS (days), n (%) | <0.001 | ||
| 1. ≤10 | 4742 (77.1) | 517,390 (86.4) | |
| 2. >10 | 1110 (22.9) | 81,589 (13.6) | |
| Total charges, mean (SE) | 114,912 (219,292) | 81,344 (116,646) | <0.001 |
| Patient location, n (%) | <0.001 | ||
| 1. “Central” counties with population ≥ 1 million | 1580 (32.6) | 170,012 (28.4) | |
| 2. “Fringe” counties with population ≥ 1 million | 1371 (28.3) | 162,637 (27.2) | |
| 3. Population of 250,000–999,999 | 1002 (20.7) | 126,260 (21.1) | |
| 4. Population of 50,000–249,999 | 402 (8.3) | 55,841 (9.3) | |
| 5. Micropolitan counties | 292 (6.0) | 46,925 (7.8) | |
| 6. Not metropolitan or micropolitan counties | 205 (4.2) | 37,304 (6.2) | |
| Primary expected payer, n (%) | <0.001 | ||
| 1. Medicare | 2932 (60.4) | 367,355 (61.3) | |
| 2. Medicaid | 615 (12.7) | 52,496 (8.8) | |
| 3. Private insurance | 1133 (23.4) | 155,192 (25.9) | |
| 4. Self-pay | 91 (1.9) | 9048 (1.5) | |
| 5. No charge | 13 (0.3) | 1248 (0.2) | |
| 6. Others | 68 (1.4) | 13,640 (2.3) | |
| Median household income, n (%) | 0.001 | ||
| 1. 0–25th percentile (USD 1–USD 45,999) | 1224 (25.2) | 141,811 (23.7) | |
| 2. 26th to 50th percentile (USD 46,000–USD 58,999) | 1208 (24.9) | 159,527 (26.6) | |
| 3. 51st to 75th percentile (USD 59,000–USD 78,999) | 1187 (24.5) | 154,022 (25.7) | |
| 4. 76th to 100th percentile (USD 79,000 or more) | 1233 (25.4) | 143,619 (24.0) | |
| Disposition of patient, n (%) | <0.001 | ||
| 1. Routine | 3006 (62.0) | 355,505 (59.4) | |
| 2. Transfer to short-term hospital | 60 (1.2) | 6758 (1.1) | |
| 3. Transfer to other | 627 (12.9) | 87,225 (14.6) | |
| 4. Home health care | 1106 (22.8) | 145,154 (24.2) | |
| 5. Against medical advice | 50 (1.0) | 3992 (0.7) | |
| 6. Discharged alive, destination unknown | 3 (0.1) | 345 (0.1) | |
| Readmission (unadjusted), n (%) | 2293 (47.3) | 219,155 (36.6) | <0.001 |
| Index admission by malignancy | |||
| 1. Bladder | 100 (2.1) | 27,644 (4.6) | <0.001 |
| 2. Brain and other nervous | 50 (1.0) | 16,820 (2.8) | <0.001 |
| 3. Breast | 178 (3.7) | 62,055 (10.4) | <0.001 |
| 4. Cervical | 40 (0.8) | 6930 (1.2) | 0.031 |
| 5. Colorectal | 282 (5.8) | 80,937 (13.5) | <0.001 |
| 6. Esophageal | 49 (1.0) | 11,772 (2.0) | <0.001 |
| 7. Leukemia | 1879 (38.7) | 60,180 (10.0) | <0.001 |
| 8. Liver | 126 (2.6) | 20,883 (3.5) | 0.001 |
| 9. Lung | 494 (10.2) | 117,233 (19.6) | <0.001 |
| 10. non-Hodgkin lymphoma | 1683 (34.7) | 49,378 (8.3) | <0.001 |
| 11. Ovarian | 82 (1.7) | 36,371 (6.1) | <0.001 |
| 12. Pancreatic | 101 (2.1) | 29,573 (4.9) | <0.001 |
| 13. Prostate | 252 (5.2) | 78,727 (13.1) | <0.001 |
| 14. Stomach | 30 (0.6) | 11,417 (1.9) | <0.001 |
| 15. Thyroid | 20 (0.4) | 7291 (1.2) | <0.001 |
| 16. Uterine | 30 (0.6) | 19,585 (3.3) | <0.001 |
| Elective | Immunity Status | 30-Day Adjusted * HR (95% CI) | p-Value | 90-Day Adjusted * HR (95% CI) | p-Value | 180-Day Adjusted * HR (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|
| Uncategorized | NOIDD | 1.0 (ref) | 1.0 (ref) | 1.0 (ref) | |||
| IDD | 1.32 (1.25–1.40) | <0.001 | 1.27 (1.21–1.34) | <0.001 | 1.28 (1.22–1.35) | <0.001 | |
| PR | NOIDD | 1.0 (ref) | 1.0 (ref) | 1.0 (ref) | |||
| IDD | 1.68 (1.46–1.92) | <0.001 | 1.38 (1.22–1.57) | <0.001 | 1.33 (1.17–1.52) | <0.001 | |
| UPR | NOIDD | 1.0 (ref) | 1.0 (ref) | 1.0 (ref) | |||
| IDD | 1.29 (1.22–1.38) | <0.001 | 1.27 (1.21–1.34) | <0.001 | 1.29 (1.22–1.37) | <0.001 |
| Causes of UPR, n (%) | IDD, n = 611 | NOIDD, n = 50,722 | p-Value |
|---|---|---|---|
| Anemia | 270 (44.2) | 16,588 (32.7) | <0.001 |
| Fluid and electrolyte disorders | 249 (40.8) | 22,298 (44.0) | 0.112 |
| Infections | 175 (28.6) | 9099 (17.9) | <0.001 |
| Secondary malignancies | 154 (25.2) | 25,606 (50.5) | <0.001 |
| Kidney failure | 129 (21.1) | 9444 (18.6) | 0.116 |
| Pneumonia | 85 (13.9) | 5397 (10.6) | 0.009 |
| Heart diseases | 66 (10.8) | 9337 (18.4) | <0.001 |
| GERD | 49 (8.0) | 5882 (11.6) | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Meng, Q.; Cheng, Y.; Han, Y.; Xue, Y.; Kuang, Y.; Wang, X.; Ning, B.; Ke, M.; Teng, Z.; et al. Immunodeficiencies Push Readmissions in Malignant Tumor Patients: A Retrospective Cohort Study Based on the Nationwide Readmission Database. Cancers 2023, 15, 88. https://doi.org/10.3390/cancers15010088
Wang W, Meng Q, Cheng Y, Han Y, Xue Y, Kuang Y, Wang X, Ning B, Ke M, Teng Z, et al. Immunodeficiencies Push Readmissions in Malignant Tumor Patients: A Retrospective Cohort Study Based on the Nationwide Readmission Database. Cancers. 2023; 15(1):88. https://doi.org/10.3390/cancers15010088
Chicago/Turabian StyleWang, Wenchen, Qingyu Meng, Yiping Cheng, Yalin Han, Yonggan Xue, Yanshen Kuang, Xuning Wang, Bobin Ning, Mu Ke, Zhipeng Teng, and et al. 2023. "Immunodeficiencies Push Readmissions in Malignant Tumor Patients: A Retrospective Cohort Study Based on the Nationwide Readmission Database" Cancers 15, no. 1: 88. https://doi.org/10.3390/cancers15010088