
Short and Long-Term Surgical Outcomes of Laparoscopic Total Gastrectomy Compared with Open Total Gastrectomy in Gastric Cancer Patients

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcome Assessments
2.3. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics
3.2. Surgical Outcomes
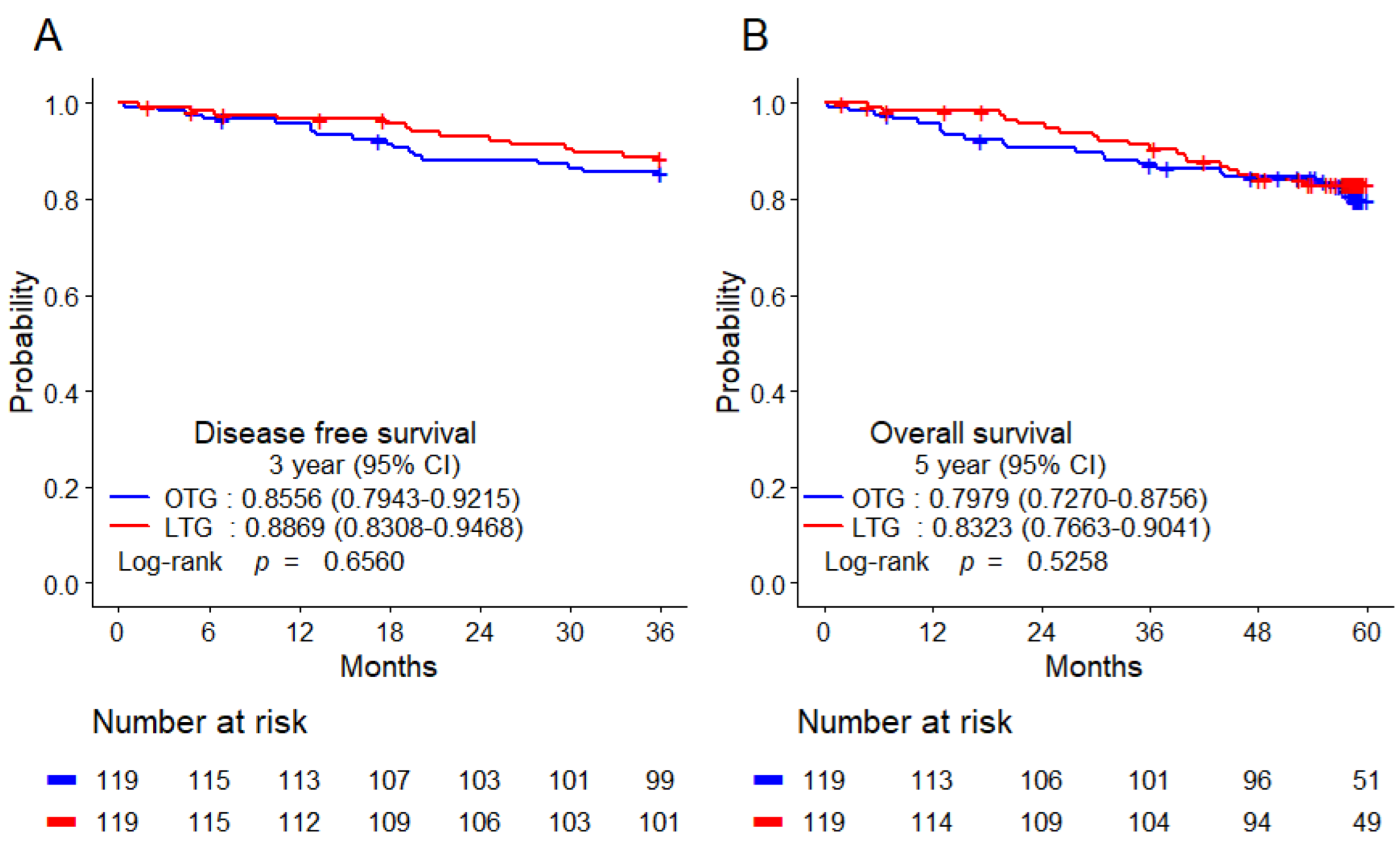
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Hartgrink, H.H.; Jansen, E.P.; van Grieken, N.C.; van de Velde, C.J. Gastric Cancer. Lancet 2009, 374, 477–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Information Committee of the Korean Gastric Cancer Association. Korean Gastric Cancer Association-Led Nationwide Survey on Surgically Treated Gastric Cancers in 2019. J. Gastric Cancer 2021, 21, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Machlowska, J.; Baj, J.; Sitarz, M.; Maciejewski, R.; Sitarz, R. Gastric Cancer: Epidemiology, Risk Factors, Classification, Genomic Characteristics and Treatment Strategies. Int. J. Mol. Sci. 2020, 21, 4012. [Google Scholar] [CrossRef]
- Deans, C.; Yeo, M.S.; Soe, M.Y.; Shabbir, A.; Ti, T.K.; So, J.B. Cancer of the Gastric Cardia Is Rising in Incidence in an Asian Population and Is Associated with Adverse Outcome. World J. Surg. 2011, 35, 617–624. [Google Scholar] [CrossRef]
- Park, S.H.; Kang, M.J.; Yun, E.H.; Jung, K.W. Epidemiology of Gastric Cancer in Korea: Trends in Incidence and Survival Based on Korea Central Cancer Registry Data (1999–2019). J. Gastric Cancer 2022, 22, 160–168. [Google Scholar] [CrossRef]
- Eom, S.S.; Choi, W.; Eom, B.W.; Park, S.H.; Kim, S.J.; Kim, Y.I.; Yoon, H.M.; Lee, J.Y.; Kim, C.G.; Kim, H.K.; et al. A Comprehensive and Comparative Review of Global Gastric Cancer Treatment Guidelines. J. Gastric Cancer 2022, 22, 3–23. [Google Scholar] [CrossRef]
- Lee, J.H.; Nam, B.H.; Ryu, K.W.; Ryu, S.Y.; Park, Y.K.; Kim, S.; Kim, Y.W. Comparison of Outcomes After Laparoscopy-Assisted and Open Total Gastrectomy for Early Gastric Cancer. Br. J. Surg. 2015, 102, 1500–1505. [Google Scholar] [CrossRef]
- Li, G.Z.; Doherty, G.M.; Wang, J. Surgical Management of Gastric Cancer: A Review. JAMA Surg. 2022, 157, 446–454. [Google Scholar] [CrossRef]
- Buia, A.; Stockhausen, F.; Hanisch, E. Laparoscopic Surgery: A Qualified Systematic Review. World J. Methodol. 2015, 5, 238–254. [Google Scholar] [CrossRef]
- Kim, W.; Kim, H.H.; Han, S.U.; Kim, M.C.; Hyung, W.J.; Ryu, S.W.; Cho, G.S.; Kim, C.Y.; Yang, H.K.; Park, D.J.; et al. Decreased Morbidity of Laparoscopic Distal Gastrectomy Compared with Open Distal Gastrectomy for Stage I Gastric Cancer: Short-Term Outcomes from a Multicenter Randomized Controlled Trial (KLASS-01). Ann. Surg. 2016, 263, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Hyung, W.J.; Yang, H.K.; Han, S.U.; Park, Y.K.; An, J.Y.; Kim, W.; Kim, H.I.; Kim, H.H.; Ryu, S.W.; et al. Short-Term Outcomes of a Multicenter Randomized Controlled Trial Comparing Laparoscopic Distal Gastrectomy with D2 Lymphadenectomy to Open Distal Gastrectomy for Locally Advanced Gastric Cancer (KLASS-02-RCT). Ann. Surg. 2019, 270, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.H.; Han, S.U.; Kim, M.C.; Kim, W.; Lee, H.J.; Ryu, S.W.; Cho, G.S.; Kim, C.Y.; Yang, H.K.; Park, D.J.; et al. Effect of Laparoscopic Distal Gastrectomy vs Open Distal Gastrectomy on Long-Term Survival Among Patients with Stage I Gastric Cancer: The KLASS-01 Randomized Clinical Trial. JAMA Oncol. 2019, 5, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Hyung, W.J.; Yang, H.K.; Park, Y.K.; Lee, H.J.; An, J.Y.; Kim, W.; Kim, H.I.; Kim, H.H.; Ryu, S.W.; Hur, H.; et al. Long-Term Outcomes of Laparoscopic Distal Gastrectomy for Locally Advanced Gastric Cancer: The KLASS-02-RCT Randomized Clinical Trial. J. Clin. Oncol. 2020, 38, 3304–3313. [Google Scholar] [CrossRef]
- Nakamura, K.; Katai, H.; Mizusawa, J.; Yoshikawa, T.; Ando, M.; Terashima, M.; Ito, S.; Takagi, M.; Takagane, A.; Ninomiya, M.; et al. A Phase III Study of Laparoscopy-Assisted Versus Open Distal Gastrectomy with Nodal Dissection for Clinical Stage IA/IB Gastric Cancer (JCOG0912). Jpn. J. Clin. Oncol. 2013, 43, 324–327. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Huang, C.; Sun, Y.; Su, X.; Cao, H.; Hu, J.; Wang, K.; Suo, J.; Tao, K.; He, X.; et al. Effect of Laparoscopic vs Open Distal Gastrectomy on 3-Year Disease-Free Survival in Patients with Locally Advanced Gastric Cancer: The CLASS-01 Randomized Clinical Trial. JAMA 2019, 321, 1983–1992. [Google Scholar] [CrossRef] [Green Version]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Gastric Cancer. v. 3. Volume 2021. Available online: https://www.nccn.org (accessed on 13 July 2021).
- Wang, F.H.; Zhang, X.T.; Li, Y.F.; Tang, L.; Qu, X.J.; Ying, J.E.; Zhang, J.; Sun, L.Y.; Lin, R.B.; Qiu, H.; et al. The Chinese Society of Clinical Oncology (CSCO): Clinical Guidelines for the Diagnosis and Treatment of Gastric Cancer, 2021. Cancer Commun. 2021, 41, 747–795. [Google Scholar] [CrossRef]
- Okabe, H.; Tsunoda, S.; Tanaka, E.; Hisamori, S.; Kawada, H.; Sakai, Y. Is Laparoscopic Total Gastrectomy a Safe Operation? A Review of Various Anastomotic Techniques and Their Outcomes. Surg. Today 2015, 45, 549–558. [Google Scholar] [CrossRef]
- Han, W.H.; Oh, Y.J.; Eom, B.W.; Yoon, H.M.; Kim, Y.W.; Ryu, K.W. A Comparative Study of the Short-Term Operative Outcome Between Intracorporeal and Extracorporeal Anastomoses During Laparoscopic Total Gastrectomy. Surg. Endosc. 2021, 35, 1602–1609. [Google Scholar] [CrossRef]
- Pang, H.Y.; Zhao, L.Y.; Zhang, Z.Q.; Galiullin, D.; Chen, X.L.; Liu, K.; Zhang, W.H.; Yang, K.; Chen, X.Z.; Hu, J.K. Comparisons of Perioperative and Survival Outcomes of Laparoscopic Versus Open Gastrectomy for Serosa-Positive (pT4a) Gastric Cancer Patients: A Propensity Score Matched Analysis. Langenbecks Arch. Surg. 2021, 406, 641–650. [Google Scholar] [CrossRef]
- Gambhir, S.; Inaba, C.S.; Whealon, M.; Sujatha-Bhaskar, S.; Pejcinovska, M.; Nguyen, N.T. Short- and Long-Term Survival After Laparoscopic Versus Open Total Gastrectomy for Gastric Adenocarcinoma: A National Database Study. Surg. Endosc. 2021, 35, 1872–1878. [Google Scholar] [CrossRef] [PubMed]
- Guideline Committee of the Korean Gastric Cancer Association (KGCA); Development Working Group & Review Panel. Korean practice guideline for gastric cancer 2018: An evidence-based, multi-disciplinary approach. J. Gastric Cancer 2019, 19, 1–48. [Google Scholar] [CrossRef] [PubMed]
- Information Committee of Korean Gastric Cancer Association. Korean Gastric Cancer Association Nationwide Survey on Gastric Cancer in 2014. J. Gastric Cancer 2016, 16, 131–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, D.H.; Son, S.Y.; Park, Y.S.; Shin, D.J.; Ahn, H.S.; Ahn, S.H.; Park, D.J.; Kim, H.H. The Learning Curve Associated With Laparoscopic Total Gastrectomy. Gastric Cancer 2016, 19, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Etoh, T.; Honda, M.; Kumamaru, H.; Miyata, H.; Yoshida, K.; Kodera, Y.; Kakeji, Y.; Inomata, M.; Konno, H.; Seto, Y.; et al. Morbidity and Mortality From a Propensity Score-Matched, Prospective Cohort Study of Laparoscopic Versus Open Total Gastrectomy for Gastric Cancer: Data From a Nationwide Web-Based Database. Surg. Endosc. 2018, 32, 2766–2773. [Google Scholar] [CrossRef]
- Jeong, O.; Jung, M.R.; Kim, G.Y.; Kim, H.S.; Ryu, S.Y.; Park, Y.K. Comparison of Short-Term Surgical Outcomes Between Laparoscopic and Open Total Gastrectomy for Gastric Carcinoma: Case-Control Study Using Propensity Score Matching Method. J. Am. Coll. Surg. 2013, 216, 184–191. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, B.S.; Lee, I.S.; Lee, S.; Yook, J.H.; Kim, B.S. Comparison of Totally Laparoscopic Total Gastrectomy and Open Total Gastrectomy for Gastric Cancer. J. Laparoendosc. Adv. Surg. Tech. A 2013, 23, 323–331. [Google Scholar] [CrossRef]
- Bo, T.; Peiwu, Y.; Feng, Q.; Yongliang, Z.; Yan, S.; Yingxue, H.; Huaxing, L. Laparoscopy-Assisted vs. Open Total Gastrectomy for Advanced Gastric Cancer: Long-Term Outcomes and Technical Aspects of a Case-Control Study. J. Gastrointest. Surg. 2013, 17, 1202–1208. [Google Scholar] [CrossRef]
- Zhang, F.; Lan, Y.; Tang, B.; Hao, Y.; Shi, Y.; Yu, P. Comparative Study of Laparoscopy-Assisted and Open Radical Gastrectomy for Stage T4a Gastric Cancer. Int. J. Surg. 2017, 41, 23–27. [Google Scholar] [CrossRef]
- Shida, A.; Mitsumori, N.; Fujioka, S.; Takano, Y.; Iwasaki, T.; Takahashi, N.; Ishibashi, Y.; Omura, N.; Yanaga, K. Comparison of Short-Term and Long-Term Clinical Outcomes Between Laparoscopic and Open Total Gastrectomy for Patients with Gastric Cancer. Surg. Laparosc. Endosc. Percutan. Tech. 2016, 26, 319–323. [Google Scholar] [CrossRef]
- Kim, K.H.; Kim, Y.M.; Kim, M.C.; Jung, G.J. Is Laparoscopy-Assisted Total Gastrectomy Feasible for the Treatment of Gastric Cancer? A Case-Matched Study. Dig. Surg. 2013, 30, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Yu, D.; Li, Y.; Fan, C.; Li, G. Laparoscopic Versus Open Gastrectomy for Advanced Gastric Cancer: A Meta-analysis Based on High-Quality Retrospective Studies and Clinical Randomized Trials. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Xu, X.W.; Mou, Y.P.; Pan, Y.; Zhou, Y.C.; Zhang, R.C.; Wu, D. Systematic Review and Meta-analysis of Laparoscopic and Open Gastrectomy for Advanced Gastric Cancer. World J. Surg. Oncol. 2013, 11, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.K.; Hyung, W.J.; Han, S.U.; Lee, Y.J.; Park, J.M.; Cho, G.S.; Kwon, O.K.; Kong, S.H.; Kim, H.I.; Lee, H.J.; et al. Comparison of Surgical Outcomes Among Different Methods of Esophagojejunostomy in Laparoscopic Total Gastrectomy for Clinical Stage I Proximal Gastric Cancer: Results of a Single-Arm Multicenter Phase II Clinical Trial in Korea, KLASS 03. Surg. Endosc. 2021, 35, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Katai, H.; Mizusawa, J.; Katayama, H.; Kunisaki, C.; Sakuramoto, S.; Inaki, N.; Kinoshita, T.; Iwasaki, Y.; Misawa, K.; Takiguchi, N.; et al. Single-Arm Confirmatory Trial of Laparoscopy-Assisted Total or Proximal Gastrectomy with Nodal Dissection for Clinical Stage I Gastric Cancer: Japan Clinical Oncology Group Study JCOG1401. Gastric Cancer 2019, 22, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Huang, C.; Xu, Z.; Su, X.; Zhao, G.; Ye, J.; Du, X.; Huang, H.; Hu, J.; Li, G.; et al. Morbidity and Mortality of Laparoscopic vs Open Total Gastrectomy for Clinical Stage I Gastric Cancer: The CLASS02 Multicenter Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1590–1597. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Before PSM | After PSM | ||||||
|---|---|---|---|---|---|---|---|---|
| OTG (n = 409) | LTG (n = 151) | SMD | p Value | OTG (n = 119) | LTG (n = 119) | SMD | p Value | |
| Age, years | 59.5 ± 12.9 | 60.6 ± 12.0 | 0.085 | 0.3781 | 60.2 ± 11.6 | 62.3 ± 11.4 | 0.181 | 0.1645 |
| Sex, n (%) | 0.212 | 0.0243 | 0.020 | 0.8745 | ||||
| Male | 295 (72.1) | 94 (62.3) | 94 (79.0) | 93 (78.2) | ||||
| Female | 114 (27.9) | 57 (37.8) | 25 (21.0) | 26 (21.9) | ||||
| BMI | 23.3 ± 3.5 | 23.4 ± 3.2 | 0.027 | 0.7841 | 23.8 ± 3.3 | 23.3 ± 3.1 | 0.151 | 0.2447 |
| ASA score | 0.074 | 0.4191 | 0.035 | 0.7897 | ||||
| I, II | 389 (95.1) | 141 (93.4) | 112 (94.1) | 111 (93.3) | ||||
| III | 20 (4.9) | 10 (6.6) | 7 (5.9) | 8 (6.7) | ||||
| Location | 0.506 | 0.0003 | 0.497 | 0.0032 | ||||
| EG junction | 91 (22.3) | 18 (11.9) | 24 (20.2) | 14 (11.8) | ||||
| Upper | 241 (58.9) | 114 (75.5) | 72 (60.5) | 91 (76.5) | ||||
| Middle | 49 (12.0) | 19 (12.6) | 14 (11.8) | 14 (11.8) | ||||
| Lower | 12 (2.9) | 0 (0) | 8 (6.7) | 0 (0) | ||||
| Duodenum | 5 (1.2) | 0 (0) | 0 (0) | 0 (0) | ||||
| Whole stomach | 11 (2.7) | 0 (0) | 1 (0.8) | 0 (0) | ||||
| Histology | 0.098 | 0.5169 | 0.198 | 0.2440 | ||||
| WD | 72 (17.6) | 32 (21.2) | 29 (24.4) | 30 (25.2) | ||||
| MD | 106 (25.9) | 38 (25.2) | 38 (31.9) | 32 (26.9) | ||||
| PD | 135 (33) | 47 (31.1) | 27 (22.7) | 34 (28.6) | ||||
| SRC | 83 (20.3) | 34 (22.5) | 20 (16.8) | 23 (19.3) | ||||
| Others | 13 (3.2) | 0 (0) | 5 (4.2) | 0 (0) | ||||
| Pathologic stage | 1.541 | <0.0001 | <0.001 | 1 | ||||
| I | 95 (23.2) | 125 (82.8) | 93 (78.2) | 93 (78.2) | ||||
| II | 119 (29.1) | 17 (11.3) | 17 (14.3) | 17 (14.3) | ||||
| III | 148 (36.2) | 9 (6.0) | 9 (7.6) | 9 (7.6) | ||||
| IV | 47 (11.5) | 0 (0) | 0(0) | 0 (0) | ||||
| Tumor size | 0.577 | <0.0001 | 0.040 | 0.7569 | ||||
| < 5 cm | 218 (53.3) | 120 (79.5) | 93 (78.2) | 91 (76.5) | ||||
| ≥ 5 cm | 191 (46.7) | 31 (20.5) | 26 (21.9) | 28 (23.5) | ||||
| LN Dissection | 0.757 | <0.0001 | 0.399 | 0.0025 | ||||
| < D2 | 49 (12) | 66 (43.7) | 29 (24.4) | 51 (42.9) | ||||
| ≥ D2 | 360 (88) | 85 (56.3) | 90 (75.6) | 68 (57.1) | ||||
| Chemotherapy | 1.371 | <0.0001 | 0.126 | 0.3324 | ||||
| No | 124 (30.3) | 130 (86.1) | 92 (77.3) | 98 (82.4) | ||||
| Yes | 285 (69.7) | 21 (13.9) | 27 (22.7) | 21 (17.7) | ||||
| Characteristic | Before PSM | After PSM | ||||||
|---|---|---|---|---|---|---|---|---|
| OTG (n = 409) | LTG (n = 151) | SMD | p Value | OTG (n = 119) | LTG (n = 119) | SMD | p Value | |
| Operating time (min) | 205 (85–605) | 201 (115–480) | 0.098 | 0.5169 | 200 (85–395) | 205 (115–480) | 0.198 | 0.2440 |
| EBL (mL) | 200 (0–2100) | 50 (0–1050) | 0.707 | <0.0001 | 180 (0–1100) | 50 (0–1050) | 0.626 | <0.0001 |
| Positive LN | 1 (0–117) | 0 (0–20) | 0.669 | <0.0001 | 0 (0–26) | 0 (0–20) | 0.017 | 0.5135 |
| Dissected LN | 44 (0–154) | 39 (0–97) | 0.218 | 0.0163 | 37 (0–91) | 38 (2–97) | 0.088 | 0.3058 |
| PRM (cm) | 3 (0–18.5) | 3.1 (0–16.5) | 0.081 | 0.8352 | 3.7 (0–18.5) | 3.1 (0–16.5) | 0.368 | 0.0491 |
| DRM (cm) | 8.8 (0–27.8) | 12.2 (0–25.7) | 0.612 | <0.0001 | 10 (0–27.8) | 12.6 (0–25.7) | 0.402 | 0.0034 |
| HD (day) | 8 (5–120) | 7 (4–95) | 0.050 | 0.0005 | 8 (5–120) | 7 (4–95) | 0.048 | 0.1396 |
| Characteristics | OTG (n = 119) | LTG (n = 119) | p Value |
|---|---|---|---|
| Postoperative complication | |||
| Wound infection | 2(1.7) | 1(0.8) | 1 |
| Fluid collection | 7(5.9) | 1(0.8) | 0.0657 |
| Inflammatory fluid collection | 5(4.2) | 0(0) | 0.0599 |
| Intraabdominal bleeding | 1(0.8) | 2(1.7) | 1 |
| Intestinal obstruction | 3(2.5) | 2(1.7) | 1 |
| Paralytic ileus | 3(2.5) | 3(2.5) | 1 |
| Anastomosis stenosis | 1(0.8) | 2(1.7) | 1 |
| Anastomosis leakage | 3(2.5) | 8(6.7) | 0.1227 |
| Atelectasis | 1(0.8) | 0(0) | 1 |
| Pneumonia | 3(2.5) | 5(4.2) | 0.7219 |
| Urologic | 1(0.8) | 0(0) | 1 |
| Hepatic | 1(0.8) | 0(0) | 1 |
| Cardiac | 1(0.8) | 0(0) | 1 |
| Pancreas | 2(1.7) | 0(0) | 0.4979 |
| Others | 6(5.0) | 5(4.2) | 1 |
| Duodenal stump leakage | 1(0.8) | 1(0.8) | 1 |
| Overall complication (%) | 41(34.5) | 30(25.2) | 0.1191 |
| Clavien–Dindo classification | |||
| Grade I | 13(11.0) | 4(3.4) | 0.0224 |
| Grade II | 8(6.8) | 9(7.6) | 0.8152 |
| Grade IIIa | 15(12.7) | 9(7.6) | 0.1889 |
| Grade IIIb | 3(2.5) | 3(2.5) | 1 |
| Grade IV | 1(0.9) | 5(4.2) | 0.2128 |
| Grade V | 1(0.9) | 0(0) | 0.4979 |
| Clavien–Dindo classification ≥ IIIa | 20(17.0) | 17(14.3) | 0.5722 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eom, S.S.; Park, S.H.; Eom, B.W.; Yoon, H.M.; Kim, Y.-W.; Ryu, K.W. Short and Long-Term Surgical Outcomes of Laparoscopic Total Gastrectomy Compared with Open Total Gastrectomy in Gastric Cancer Patients. Cancers 2023, 15, 76. https://doi.org/10.3390/cancers15010076
Eom SS, Park SH, Eom BW, Yoon HM, Kim Y-W, Ryu KW. Short and Long-Term Surgical Outcomes of Laparoscopic Total Gastrectomy Compared with Open Total Gastrectomy in Gastric Cancer Patients. Cancers. 2023; 15(1):76. https://doi.org/10.3390/cancers15010076
Chicago/Turabian StyleEom, Sang Soo, Sin Hye Park, Bang Wool Eom, Hong Man Yoon, Young-Woo Kim, and Keun Won Ryu. 2023. "Short and Long-Term Surgical Outcomes of Laparoscopic Total Gastrectomy Compared with Open Total Gastrectomy in Gastric Cancer Patients" Cancers 15, no. 1: 76. https://doi.org/10.3390/cancers15010076