
Adherence to the CDK 4/6 Inhibitor Palbociclib and Omission of Dose Management Supported by Pharmacometric Modelling as Part of the OpTAT Study

 , , , , , , , , and
, , , , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Background
1.2. Objectives
1.3. Outcomes
1.4. Hypothesis
2. Methods
2.1. Ethical Considerations and Guidelines
2.2. OpTAT Medication Adherence Study
2.2.1. Study Design and Participants’ Enrolment
2.2.2. Procedures for the Medication Adherence Study
2.3. Database Construction
2.3.1. Patients’ Sociodemographic and Clinical Data
2.3.2. EM Database
2.4. Statistical Analysis
2.4.1. Descriptive Analysis
2.4.2. Implementation
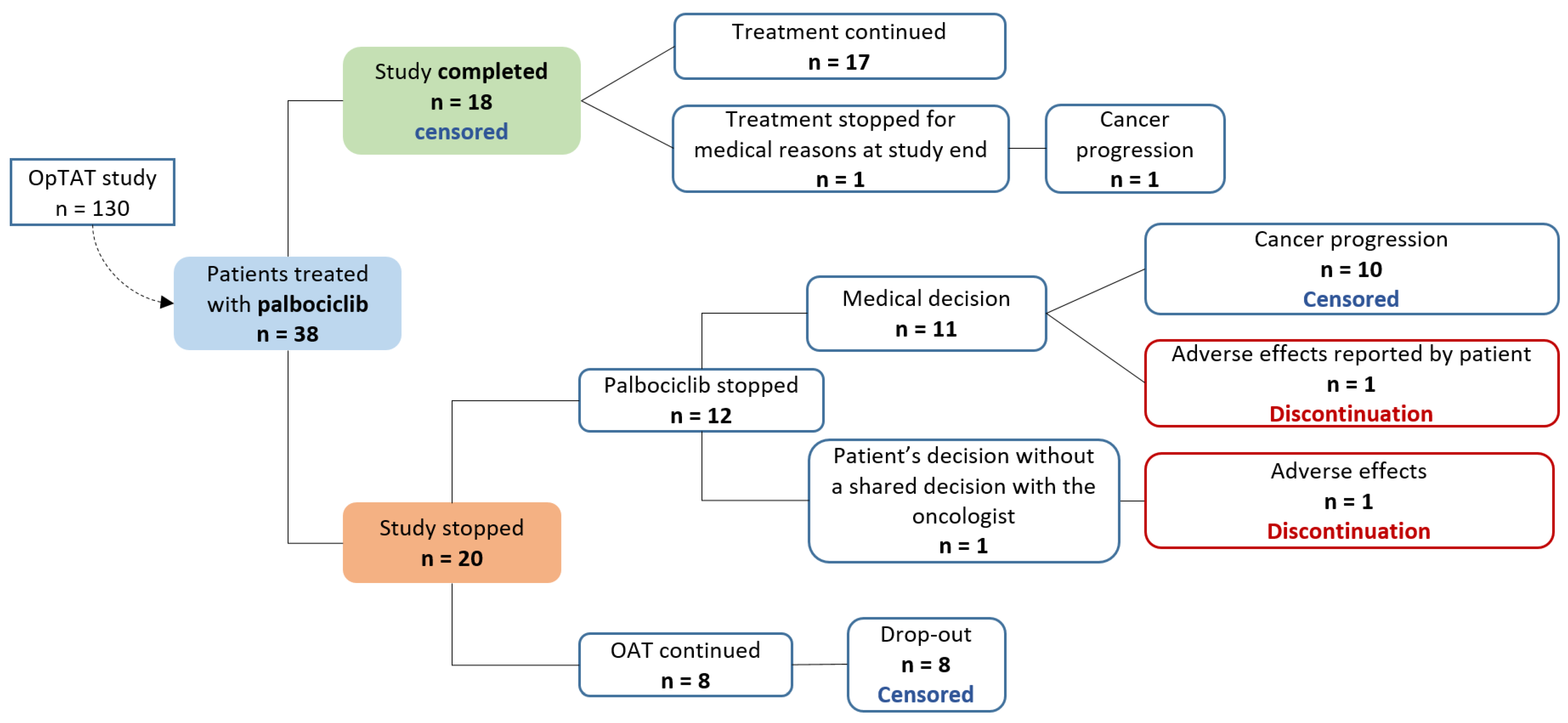
2.4.3. Persistence
2.4.4. Pharmacokinetic Modelling
3. Results
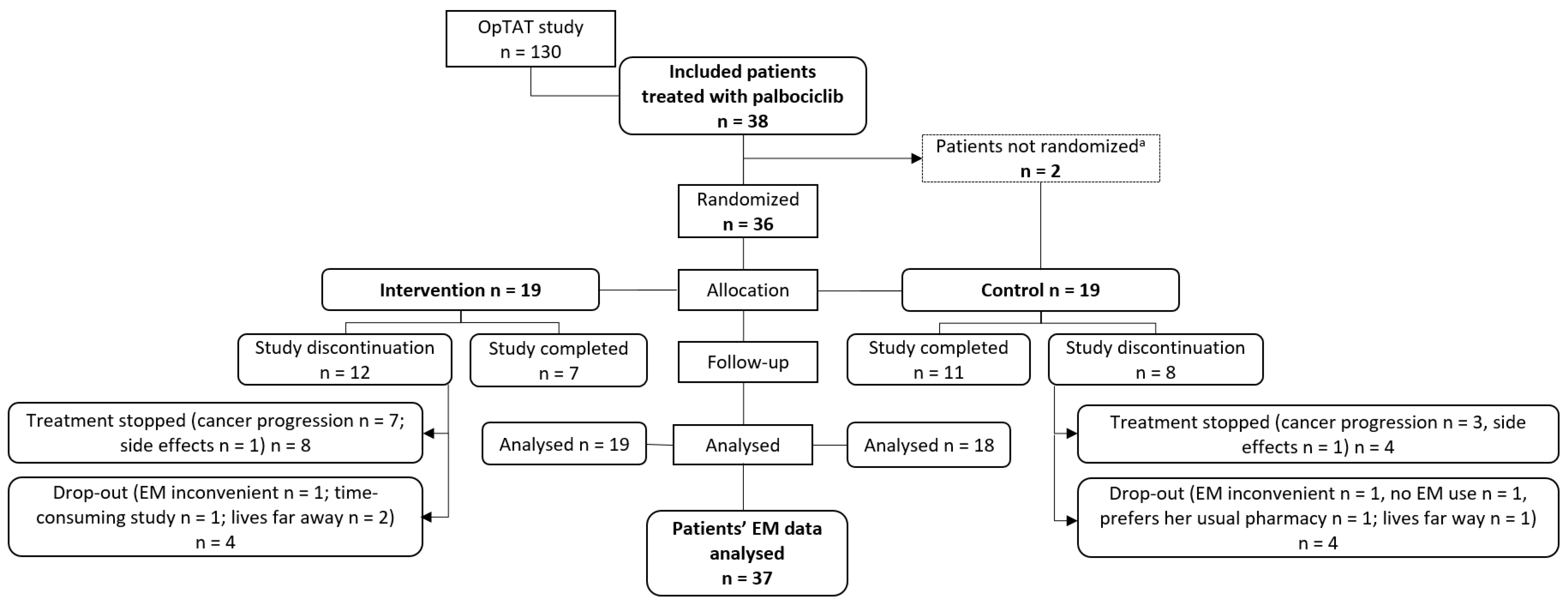
3.1. Included Patients
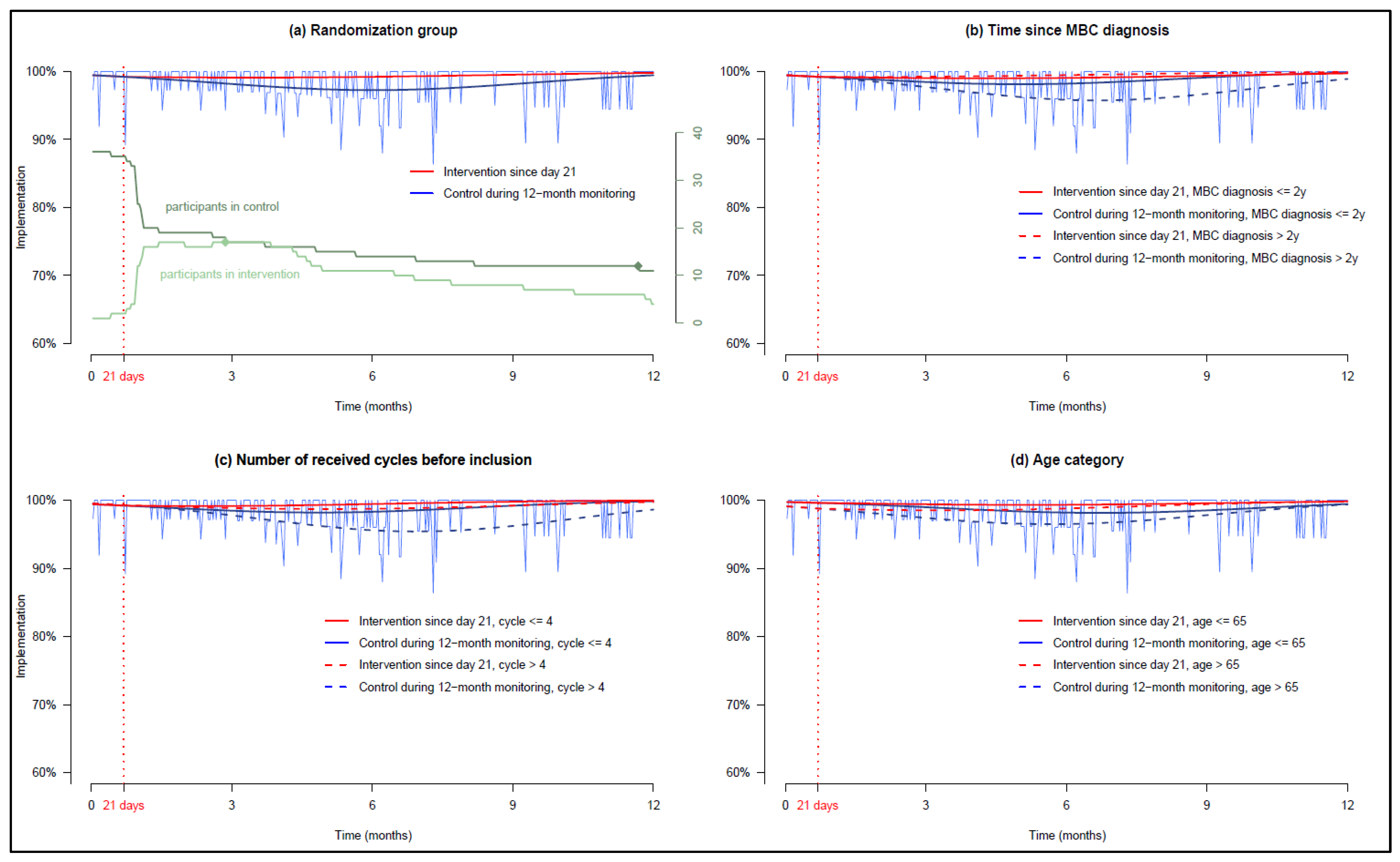
3.2. Palbociclib Implementation and Persistence
3.3. Recommendations for CDK4/6i Cycle Management
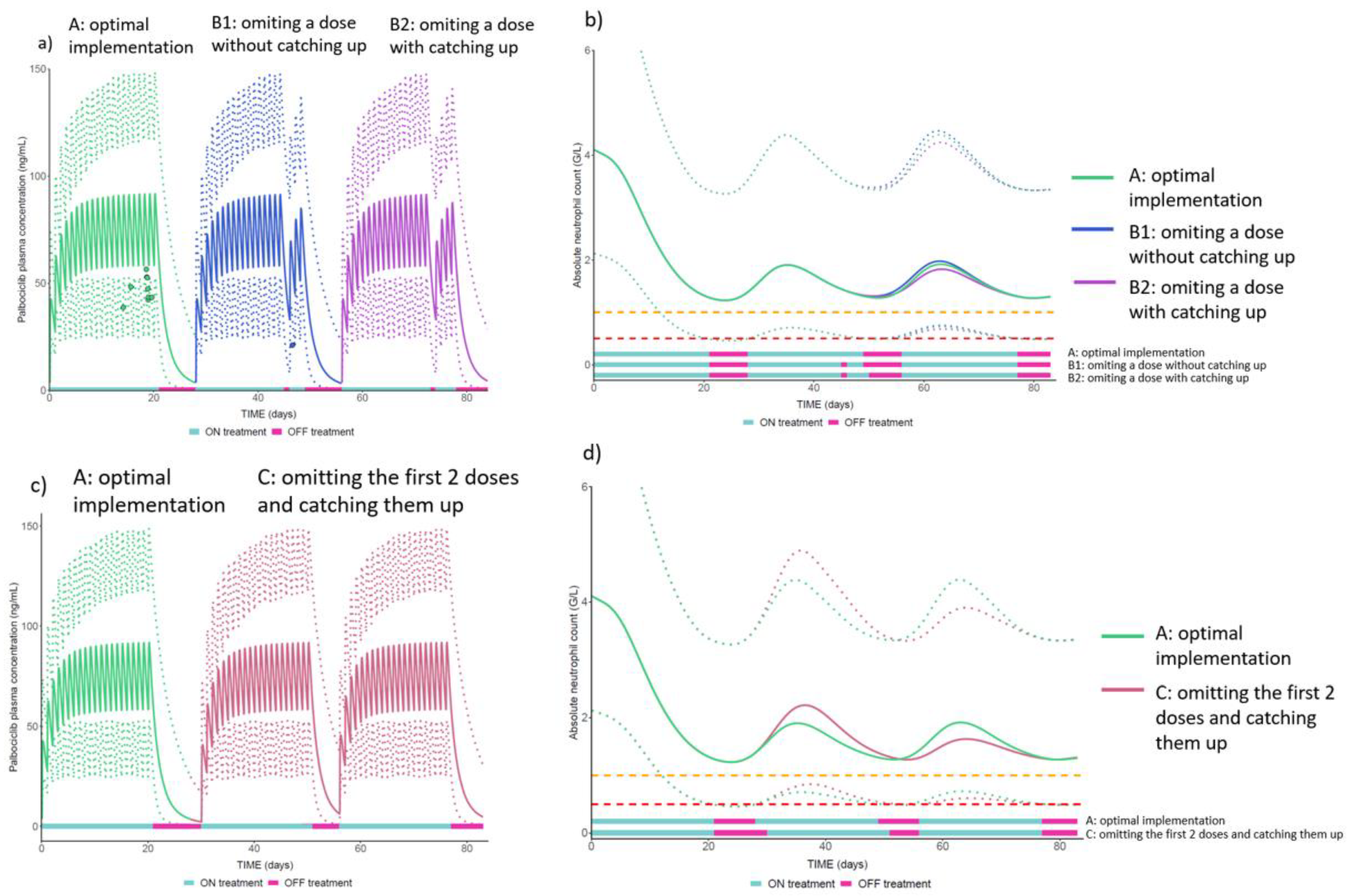
3.3.1. Missed Dose Management Recommendation Supported by Pharmacometric Modelling
3.3.2. Transient Interruption during the ON Phase, Cycle Deferrals and Discrepancies of Cycle Dates in the Electronic Medical Record and the Prescription Sheet
4. Discussion
4.1. Main Results
4.2. Impact of IMAP on Palbociclib Implementation
4.3. Patient Empowerment to Self-Manage CDK4/6i
4.4. Electronic Adherence Monitoring Databases for Cyclic Regimens
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BC | Breast Cancer |
| CDK4i and CDK6i | Cyclin-dependent kinases 4 and 6 inhibitors |
| CI | Confidence interval |
| CHUV | Lausanne University Hospital |
| CONSORT | Consolidated Standards of Reporting Trials |
| COVID | Coronavirus Disease |
| CRF | Case Report Form |
| EMERGE | ESPACOMP Medication Adherence Reporting Guideline |
| GEE | Generalized estimating equation |
| HCPs | Health care providers |
| HR+/HER2− | Endocrine-sensitive and human epidermal growth factor receptor 2 negative |
| HIV | Human Immunodeficiency Virus |
| IMAP | Interprofessional Medication Adherence Program |
| IQR | Interquartile ranges |
| EM | Electronic monitor |
| MBC | Metastatic breast cancer |
| OAT | Oral anticancer therapies |
| OpTAT | Optimizing Targeted Anticancer Therapies study |
| PK-PD | Pharmacokinetics/pharmacodynamics |
| PI | Prediction Interval |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| At 6 Months | Implementation (%) | ||||
|---|---|---|---|---|---|
| Intervention | Control | Difference | 95%CI | ||
| 99.20 | 97.25 | 1.95 | 1.11 | 2.87 | |
| Number of received palbociclib cycles at inclusion ≤4 | 99.43 | 98.28 | 1.15 | 0.40 | 1.96 |
| Number of received palbociclib cycles at inclusion >4 | 98.74 | 95.62 | 3.12 | 1.69 | 4.75 |
| Time since MBC ≤2 years | 99.04 | 98.19 | 0.85 | −0.04 | 1.72 |
| Time since MBC >2 years | 99.45 | 95.85 | 3.60 | 2.06 | 5.36 |
| Age ≤65 years old | 99.33 | 98.19 | 1.14 | 0.36 | 2.09 |
| Age >65 years old | 98.78 | 96.49 | 2.28 | 0.83 | 3.63 |
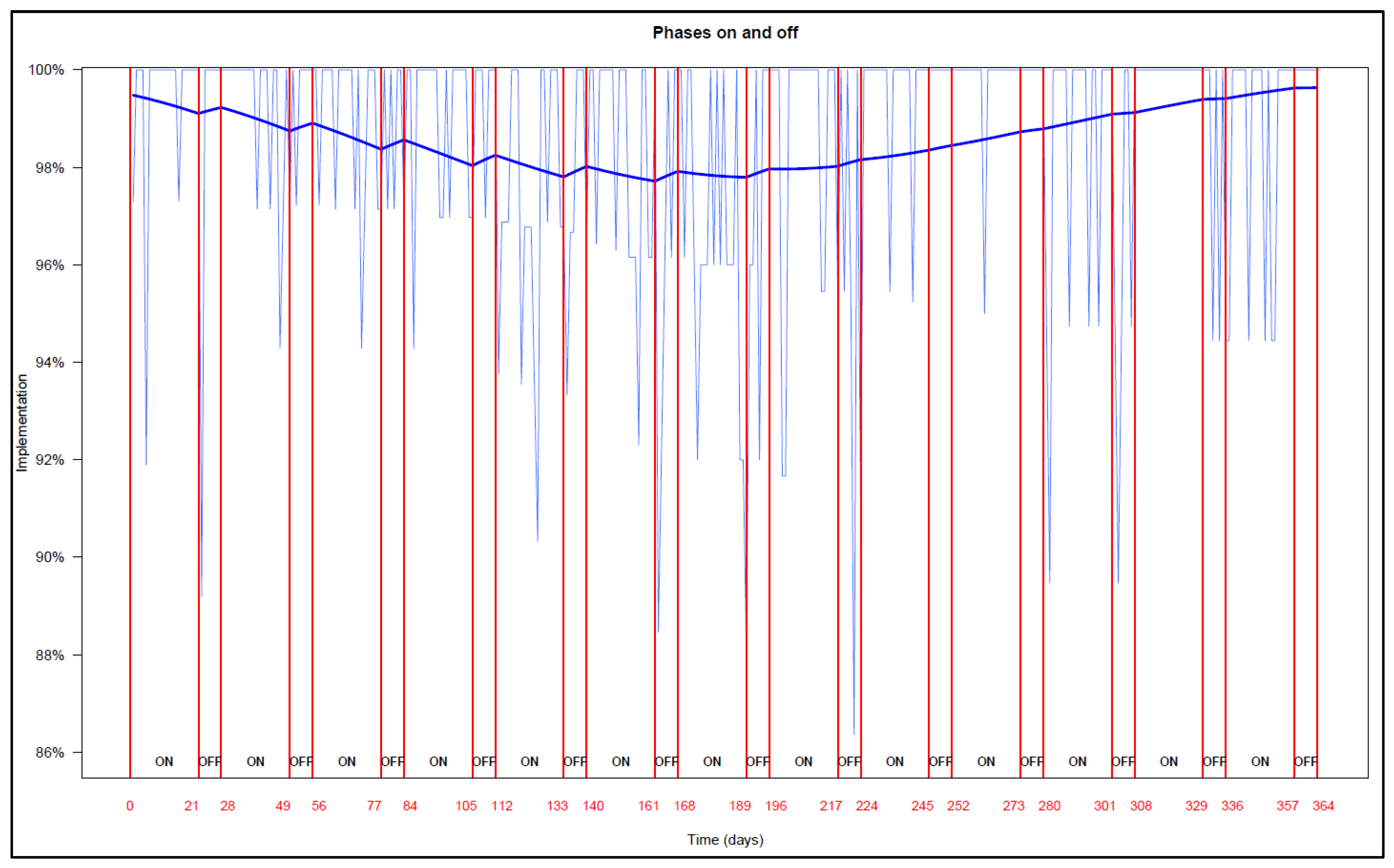
Appendix B. Patients’ Implementation in ON and OFF Phases

Appendix C
| Models | Equations | |||||||
|---|---|---|---|---|---|---|---|---|
| Total sample | logit(imp) = 5.2 | +3.4 × 10−5 | +4.4 × 10−5 | |||||
| Group | logit (imp) = 5.2 | −1.8 × 10−2 | + 4.8 × 10−5 | −3.6 × 10−3 | + 2.2 × 10−5 | |||
| Group + Cycle | logit (imp) = 5.1 | +2.3 × 10−1 (cycle > 4) | −1.5 × 10−2 | −6.6 × 10−3 * (cycle > 4) | +5.2 × 10−5 | −3.3 × 10−3 | −5.6 × 10−3 * (cycle > 4) | +3.4 × 10−5 |
| Group + Age | logit (imp) = 5.9 | −1.2 × 10+00 (age > 65) | −1.9 × 10−2 | +3.1 × 10−3 * (age > 65) | +4.7 × 10−5 | −8.4 × 10−3 | +3.5 × 10−3 * (age > 65) | +3.1 × 10−5 |
| Group + t.MBC | logit (imp) = 5.2 | +7.2 × 10−2 (t.MBC > 2) | −1.6 × 10−2 | −5.1 × 10−3 * (t.MBC > 2) | 5.2 × 10−5 | −4.8 × 10−3 | +3.8 × 10−3 * (t.MBC > 2) | +2.2 × 10−5 |
| phase | logit (imp) = 5.3 | −3.0 × 10−2 | +9.8 × 10−5 | +2.2 × 10−2 | −1.1 × 10−4 | |||
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ligue-Suisse-Contre-Le-Cancer. Les Chiffres Du Cancer-Période Considérée: Années 2014 à 2018. Available online: https://www.liguecancer.ch/a-propos-du-cancer/les-chiffres-du-cancer/?gclid=Cj0KCQiA3-yQBhD3ARIsAHuHT65_nXdCauLklKDGpKWR6rqAoSaC8NxK5nBnb8VXZfdwjpp3q48Oe5YaAgzbEALw_wcB (accessed on 28 February 2022).
- Caswell-Jin, J.L.; Sun, L.; Munoz, D.; Lu, Y.; Li, Y.; Huang, H.; Hampton, J.M.; Song, J.; Jayasekera, J.; Schechter, C.; et al. Contributions of screening, early-stage treatment, and metastatic treatment to breast cancer mortality reduction by molecular subtype in U.S. women, 2000–2017. J. Clin. Oncol. 2022, 40, 1008. [Google Scholar] [CrossRef]
- Ciruelos, E.M.; Diaz, M.N.; Isla, M.D.; Lopez, R.; Bernabe, R.; Gonzalez, E.; Cirauqui, B.; Coves, J.; Morales, S.; Arcediano, A.; et al. Patient preference for oral chemotherapy in the treatment of metastatic breast and lung cancer. Eur. J. Cancer Care 2019, 28, e13164. [Google Scholar] [CrossRef] [PubMed]
- Foulon, V.; Schöffski, P.; Wolter, P. Patient adherence to oral anticancer drugs: An emerging issue in modern oncology. Acta Clin. Belg. 2011, 66, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Vrijens, B.; De Geest, S.; Hughes, D.A.; Przemyslaw, K.; Demonceau, J.; Ruppar, T.; Dobbels, F.; Fargher, E.; Morrison, V.; Lewek, P.; et al. A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharm. 2012, 73, 691–705. [Google Scholar] [CrossRef]
- Huang, W.C.; Chen, C.Y.; Lin, S.J.; Chang, C.S. Medication adherence to oral anticancer drugs: Systematic review. Expert Rev. Anticancer Ther. 2016, 16, 423–432. [Google Scholar] [CrossRef]
- Lasala, R.; Santoleri, F. Association between adherence to oral therapies in cancer patients and clinical outcome: A systematic review of the literature. Br. J. Clin. Pharm. 2021, 88, 1999–2018. [Google Scholar] [CrossRef]
- Ibrahim, A.R.; Eliasson, L.; Apperley, J.F.; Milojkovic, D.; Bua, M.; Szydlo, R.; Mahon, F.X.; Kozlowski, K.; Paliompeis, C.; Foroni, L.; et al. Poor adherence is the main reason for loss of CCyR and imatinib failure for chronic myeloid leukemia patients on long-term therapy. Blood 2011, 117, 3733–3736. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, E.; Csajka, C.; Schneider, M.P.; Widmer, N. Effect of Adherence on Pharmacokinetic/Pharmacodynamic Relationships of Oral Targeted Anticancer Drugs. Clin. Pharmacokinet. 2018, 57, 1–6. [Google Scholar] [CrossRef]
- Murphy, C.C.; Bartholomew, L.K.; Carpentier, M.Y.; Bluethmann, S.M.; Vernon, S.W. Adherence to adjuvant hormonal therapy among breast cancer survivors in clinical practice: A systematic review. Breast Cancer Res. Treat. 2012, 134, 459–478. [Google Scholar] [CrossRef]
- Hershman, D.L.; Shao, T.; Kushi, L.H.; Buono, D.; Tsai, W.Y.; Fehrenbacher, L.; Kwan, M.; Gomez, S.L.; Neugut, A.I. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res. Treat. 2011, 126, 529–537. [Google Scholar] [CrossRef] [Green Version]
- Turner, N.C.; Slamon, D.J.; Ro, J.; Bondarenko, I.; Im, S.A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Overall Survival with Palbociclib and Fulvestrant in Advanced Breast Cancer. N. Engl. J. Med. 2018, 379, 1926–1936. [Google Scholar] [CrossRef]
- European Medicines Agency. Ibrance—Assessment Report; European Medicines Agency: Amsterdam, The Netherlands, 2016.
- Finn, R.S.; Crown, J.P.; Lang, I.; Boer, K.; Bondarenko, I.M.; Kulyk, S.O.; Ettl, J.; Patel, R.; Pinter, T.; Schmidt, M.; et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): A randomised phase 2 study. Lancet Oncol. 2015, 16, 25–35. [Google Scholar] [CrossRef]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.E.; Im, S.-A.; Gelmon, K.A.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.L.; et al. PALOMA-2: Primary results from a phase III trial of palbociclib (P) with letrozole (L) compared with letrozole alone in postmenopausal women with ER+/HER2− advanced breast cancer (ABC). J. Clin. Oncol. 2016, 34, 507. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Im, S.-A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016, 17, 425–439. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.S.; Im, S.A.; Colleoni, M.; Franke, F.; Bardia, A.; Cardoso, F.; Harbeck, N.; Hurvitz, S.; Chow, L.; Sohn, J.; et al. Updated Overall Survival of Ribociclib plus Endocrine Therapy versus Endocrine Therapy Alone in Pre- and Perimenopausal Patients with HR+/HER2− Advanced Breast Cancer in MONALEESA-7: A Phase III Randomized Clinical Trial. Clin. Cancer Res. 2022, 28, 851–859. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.S.; Sonke, G.S.; Paluch-Shimon, S.; Campone, M.; Petrakova, K.; Blackwell, K.L.; Winer, E.P.; et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann. Oncol. 2018, 29, 1541–1547. [Google Scholar] [CrossRef]
- Slamon, D.J.; Neven, P.; Chia, S.; Fasching, P.A.; De Laurentiis, M.; Im, S.A.; Petrakova, K.; Bianchi, G.V.; Esteva, F.J.; Martin, M.; et al. Phase III Randomized Study of Ribociclib and Fulvestrant in Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer: MONALEESA-3. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 2465–2472. [Google Scholar] [CrossRef]
- PfizerLabs. Ibrance, Palbociclib Dosing and Administration Guide; PfizerLabs: New York, NY, USA, 2015. [Google Scholar]
- Watson, G.A.; Deac, O.; Aslam, R.; O’Dwyer, R.; Tierney, A.; Sukor, S.; Kennedy, J. Real-World Experience of Palbociclib-Induced Adverse Events and Compliance With Complete Blood Count Monitoring in Women With Hormone Receptor-Positive/HER2-Negative Metastatic Breast Cancer. Clin. Breast Cancer 2019, 19, e186–e194. [Google Scholar] [CrossRef] [Green Version]
- Spring, L.M.; Zangardi, M.L.; Moy, B.; Bardia, A. Clinical Management of Potential Toxicities and Drug Interactions Related to Cyclin-Dependent Kinase 4/6 Inhibitors in Breast Cancer: Practical Considerations and Recommendations. Oncologist 2017, 22, 1039–1048. [Google Scholar] [CrossRef]
- Bandiera, C.; Cardoso, E.; Locatelli, I.; Digklia, A.; Zaman, K.; Diciolla, A.; Cristina, V.; Stravodimou, A.; Veronica, A.L.; Dolcan, A.; et al. Optimizing Oral Targeted Anticancer Therapies Study for Patients With Solid Cancer: Protocol for a Randomized Controlled Medication Adherence Program Along With Systematic Collection and Modeling of Pharmacokinetic and Pharmacodynamic Data. JMIR Res. Protoc. 2021, 10, e30090. [Google Scholar] [CrossRef] [PubMed]
- De Geest, S.; Zullig, L.L.; Dunbar-Jacob, J.; Helmy, R.; Hughes, D.A.; Wilson, I.B.; Vrijens, B. ESPACOMP Medication Adherence Reporting Guideline (EMERGE). Ann. Intern. Med. 2018, 169, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Group, C. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.D.; Fisher, W.A.; Amico, K.R.; Harman, J.J. An information-motivation-behavioral skills model of adherence to antiretroviral therapy. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2006, 25, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Lelubre, M.; Kamal, S.; Genre, N.; Celio, J.; Gorgerat, S.; Hugentobler Hampai, D.; Bourdin, A.; Berger, J.; Bugnon, O.; Schneider, M. Interdisciplinary Medication Adherence Program: The Example of a University Community Pharmacy in Switzerland. BioMed Res. Int. 2015, 2015, 103546. [Google Scholar] [CrossRef] [PubMed]
- Lelubre, M.; Clerc, O.; Grosjean, M.; Amighi, K.; De Vriese, C.; Bugnon, O.; Schneider, M.P. Implementation of an interprofessional medication adherence program for HIV patients: Description of the process using the framework for the implementation of services in pharmacy. BMC Health Serv. Res. 2018, 18, 698. [Google Scholar] [CrossRef]
- Perraudin, C.; Locca, J.-F.; Rossier, C.; Bugnon, O.; Schneider, M.-P. Implementation of an interprofessional medication adherence program for chronic patients in community pharmacies: How much does it cost for the provider? BMC Health Serv. Res. 2019, 19, 15. [Google Scholar] [CrossRef] [Green Version]
- Rotzinger, A.; Cavassini, M.; Bugnon, O.; Schneider, M.P. Development of an algorithm for analysing the electronic measurement of medication adherence in routine HIV care. Int. J. Clin. Pharm. 2016, 38, 1210–1218. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- R-Development-Core-Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; ISBN 3-900051-07-0. [Google Scholar]
- Schneider, M.P.; Achtari Jeanneret, L.; Chevaux, B.; Backes, C.; Wagner, A.D.; Bugnon, O.; Luthi, F.; Locatelli, I. A Novel Approach to Better Characterize Medication Adherence in Oral Anticancer Treatments. Front. Pharmacol. 2019, 9, 1567. [Google Scholar] [CrossRef]
- Courlet, P.; Cardoso, E.; Bandiera, C.; Stravodimou, A.; Zurcher, J.-P.; Chtioui, H.; Locatelli, I.; Decosterd, L.A.; Darnaud, L.; Blanchet, B.; et al. Population Pharmacokinetics of Palbociclib and Its Correlation with Clinical Efficacy and Safety in Patients with Advanced Breast Cancer. Pharmaceutics 2022, 14, 1317. [Google Scholar] [CrossRef]
- Le Marouille, A.; Petit, E.; Kaderbhai, C.; Desmoulins, I.; Hennequin, A.; Mayeur, D.; Fumet, J.D.; Ladoire, S.; Tharin, Z.; Ayati, S.; et al. Pharmacokinetic/Pharmacodynamic Model of Neutropenia in Real-Life Palbociclib-Treated Patients. Pharmaceutics 2021, 13, 1708. [Google Scholar] [CrossRef]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef] [Green Version]
- Gater, A.; Heron, L.; Abetz-Webb, L.; Coombs, J.; Simmons, J.; Guilhot, F.; Rea, D. Adherence to oral tyrosine kinase inhibitor therapies in chronic myeloid leukemia. Leuk. Res. 2012, 36, 817–825. [Google Scholar] [CrossRef]
- Skrabal Ross, X.; Gunn, K.M.; Suppiah, V.; Patterson, P.; Olver, I. A review of factors influencing non-adherence to oral antineoplastic drugs. Support. Care Cancer 2020, 28, 4043–4050. [Google Scholar] [CrossRef]
- Heckman, B.W.; Mathew, A.R.; Carpenter, M.J. Treatment Burden and Treatment Fatigue as Barriers to Health. Curr. Opin. Psychol. 2015, 5, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, J.J.; Gable, J.C.; Zincavage, R.; Price, G.L.; Churchill, C.; Zhu, E.; Stenger, K.; Singhal, M.; Nepal, B.; Grabner, M.; et al. Treatment Experiences with CDK4&6 Inhibitors Among Women with Metastatic Breast Cancer: A Qualitative Study. Patient Prefer. Adherence 2021, 15, 2417–2429. [Google Scholar] [CrossRef]
- Conley, C.C.; McIntyre, M.; Pensak, N.A.; Lynce, F.; Graham, D.; Ismail-Khan, R.; Lopez, K.; Vadaparampil, S.T.; O’Neill, S.C. Barriers and facilitators to taking CDK4/6 inhibitors among patients with metastatic breast cancer: A qualitative study. Breast Cancer Res. Treat. 2022, 192, 385–399. [Google Scholar] [CrossRef]
- Conn, V.S.; Ruppar, T.M. Medication adherence outcomes of 771 intervention trials: Systematic review and meta-analysis. Prev. Med. 2017, 99, 269–276. [Google Scholar] [CrossRef]
- Williams, A.B.; Amico, K.R.; Bova, C.; Womack, J.A. A Proposal for Quality Standards for Measuring Medication Adherence in Research. AIDS Behav. 2013, 17, 284–297. [Google Scholar] [CrossRef]
- McGrady, M.E.; Ramsey, R.R. Using Electronic Monitoring Devices to Assess Medication Adherence: A Research Methods Framework. J. Gen. Intern. Med. 2020, 35, 2707–2714. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, A.E.; Van Wijngaerden, E.; Denhaerynck, K.; De Geest, S.; Vandamme, A.M. Use of electronic monitoring induces a 40-day intervention effect in HIV patients. J. Acquir. Immune Defic. Syndr. 2006, 43, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Van Heuckelum, M.; van den Ende, C.H.M.; Houterman, A.E.J.; Heemskerk, C.P.M.; van Dulmen, S.; van den Bemt, B.J.F. The effect of electronic monitoring feedback on medication adherence and clinical outcomes: A systematic review. PLoS ONE 2017, 12, e0185453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarney, R.; Warner, J.; Iliffe, S.; van Haselen, R.; Griffin, M.; Fisher, P. The Hawthorne Effect: A randomised, controlled trial. BMC Med. Res. Methodol. 2007, 7, 30. [Google Scholar] [CrossRef] [Green Version]
- Cook, P.; Schmiege, S.; McClean, M.; Aagaard, L.; Kahook, M. Practical and analytic issues in the electronic assessment of adherence. West. J. Nurs. Res. 2012, 34, 598–620. [Google Scholar] [CrossRef]
- Anghel, L.A.; Farcas, A.M.; Oprean, R.N. An overview of the common methods used to measure treatment adherence. Med. Pharm. Rep. 2019, 92, 117–122. [Google Scholar] [CrossRef]
- European Medicine Agency. Ibrance: EPAR—Product Information—Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/ibrance-epar-product-information_en.pdf (accessed on 23 December 2022).
- Krummenacher, I.; Cavassini, M.; Bugnon, O.; Schneider, M.P. An interdisciplinary HIV-adherence program combining motivational interviewing and electronic antiretroviral drug monitoring. AIDS Care 2011, 23, 550–561. [Google Scholar] [CrossRef]




| Intervention (n = 19) | Control (n = 17) + Not Randomized c (n = 2) | |
|---|---|---|
| Demographic Data | ||
| Age (years), median (IQR) | 62 (52–73) | 64 (55–75) |
| Marital civil status a, n (%) | 10 (52.6) | 11 (57.9) |
| Caucasian ethnicity b, n (%) | 19 (100) | 17 (89.5) |
| Clinical data | ||
| Time since primary BC diagnosis (years), median (IQR) | 7.5 (4.5–16.9) | 7.3 (3.1–12.8) |
| Time since MBC diagnosis (years), median (IQR) | 1.8 (0.8–3.0) | 1.6 (0.5–3.4) |
| Cancer stage IV, n (%) | 19 (100) | 19 (100) |
| Visceral metastases, n (%) | 16 (84.2) | 10 (52.6) |
| Palbociclib line of treatment for MBC, n (%) | 1st line: 6 (31.6) 2nd line: 3 (15.8) >= 3rd line: 10 (52.6) | 1st line: 5 (26.3) 2nd line: 6 (31.6) >= 3rd line: 8 (42.1) |
| Previous treatment for MBC (if palbociclib is ≥ 2nd treatment for MBC), n (%) | Endocrine therapy: 11 (84.6) Chemotherapy: 2 (15.4) | Endocrine therapy: 7 (50) Chemotherapy: 7 (50) |
| Combined anticancer therapy in addition to palbociclib at inclusion, n (%) | Aromatase inhibitor: 7 (36.8) Fulvestrant: 11 (57.9) Goserelin, leuprorelin: 2 (10.5) | Aromatase inhibitor: 6 (31.6) Fulvestrant: 13 (68.4) Goserelin, leuprorelin: 2 (10.5) |
| Number of palbociclib cycles received before inclusion, n (%) | 0–4 cycle(s): 11 (57.9) >4 cycles: 8 (42.1) | 0–4 cycle(s): 10 (52.6) >4 cycles: 9 (47.4) |
| Time since palbociclib initiation (days), median (IQR) | 97 (14–230) | 83 (28–228) |
| Previous oncologic therapies since BC diagnosis, n (%) | Tumor surgery: 19 (100) Aromatase inhibitor: 17 (89.5) IV chemotherapy: 14 (73.7) Radiotherapy: 11 (57.9) Fulvestrant: 4 (21.0) Goserelin, leuprorelin: 4 (21.0) Trastuzumab: 0 (0) Bevacizumab: 4 (21.0) Everolimus: 3 (15.8) Capecitabine: 2 (10.5) | Tumor surgery: 19 (100) Aromatase inhibitor: 17 (89.5) IV chemotherapy: 12 (63.2) Radiotherapy: 15 (79.0) Fulvestrant: 3 (15.8) Goserelin, leuprorelin: 1 (5.3) Trastuzumab: 1 (5.3) Bevacizumab: 5 (26.3) Everolimus: 2 (10.5) Capecitabine: 3 (15.8) |
| Number of oral prescribed chronic nononcologic treatments at inclusion time, median (IQR) | 3 (1–4) | 3 (1–3) |
| Adherence study | ||
| Time spent in the adherence study (days), median (IQR) | 209 (133–363) | 366 (171–392) |
| Intervention Group (npatients = 19; ncycles = 155) | Control Group (npatients = 18; ncycles = 184) | p-Value | |
|---|---|---|---|
| Patients’ Behaviour When a Dose is Missed | |||
| Patients who missed at least one dose, n (%) | 10/19 (53) | 15/18 (83) | 0.046 |
| Number of cycles impacted by a missed dose (%) | 18/155 (12) | 44/184 (24) | 0.004 |
| Number of ON cycles extended because a missed dose was caught up, n (%) | 11/18 (61) | 15/44 (34) | 0.050 |
| Number of cycles—among those with a caught up dose-in which the OFF phase was shortened from 7 to 6 days, n (%) | 2/11 (18) | 5/15 (33) | 0.658 |
| Number of patients—among those who missed at least one dose-who caught up at least one missed dose, n (%) | 7/10 (70) | 10/15 (67) | 1.000 |
| Number of patients—among those who missed at least one dose-who caught up a missed dose in some cycles and did not caught up in the other cycles, n (%) | 3/10 (30) | 7/15 (47) | 0.679 |
| Transient interruptions of palbociblib during the phase ON | |||
| Number of patients who experienced at least one transient interruption of palbociclib during the ON phase, n (%) | 6/19 (32) | 3/18 (17) | 0.447 |
| Number of cycles impacted by an interruption in phase ON, n (%) | 10/155 (6) | 4/184 (2) | 0.049 |
| Number of cycles—among those which were interrupted-that were resumed after the interruption, n (%) | 4/10 (40) | 2/4 (50) | 1.000 |
| Number of phases ON—among those with an interruption-interrupted because of infection, n (%) | 5/10 (50) | 2/4 (50) | 1.000 |
| Number of phases ON—among those with an interruption-interrupted because of surgery, n (%) | 2/10 (20) | 1/4 (25) | 1.000 |
| Number of phases ON—among those with an interruption-interrupted because of side effects, n (%) | 1/10 (10) | 1/4 (25) | 0.506 |
| Number of phases ON—among those with an interruption-interrupted because of synchronization with the fulvestrant cycle or with previous palbociclib cycles, n (%) | 2/10 (20) | 0/4 (0) | 1.000 |
| Cycle start deferrals | |||
| Number of patients who experienced at least one cycle deferral, n (%) | 13/19 (68) | 15/18 (83) | 0.447 |
| Number of cycles impacted by a deferral, n (%) | 40/155 (26) | 36/184 (20) | 0.170 |
| Number of patients who experienced a cycle deferral due to neutropenia, n (%) | 9/19 (47) | 7/18 (39) | 0.603 |
| Number of cycles deferred because of neutropenia, n (%) | 20/155 (13) | 11/184 (6) | 0.028 |
| Number of patients who experienced a cycle deferral due to radiotherapy sessions, n (%) | 2/19 (11) | 0/18 (0) | 0.487 |
| Number of patients who experienced a cycle deferral due to infection, n (%) | 3/19 (16) | 3/18 (17) | 1.000 |
| Number of patients who experienced a cycle deferral due to prevent the risk of SARS-COV-2 infection during the COVID-19 pandemic, n (%) | 0/19 (0) | 1/18 (6) | 0.487 |
| Number of patients who experienced a cycle deferral due to a medical appointment set too late (oncologist not available or PET-scan results pending), n (%) | 5/19 (26) | 7/18 (39) | 0.414 |
| Number of patients who experienced a cycle deferral due to insurance reimbursement decision pending, n (%) | 0/19 (0) | 1/18 (6) | 0.487 |
| Number of patients who experienced a cycle deferral due to the delayed order of the treatment at the external pharmacy, n (%) | 1/19 (5) | 0/18 (0) | 1.000 |
| Number of patients who asked their oncologist to defer the start of at least one cycle for personal reasons (e.g., holidays), n (%) | 4/19 (21) | 4/18 (22) | 1.000 |
| Dose reduction | |||
| Patients who experienced a dose reduction due to neutropenia a, n (%) | 3/19 (16) | 2/18 (11) | 1.000 |
| Discrepancies of cycle dates notification in the electronic medical record or in the prescription sheet compared to the actual cycles dates | |||
| Number of patients impacted by at least one discrepancy in the cycle dates compared to the actual cycle dates, n (%) | 10/19 (53) | 11/18 (61) | 0.603 |
| Number of patients—among those impacted by a discrepancy-for which the prescription was not modified by pharmacists (i.e., the phase OFF was shortened or extended) b, n (%) | 4/10 (40) | 5/11 (45) | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bandiera, C.; Locatelli, I.; Courlet, P.; Cardoso, E.; Zaman, K.; Stravodimou, A.; Dolcan, A.; Sarivalasis, A.; Zurcher, J.-P.; Aedo-Lopez, V.; et al. Adherence to the CDK 4/6 Inhibitor Palbociclib and Omission of Dose Management Supported by Pharmacometric Modelling as Part of the OpTAT Study. Cancers 2023, 15, 316. https://doi.org/10.3390/cancers15010316
Bandiera C, Locatelli I, Courlet P, Cardoso E, Zaman K, Stravodimou A, Dolcan A, Sarivalasis A, Zurcher J-P, Aedo-Lopez V, et al. Adherence to the CDK 4/6 Inhibitor Palbociclib and Omission of Dose Management Supported by Pharmacometric Modelling as Part of the OpTAT Study. Cancers. 2023; 15(1):316. https://doi.org/10.3390/cancers15010316
Chicago/Turabian StyleBandiera, Carole, Isabella Locatelli, Perrine Courlet, Evelina Cardoso, Khalil Zaman, Athina Stravodimou, Ana Dolcan, Apostolos Sarivalasis, Jean-Philippe Zurcher, Veronica Aedo-Lopez, and et al. 2023. "Adherence to the CDK 4/6 Inhibitor Palbociclib and Omission of Dose Management Supported by Pharmacometric Modelling as Part of the OpTAT Study" Cancers 15, no. 1: 316. https://doi.org/10.3390/cancers15010316