
A “Seed-and-Soil” Radiomics Model Predicts Brain Metastasis Development in Lung Cancer: Implications for Risk-Stratified Prophylactic Cranial Irradiation
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patient Selection
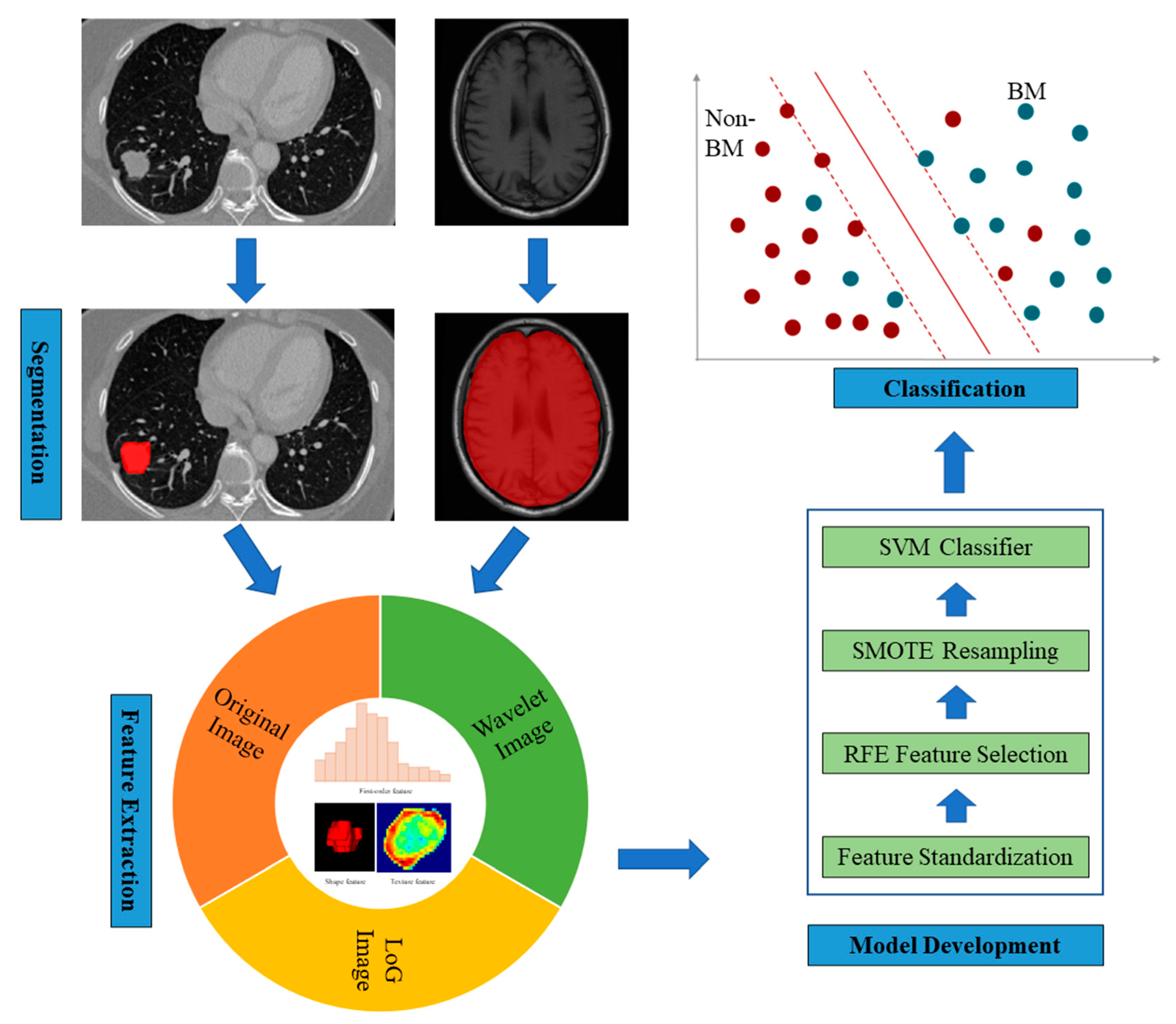
2.2. Radiomics Model Development
2.3. Documentation of the NSCLC Brain Metastasis Lesions
2.4. Statistics
3. Results
NSCLC Brain Lesion Distribution and Implication for Hippocampal Avoidance PCI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Auperin, A.; Arriagada, R.; Pignon, J.; Le Pechoux, C.; Gregor, A.; Stephens, R.; Kristjansen, P.; Johnson, B.; Ueoka, H.; Wagner, H.; et al. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. Prophylactic Cranial Irradiation Overview Collaborative Group. N. Engl. J. Med. 1999, 341, 476–484. [Google Scholar] [CrossRef]
- Slotman, B.; Faivre-Finn, C.; Kramer, G.; Rankin, E.; Snee, M.; Hatton, M.; Postmus, P.; Collette, L.; Musat, E.; Senan, S.; et al. Prophylactic cranial irradiation in extensive small-cell lung cancer. N. Engl. J. Med. 2007, 357, 664–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, A.; Bae, K.; Gore, E.M.; Movsas, B.; Wong, S.J.; Meyers, C.A.; Bonner, J.A.; Schild, S.E.; Gaspar, L.E.; Bogart, J.A.; et al. Phase III trial of prophylactic cranial irradiation compared with observation in patients with locally advanced non-small-cell lung cancer: Neurocognitive and quality-of-life analysis. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Gore, E.M.; Bae, K.; Wong, S.J.; Sun, A.; Bonner, J.A.; Schild, S.E.; Gaspar, L.E.; Bogart, J.A.; Werner-Wasik, M.; Choy, H. Phase III comparison of prophylactic cranial irradiation versus observation in patients with locally advanced non-small-cell lung cancer: Primary analysis of radiation therapy oncology group study RTOG 0214. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 272–278. [Google Scholar] [CrossRef]
- Chalubinska-Fendler, J.; Kepka, L. Prophylactic cranial irradiation in non-small cell lung cancer: Evidence and future development. J. Thorac. Dis. 2021, 13, 3279–3288. [Google Scholar] [CrossRef] [PubMed]
- Paget, S. The distribution of secondary growths in cancer of the breast. 1889. Cancer Metastasis Rev. 1989, 8, 98–101. [Google Scholar]
- Nguyen, D.X.; Bos, P.D.; Massague, J. Metastasis: From dissemination to organ-specific colonization. Nat. Rev. Cancer 2009, 9, 274–284. [Google Scholar] [CrossRef]
- Tomaszewski, M.R.; Gillies, R.J. The Biological Meaning of Radiomic Features. Radiology 2021, 299, E256. [Google Scholar] [CrossRef]
- Xu, X.; Huang, L.; Chen, J.; Wen, J.; Liu, D.; Cao, J.; Wang, J.; Fan, M. Application of radiomics signature captured from pretreatment thoracic CT to predict brain metastases in stage III/IV ALK-positive non-small cell lung cancer patients. J. Thorac. Dis. 2019, 11, 4516–4528. [Google Scholar] [CrossRef]
- Sun, F.; Chen, Y.; Chen, X.; Sun, X.; Xing, L. CT-based radiomics for predicting brain metastases as the first failure in patients with curatively resected locally advanced non-small cell lung cancer. Eur. J. Radiol. 2021, 134, 109411. [Google Scholar] [CrossRef]
- Farjam, R.; Tsien, C.I.; Feng, F.Y.; Gomez-Hassan, D.; Hayman, J.A.; Lawrence, T.S.; Cao, Y. Investigation of the diffusion abnormality index as a new imaging biomarker for early assessment of brain tumor response to radiation therapy. Neuro-oncology 2014, 16, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, A.; Birger, M.; Veeraraghavan, H.; Um, H.; Tixier, F.; McKenney, A.S.; Cugliari, M.; Caviasco, A.; Bialczak, A.; Malani, R.; et al. MRI radiomic features are associated with survival in melanoma brain metastases treated with immune checkpoint inhibitors. Neuro-oncology 2019, 21, 1578–1586. [Google Scholar] [CrossRef]
- Zhao, S.; Hou, D.; Zheng, X.; Song, W.; Liu, X.; Wang, S.; Zhou, L.; Tao, X.; Lv, L.; Sun, Q.; et al. MRI radiomic signature predicts intracranial progression-free survival in patients with brain metastases of ALK-positive non-small cell lung cancer. Transl. Lung Cancer Res. 2021, 10, 368–380. [Google Scholar] [CrossRef] [PubMed]
- Mamon, H.J.; Yeap, B.Y.; Janne, P.A.; Reblando, J.; Shrager, S.; Jaklitsch, M.T.; Mentzer, S.; Lukanich, J.M.; Sugarbaker, D.J.; Baldini, E.H.; et al. High risk of brain metastases in surgically staged IIIA non-small-cell lung cancer patients treated with surgery, chemotherapy, and radiation. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 1530–1537. [Google Scholar] [CrossRef] [PubMed]
- Hubbs, J.L.; Boyd, J.A.; Hollis, D.; Chino, J.P.; Saynak, M.; Kelsey, C.R. Factors associated with the development of brain metastases: Analysis of 975 patients with early stage nonsmall cell lung cancer. Cancer 2010, 116, 5038–5046. [Google Scholar] [CrossRef]
- Ji, Z.; Bi, N.; Wang, J.; Hui, Z.; Xiao, Z.; Feng, Q.; Zhou, Z.; Chen, D.; Lv, J.; Liang, J.; et al. Risk factors for brain metastases in locally advanced non-small cell lung cancer with definitive chest radiation. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 330–337. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, B.; Qu, J.; Yu, F.; Zhao, Y.; Li, S.; Zeng, Y.; Yang, X.; Chu, L.; Chu, X.; et al. Survival outcomes and symptomatic central nervous system (CNS) metastasis in EGFR-mutant advanced non-small cell lung cancer without baseline CNS metastasis: Osimertinib vs. first-generation EGFR tyrosine kinase inhibitors. Lung Cancer 2020, 150, 178–185. [Google Scholar] [CrossRef]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Kniep, H.C.; Madesta, F.; Schneider, T.; Hanning, U.; Schonfeld, M.H.; Schon, G.; Fiehler, J.; Gauer, T.; Werner, R.; Gellissen, S. Radiomics of Brain MRI: Utility in Prediction of Metastatic Tumor Type. Radiology 2019, 290, 479–487. [Google Scholar] [CrossRef]
- Gong, J.; Bao, X.; Wang, T.; Liu, J.; Peng, W.; Shi, J.; Wu, F.; Gu, Y. A short-term follow-up CT based radiomics approach to predict response to immunotherapy in advanced non-small-cell lung cancer. Oncoimmunology 2022, 11, 2028962. [Google Scholar] [CrossRef]
- Gondi, V.; Tolakanahalli, R.; Mehta, M.P.; Tewatia, D.; Rowley, H.; Kuo, J.S.; Khuntia, D.; Tome, W.A. Hippocampal-sparing whole-brain radiotherapy: A "how-to" technique using helical tomotherapy and linear accelerator-based intensity-modulated radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1244–1252. [Google Scholar] [CrossRef] [PubMed]
- Albain, K.S.; Rusch, V.W.; Crowley, J.J.; Rice, T.W.; Turrisi, A.T., 3rd; Weick, J.K.; Lonchyna, V.A.; Presant, C.A.; McKenna, R.J.; Gandara, D.R.; et al. Concurrent cisplatin/etoposide plus chest radiotherapy followed by surgery for stages IIIA (N2) and IIIB non-small-cell lung cancer: Mature results of Southwest Oncology Group phase II study 8805. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1995, 13, 1880–1892. [Google Scholar] [CrossRef]
- Andre, F.; Grunenwald, D.; Pujol, J.L.; Girard, P.; Dujon, A.; Brouchet, L.; Brichon, P.Y.; Westeel, V.; Le Chevalier, T. Patterns of relapse of N2 nonsmall-cell lung carcinoma patients treated with preoperative chemotherapy: Should prophylactic cranial irradiation be reconsidered? Cancer 2001, 91, 2394–2400. [Google Scholar] [CrossRef] [PubMed]
- Carolan, H.; Sun, A.Y.; Bezjak, A.; Yi, Q.L.; Payne, D.; Kane, G.; Waldron, J.; Leighl, N.; Feld, R.; Burkes, R.; et al. Does the incidence and outcome of brain metastases in locally advanced non-small cell lung cancer justify prophylactic cranial irradiation or early detection? Lung Cancer 2005, 49, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, L.E.; Chansky, K.; Albain, K.S.; Vallieres, E.; Rusch, V.; Crowley, J.J.; Livingston, R.B.; Gandara, D.R. Time from treatment to subsequent diagnosis of brain metastases in stage III non-small-cell lung cancer: A retrospective review by the Southwest Oncology Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 2955–2961. [Google Scholar] [CrossRef]
- Robnett, T.J.; Machtay, M.; Stevenson, J.P.; Algazy, K.M.; Hahn, S.M. Factors affecting the risk of brain metastases after definitive chemoradiation for locally advanced non-small-cell lung carcinoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2001, 19, 1344–1349. [Google Scholar] [CrossRef]
- Strauss, G.M.; Herndon, J.E.; Sherman, D.D.; Mathisen, D.J.; Carey, R.W.; Choi, N.C.; Rege, V.B.; Modeas, C.; Green, M.R. Neoadjuvant chemotherapy and radiotherapy followed by surgery in stage IIIA non-small-cell carcinoma of the lung: Report of a Cancer and Leukemia Group B phase II study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1992, 10, 1237–1244. [Google Scholar] [CrossRef]
- Fidler, I.J. The pathogenesis of cancer metastasis: The ‘seed and soil’ hypothesis revisited. Nat. Rev. Cancer 2003, 3, 453–458. [Google Scholar] [CrossRef]
- Gao, Y.; Bado, I.; Wang, H.; Zhang, W.; Rosen, J.M.; Zhang, X.H. Metastasis Organotropism: Redefining the Congenial Soil. Dev. Cell 2019, 49, 375–391. [Google Scholar] [CrossRef]
- Gondi, V.; Hermann, B.P.; Mehta, M.P.; Tome, W.A. Hippocampal dosimetry predicts neurocognitive function impairment after fractionated stereotactic radiotherapy for benign or low-grade adult brain tumors. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 348–354. [Google Scholar] [CrossRef] [Green Version]
- Gondi, V.; Paulus, R.; Bruner, D.W.; Meyers, C.A.; Gore, E.M.; Wolfson, A.; Werner-Wasik, M.; Sun, A.Y.; Choy, H.; Movsas, B. Decline in tested and self-reported cognitive functioning after prophylactic cranial irradiation for lung cancer: Pooled secondary analysis of Radiation Therapy Oncology Group randomized trials 0212 and 0214. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Gondi, V.; Pugh, S.L.; Tome, W.A.; Caine, C.; Corn, B.; Kanner, A.; Rowley, H.; Kundapur, V.; DeNittis, A.; Greenspoon, J.N.; et al. Preservation of memory with conformal avoidance of the hippocampal neural stem-cell compartment during whole-brain radiotherapy for brain metastases (RTOG 0933): A phase II multi-institutional trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 3810–3816. [Google Scholar] [CrossRef] [PubMed]
- Gondi, V.; Tome, W.A.; Mehta, M.P. Why avoid the hippocampus? A comprehensive review. Radiother. Oncol. 2010, 97, 370–376. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | BM + Cohort (n = 128) | BM − Cohort (n = 128) | p |
|---|---|---|---|
| Gender | ☐ | ☐ | 0.676 |
| Male | 66 | 56 | |
| Female | 62 | 72 | |
| Smoking status | ☐ | ☐ | 0.52 |
| ever-smokers | 52 | 46 | |
| never-smokers | 76 | 82 | |
| TNM stage | ☐ | ☐ | 0.566 |
| I | 32 | 45 | |
| II | 37 | 29 | |
| III | 7 | 6 | |
| IV | 52 | 48 | |
| Age at diagnosis (years) | 57 (30–72) | 60 (32–76) | <0.001 |
| Follow-up (months) | 17 (1–73) | 52 (36–84) | <0.001 |
| Model | ACC (%) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | OR | |
|---|---|---|---|---|---|---|---|
| MRI radiomics model | Training dataset | 71.3 | 75.5 | 65.2 | 76.2 | 64.3 | 5.8 |
| Testing dataset | 60.5 | 38.5 | 94.1 | 90.9 | 50 | 10 | |
| CT radiomics model | Training dataset | 73.7 | 87.3 | 53.6 | 73.6 | 74 | 7.9 |
| Testing dataset | 67.4 | 50 | 94.1 | 92.9 | 55.2 | 16 | |
| “Seed-Soil” fusion radiomics model | Training dataset | 77.7 | 74.4 | 80.9 | 79.8 | 75.8 | 12.3 |
| Testing dataset | 71.4 | 78.9 | 64.1 | 68.2 | 75.8 | 6.7 | |
| Within HA | Rest of The Brain | ||
|---|---|---|---|
| within 5 mm of HC | 5–15 mm from HC | >15 mm from HC | |
| No. of lesions (565 in 128 patients) | 7 | 23 | 535 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, X.; Gong, J.; Yang, X.; Ni, J.; Gu, Y.; Zhu, Z. A “Seed-and-Soil” Radiomics Model Predicts Brain Metastasis Development in Lung Cancer: Implications for Risk-Stratified Prophylactic Cranial Irradiation. Cancers 2023, 15, 307. https://doi.org/10.3390/cancers15010307
Chu X, Gong J, Yang X, Ni J, Gu Y, Zhu Z. A “Seed-and-Soil” Radiomics Model Predicts Brain Metastasis Development in Lung Cancer: Implications for Risk-Stratified Prophylactic Cranial Irradiation. Cancers. 2023; 15(1):307. https://doi.org/10.3390/cancers15010307
Chicago/Turabian StyleChu, Xiao, Jing Gong, Xi Yang, Jianjiao Ni, Yajia Gu, and Zhengfei Zhu. 2023. "A “Seed-and-Soil” Radiomics Model Predicts Brain Metastasis Development in Lung Cancer: Implications for Risk-Stratified Prophylactic Cranial Irradiation" Cancers 15, no. 1: 307. https://doi.org/10.3390/cancers15010307