
The Impact of Mutation of Myelodysplasia-Related Genes in De Novo Acute Myeloid Leukemia Carrying NPM1 Mutation †
 , , , , , , , ,
, , , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment and Follow-Up
2.3. Multiparameter Flow Cytometric (MFC) Immunophenotyping
2.4. Polymerase Chain Reaction (PCR) and Next-Generation Sequencing (NGS)
2.5. Mutational Profile and Assignment of Molecular Risk Groups
2.6. Statistical Analysis
3. Results
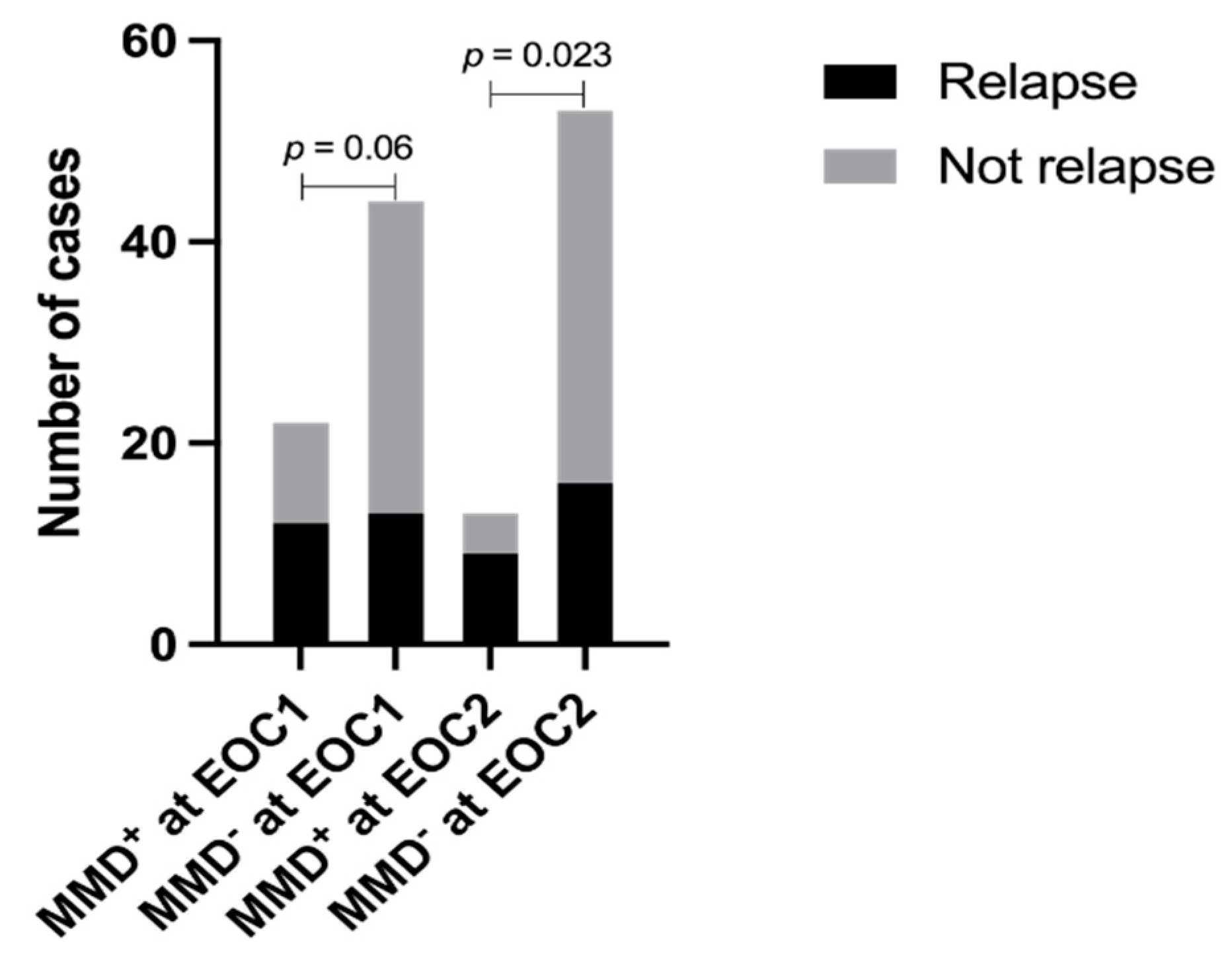
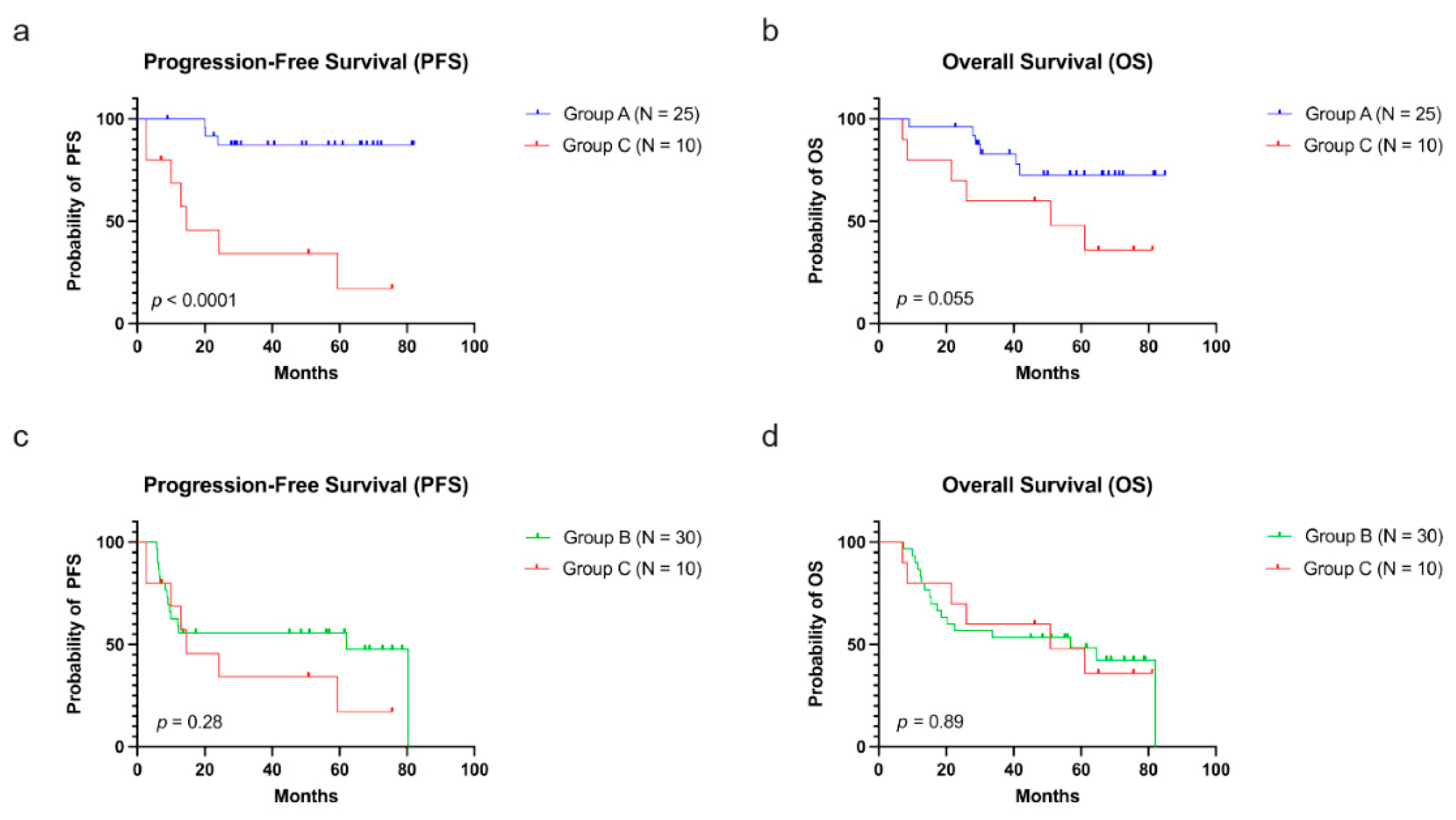
3.1. Correlation between MMD and Relapse and Survival
3.2. Comparison of MFC to Molecular Testing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelemen, K. The Role of Nucleophosmin 1 (NPM1) Mutation in the Diagnosis and Management of Myeloid Neoplasms. Life 2022, 12, 109. [Google Scholar] [CrossRef]
- Oñate, G.; Bataller, A.; Garrido, A.; Hoyos, M.; Arnan, M.; Vives, S.; Coll, R.; Tormo, M.; Sampol, A.; Escoda, L.; et al. Prognostic impact of DNMT3A mutation in acute myeloid leukemia with mutated NPM1. Blood Adv. 2022, 6, 882–890. [Google Scholar] [CrossRef]
- Tazi, Y.; Arango-Ossa, J.E.; Zhou, Y.; Bernard, E.; Thomas, I.; Gilkes, A.; Freeman, S.; Pradat, Y.; Johnson, S.J.; Hills, R.; et al. Unified classification and risk-stratification in Acute Myeloid Leukemia. Nat. Commun. 2022, 13, 4622. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [Green Version]
- Falini, B.; Sciabolacci, S.; Falini, L.; Brunetti, L.; Martelli, M.P. Diagnostic and therapeutic pitfalls in NPM1-mutated AML: Notes from the field. Leukemia 2021, 35, 3113–3126. [Google Scholar] [CrossRef]
- Döhner, H.; Wei, A.H.; Appelbaum, F.R.; Craddock, C.; DiNardo, C.D.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Godley, L.A.; Hasserjian, R.P.; et al. Diagnosis and Management of AML in Adults: 2022 ELN Recommendations from an International Expert Panel. Blood 2022, 140, 1345–1377. [Google Scholar] [CrossRef]
- Falini, B.; Brunetti, L.; Martelli, M.P. How I diagnose and treat NPM1-mutated AML. Blood 2021, 137, 589–599. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.P.; Borowitz, M.J.; Calvo, K.R.; Kvasnicka, H.M.; Wang, S.A.; Bagg, A.; Barbui, T.; Branford, S.; et al. International Consensus Classification of Myeloid Neoplasms and Acute Leukemia: Integrating Morphological, Clinical, and Genomic Data. Blood 2022, 140, 1200–1228. [Google Scholar]
- Lindsley, R.C.; Mar, B.G.; Mazzola, E.; Grauman, P.V.; Shareef, S.; Allen, S.L.; Pigneux, A.; Wetzler, M.; Stuart, R.K.; Erba, H.P.; et al. Acute myeloid leukemia ontogeny is defined by distinct somatic mutations. Blood 2015, 125, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Tashakori, M.; Kadia, T.; Loghavi, S.; Daver, N.; Kanagal-Shamanna, R.; Pierce, S.; Sui, D.; Wei, P.; Khodakarami, F.; Tang, Z.; et al. TP53 copy number and protein expression inform mutation status across risk categories in acute myeloid leukemia. Blood 2022, 140, 58–72. [Google Scholar] [CrossRef]
- Grossmann, V.; Schnittger, S.; Kohlmann, A.; Eder, C.; Roller, A.; Dicker, F.; Schmid, C.; Wendtner, C.M.; Staib, P.; Serve, H.; et al. A novel hierarchical prognostic model of AML solely based on molecular mutations. Blood 2012, 120, 2963–2972. [Google Scholar] [CrossRef] [PubMed]
- Walter, R.B.; Othus, M.; Burnett, A.K.; Löwenberg, B.; Kantarjian, H.M.; Ossenkoppele, G.J.; Hills, R.K.; Ravandi, F.; Pabst, T.; Evans, A.; et al. Resistance prediction in AML: Analysis of 4601 patients from MRC/NCRI, HOVON/SAKK, SWOG and MD Anderson Cancer Center. Leukemia 2015, 29, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Estey, E.H. Acute myeloid leukemia: 2021 update on risk-stratification and management. Am. J. Hematol. 2020, 95, 1368–1398. [Google Scholar] [CrossRef]
- Forghieri, F.; Comoli, P.; Marasca, R.; Potenza, L.; Luppi, M. Minimal/Measurable Residual Disease Monitoring in NPM1-Mutated Acute Myeloid Leukemia: A Clinical Viewpoint and Perspectives. Int. J. Mol. Sci. 2018, 19, 3492. [Google Scholar] [CrossRef] [Green Version]
- Sabattini, E.; Bacci, F.; Sagramoso, C.; Pileri, S.A. WHO classification of tumours of haematopoietic and lymphoid tissues in 2008: An overview. Pathologica 2010, 102, 83–87. [Google Scholar]
- Haferlach, C.; Mecucci, C.; Schnittger, S.; Kohlmann, A.; Mancini, M.; Cuneo, A.; Testoni, N.; Rege-Cambrin, G.; Santucci, A.; Vignetti, M.; et al. AML with mutated NPM1 carrying a normal or aberrant karyotype show overlapping biologic, pathologic, immunophenotypic, and prognostic features. Blood 2009, 114, 3024–3032. [Google Scholar] [CrossRef] [Green Version]
- Walter, R.B.; Othus, M.; Paietta, E.M.; Racevskis, J.; Fernandez, H.F.; Lee, J.W.; Sun, Z.; Tallman, M.S.; Patel, J.; Gönen, M.; et al. Effect of genetic profiling on prediction of therapeutic resistance and survival in adult acute myeloid leukemia. Leukemia 2015, 29, 2104–2107. [Google Scholar] [CrossRef] [Green Version]
- Grimwade, D.; Walker, H.; Oliver, F.; Wheatley, K.; Harrison, C.; Harrison, G.; Rees, J.; Hann, I.; Stevens, R.; Burnett, A.; et al. The importance of diagnostic cytogenetics on outcome in AML: Analysis of 1612 patients entered into the MRC AML 10 trial. Blood 1998, 92, 2322–2333. [Google Scholar]
- Grimwade, D.; Hills, R.K.; Moorman, A.V.; Walker, H.; Chatters, S.; Goldstone, A.H.; Wheatley, K.; Harrison, C.J.; Burnett, A.K. Refinement of cytogenetic classification in acute myeloid leukemia: Determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood 2010, 116, 354–365. [Google Scholar] [CrossRef] [Green Version]
- Jaso, J.M.; Wang, S.A.; Jorgensen, J.L.; Lin, P. Multi-color flow cytometric immunophenotyping for detection of minimal residual disease in AML: Past, present and future. Bone Marrow Transplant. 2014, 49, 1129–1138. [Google Scholar] [CrossRef] [Green Version]
- Loghavi, S.; DiNardo, C.D.; Furudate, K.; Takahashi, K.; Tanaka, T.; Short, N.J.; Kadia, T.; Konopleva, M.; Kanagal-Shamanna, R.; Farnoud, N.R.; et al. Flow cytometric immunophenotypic alterations of persistent clonal haematopoiesis in remission bone marrows of patients with NPM1-mutated acute myeloid leukaemia. Br. J. Haematol 2021, 192, 1054–1063. [Google Scholar] [CrossRef]
- Warren, M.; Luthra, R.; Yin, C.C.; Ravandi, F.; Cortes, J.E.; Kantarjian, H.M.; Medeiros, L.J.; Zuo, Z. Clinical impact of change of FLT3 mutation status in acute myeloid leukemia patients. Mod. Pathol. 2012, 25, 1405–1412. [Google Scholar] [CrossRef] [Green Version]
- Barakat, F.H.; Luthra, R.; Yin, C.C.; Barkoh, B.A.; Hai, S.; Jamil, W.; Bhakta, Y.I.; Chen, S.; Medeiros, L.J.; Zuo, Z. Detection of nucleophosmin 1 mutations by quantitative real-time polymerase chain reaction versus capillary electrophoresis: A comparative study. Arch. Pathol. Lab. Med. 2011, 135, 994–1000. [Google Scholar] [CrossRef]
- Patel, J.P.; Gönen, M.; Figueroa, M.E.; Fernandez, H.; Sun, Z.; Racevskis, J.; Van Vlierberghe, P.; Dolgalev, I.; Thomas, S.; Aminova, O.; et al. Prognostic relevance of integrated genetic profiling in acute myeloid leukemia. N. Engl. J. Med. 2012, 366, 1079–1089. [Google Scholar] [CrossRef] [Green Version]
- Metzeler, K.H.; Maharry, K.; Kohlschmidt, J.; Volinia, S.; Mrózek, K.; Becker, H.; Nicolet, D.; Whitman, S.P.; Mendler, J.H.; Schwind, S.; et al. A stem cell-like gene expression signature associates with inferior outcomes and a distinct microRNA expression profile in adults with primary cytogenetically normal acute myeloid leukemia. Leukemia 2013, 27, 2023–2031. [Google Scholar] [CrossRef] [Green Version]
- Hollink, I.H.; van den Heuvel-Eibrink, M.M.; Zimmermann, M.; Balgobind, B.V.; Arentsen-Peters, S.T.; Alders, M.; Willasch, A.; Kaspers, G.J.; Trka, J.; Baruchel, A.; et al. Clinical relevance of Wilms tumor 1 gene mutations in childhood acute myeloid leukemia. Blood 2009, 113, 5951–5960. [Google Scholar] [CrossRef] [Green Version]
- Owen, C.; Fitzgibbon, J.; Paschka, P. The clinical relevance of Wilms Tumour 1 (WT1) gene mutations in acute leukaemia. Hematol. Oncol. 2010, 28, 13–19. [Google Scholar] [CrossRef]
- Eisfeld, A.K.; Kohlschmidt, J.; Mims, A.; Nicolet, D.; Walker, C.J.; Blachly, J.S.; Carroll, A.J.; Papaioannou, D.; Kolitz, J.E.; Powell, B.E.; et al. Additional gene mutations may refine the 2017 European LeukemiaNet classification in adult patients with de novo acute myeloid leukemia aged <60 years. Leukemia 2020, 34, 3215–3227. [Google Scholar]
- Shallis, R.M.; Pollyea, D.A.; Zeidan, A.M. The complete story of less than complete responses: The evolution and application of acute myeloid leukemia clinical responses. Blood Rev. 2021, 48, 100806. [Google Scholar] [CrossRef]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Büchner, T.; Willman, C.L.; Estey, E.H.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef]
- Carbonell, D.; Suárez-González, J.; Chicano, M.; Andrés-Zayas, C.; Díez-Díez, M.; Rodríguez-Macías, G.; Muñiz, P.; Kwon, M.; Anguita, J.; Díez-Martín, J.L.; et al. Genetic biomarkers identify a subgroup of high-risk patients within low-risk NPM1-mutated acute myeloid leukemia. Leuk. Lymphoma 2021, 62, 1178–1186. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.F.; Pozdnyakova, O.; Hasserjian, R.P.; Aggarwal, N.; Shaver, A.C.; Weinberg, O.K.; Irlmeier, R.; Koyama, T.; Seegmiller, A.C.; Strickland, S.A.; et al. Secondary-type mutations do not impact prognosis in acute myelogenous leukemia AML with mutated NPM1. Am. J. Hematol. 2022, 97, E462–E465. [Google Scholar] [CrossRef]
- Freeman, S.D.; Hills, R.K.; Virgo, P.; Khan, N.; Couzens, S.; Dillon, R.; Gilkes, A.; Upton, L.; Nielsen, O.J.; Cavenagh, J.D.; et al. Measurable Residual Disease at Induction Redefines Partial Response in Acute Myeloid Leukemia and Stratifies Outcomes in Patients at Standard Risk Without NPM1 Mutations. J. Clin. Oncol. 2018, 36, 1486–1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Rau, R.; Goodell, M.A. DNMT3A in haematological malignancies. Nat. Rev. Cancer 2015, 15, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Krönke, J.; Bullinger, L.; Teleanu, V.; Tschürtz, F.; Gaidzik, V.I.; Kühn, M.W.; Rücker, F.G.; Holzmann, K.; Paschka, P.; Kapp-Schwörer, S.; et al. Clonal evolution in relapsed NPM1-mutated acute myeloid leukemia. Blood 2013, 122, 100–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corces-Zimmerman, M.R.; Hong, W.J.; Weissman, I.L.; Medeiros, B.C.; Majeti, R. Preleukemic mutations in human acute myeloid leukemia affect epigenetic regulators and persist in remission. Proc. Natl. Acad. Sci. USA 2014, 111, 2548–2553. [Google Scholar] [CrossRef] [Green Version]
- Cappelli, L.V.; Meggendorfer, M.; Baer, C.; Nadarajah, N.; Hutter, S.; Jeromin, S.; Dicker, F.; Kern, W.; Haferlach, T.; Haferlach, C.; et al. Indeterminate and oncogenic potential: CHIP vs. CHOP mutations in AML with NPM1 alteration. Leukemia 2022, 36, 394–402. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Intensively Treated | Not Intensively Treated | p-Value | |
|---|---|---|---|
| Number | 69 | 38 | N/A |
| Age (years) median and range | 53, (17–69) | 72, (23–87) | <0.0001 |
| Sex: | |||
| -Men -Women | 35 (50.72%) 34 (49.28%) | 18 (47.37%) 20 (52.63%) | 0.84 |
| BM blasts (%) median and range | 64, (1–95) | 59.5, (6–90) | 0.96 |
| WBC (k/µL) median and range | 12.25, (0.1–378.4) | 18.55, (0.9–140) | 0.70 |
| Response: | |||
| -CR/CRi | 56/68 (82.35%) | 33/37 (89.19%) | 0.06 |
| -MLFS | 10/68 (14.71%) | 1/37 (2.70%) | |
| -Refractory | 2/68 (2.94%) | 3/37 (8.11%) | |
| MMD (EOC1) | 22/66 (33.33%) | 26/34 (76.47%) | <0.0001 |
| Relapse | 27 (39.13%) | 20 (52.63%) | 0.22 |
| HSCT | 43 (62.32%) | 3 (7.89%) | <0.0001 |
| Mutation profiles: | |||
| -Group A | 25 (36.23%) | 21 (55.26%) | |
| -Group B | 30 (43.48%) | 15 (39.47%) | |
| -Group C | 10 (14.49%) | 2 (5.26%) | |
| TP53 | 2 | 0 | |
| RUNX1/ASXL1/SRSF2/EZH2 | 2/2/3/1 | 0/2/0/0 | |
| -Group D | 4 (5.80%) | 0 (0.00%) |
| Group A | Group B | Group C | p-Value | |
|---|---|---|---|---|
| Number | 25 | 30 | 10 | N/A |
| Age (years) median and range | 57, (17–69) | 51.5, (19–67) | 59, (33–68) | 0.58 |
| Age > 65 years | 4 (16.00%) | 5 (16.67%) | 3 (30%) | 0.59 |
| Sex: | ||||
| -Men -Women | 13 (52.00%) 12 (48.00%) | 14 (46.67%) 16 (53.33%) | 6 (60.00%) 4 (40.00%) | 0.76 |
| BM blasts (%) median and range | 51.5, (4–94) | 68, (1–95) | 67, (19–86) | 0.48 |
| WBC (k/µL) median and range | 11.2, (0.5–378.4) | 14.9, (1–160.4) | 17.95, (1–44.1) | 0.37 |
| PB blasts (%) median and range | 23.5, (0–97) | 35.5, (0–98) | 16, (0–83) | 0.43 |
| Hb (g/dL) median and range | 8.95, (5.1–12.4) | 9.35, (7.7–15.5) | 9.15, (8.5–14.4) | 0.17 |
| platelets (k/µL) median and range | 53, (11–385) | 57.5, (9–553) | 29.5, (7–87) | 0.18 |
| Response: | ||||
| -CR/CRi | 23/25 (92.00%) | 22/29 (75.86%) | 7/10 (70.00%) | 0.028 |
| -MLFS | 2/25 (8.00%) | 7/29 (24.14%) | 1/10 (10.00%) | |
| -Refractory | 0 (0.00%) | 0 (0.00%) | 2/10 (20.00%) | |
| MMD (EOC1) | 6/25 (24.00%) | 11/29 (37.93%) | 5/8 (62.50%) | 0.13 |
| MMD (EOC2) | 4/25 (16.00%) | 7/29 (24.14%) | 2/8 (25.00%) | 0.68 |
| Relapse | 3 (12.00%) | 15 (50.00%) | 7 (70.00%) | 0.0009 |
| Median OS (months) | NR | 56.90 | 50.80 | 0.045 |
| Median OS (months) (HSCT censored) | NR | NR | NR | 0.14 |
| Median PFS (months) | NR | 62.10 | 14.60 | 0.0006 |
| Median PFS (months) (HSCT censored) | NR | NR | 24.3 | 0.0014 |
| Group A | Group C | p-Value | |
|---|---|---|---|
| Number | 25 | 10 | N/A |
| Age (years) median and range | 57, (17–69) | 59, (33–68) | 0.90 |
| Age > 65 years | 4 (16.00%) | 3 (30%) | 0.38 |
| Sex: | |||
| -Men -Women | 13 (52.00%) 12 (48.00%) | 6 (60.00%) 4 (40.00%) | 0.72 |
| BM blasts (%) median and range | 51.5, (4–94) | 67, (19–86) | 0.87 |
| WBC (k/µL) median and range | 11.2, (0.5–378.4) | 17.95, (1–44.1) | 0.25 |
| PB blasts (%) median and range | 23.5, (0–97) | 16, (0–83) | 0.42 |
| Hb (g/dL) median and range | 8.95, (5.1–12.4) | 9.15, (8.5–14.4) | 0.09 |
| platelets (k/µL) median and range | 53, (11–385) | 29.5, (7–87) | 0.13 |
| Response: | |||
| -CR/CRi | 23/25 (92.00%) | 7/10 (70.00%) | 0.09 |
| -MLFS | 2/25 (8.00%) | 1/10 (10.00%) | |
| -Refractory | 0 (0.00%) | 2/10 (20.00%) | |
| MMD (EOC1) | 6/25 (24.00%) | 5/8 (62.50%) | 0.08 |
| MMD (EOC2) | 4/25 (16.00%) | 2/8 (25.00%) | 0.62 |
| Relapse | 3 (12.00%) | 7 (70.00%) | 0.0016 |
| Median OS (months) | NR | 50.80 | 0.055 |
| Median OS (months) (HSCT censored) | NR | NR | 0.051 |
| Median PFS (months) | NR | 14.60 | <0.0001 |
| Median PFS (months) (HSCT censored) | NR | 24.3 | <0.0001 |
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Overall Survival (OS) | |||
| -WBC count (>100 k/µL) | 3.73 | (1.14, 12.14) | 0.029 |
| -BM blast (%) | 0.98 | (0.97, 1.00) | 0.11 |
| -Age (>65 years) | 0.83 | (0.22, 3.20) | 0.79 |
| -MMD (EOC2) | 1.49 | (0.58, 3.84) | 0.41 |
| -Group (A as reference) | |||
| B | 2.77 | (1.05, 7.32) | 0.040 |
| C | 3.18 | (0.86, 11.80) | 0.08 |
| Progression-Free Survival (PFS) | |||
| -WBC count (>100 k/µL) | 0.93 | (0.23, 3.73) | 0.91 |
| -BM blast (%) | 1.01 | (0.99, 1.03) | 0.31 |
| -Age (>65 years) | 1.78 | (0.51, 6.25) | 0.37 |
| -MMD (EOC2) | 2.34 | (0.88, 6.23) | 0.09 |
| -Group (A as reference) | |||
| B | 5.16 | (1.42, 18.69) | 0.013 |
| C | 7.65 | (1.70, 34.48) | 0.0080 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Quesada, A.E.; Zuo, Z.; Medeiros, L.J.; Yin, C.C.; Li, S.; Xu, J.; Borthakur, G.; Li, Y.; Yang, C.; et al. The Impact of Mutation of Myelodysplasia-Related Genes in De Novo Acute Myeloid Leukemia Carrying NPM1 Mutation. Cancers 2023, 15, 198. https://doi.org/10.3390/cancers15010198
Wang Y, Quesada AE, Zuo Z, Medeiros LJ, Yin CC, Li S, Xu J, Borthakur G, Li Y, Yang C, et al. The Impact of Mutation of Myelodysplasia-Related Genes in De Novo Acute Myeloid Leukemia Carrying NPM1 Mutation. Cancers. 2023; 15(1):198. https://doi.org/10.3390/cancers15010198
Chicago/Turabian StyleWang, Yi, Andres E. Quesada, Zhuang Zuo, L. Jeffrey Medeiros, C. Cameron Yin, Shaoying Li, Jie Xu, Gautam Borthakur, Yisheng Li, Chao Yang, and et al. 2023. "The Impact of Mutation of Myelodysplasia-Related Genes in De Novo Acute Myeloid Leukemia Carrying NPM1 Mutation" Cancers 15, no. 1: 198. https://doi.org/10.3390/cancers15010198