
Tumor Response, Disease Control, and Progression-Free Survival as Surrogate Endpoints in Trials Evaluating Immune Checkpoint Inhibitors in Advanced Non-Small Cell Lung Cancer: Study- and Patient-Level Analyses

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Overview
2.2. Patient-Level Analysis
2.2.1. Data Access
2.2.2. Study Selection
2.2.3. Patient Selection
2.3. Treatment
2.4. Outcomes
Statistics
2.5. Study-Level Analysis
2.5.1. Study Selection
2.5.2. Patient Selection
2.6. Treatment
2.7. Study Search
2.8. Data Extraction
2.9. Outcome
2.10. Assessment of Risk of Bias
2.11. Statistics
3. Results
3.1. Patient-Level Analysis
3.1.1. Patient Characteristics
3.1.2. Patient-Level Surrogacy
3.2. Study-Level Analysis
3.2.1. Study Selection
3.2.2. Study-Level Surrogacy and Traditional Arm Definition
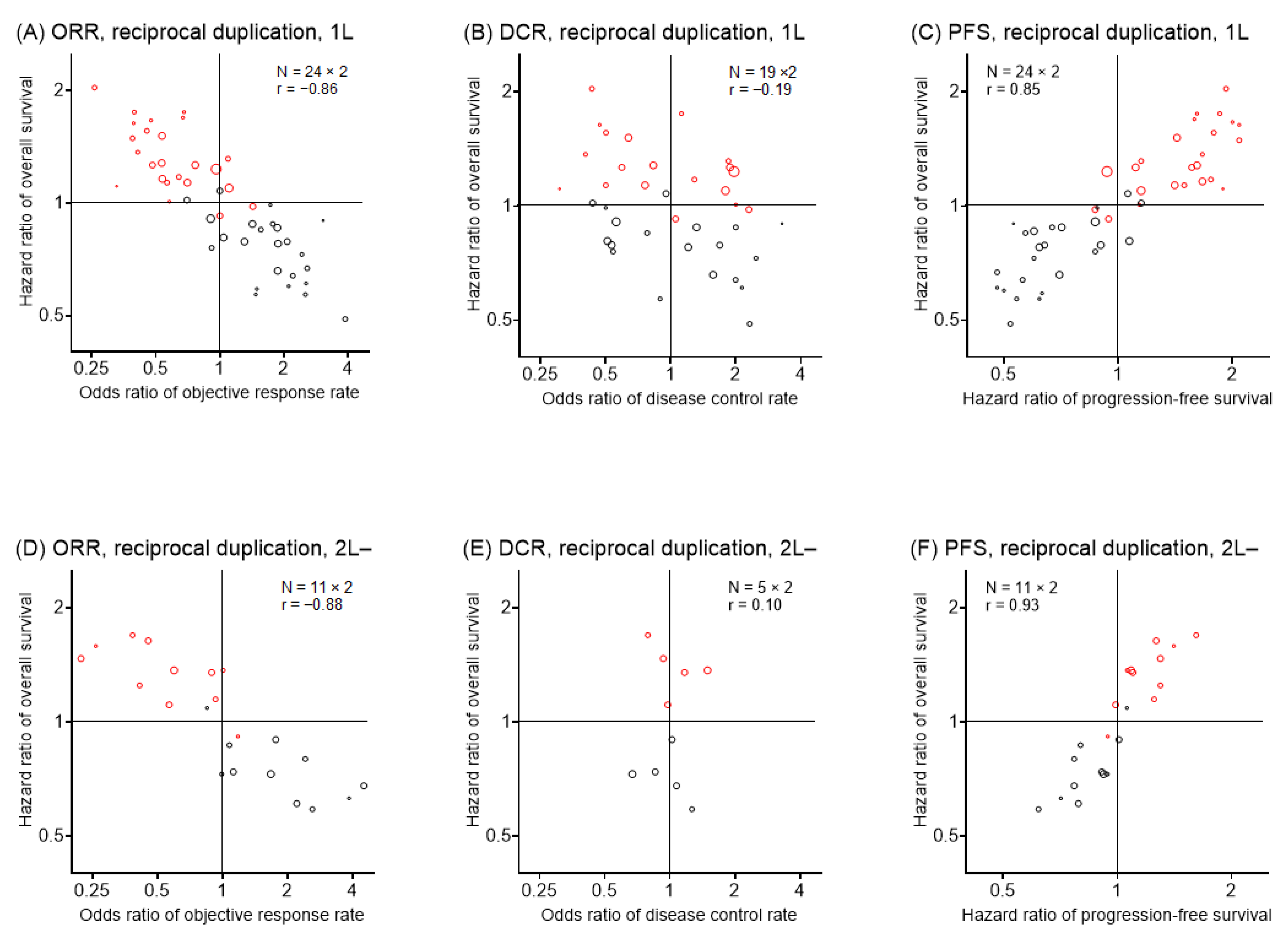
3.2.3. The Rationale of Reciprocal Duplication
3.2.4. Study-Level Surrogacy following Reciprocal Duplication
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.M. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [PubMed] [Green Version]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.; Chirieac, L.R.; D’Amico, T.A.; DeCamp, M.M.; Dilling, T.J.; Dobelbower, M.; et al. Non-Small Cell Lung Cancer, Version 5.2017 Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 504–535. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, 192–237. [Google Scholar] [CrossRef]
- Hanna, N.; Johnson, D.; Temin, S.; Baker, S.; Brahmer, J.; Ellis, P.M.; Giaccone, G.; Hesketh, P.J.; Jaiyesimi, I.; Leighl, N.B.; et al. Systemic Therapy for Stage IV Non-Small-Cell Lung Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 3484. [Google Scholar] [CrossRef]
- Herzberg, B.; Campo, M.J.; Gainor, J.F. Immune Checkpoint Inhibitors in Non-Small Cell Lung Cancer. Oncologist 2017, 22, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Fleming, T.R. Objective response rate as a surrogate end point: A commentary. J. Clin. Oncol. 2005, 23, 4845–4846. [Google Scholar] [CrossRef]
- Nakashima, K.; Horita, N.; Nagai, K.; Manabe, S.; Murakami, S.; Ota, E.; Kaneko, T. Progression-Free Survival, Response Rate, and Disease Control Rate as Predictors of Overall Survival in Phase III Randomized Controlled Trials Evaluating the First-Line Chemotherapy for Advanced, Locally Advanced, and Recurrent Non-Small Cell Lung Carcinoma. J. Thorac. Oncol. 2016, 11, 1574–1585. [Google Scholar]
- Shi, Q.; Sargent, D.J. Meta-analysis for the evaluation of surrogate endpoints in cancer clinical trials. Int. J. Clin. Oncol. 2009, 14, 102–111. [Google Scholar] [CrossRef]
- George, S.L. Response rate as an endpoint in clinical trials. J. Natl. Cancer Inst. 2007, 99, 98–99. [Google Scholar] [CrossRef] [Green Version]
- Ghimire, S.; Kyung, E.; Kim, E. Reporting trends of outcome measures in phase II and phase III trials conducted in advanced-stage non-small-cell lung cancer. Lung 2013, 191, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef]
- Mok, T.; Camidge, D.R.; Gadgeel, S.M.; Rosell, R.; Dziadziuszko, R.; Kim, D.W.; Pérol, M.; Ou, S.I.; Ahn, J.S.; Shaw, A.T.; et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Ann Oncol. 2020, 31, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Amit, O.; Bushnell, W.; Dodd, L.; Roach, N.; Sargent, D. Blinded independent central review of the progression-free survival endpoint. Oncologist 2010, 15, 492–495. [Google Scholar] [CrossRef] [Green Version]
- Broglio, K.R.; Berry, D.A. Detecting an overall survival benefit that is derived from progression-free survival. J. Natl. Cancer Inst. 2009, 101, 1642–1649. [Google Scholar] [CrossRef] [PubMed]
- Saad, E.D.; Katz, A.; Hoff, P.M.; Buyse, M. Progression-free survival as surrogate and as true end point: Insights from the breast and colorectal cancer literature. Ann Oncol. 2010, 21, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, G.M.; Karuri, S.W.; Zhang, H.; Zhang, L.; Khozin, S.; Kazandjian, D.; Tang, S.; Sridhara, R.; Keegan, P.; Pazdur, R. Overall response rate, progression-free survival, and overall survival with targeted and standard therapies in advanced non-small-cell lung cancer: US Food and Drug Administration trial-level and patient-level analyses. J. Clin. Oncol. 2015, 33, 1008–1014. [Google Scholar] [CrossRef] [Green Version]
- Small, E.J.; Schellhammer, P.F.; Higano, C.S.; Redfern, C.H.; Nemunaitis, J.J.; Valone, F.H.; Verjee, S.S.; Jones, L.A.; Hershberg, R.M. Placebo-controlled phase III trial of immunologic therapy with sipuleucel-T (APC8015) in patients with metastatic, asymptomatic hormone refractory prostate cancer. J. Clin. Oncol. 2006, 24, 3089–3094. [Google Scholar] [CrossRef] [Green Version]
- Chiou, V.L.; Burotto, M. Pseudoprogression and Immune-Related Response in Solid Tumors. J. Clin. Oncol. 2015, 33, 3541–3543. [Google Scholar] [CrossRef] [Green Version]
- Equator Network. Enhancing the QUAlity and Transparency Of Health Research. Available online: https://www.equator-network.org/ (accessed on 1 March 2022).
- University Hospital Medical Information Network (UMIN) Center. UMIN Clinical Trials Registry. Available online: https://www.umin.ac.jp/ctr/index-j.htm (accessed on 1 March 2022).
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Higgins, P.J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0). 2011. Available online: http://handbook.cochrane.org/front_page.htm (accessed on 21 February 2022).
- Ripley, B. Package ‘Boot’. 2015. Available online: https://cran.r-project.org/web/packages/boot/boot.pdf#search=‘corr+boot+r’ (accessed on 22 February 2022).
- Bohnsack, O.; Hoos, A.; Ludajic, K. Adaptaion of the immune related response criteria: irRECIST. Ann. Oncol. 2014, 25 (Suppl. 4), 361–372. [Google Scholar] [CrossRef]
- Andreo, P. Monte-Carlo techniques in medical radiation physics. Phys. Med. Biol. 1991, 36, 861–920. [Google Scholar] [CrossRef] [PubMed]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Jotte, R.; Cappuzzo, F.; Vynnychenko, I.; Stroyakovskiy, D.; Rodríguez-Abreu, D.; Hussein, M.; Soo, R.; Conter, H.J.; Kozuki, T.; Huang, K.C.; et al. Atezolizumab in Combination With Carboplatin and Nab-Paclitaxel in Advanced Squamous NSCLC (IMpower131): Results From a Randomized Phase III Trial. J. Thorac. Oncol. 2020, 15, 1351–1360. [Google Scholar] [CrossRef]
- Peters, S.; Gettinger, S.; Johnson, M.L.; Jänne, P.A.; Garassino, M.C.; Christoph, D.; Toh, C.K.; Rizvi, N.A.; Chaft, J.E.; Carcereny Costa, E.; et al. Phase II Trial of Atezolizumab As First-Line or Subsequent Therapy for Patients With Programmed Death-Ligand 1-Selected Advanced Non-Small-Cell Lung Cancer (BIRCH). J. Clin. Oncol. 2017, 35, 2781–2789. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Spigel, D.R.; Chaft, J.E.; Gettinger, S.; Chao, B.H.; Dirix, L.; Schmid, P.; Chow, L.Q.M.; Hicks, R.J.; Leon, L.; Fredrickson, J.; et al. FIR: Efficacy, Safety, and Biomarker Analysis of a Phase II Open-Label Study of Atezolizumab in PD-L1-Selected Patients With NSCLC. J. Thorac. Oncol. 2018, 13, 1733–1742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Branchoux, S.; Bellera, C.; Italiano, A.; Rustand, D.; Gaudin, A.F.; Rondeau, V. Immune-checkpoint inhibitors and candidate surrogate endpoints for overall survival across tumour types: A systematic literature review. Crit. Rev. Oncol. Hematol. 2019, 137, 35–42. [Google Scholar] [CrossRef]
- Ritchie, G.; Gasper, H.; Man, J.; Lord, S.; Marschner, I.; Friedlander, M.; Lee, C.K. Defining the Most Appropriate Primary End Point in Phase 2 Trials of Immune Checkpoint Inhibitors for Advanced Solid Cancers: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Nie, R.C.; Chen, F.P.; Yuan, S.Q.; Luo, Y.S.; Chen, S.; Chen, Y.M.; Chen, X.J.; Chen, Y.B.; Li, Y.F.; Zhou, Z.W. Evaluation of objective response, disease control and progression-free survival as surrogate end-points for overall survival in anti-programmed death-1 and anti-programmed death ligand 1 trials. Eur. J. Cancer 2019, 106, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kok, P.S.; Yoon, W.H.; Lord, S.; Marschner, I.; Friedlander, M.; Lee, C.K. Tumor Response End Points as Surrogates for Overall Survival in Immune Checkpoint Inhibitor Trials: A Systematic Review and Meta-Analysis. JCO Precis. Oncol. 2021, 5, 1151–1159. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Hoos, A.; O’Day, S.; Weber, J.S.; Hamid, O.; Lebbé, C.; Maio, M.; Binder, M.; Bohnsack, O.; Nichol, G.; et al. Guidelines for the evaluation of immune therapy activity in solid tumors: Immune-related response criteria. Clin. Cancer Res. 2009, 15, 7412–7420. [Google Scholar] [CrossRef] [Green Version]
- Rossi, G.; Pezzuto, A.; Sini, C.; Tuzi, A.; Citarella, G.; McCusker, M.G.; Nigro, O.; Tanda, E.; Russo, A. Concomitant medications during immune checkpoint blockage in cancer patients: Novel insights in this emerging clinical scenario. Crit. Rev. Oncol. Hematol. 2019, 142, 26–34. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 1st Line | 2nd or Later Line | |
|---|---|---|
| N | 2003 | 1309 |
| Age (year) | 64 (58–70) | 63 (57–70) |
| Sex | ||
| Men | 1328 (66.3%) | 803 (61.3%) |
| Women | 675 (33.7%) | 506 (38.7%) |
| Race | ||
| Asian | 199 (9.9%) | 199 (15.2%) |
| Black or African American | 36 (1.8%) | 24 (1.8%) |
| White | 1693 (84.5%) | 1027 (78.5%) |
| Other/unknown | 75 (3.7%) | 59 (4.5%) |
| Pathology | ||
| Squamous | 677 (33.8%) | 364 (27.8%) |
| Non-squamous | 1309 (65.4%) | 945 (72.2%) |
| Unknown | 17 (0.8%) | 0 (0.0%) |
| Stage | ||
| IA | 60 (3.0%) | 39 (3.0%) |
| IB | 44 (2.2%) | 56 (4.3%) |
| IIA | 46 (2.3%) | 49 (3.7%) |
| IIB | 48 (2.4%) | 75 (5.7%) |
| IIIA | 134 (6.7%) | 193 (14.7%) |
| IIIB | 96 (4.8%) | 159 (12.1%) |
| IV (not specified for A/B) | 1489 (74.3%) | 55 (4.2%) |
| IVA | 27 (1.3%) | 310 (23.7%) |
| IVB | 24 (1.2%) | 346 (26.4%) |
| Unknown | 35 (1.7%) | 27 (2.1%) |
| TD-L1 (IC) | ||
| 0–0.9 | 917 (45.8%) | 326 (24.9%) |
| 1–4.9 | 645 (32.2%) | 315 (24.1%) |
| 5–9.9 | 212 (10.6%) | 207 (15.8%) |
| 10–49.9 | 191 (9.5%) | 321 (24.5%) |
| 50–100 | 38 (1.9%) | 131 (10.0%) |
| Unknown | 0 (0.0%) | 9 (0.7%) |
| PD-LI (TC) | ||
| 0–0.9 | 1229 (61.4%) | 550 (42.0%) |
| 1–4.9 | 205 (10.2%) | 292 (22.3%) |
| 5–9.9 | 73 (3.6%) | 61 (4.7%) |
| 10–49.9 | 241 (12.0%) | 181 (13.8%) |
| 50–100 | 255 (12.7%) | 218 (16.7%) |
| Unknown | 0 (0.0%) | 7 (0.5%) |
| Smoking history | ||
| Never | 290 (14.5%) | 239 (18.3%) |
| Previous | 1224 (61.1%) | 901 (68.8%) |
| Current | 489 (24.4%) | 169 (12.9%) |
| Country | Phase | Patho | Stage | PD-L1 Status | Driver | PS | Line | Imaging Evaluation | Treatment | ROB H/U/L | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antonia (2017) PACIFIC | USA | III | NSCLC | IIIa, IIIb | Any | ANY | 0–1 | After CCR | RECIST ICR | Dur (10 mg/kg) q2w No active treatment | 0/0/6 |
| Barlesi (2018) JAVELIN Lung 200 | South Korea | III | NSCLC | IIIb, IV, Rec | TC > 1% | EGFR(-), ALK(-) | 0–1 | 2–4 | RECIST ICR | Avel (10 mg/kg) q2w Dtx (75 mg/m2) q3w | 1/0/5 |
| Borghaei (2015) CheckMate057 | USA | III | NSQ | IIIb, IV | Any | Any | 0–1 | 2–3 | RECIST | Niv (3 mg/kg) q2w Dtx (75 mg/m2) q3w | 2/0/4 |
| Boyer (2021) KEYNOTE-598 | Australia | III | NSCLC | IV | TC > 50% | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Pemb (200 mg) q3w + Ipi (1 mg/kg) q6w Pemb (200 mg) q3w | 0/0/6 |
| Brahmer (2015) CheckMate017 | USA | III | SQ | IIIb, IV | Any | Any | 0–1 | 2 | RECIST, | Niv (3 mg/kg) q2w Dtx (75 mg/m2) q3w | 2/0/4 |
| Carbone (2017) CheckMate026 | USA | III | NSCLC | IV, Rec | TC > 5% | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Niv (3 mg/kg) q2w Platinum doublet | 1/0/5 |
| Fehrenbacher (2016) POPLAR | USA | II | NSCLC | Adv, Met | Any | Any | 0–1 | 2–3 | RECIST | Atz (1200 mg) q3w Dtx (75 mg/m2) q3w | 2/0/4 |
| Gandhi (2018) KEYNOTE-189 | USA | III | NSQ | Met | Any | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Pemb (200 mg) + Platinum + Pemt (500 mg/m2) q3w Platinum + Pemt (500 mg/m2) q3w | 1/0/5 |
| Gettinger (2021) Lung-MAP S1400I | USA | III | SQ | IV | Any | Any | 0–1 (Z) | 2- | RECIST | Niv (3 mg/kg) q2w + Ipi (1 mg/kg) q6w Niv (3 mg/kg) q2w | 2/0/4 |
| Govindan (2017) Study 104 | USA | III | SQ | IV, Rec | Any | Any | 0–1 | 1 | mWHO | Ipi (10 mg/kg) + Cbdca (AUC 6) + Ptx (175 mg/m2) q3w Cbdca (AUC 6) + Ptx (175 mg/m2) q3w | 0/0/6 |
| Hellmann (2019) CheckMate227 | USA | III | NSCLC | IV, Rec | TC >1% | EGFR(-), ALK(-) | 0–1 | 1 | RECIST ICR | Niv (3 mg/kg) q2w + Ipi (1 mg/kg) q6w Platinum doublet | 1/0/5 |
| Hensing (2021) Alliance 09 | USA | II | NSCLC | IV | Any | EGFR(-), ALK(-) | 0–1 | no previous ICI | RECIST, ICR | Cbdca doublet q3w x4 followed by Pemb (200 mg) q3w x4 Pemb (200 mg) q3w x4 followed by Cbdca doublet q3w x4 | 1/0/5 |
| Herbst (2016) KEYNOTE-010 | USA | II/III | NSCLC | Adv | TC >1% | Any | 0–1 | 2- | RECIST, ICR | Pemb (10 mg/kg) q3w Dtx (75 mg/m2) q3w | 1/0/5 |
| Herbst (2020) IMpower110 | USA | III | NSCLC | IV | IC>10% or TC>50% | EGFR(-), ALK(-) | 0–1 | 1 | RECIST | Atz (1200 mg) q3w Dtx (75 mg/m2) q3w | 1/0/5 |
| Jotte (2020) IMpower131 | USA | III | SQ | IV | Any | Any | 0–1 | 1 | RECIST | Atz (1200 mg) + Cbdca (AUC 6) + nPtx (100 mg/m2) q3w Cbdca (AUC 6) + nPtx (100 mg/m2) q3w | 1/0/5 |
| Jung (2022) NCT03656094 | South Korea | II | NSCLC | Adv | Any | EGFR(-), ALK(-) | 0–1 | 2–3 | RECIST | Pemb (200 mg) q3w + Single-agent Chemotherpay Single-agent Chemotherpay | 0/0/6 |
| Langer (2016) KEYNOTE-021 | USA | II | NSQ | III, IV | Any | EGFR(-), ALK(-) | 0–1 | 1 | RECIST | Pemb (200 mg) + Cbdca (AUC 5) + Pemt (500 mg/m2) q3w Cbdca (AUC 5) + Pemt (500 mg/m2) q3w | 2/0/4 |
| Leighl (2021) CCTG BR34 | Canada | II | NSCLC | IVa, IVb | Any | EGFR(-), ALK(-) | 0–1 | 1 | RECIST | Durv (1500 mg) + Trem (75 mg) + Platinum doublet q3w Durv (1500 mg) + Trem (75 mg) | 2/0/4 |
| Lynch (2012) NCT00527735 | Netherlands | II | NSCLC | IIIb, IV | Any | EGFR(-), ALK(-) | 0–1 | 1 | mWHO, ICR | Ipi (10 mg/kg) + Cbdca (AUC 6) + Ptx (175 mg/m2) q3w Cbdca (AUC 6) + Ptx (175 mg/m2) q3w | 0/0/6 |
| Mok (2019) KEYNOTE-042 | HK | III | NSCLC | LocAdv, Met | TC>1% | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Pemb (200 mg) q3w Cbdca doublet | 1/0/5 |
| Nishio (2021) IMpower132 | Japan | III | NSQ | IV | Any | Any | 0–1 | 1 | RECIST | Atz (1200 mg) + Platinum + Pemt (500 mg/m2) q3w Platinum + Pemt (500 mg/m2) q3w | 2/0/4 |
| Paz-Ares (2018) KEYNOTE-407 | Spain | III | SQ | IV | TC >50% | Any | 0–1 | 1 | RECIST, ICR | Pemb (200 mg) +Cbdca (AUC 6) + (Ptx (200 mg/m2) or nPtx (100 mg/m2)) q3w Cbdca (AUC 6) + (Ptx (200 mg/m2) or nPtx (100 mg/m2)) q3w | 0/0/6 |
| Paz-Ares (2021) CheckMate9LA | Spain | III | NSCLC | IV, Rec | Any | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Niv (360 mg) q3w + Ipi (1 mg/kg) q6w + Platinum doublet q3w Platinum doublet q3w | 1/0/5 |
| Planchard (2020) ARCTIC-A | France | III | NSCLC | IIIb, IV | TC >25% | EGFR(-), ALK(-) | 0–1 | 3- | RECIST | Durv (10 mg/kg) q2w Gem and Vin or Erl | 2/0/4 |
| Planchard (2020) ARCTIC-B | France | III | NSCLC | IIIb, IV | TC <25% | EGFR(-), ALK(-) | 0–1 | 3- | RECIST | Durv (20 mg/kg) + Trem (1 mg/kg) q4w Gem and Vin or Erl | 2/0/4 |
| Reck (2016) KEYNOTE-024 | USA | III | NSCLC | IV | TC>50% | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Pemb (200 mg) q3w Platinum doublet | 1/0/5 |
| Rittmeyer (2017) OAK | USA | III | NSCLC | IIIb-IV | IC>1% or TC>1% | Any | 0–1 | 2–3 | RECIST | Atz (1200 mg) Dtx (75 mg/m2) q3w | 2/0/4 |
| Rizvi (2020) MYSTIC | USA | III | NSCLC | IV | TC>25% | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Durv (20 mg/kg) q4w Platinum doublet | 1/0/5 |
| Sezer (2021) EMPOWER-Lung 1 | Turkey | III | NSCLC | IIIb, IIIc, IV | TC >50% | EGFR(-), ALK(-), ROS1(-) | 0–1 | 1 | RECIST, ICR | Cemi (350 mg) q3w Platinum doublet | 1/0/5 |
| Socinski (2018) IMpower150 | Germany | III | NSQ | IV, Rec | Any | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Atz (1200 mg) + Bev (15 mg/kg) + Cbdca (AUC 6) + Ptx (200 mg/m2) Bev (15 mg/kg) + Cbdca (AUC 6) + Ptx (200 mg/m2) | 1/0/5 |
| Sugawara (2021) ONO-4538-52/TASUKI-52 | Japan | III | NSQ | IIIb, IV | Any | EGFR(-), ALK(-), ROS1(-) | 0–1 | 1 | RECIST, ICR | Niv (360 mg) + Cbdca (AUC 6) + Ptx (200 mg/m2) + Bev (15 mg/kg) Cbdca (AUC 6) + Ptx (200 mg/m2) + Bev (15 mg/kg) | 0/0/6 |
| West (2019) IMpower130 | Italy | III | NSQ | IV | Any | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Atz (1200 mg) q3w + Cbdca (AUC 6) q3w + nPtx (100 mg/m2) q1w Cbdca (AUC 6) q3w + nPtx (100 mg/m2) q1w | 1/0/5 |
| Wu (2019) CheckMate078 | China | III | NSCLC | IIIb, IV | Any | EGFR(-), ALK(-) | 0–1 | 2 | RECIST | Niv (3 mg/kg) q2w Dtx (75 mg/m2) q3w | 2/0/4 |
| Yang (2020) ORIENT-11 | China | III | NSQ | IIIb, IIIc, IV | Any | EGFR(-), ALK(-) | 0–1 | 1 | RECIST | Sint (200 mg) + Platinum +Pemt (500 mg/m2) q3w Platinum + Pemt (500 mg/m2) q3w | 0/0/6 |
| ZhouC (2021) ORIENT-12 | China | III | SQ | IIIb, IIIc, IV | Any | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Sint (200 mg) + Platinum +Gem (1000 mg/m2, d 1, 8) q3w Platinum +Gem (1000 mg/m2, d 1, 8) q3w | 0/0/6 |
| ZhouC (2022) GEMSTONE-302 | China | III | NSCLC | IV | Any | EGFR(-), ALK(-), ROS1(-), RET(-) | 0–1 | 1 | RECIST, ICR | Suge (1200 mg) + Cbdca doublet q3w Cbdca doublet q3w | 0/0/6 |
| ZhouQ (2022) GEMSTONE-301 | China | III | NSCLC | III | Any | EGFR(-), ALK(-), ROS1(-) | 0–1 | After CCR | RECIST, ICR | Suge (1200 mg) No active treatment | 0/0/6 |
| ZhouC (2021) CameL | China | III | NSQ | IIIb, IV | Any | EGFR(-), ALK(-) | 0–1 | 1 | RECIST, ICR | Camr (200 mg) + Cbdca (AUC 5) + Pemt (500 mg/m2) q3w Cbdca (AUC 5) + Pemt (500 mg/m2) q3w | 1/0/5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horita, N. Tumor Response, Disease Control, and Progression-Free Survival as Surrogate Endpoints in Trials Evaluating Immune Checkpoint Inhibitors in Advanced Non-Small Cell Lung Cancer: Study- and Patient-Level Analyses. Cancers 2023, 15, 185. https://doi.org/10.3390/cancers15010185
Horita N. Tumor Response, Disease Control, and Progression-Free Survival as Surrogate Endpoints in Trials Evaluating Immune Checkpoint Inhibitors in Advanced Non-Small Cell Lung Cancer: Study- and Patient-Level Analyses. Cancers. 2023; 15(1):185. https://doi.org/10.3390/cancers15010185
Chicago/Turabian StyleHorita, Nobuyuki. 2023. "Tumor Response, Disease Control, and Progression-Free Survival as Surrogate Endpoints in Trials Evaluating Immune Checkpoint Inhibitors in Advanced Non-Small Cell Lung Cancer: Study- and Patient-Level Analyses" Cancers 15, no. 1: 185. https://doi.org/10.3390/cancers15010185