
Comparison of the New Neo-Glasgow Prognostic Score Based on the Albumin-Bilirubin Grade with Currently Used Nutritional Indices for Prognostic Prediction following Surgical Resection of Hepatocellular Carcinoma: A Multicenter Retrospective Study in Japan

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Determination of Underlying Liver Disease
2.3. Assessment of Liver Function and Nutritional Status
2.4. Assessment of Tumor-Node-Metastasis Stage of HCC
2.5. Clinicopathologic Variables, HCC Treatment Algorithms, and Surgical Procedures
2.6. Evaluation of Complications following Surgical Resection
2.7. Statistical Analysis
3. Results
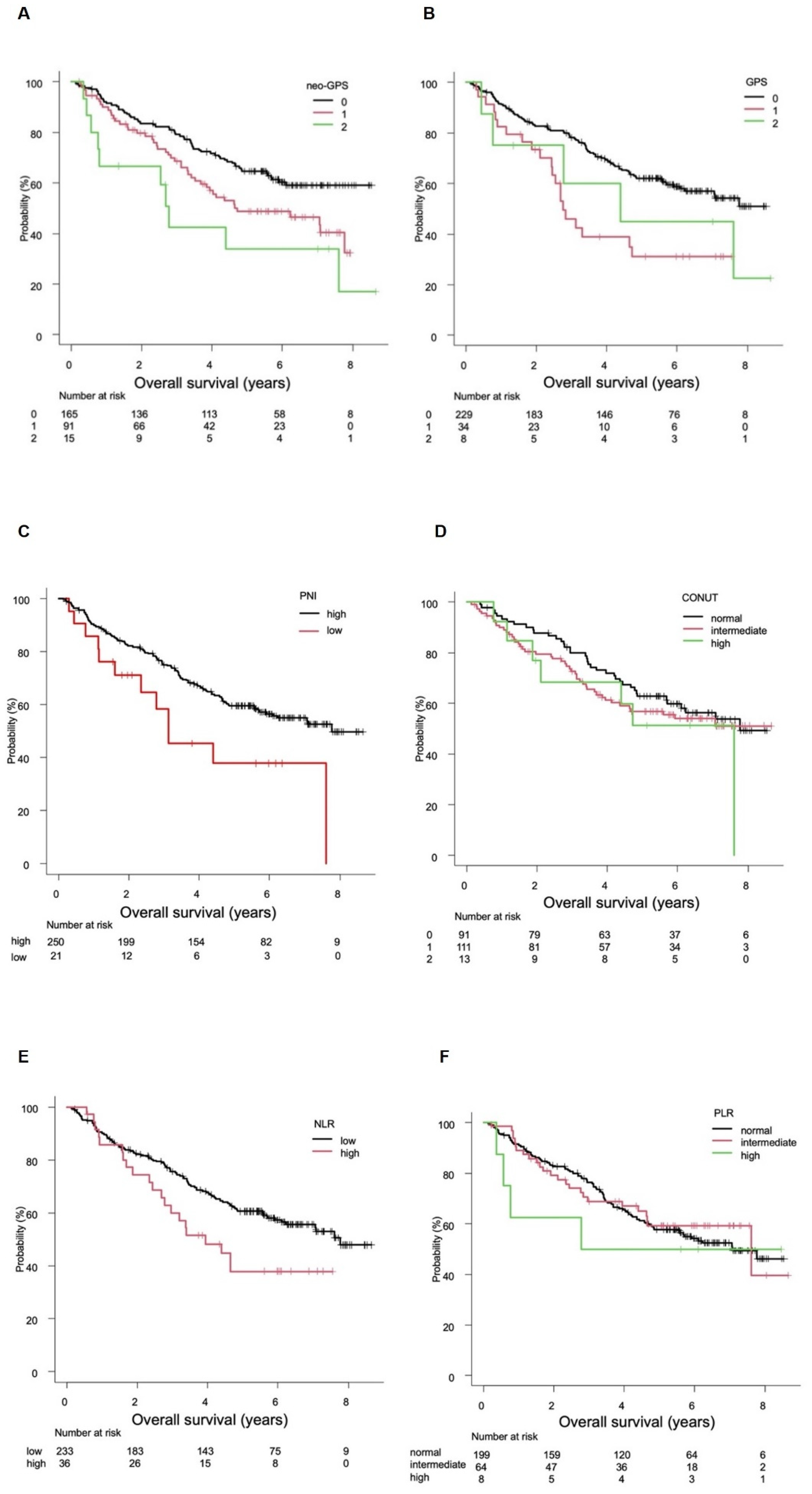
3.1. Evaluation of OS
3.2. Evaluation of PFS
3.3. Rates of High-Grade Clavien-Dindo Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Estimating the world cancer burden: Globocan 2000. Int. J. Cancer 2001, 94, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005, (Abstract in English). [Google Scholar] [PubMed]
- Broggi, M.S.; Patil, D.; Baum, Y.; Nieh, P.T.; Alemozaffar, M.; Pattaras, J.G.; Ogan, K.; Master, V.A. Onodera’s prognostic nutritional index as an independent prognostic factor in clear cell renal cell carcinoma. Urology 2016, 96, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Motomura, T.; Shirabe, K.; Mano, Y.; Muto, J.; Toshima, T.; Umemoto, Y.; Fukuhara, T.; Uchiyama, H.; Ikegami, T.; Yoshizumi, T.; et al. Neutrophil–lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment. J. Hepatol. 2013, 58, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, A.; Onoda, H.; Imai, N.; Iwaku, A.; Oishi, M.; Fushiya, N.; Koike, K.; Nishino, H.; Tajiri, H. Comparison of the prognostic value of inflammation-based prognostic scores in patients with hepatocellular carcinoma. Br. J. Cancer 2012, 107, 988–993. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Evaluation of cumulative prognostic scores based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer. Br. J. Cancer 2003, 89, 1028–1030. [Google Scholar] [CrossRef] [Green Version]
- Elahi, M.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Sattar, N. Score based on hypoalbuminemia and elevated C-reactive protein predicts survival in patients with advanced gastrointestinal cancer. Nutr. Cancer 2004, 48, 171–173. [Google Scholar] [CrossRef]
- Crumley, A.B.; McMillan, D.C.; McKernan, M.; McDonald, A.C.; Stuart, R.C. Evaluation of an inflammation-based prognostic score in patients with inoperable gastro-oesophageal cancer. Br. J. Cancer 2006, 94, 637–641. [Google Scholar] [CrossRef] [Green Version]
- Shimoda, Y.; Fujikawa, H.; Komori, K.; Watanabe, H.; Kano, K.; Yamada, T.; Shiozawa, M.; Morinaga, S.; Katsumata, K.; Tsuchida, A.; et al. Preoperative utility of the Glasgow prognostic score on outcomes of patients with locally advanced gastric cancer. J. Gastrointest. Cancer 2021. [Google Scholar] [CrossRef]
- Kaibori, M.; Hiraoka, A.; Matsui, K.; Matsushima, H.; Kosaka, H.; Yamamoto, H.; Yamaguchi, H.; Yoshida, K.; Sekimoto, M. Predicting complications following surgical resection of hepatocellular carcinoma using newly developed neo-Glasgow prognostic score with ALBI grade: Comparison of open and laparoscopic surgery cases. Cancers 2022, 14, 1402. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kato, M.; Marui, K.; Murakami, T.; Onishi, K.; Adachi, T.; Matsuoka, J.; Ueki, H.; Yoshino, T.; Tsuruta, M.; et al. Easy clinical predictor for low BCAA to tyrosine ratio in chronic liver disease patients with hepatocellular carcinoma: Usefulness of ALBI score as nutritional prognostic marker. Cancer Med. 2021, 10, 3584–3592. [Google Scholar] [CrossRef] [PubMed]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg 1973, 60, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, F.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Toyoda, H.; Tada, T.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; Kawakami, T.; et al. Usefulness of albumin-bilirubin grade for evaluation of prognosis of 2584 Japanese patients with hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2016, 31, 1031–1036. [Google Scholar] [CrossRef]
- The Liver Cancer Study Group of Japan. The General Rules for The Clinical and Pathological Study of Primary Liver Cancer, 6th ed.; Kanehara: Tokyo, Japan, 2015; p. 26. [Google Scholar]
- Kokudo, N.; Takemura, N.; Hasegawa, K.; Takayama, T.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Izumi, N.; Kaneko, S.; et al. Clinical practice guidelines for hepatocellular carcinoma: The Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol. Res. 2019, 49, 1109–1113. [Google Scholar] [CrossRef]
- Strasberg, S.M.; Belghiti, J.; Clavien, P.A.; Gadzijev, E.; Garden, J.O.; Lau, W.Y.; Makuuchi, M.; Strong, R.W. The Brisbane 2000 terminology of liver anatomy and resections. HPB 2000, 2, 333–339. [Google Scholar] [CrossRef]
- Couinaud, C. Le Foie: Études Anatomiques et Chirurgicales; Masson: Paris, France, 1957. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Hiraoka, A.; Michitaka, K.; Kumada, T.; Izumi, N.; Kadoya, M.; Kokudo, N.; Kubo, S.; Matsuyama, Y.; Nakashima, O.; Sakamoto, M.; et al. Validation and potential of albumin-bilirubin grade and prognostication in a nationwide survey of 46,681 hepatocellular carcinoma patients in Japan: The need for a more detailed evaluation of hepatic function. Liver Cancer 2017, 6, 325–336. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Kudo, M.; Hirooka, M.; Tsuji, K.; Itobayashi, E.; Kariyama, K.; Ishikawa, T.; Tajiri, K.; Ochi, H.; et al. Albumin-bilirubin (ALBI) grade as part of the evidence-based clinical practice guideline for HCC of the Japan Society of Hepatology: A comparison with the liver damage and Child-Pugh classifications. Liver Cancer 2017, 6, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Shrotriya, S.; Walsh, D.; Bennani-Baiti, N.; Thomas, S.; Lorton, C. C-reactive protein is an important biomarker for prognosis tumor recurrence and treatment response in adult solid tumors: A systematic review. PLoS ONE 2015, 10, e0143080. [Google Scholar] [CrossRef] [PubMed]
- Yoshiji, H.; Nagoshi, S.; Akahane, T.; Asaoka, Y.; Ueno, Y.; Ogawa, K.; Kawaguchi, T.; Kurosaki, M.; Sakaida, I.; Shimizu, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2020. Hepatol Res. 2021, 51, 725–749. [Google Scholar] [CrossRef] [PubMed]
- Yoshiji, H.; Nagoshi, S.; Akahane, T.; Asaoka, Y.; Ueno, Y.; Ogawa, K.; Kawaguchi, T.; Kurosaki, M.; Sakaida, I.; Shimizu, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2020. J. Gastroenterol. 2021, 56, 593–619. [Google Scholar] [CrossRef]
- Kaido, T.; Ogawa, K.; Fujimoto, Y.; Ogura, Y.; Hata, K.; Ito, T.; Tomiyama, K.; Yagi, S.; Mori, A.; Uemoto, S. Impact of sarcopenia on survival in patients undergoing living donor liver transplantation. Am. J. Transplant. 2013, 13, 1549–1556. [Google Scholar] [CrossRef]
- Chang, K.V.; Chen, J.D.; Wu, W.T.; Huang, K.C.; Hsu, C.T.; Han, D.S. Association between loss of skeletal muscle mass and mortality and tumor recurrence in hepatocellular carcinoma: A systematic review and meta-analysis. Liver Cancer 2018, 7, 90–103. [Google Scholar] [CrossRef]
- Hiraoka, A.; Michitaka, K.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; Kawakami, T.; Yamago, H.; Suga, Y.; Tomida, H.; et al. Sarcopenia and two types of presarcopenia in Japanese patients with chronic liver disease. Eur. J. Gastroenterol. Hepatol. 2016, 28, 940–947. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Characteristics | |
|---|---|
| Age, years * | 72 (64–77) |
| Sex, male:female | 204:67 |
| Body mass index, kg/m2 * | 23.2 (20.7–25.7) |
| Etiology, HCV:HBV:HBV&HCV:others | 109:37:4:121 |
| Positive for diabetes mellitus, n (%) | 87 (32.1) |
| Aspartate transaminase, U/L * | 36 (27–53) |
| Alanine aminotransferase, U/L * | 31 (20–51) |
| Platelet count, 104/µL* | 15.9 (12.0–21.4) |
| Total bilirubin, mg/dL * | 0.7 (0.5–0.9) |
| Albumin, g/dL * | 4.1 (3.8–4.3) |
| Prothrombin time, % * | 92.0 (83.5–100.7) |
| Child-Pugh score, 5:6 | 229:42 |
| CRP, mg/dL * | 0.09 (0.03–0.24) |
| ALBI score * | −2.77 (−2.48 to −3.02) |
| ICG-R15 (%) * | 13.8 (9.5–18.8) |
| AFP, ng/mL * | 12.3 (4.4–169.9) |
| Elevated AFP, ≥100 ng/mL, n (%) | 75 (28.5%) |
| Single tumor, n (%) | 223 (82.3) |
| Maximum tumor size, cm * | 3.6 (2.5–6.0) |
| Resection, open:laparoscopic | 138:133 |
| Microvascular invasion present, n (%) | 297 (69.2) |
| Macro-portal vein invasion, Vp2:Vp3 | 7:5 |
| Macro-hepatic vein invasion, Vv2:Vv3 | 6:0 |
| TNM-LCSGJ, I:II:II:IVa | 31:191:45:4 |
| Operation time, minutes * | 334 (264–410) |
| Blood loss, mL * | 550 (240–1094) |
| Observation period, years * | 5.1 (2.4–6.3) |
| Death, n (%) | 119 (43.9) |
| Neo-GPS, 0:1:2 | 165:91:15 |
| Clavien-Dindo classification ≥3, n (%) | 61 (22.5) |
| (A) OS | HR | Univariate | p Value | HR | Multivariate | p Value |
| 95%CI | 95%CI | |||||
| Age, ≥75 years | 1.217 | 0.828–1.787 | 0.318 | - | - | - |
| Sex, female | 0.683 | 0.428–1.090 | 0.110 | - | - | - |
| Non-viral etiology | 1.098 | 0.738–1.636 | 0.644 | - | - | - |
| Positive for diabetes mellitus | 1.086 | 0.723–1.632 | 0.690 | - | - | - |
| Child-Pugh score, 6 | 0.825 | 0.474–1.436 | 0.496 | - | - | - |
| Elevated AFP, ≥100 ng/mL | 2.333 | 1.579–3.446 | <0.001 | 2.190 | 1.493–3.211 | <0.001 |
| Tumor size, ≥5 cm | 1.825 | 1.271–2.620 | 0.001 | 1.508 | 1.037–2.193 | 0.032 |
| Tumor number, multiple | 1.686 | 1.094–2.600 | <0.001 | 1.784 | 1.178–2.703 | 0.006 |
| Within Milan criteria | 0.709 | 0.478–1.050 | 0.086 | - | - | - |
| Laparoscopic resection | 0.971 | 0.658–1.432 | 0.881 | - | - | - |
| neo-GPS, ≥1 | 1.723 | 1.164–2.549 | 0.007 | 1.554 | 1.074–2.247 | 0.019 |
| (B) PFS | HR | Univariate | p Value | HR | Multivariate | p Value |
| 95%CI | 95%CI | |||||
| Age, ≥75 years | 1.103 | 0.835–1.457 | 0.490 | - | - | - |
| Sex, female | 0.867 | 0.624–1.206 | 0.397 | - | - | - |
| Non-viral etiology | 1.207 | 0.918–1.587 | 0.178 | - | - | - |
| Positive for diabetes mellitus | 1.068 | 0.804–1.419 | 0.650 | - | - | - |
| Child-Pugh score, 6 | 0.961 | 0.780–1.184 | 0.711 | - | - | - |
| Elevated AFP, ≥100 ng/mL | 1.616 | 1.198–2.180 | 0.002 | 1.743 | 1.325–2.292 | <0.001 |
| Tumor size, ≥5 cm | 0.664 | 0.300–1.469 | 0.312 | - | - | - |
| Tumor number, multiple | 1.453 | 1.037–2.035 | 0.030 | 1.537 | 1.148–2.057 | 0.004 |
| Within Milan criteria | 0.456 | 0.208–1.003 | 0.051 | - | - | - |
| Laparoscopic resection | 0.820 | 0.627–1.073 | 0.149 | - | - | - |
| neo-GPS, ≥1 | 1.546 | 1.164–2.054 | 0.003 | 1.522 | 1.186–1.954 | <0.001 |
| Clavien-Dindo Complications | p Value | ||
|---|---|---|---|
| Neo-GPS | 0 | ≥1 | |
| Low-grade CD (<3) | 137 | 73 | |
| High-grade CD (≥3) | 28 | 33 | 0.007 |
| GPS | 0 | ≥1 | |
| Low-grade CD (<3) | 183 | 27 | |
| High-grade CD (≥3) | 46 | 15 | 0.042 |
| PNI | >40 | ≤40 | |
| Low-grade CD (<3) | 197 | 13 | |
| High-grade CD (≥3) | 53 | 8 | 0.100 |
| CONUT score | Normal (≤1) | Elevated (≥2) | |
| Low-grade CD (<3) | 73 | 93 | |
| High-grade CD (≥3) | 18 | 31 | 0.413 |
| NLR | <4.0 | ≥4.0 | |
| Low-grade CD (<3) | 180 | 28 | |
| High-grade CD (≥3) | 53 | 8 | 1.000 |
| PLR | <150 | ≥150 | |
| Low-grade CD (<3) | 156 | 54 | |
| High-grade CD (≥3) | 43 | 18 | 0.622 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaibori, M.; Hiraoka, A.; Iida, H.; Komeda, K.; Hirokawa, F.; Ueno, M.; Kosaka, H.; Matsui, K.; Sekimoto, M. Comparison of the New Neo-Glasgow Prognostic Score Based on the Albumin-Bilirubin Grade with Currently Used Nutritional Indices for Prognostic Prediction following Surgical Resection of Hepatocellular Carcinoma: A Multicenter Retrospective Study in Japan. Cancers 2022, 14, 2091. https://doi.org/10.3390/cancers14092091
Kaibori M, Hiraoka A, Iida H, Komeda K, Hirokawa F, Ueno M, Kosaka H, Matsui K, Sekimoto M. Comparison of the New Neo-Glasgow Prognostic Score Based on the Albumin-Bilirubin Grade with Currently Used Nutritional Indices for Prognostic Prediction following Surgical Resection of Hepatocellular Carcinoma: A Multicenter Retrospective Study in Japan. Cancers. 2022; 14(9):2091. https://doi.org/10.3390/cancers14092091
Chicago/Turabian StyleKaibori, Masaki, Atsushi Hiraoka, Hiroya Iida, Koji Komeda, Fumitoshi Hirokawa, Masaki Ueno, Hisashi Kosaka, Kosuke Matsui, and Mitsugu Sekimoto. 2022. "Comparison of the New Neo-Glasgow Prognostic Score Based on the Albumin-Bilirubin Grade with Currently Used Nutritional Indices for Prognostic Prediction following Surgical Resection of Hepatocellular Carcinoma: A Multicenter Retrospective Study in Japan" Cancers 14, no. 9: 2091. https://doi.org/10.3390/cancers14092091