
Sarcopenia Predicts Major Complications after Resection for Primary Hepatocellular Carcinoma in Compensated Cirrhosis

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
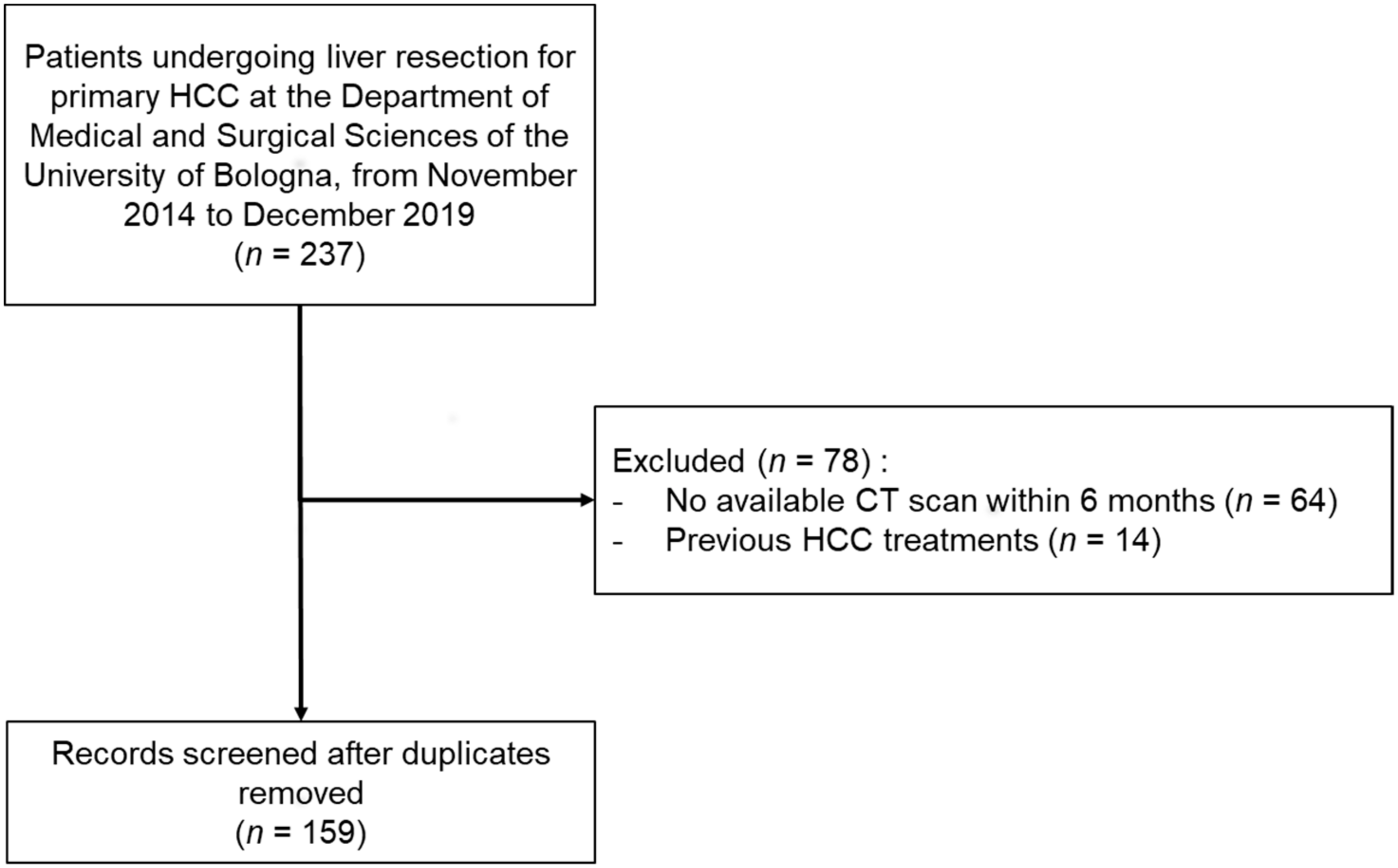
2.1. Patients Selection and Data Collection
2.2. Sarcopenia Assessment
2.3. Definitions
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
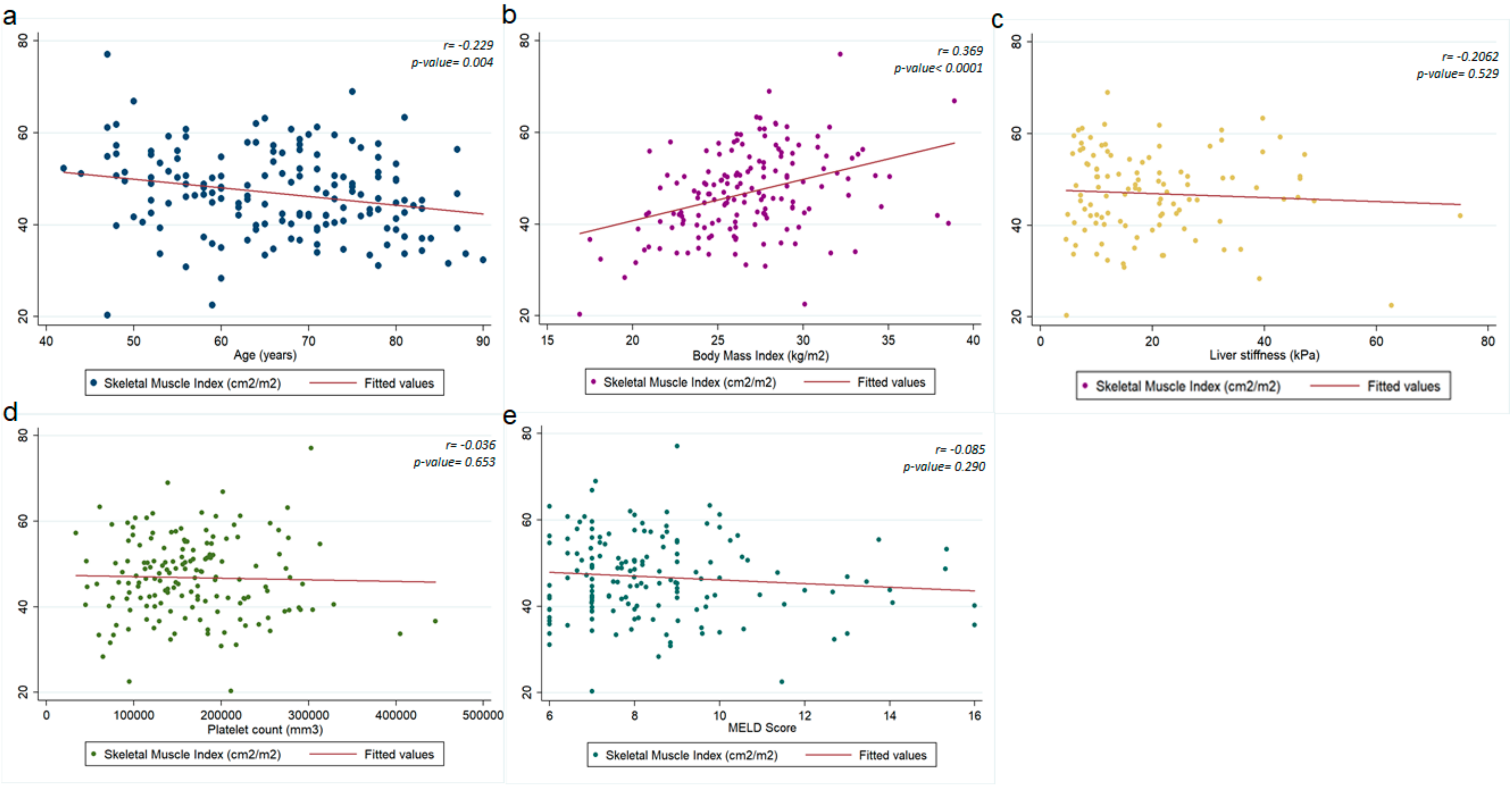
3.2. Factors Associated with the Presence of Sarcopenia among Liver Surgery Candidates
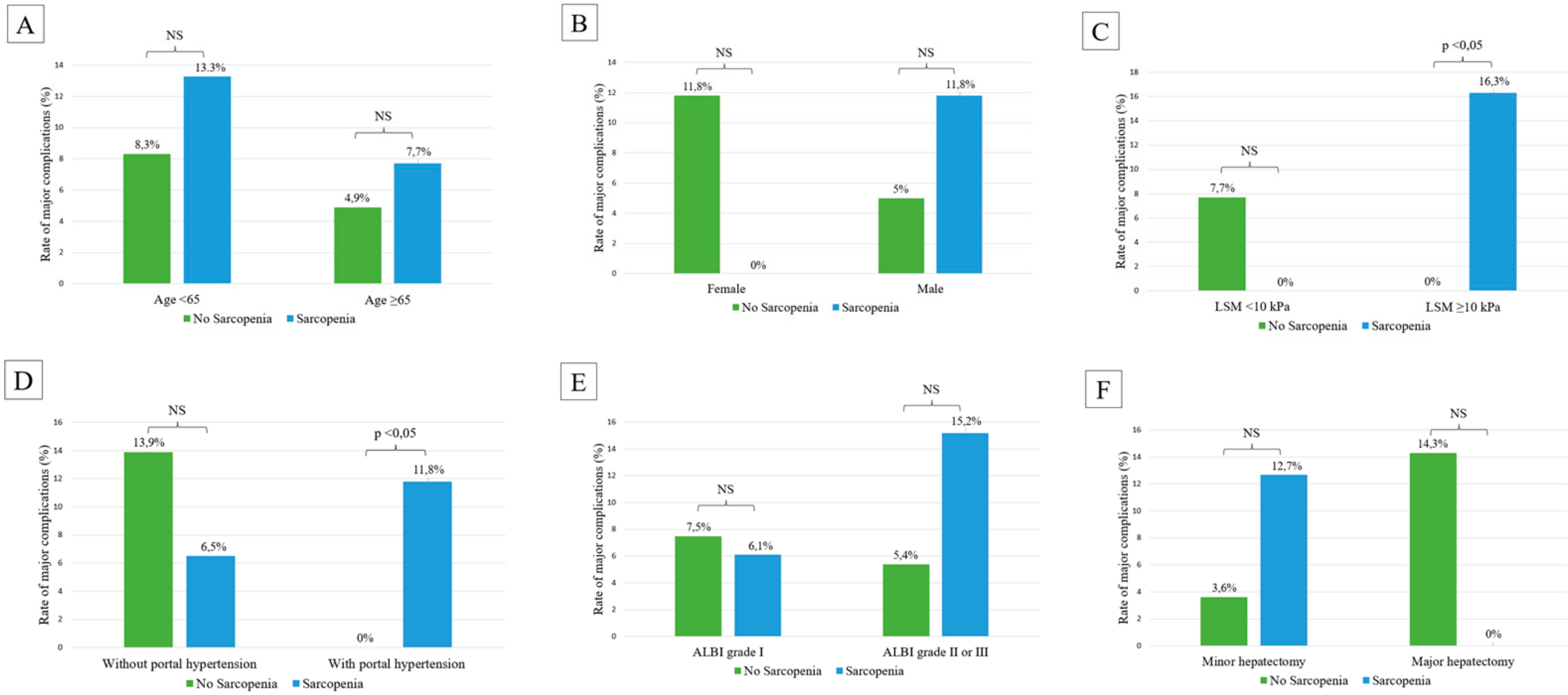
3.3. Factors Associated with Complications after Hepatic Resection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garuti, F.; Neri, A.; Avanzato, F.; Gramenzi, A.; Rampoldi, D.; Rucci, P.; Farinati, F.; Giannini, E.G.; Piscaglia, F.; Rapaccini, G.L.; et al. The changing scenario of hepatocellular carcinoma in Italy: An update. Liver Int. 2021, 41, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Marasco, G.; Colecchia, A.; Milandri, M.; Rossini, B.; Alemanni, L.V.; Dajti, E.; Ravaioli, F.; Renzulli, M.; Golfieri, R.; Festi, D. Non-invasive tests for the prediction of post-hepatectomy liver failure in the elderly. Hepatoma Res. 2020, 6, 32. [Google Scholar] [CrossRef]
- Cucchetti, A.; Cescon, M.; Colecchia, A.; Neri, F.; Cappelli, A.; Ravaioli, M.; Mazzotti, F.; Ercolani, G.; Festi, D.; Pinna, A. Adding Liver Stiffness Measurement to the Routine Evaluation of Hepatocellular Carcinoma Resectability Can Optimize Clinical Outcome. Ultraschall Med.-Eur. J. Ultrasound 2017, 38, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Capussotti, L.; Viganò, L.; Giuliante, F.; Ferrero, A.; Giovannini, I.; Nuzzo, G. Liver dysfunction and sepsis determine operative mortality after liver resection. Br. J. Surg. 2009, 96, 88–94. [Google Scholar] [CrossRef]
- Asenbaum, U.; Kaczirek, K.; Ba-Ssalamah, A.; Ringl, H.; Schwarz, C.; Waneck, F.; Fitschek, F.; Loewe, C.; Nolz, R. Post-hepatectomy liver failure after major hepatic surgery: Not only size matters. Eur. Radiol. 2018, 28, 4748–4756. [Google Scholar] [CrossRef] [Green Version]
- Marasco, G.; Colecchia, A.; Dajti, E.; Ravaioli, F.; Cucchetti, A.; Cescon, M.; Festi, D. Prediction of posthepatectomy liver failure: Role of SSM and LSPS. J. Surg. Oncol. 2019, 119, 400–401. [Google Scholar] [CrossRef]
- Theilig, D.; Steffen, I.; Malinowski, M.; Stockmann, M.; Seehofer, D.; Pratschke, J.; Hamm, B.; Denecke, T.; Geisel, D. Predicting liver failure after extended right hepatectomy following right portal vein embolization with gadoxetic acid-enhanced MRI. Eur. Radiol. 2019, 29, 5861–5872. [Google Scholar] [CrossRef]
- Fukushima, K.; Fukumoto, T.; Kuramitsu, K.; Kido, M.; Takebe, A.; Tanaka, M.; Itoh, T.; Ku, Y. Assessment of ISGLS Definition of Posthepatectomy Liver Failure and Its Effect on Outcome in Patients with Hepatocellular Carcinoma. J. Gastrointest. Surg. 2014, 18, 729–736. [Google Scholar] [CrossRef]
- Hwang, S.; Ha, T.Y.; Song, G.W.; Jung, D.H.; Ahn, C.S.; Moon, D.B.; Kim, K.H.; Lee, Y.J.; Lee, S.G. Quantified Risk Assessment for Major Hepatectomy via the Indocyanine Green Clearance Rate and Liver Volumetry Combined with Standard Liver Volume. J. Gastrointest. Surg. 2015, 19, 1305–1314. [Google Scholar] [CrossRef]
- Mai, R.Y.; Ye, J.Z.; Long, Z.R.; Shi, X.M.; Bai, T.; Chen, J.; Li, L.Q.; Wu, G.B.; Wu, F.X. Preoperative aspartate aminotransferase-to-platelet-ratio index as a predictor of posthepatectomy liver failure for resectable hepatocellular carcinoma. Cancer Manag. Res. 2019, 11, 1401–1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marasco, G.; Dajti, E.; Ravaioli, F.; Alemanni, L.V.; Capuano, F.; Gjini, K.; Colecchia, L.; Puppini, G.; Cusumano, C.; Renzulli, M.; et al. Spleen stiffness measurement for assessing the response to β-blockers therapy for high-risk esophageal varices patients. Hepatol. Int. 2020, 14, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Stefanescu, H.; Marasco, G.; Calès, P.; Fraquelli, M.; Rosselli, M.; Ganne-Carriè, N.; De Ledinghen, V.; Ravaioli, F.; Colecchia, A.; Rusu, C.; et al. A novel spleen-dedicated stiffness measurement by FibroScan® improves the screening of high-risk oesophageal varices. Liver Int. 2020, 40, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Ravaioli, F.; Colecchia, A.; Dajti, E.; Marasco, G.; Alemanni, L.V.; Tamè, M.; Azzaroli, F.; Brillanti, S.; Mazzella, G.; Festi, D. Spleen stiffness mirrors changes in portal hypertension after successful interferon-free therapy in chronic-hepatitis C virus patients. World J. Hepatol. 2018, 10, 731–742. [Google Scholar] [CrossRef]
- Dajti, E.; Ravaioli, F.; Colecchia, A.; Marasco, G.; Reggiani, M.L.B.; Colli, A.; Alemanni, L.V.; Tamè, M.; Andreone, P.; Brillanti, S.; et al. Spleen Stiffness Measurements Predict the Risk of Hepatic Decompensation after Direct-Acting Antivirals in HCV Cirrhotic Patients. Ultraschall Med.-Eur. J. Ultrasound 2020. [Google Scholar] [CrossRef]
- Cescon, M.; Colecchia, A.; Cucchetti, A.; Peri, E.; Montrone, L.; Ercolani, G.; Festi, D.; Pinna, A.D. Value of Transient Elastography Measured With Fibroscan in Predicting the Outcome of Hepatic Resection for Hepatocellular Carcinoma. Ann. Surg. 2012, 256, 706–713. [Google Scholar] [CrossRef]
- Marasco, G.; Dajti, E.; Ravaioli, F.; Brocchi, S.; Rossini, B.; Alemanni, L.V.; Peta, G.; Bartalena, L.; Golfieri, R.; Festi, D.; et al. Clinical impact of sarcopenia assessment in patients with liver cirrhosis. Expert Rev. Gastroenterol. Hepatol. 2020, 15, 377–388. [Google Scholar] [CrossRef]
- Marasco, G.; Sadalla, S.; Vara, G.; Golfieri, R.; Festi, D.; Colecchia, A.; Renzulli, M. Imaging Software-Based Sarcopenia Assessment in Gastroenterology: Evolution and Clinical Meaning. Can. J. Gastroenterol. Hepatol. 2021, 2021, 6669480. [Google Scholar] [CrossRef]
- Marasco, G.; Serenari, M.; Renzulli, M.; Alemanni, L.V.; Rossini, B.; Pettinari, I.; Dajti, E.; Ravaioli, F.; Golfieri, R.; Cescon, M.; et al. Clinical impact of sarcopenia assessment in patients with hepatocellular carcinoma undergoing treatments. J. Gastroenterol. 2020, 55, 927–943. [Google Scholar] [CrossRef]
- Otsuji, H.; Yokoyama, Y.; Ebata, T.; Igami, T.; Sugawara, G.; Mizuno, T.; Nagino, M. Preoperative sarcopenia negatively impacts postoperative outcomes following major hepatectomy with extrahepatic bile duct resection. World J. Surg. 2015, 39, 1494–1500. [Google Scholar] [CrossRef]
- Gomez-Perez, S.L.; Haus, J.M.; Sheean, P.; Patel, B.; Mar, W.; Chaudhry, V.; McKeever, L.; Braunschweig, C. Measuring abdominal circumference and skeletal muscle from a single cross-sectional computed tomography image: A step-by-step guide for clinicians using National Institutes of Health ImageJ. J. Parenter. Enter. Nutr. 2016, 40, 308–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carey, E.J.; Lai, J.C.; Wang, C.W.; Dasarathy, S.; Lobach, I.; Montano-Loza, A.J.; Dunn, M.A. A multicenter study to define sarcopenia in patients with end-stage liver disease. Liver Transpl. 2017, 23, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Berzigotti, A.; Zelber-Sagi, S.; Dasarathy, S.; Montagnese, S.; Genton, L.; Plauth, M.; Parés, A. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dajti, E.; Marasco, G.; Ravaioli, F.; Colecchia, L.; Ferrarese, A.; Festi, D.; Colecchia, A. Risk of hepatocellular carcinoma after HCV eradication: Determining the role of portal hypertension by measuring spleen stiffness. JHEP Rep. 2021, 3, 100289. [Google Scholar] [CrossRef]
- Marasco, G.; Alemanni, L.V.; Colecchia, A.; Festi, D.; Bazzoli, F.; Mazzella, G.; Montagnani, M.; Azzaroli, F. Prognostic value of the albumin-bilirubin grade for the prediction of post-hepatectomy liver failure: A systematic review and meta-analysis. J. Clin. Med. 2021, 10, 2011. [Google Scholar] [CrossRef]
- Marasco, G.; Colecchia, A.; Silva, G.; Rossini, B.; Eusebi, L.H.; Ravaioli, F.; Dajti, E.; Alemanni, L.V.; Colecchia, L.; Renzulli, M.; et al. Non-invasive tests for the prediction of primary hepatocellular carcinoma. World J. Gastroenterol. 2020, 26, 3326–3343. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. A nssessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach—The albi grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Brooke-Smith, M.; Crawford, M.; Adam, R.; Koch, M.; Makuuchi, M.; Dematteo, R.P.; Christophi, C.; et al. Posthepatectomy liver failure: A definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery 2011, 149, 713–724. [Google Scholar] [CrossRef]
- Tandon, P.; Ney, M.; Irwin, I.; Ma, M.M.; Gramlich, L.; Bain, V.G.; Esfandiari, N.; Baracos, V.; Montano-Loza, A.J.; Myers, R.P. Severe muscle depletion in patients on the liver transplant wait list: Its prevalence and independent prognostic value. Liver Transpl. 2012, 18, 1209–1216. [Google Scholar] [CrossRef]
- Durand, F.; Buyse, S.; Francoz, C.; Laouénan, C.; Bruno, O.; Belghiti, J.; Moreau, R.; Vilgrain, V.; Valla, D. Prognostic value of muscle atrophy in cirrhosis using psoas muscle thickness on computed tomography. J. Hepatol. 2014, 60, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Montano-Loza, A.J.; Meza-Junco, J.; Prado, C.M.M.; Lieffers, J.R.; Baracos, V.E.; Bain, V.G.; Sawyer, M.B. Muscle Wasting Is Associated With Mortality in Patients With Cirrhosis. Clin. Gastroenterol. Hepatol. 2012, 10, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Van Vugt, J.L.A.; Alferink, L.J.M.; Buettner, S.; Gaspersz, M.P.; Bot, D.; Murad, S.D.; Feshtali, S.; Van Ooijen, P.M.A.; Polak, W.G.; Porte, R.J.; et al. A model including sarcopenia surpasses the MELD score in predicting waiting list mortality in cirrhotic liver transplant candidates: A competing risk analysis in a national cohort. J. Hepatol. 2018, 68, 707–714. [Google Scholar] [CrossRef]
- Kamachi, S.; Mizuta, T.; Otsuka, T.; Nakashita, S.; Ide, Y.; Miyoshi, A.; Kitahara, K.; Eguchi, Y.; Ozaki, I.; Anzai, K. Sarcopenia is a risk factor for the recurrence of hepatocellular carcinoma after curative treatment. Hepatol. Res. 2016, 46, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Meza-Junco, J.; Montano-Loza, A.J.; Baracos, V.E.; Prado, C.M.M.; Bain, V.G.; Beaumont, C.; Esfandiari, N.; Lieffers, J.R.; Sawyer, M.B. Sarcopenia as a prognostic index of nutritional status in concurrent cirrhosis and hepatocellular carcinoma. J. Clin. Gastroenterol. 2013, 47, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Levolger, S.; Van Vledder, M.G.; Muslem, R.; Koek, M.; Niessen, W.J.; De Man, R.A.; De Bruin, R.W.F.; Ijzermans, J.N.M. Sarcopenia impairs survival in patients with potentially curable hepatocellular carcinoma. J. Surg. Oncol. 2015, 112, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Wang, C.W.; Lai, J.C.; Dasarathy, S.; Kappus, M.R.; Dunn, M.A.; Carey, E.J.; Montano-Loza, A.J. Poor performance of psoas muscle index for identification of patients with higher waitlist mortality risk in cirrhosis. J. Cachexia Sarcopenia Muscle 2018, 9, 1053–1062. [Google Scholar] [CrossRef]
- Liao, C.; Li, G.; Bai, Y.; Zhou, S.; Huang, L.; Yan, M.; Qiu, F.; Chen, J.; Wang, Y.; Tian, Y.; et al. Prognostic value and association of sarcopenic obesity and systemic inflammatory indexes in patients with hepatocellular carcinoma following hepatectomy and the establishment of novel predictive nomograms. J. Gastrointest. Oncol. 2021, 12, 669–693. [Google Scholar] [CrossRef]
- Tanaka, S.; Ueno, M.; Iida, H.; Kaibori, M.; Nomi, T.; Hirokawa, F.; Ikoma, H.; Nakai, T.; Eguchi, H.; Kubo, S. Preoperative assessment of frailty predicts age-related events after hepatic resection: A prospective multicenter study. J. Hepatobiliary Pancreat. Sci. 2018, 25, 377–387. [Google Scholar] [CrossRef]
- Bosch, J.; Abraldes, J.G.; Berzigotti, A.; García-Pagan, J.C. The clinical use of HVPG measurements in chronic liver disease. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 573–582. [Google Scholar] [CrossRef]
- Cucchetti, A.; Ercolani, G.; Vivarelli, M.; Cescon, M.; Ravaioli, M.; Ramacciato, G.; Grazi, G.L.; Pinna, A.D. Is portal hypertension a contraindication to hepatic resection? Ann. Surg. 2009, 250, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Cucchetti, A.; Cescon, M.; Golfieri, R.; Piscaglia, F.; Renzulli, M.; Neri, F.; Cappelli, A.; Mazzotti, F.; Mosconi, C.; Colecchia, A.; et al. Hepatic venous pressure gradient in the preoperative assessment of patients with resectable hepatocellular carcinoma. J. Hepatol. 2016, 64, 79–86. [Google Scholar] [CrossRef]
- Berzigotti, A.; Reig, M.; Abraldes, J.G.; Bosch, J.; Bruix, J. Portal hypertension and the outcome of surgery for hepatocellular carcinoma in compensated cirrhosis: A systematic review and meta-analysis. Hepatology 2015, 61, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.-H.; Li, L.-Q. Portal hypertension should not be a contraindication of hepatic resection to treat hepatocellular carcinoma with compensated cirrhosis. Hepatology 2015, 62, 977–978. [Google Scholar] [CrossRef]
- Rodrigues, S.G.; Brabandt, B.; Stirnimann, G.; Maurer, M.H.; Berzigotti, A. Adipopenia correlates with higher portal pressure in patients with cirrhosis. Liver Int. 2019, 39, 1672–1681. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Jeong, W.K.; Baik, S.K.; Cha, S.H.; Kim, M.Y. Impact of sarcopenia on prognostic value of cirrhosis: Going beyond the hepatic venous pressure gradient and MELD score. J. Cachexia Sarcopenia Muscle 2018, 9, 860–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koya, S.; Kawaguchi, T.; Hashida, R.; Hirota, K.; Bekki, M.; Goto, E.; Yamada, M.; Sugimoto, M.; Hayashi, S.; Goshima, N.; et al. Effects of in-hospital exercise on sarcopenia in hepatoma patients who underwent transcatheter arterial chemoembolization. J. Gastroenterol. Hepatol. 2019, 34, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Brustia, R.; Savier, E.; Scatton, O. Physical exercise in cirrhotic patients: Towards prehabilitation on waiting list for liver transplantation. A systematic review and meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Duarte-Rojo, A.; Ruiz-Margáin, A.; Montaño-Loza, A.J.; Macías-Rodríguez, R.U.; Ferrando, A.; Kim, W.R. Exercise and physical activity for patients with end-stage liver disease: Improving functional status and sarcopenia while on the transplant waiting list. Liver Transpl. 2018, 24, 122–139. [Google Scholar] [CrossRef] [Green Version]
- Sato, N.; Kenjo, A.; Kimura, T.; Okada, R.; Ishigame, T.; Kofunato, Y.; Shimura, T.; Abe, K.; Ohira, H.; Marubashi, S. Prediction of major complications after hepatectomy using liver stiffness values determined by magnetic resonance elastography. Br. J. Surg. 2018, 105, 1192–1199. [Google Scholar] [CrossRef]
- Zhou, P.; Chen, B.; Miao, X.Y.; Zhou, J.J.; Xiong, L.; Wen, Y.; Zou, H. Comparison of FIB-4 Index and Child-Pugh Score in Predicting the Outcome of Hepatic Resection for Hepatocellular Carcinoma. J. Gastrointest. Surg. 2019, 24, 823–831. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 159) | Patients with Sarcopenia (n = 82) | Patients without Sarcopenia (n = 77) | p-Value |
|---|---|---|---|---|
| Age | 68 (58–75) | 71 (60–78) | 65 (54–71) | 0.003 |
| Sex (male) | 128 (80.5%) | 68 (82.93%) | 60 (77.92%) | 0.426 |
| BMI (kg/m2) | 26.3 (24.4–28.7) | 25.6 (23.8–27.8) | 27.5 (25.6–29.4) | 0.0009 |
| Overweight (BMI > 25 kg/m2) | 110 (69.18%) | 47 (57.32%) | 63 (81.8%) | 0.001 |
| Liver disease etiology | 0.385 | |||
| Viral | 106 (66.67%) | 55 (67.07%) | 51 (66.23%) | |
| NAFLD | 24 (15.09%) | 14 (17.07%) | 10 (12.99%) | |
| ALD | 6 (3.77%) | 2 (2.44%) | 4 (5.19%) | |
| Other | 23 (14.47%) | 11 (13.75%) | 12 (15.58%) | |
| Co-morbidities | ||||
| Diabetes mellitus | 46 (28.93%) | 25 (30.49%) | 21 (27.27%) | 0.655 |
| Liver disease severity | ||||
| LSM (kPa) (n = 108) | 16.4 (10.1–25.4) | 17.3 (10.1–26.3) | 14 (10.1–25.1) | 0.499 |
| Platelets (cells × 109/L) | 158 (115–202) | 148 (115–211) | 165 (119–194) | 0.658 |
| Esophageal varices (n = 154) | 44 (28.57%) | 22 (27.16%) | 22 (30.14%) | 0.683 |
| Portal hypertension | 92 (57.86%) | 51 (62.2%) | 41 (53.25%) | 0.253 |
| MELD score | 8 (7–9) | 8 (7–10) | 8 (7–9) | 0.290 |
| Child-Pugh score | 5 (5–5) | 5 (5–6) | 5 (5–5) | 0.275 |
| ALBI grade > 1 | 70 (44.03%) | 33 (40.24%) | 37 (48.05%) | 0.322 |
| Liver cancer | ||||
| Alpha-fetoprotein | 17 (6–103) | 18 (4–94) | 16 (7–125) | 0.666 |
| Number of HCC | 1 (1–1) | 1 (1–1) | 1 (1–1) | 0.923 |
| Maximum diameter of HCCnodule (mm) | 37 (23–60) | 38 (25–55) | 35 (23–60) | 0.811 |
| Major hepatectomy | 40 (25.2%) | 19 (23.17%) | 21 (27.27%) | 0.551 |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95%-CI) | p-Value | OR (95%-CI) | p-Value | |
| Age | 1.046 (1.015–1.078) | 0.003 | 1.046 (1.014–1.079) | 0.004 |
| Sex (male) | 1.376 (0.626–3.026) | 0.427 | ||
| BMI (kg/m2) | 0.878 (0.802–0.962) | 0.005 | 0.879 (0.801–0.965) | 0.007 |
| Diabetes mellitus | 1.170 (0.588–2.326) | 0.655 | ||
| LSM (kPa) (n = 108) | 1.165 (0.476–2.850) | 0.739 | ||
| Platelets (cells ×109/L) | 0.999 (0.999–1.0001) | 0.726 | ||
| Esophageal varices (n = 154) | 0.864 (0.429–1.740) | 0.683 | ||
| Portal hypertension | 1.445 (0.768–2.718) | 0.254 | ||
| MELD score | 1.089 (0.949–1.250) | 0.225 | ||
| Child-Pugh score | 1.215 (0.684–2.159) | 0.506 | ||
| ALBI score | 0.837 (0.550–1.273) | 0.405 | ||
| Maximum diameter of HCC nodule (mm) | 1.0001 (0.991–1.009) | 0.988 | ||
| Number of HCC nodules | 0.956 (0.614–1.289) | 0.842 | ||
| Major Complications | PHLF B or C | |||
|---|---|---|---|---|
| Variables | Univariate Analysis | Univariate Analysis | ||
| OR (95%-CI) | p-Value | OR (95%-CI) | p-Value | |
| Age | 0.974 (0.926–1.026) | 0.322 | 0.980 (0.933–1.030) | 0.432 |
| Sex (male) | 1.363 (0.286–6.491) | 0.697 | 0.577 (0.168–1.979) | 0.382 |
| BMI (kg/m2) | 1.037 (0.895–1.201) | 0.631 | 0.890 (0.760–1.041) | 0.146 |
| Diabetes mellitus | 2.271 (0.720–7.170) | 0.162 | 0.971 (0.289–3.271) | 0.963 |
| LSM > 10 kPa (n = 108) | 2.660 (0.512–13.822) | 0.244 | 13.565 (1.705–107.907) | 0.014 |
| Thrombocytopenia | 1.011 (0.329–3.154) | 0.985 | 4.849 (1.297–18.127) | 0.019 |
| Esophageal varices (n = 154) | 0.429 (0.091–1.740) | 0.284 | 2.757 (0.906–8.391) | 0.074 |
| Portal hypertension | 0.598 (0.191–1.868) | 0.376 | 3.384 (1.076–10.642) | 0.037 |
| MELD score | 1.211 (1.018–1.442) | 0.031 | 1.144 (0.962–1.360) | 0.127 |
| Child-Pugh score | 2.050 (0.684–2.159) | 0.085 | 2.218 (1.008–4.883) | 0.048 |
| ALBI score | 1.981 (0.715–5.488) | 0.188 | 7.195 (2.171–23.844) | 0.001 |
| Major hepatectomy | 0.884 (0.231–3.385) | 0.857 | 0.818 (0.216–3.097) | 0.768 |
| Sarcopenia (dichotomous) | 1.557 (0.486–4.983) | 0.453 | 1.751 (0.559–5.479) | 0.336 |
| SMI (continuous) | 0.975 (0.918–1.036) | 0.410 | 0.972 (0.917–1.032) | 0.362 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marasco, G.; Dajti, E.; Serenari, M.; Alemanni, L.V.; Ravaioli, F.; Ravaioli, M.; Vestito, A.; Vara, G.; Festi, D.; Golfieri, R.; et al. Sarcopenia Predicts Major Complications after Resection for Primary Hepatocellular Carcinoma in Compensated Cirrhosis. Cancers 2022, 14, 1935. https://doi.org/10.3390/cancers14081935
Marasco G, Dajti E, Serenari M, Alemanni LV, Ravaioli F, Ravaioli M, Vestito A, Vara G, Festi D, Golfieri R, et al. Sarcopenia Predicts Major Complications after Resection for Primary Hepatocellular Carcinoma in Compensated Cirrhosis. Cancers. 2022; 14(8):1935. https://doi.org/10.3390/cancers14081935
Chicago/Turabian StyleMarasco, Giovanni, Elton Dajti, Matteo Serenari, Luigina Vanessa Alemanni, Federico Ravaioli, Matteo Ravaioli, Amanda Vestito, Giulio Vara, Davide Festi, Rita Golfieri, and et al. 2022. "Sarcopenia Predicts Major Complications after Resection for Primary Hepatocellular Carcinoma in Compensated Cirrhosis" Cancers 14, no. 8: 1935. https://doi.org/10.3390/cancers14081935