
Monoclonal Antibodies in the Treatment of Diffuse Large B-Cell Lymphoma: Moving beyond Rituximab

 ,
, 
Abstract
:Simple Summary
Abstract
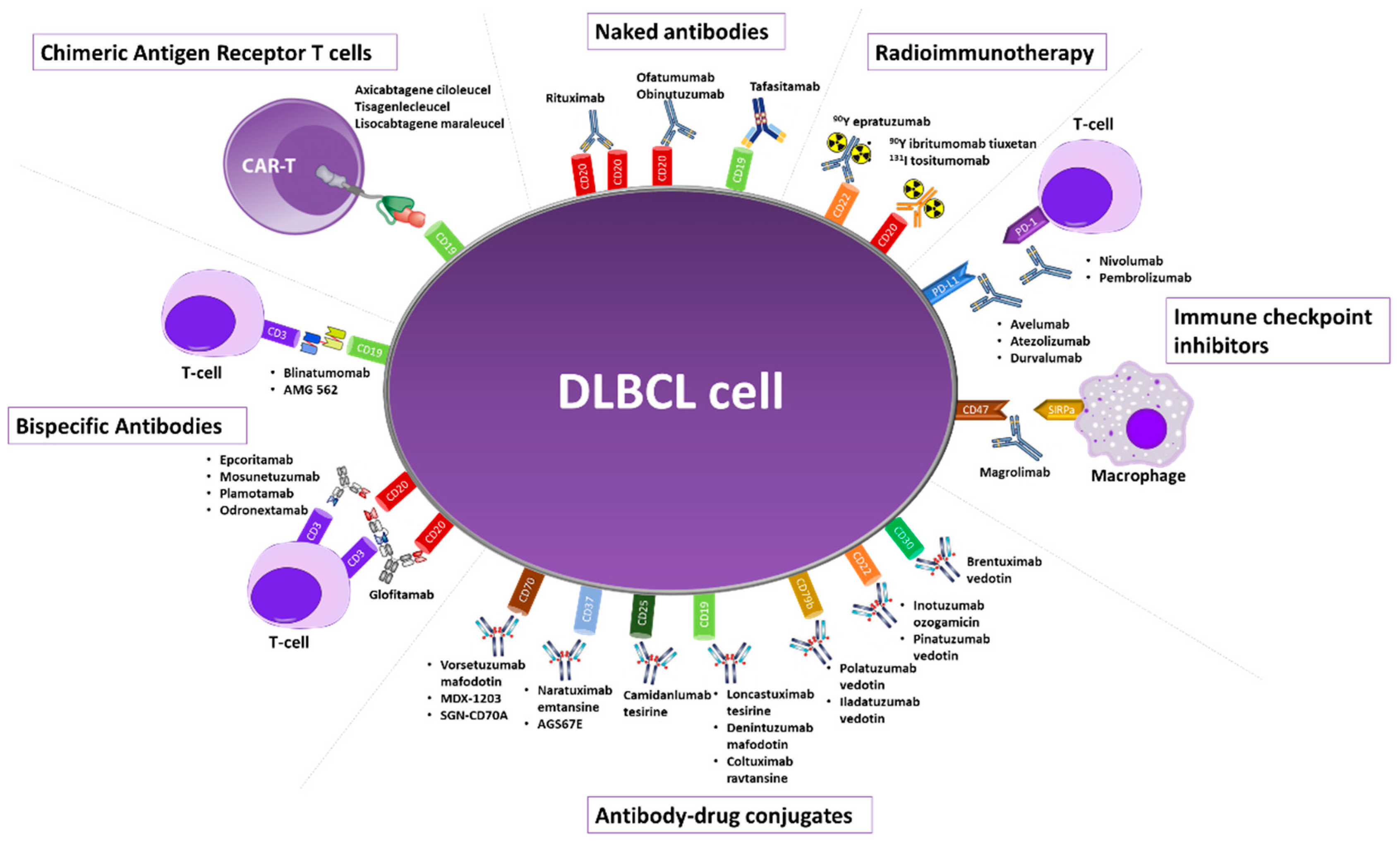
1. Introduction
2. Anti-CD20 Monoclonal Antibodies
2.1. Rituximab
2.2. Ofatumumab
2.3. Obinutuzumab
3. Enhanced Monoclonal Antibodies
Tafasitamab
4. Checkpoint Inhibitors
4.1. Nivolumab
4.2. Pembrolizumab
4.3. Magrolimab
4.4. Other Checkpoint Inhibitors
5. Radioimmunotherapy
6. Antibody-Drug Conjugates
6.1. Commercially Available Antibody-Drug Conjugates
6.1.1. Brentuximab Vedotin
6.1.2. Inotuzumab Ozogamicin
6.1.3. Polatuzumab Vedotin
6.1.4. Loncastuximab Tesirine
6.2. Investigational Antibody-Drug Conjugates
6.2.1. Other Anti-CD19
6.2.2. Other Anti-CD22
6.2.3. Anti-CD25
6.2.4. Anti-CD37
6.2.5. Anti-CD70
6.2.6. Anti-CD79b
6.2.7. Anti-ROR1
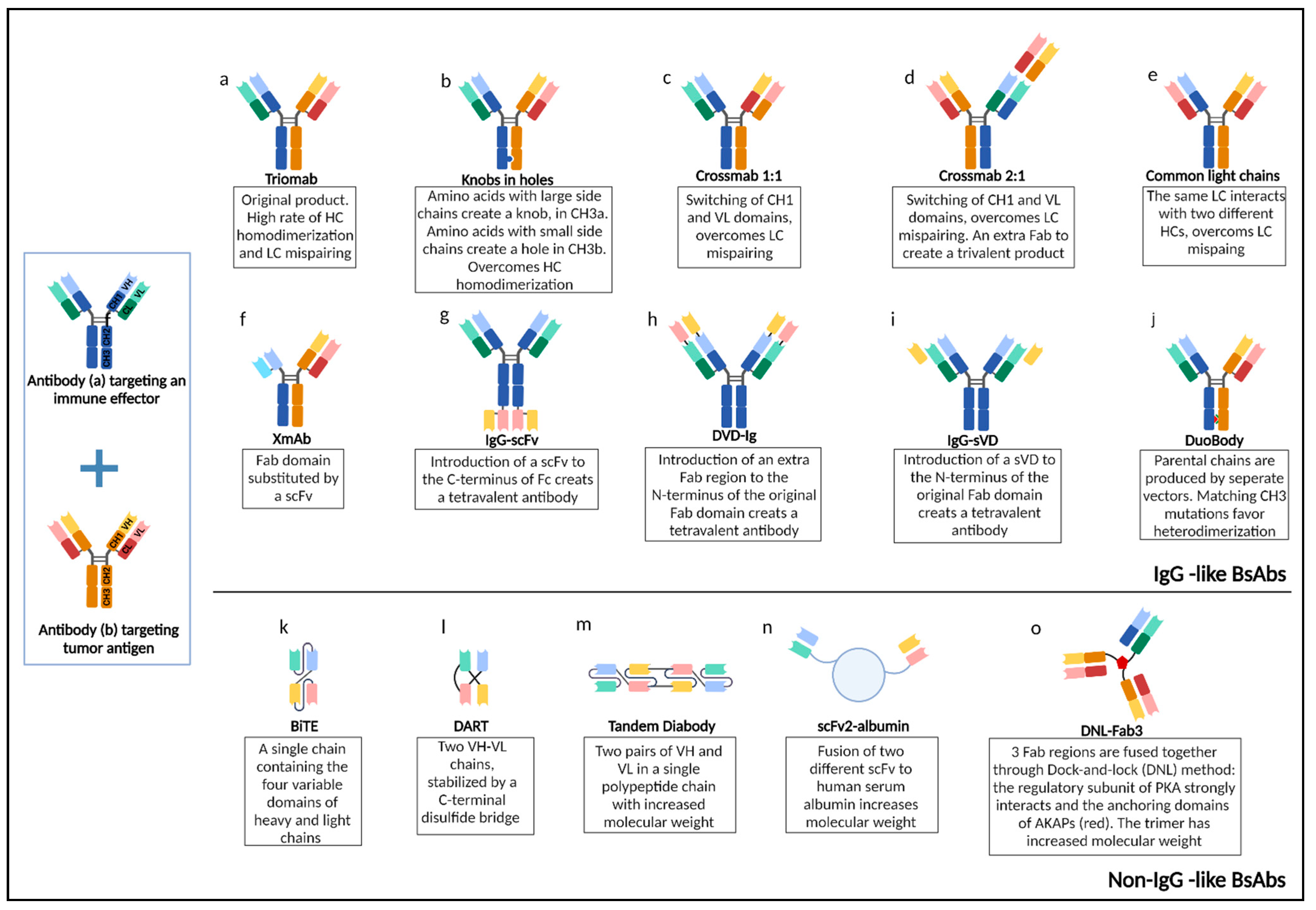
7. Bispecific Antibodies
7.1. Targeting CD20
7.1.1. Glofitamab
7.1.2. Epcoritamab
7.1.3. Mosunetuzumab
7.1.4. Odronextamab
7.1.5. Plamotamab
7.2. Targeting CD19
7.2.1. Blinatumomab
7.2.2. Other CD19 Targeting BsAbs
7.3. Targeting CD47
7.4. Bispecific ADCs
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fisher, R.I.; Gaynor, E.R.; Dahlberg, S.; Oken, M.M.; Grogan, T.M.; Mize, E.M.; Glick, J.H.; Coltman, C.A., Jr.; Miller, T.P. Comparison of a standard regimen (CHOP) with three intensive chemotherapy regimens for advanced non-Hodgkin’s lymphoma. N. Engl. J. Med. 1993, 328, 1002–1006. [Google Scholar] [CrossRef]
- Pfreundschuh, M.; Trumper, L.; Kloess, M.; Schmits, R.; Feller, A.C.; Rube, C.; Rudolph, C.; Reiser, M.; Hossfeld, D.K.; Eimermacher, H.; et al. Two-weekly or 3-weekly CHOP chemotherapy with or without etoposide for the treatment of elderly patients with aggressive lymphomas: Results of the NHL-B2 trial of the DSHNHL. Blood 2004, 104, 634–641. [Google Scholar] [CrossRef]
- Pfreundschuh, M.; Trumper, L.; Kloess, M.; Schmits, R.; Feller, A.C.; Rudolph, C.; Reiser, M.; Hossfeld, D.K.; Metzner, B.; Hasenclever, D.; et al. Two-weekly or 3-weekly CHOP chemotherapy with or without etoposide for the treatment of young patients with good-prognosis (normal LDH) aggressive lymphomas: Results of the NHL-B1 trial of the DSHNHL. Blood 2004, 104, 626–633. [Google Scholar] [CrossRef] [Green Version]
- Stiff, P.J.; Unger, J.M.; Cook, J.R.; Constine, L.S.; Couban, S.; Stewart, D.A.; Shea, T.C.; Porcu, P.; Winter, J.N.; Kahl, B.S.; et al. Autologous transplantation as consolidation for aggressive non-Hodgkin’s lymphoma. N. Engl. J. Med. 2013, 369, 1681–1690. [Google Scholar] [CrossRef] [Green Version]
- Papageorgiou, S.G.; Thomopoulos, T.P.; Katagas, I.; Bouchla, A.; Pappa, V. Prognostic molecular biomarkers in diffuse large B-cell lymphoma in the rituximab era and their therapeutic implications. Ther. Adv. Hematol. 2021, 12, 20406207211013987. [Google Scholar] [CrossRef]
- Coiffier, B.; Haioun, C.; Ketterer, N.; Engert, A.; Tilly, H.; Ma, D.; Johnson, P.; Lister, A.; Feuring-Buske, M.; Radford, J.A.; et al. Rituximab (anti-CD20 monoclonal antibody) for the treatment of patients with relapsing or refractory aggressive lymphoma: A multicenter phase II study. Blood 1998, 92, 1927–1932. [Google Scholar]
- Coiffier, B.; Lepage, E.; Brière, J.; Herbrecht, R.; Tilly, H.; Bouabdallah, R.; Morel, P.; Van Den Neste, E.; Salles, G.; Gaulard, P.; et al. CHOP Chemotherapy plus Rituximab Compared with CHOP Alone in Elderly Patients with Diffuse Large-B-Cell Lymphoma. N. Engl. J. Med. 2002, 346, 235–242. [Google Scholar] [CrossRef]
- Coiffier, B.; Thieblemont, C.; Van Den Neste, E.; Lepeu, G.; Plantier, I.; Castaigne, S.; Lefort, S.; Marit, G.; Macro, M.; Sebban, C.; et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: A study by the Groupe d’Etudes des Lymphomes de l’Adulte. Blood 2010, 116, 2040–2045. [Google Scholar] [CrossRef]
- Pfreundschuh, M.; Kuhnt, E.; Trümper, L.; Osterborg, A.; Trneny, M.; Shepherd, L.; Gill, D.S.; Walewski, J.; Pettengell, R.; Jaeger, U.; et al. CHOP-like chemotherapy with or without rituximab in young patients with good-prognosis diffuse large-B-cell lymphoma: 6-year results of an open-label randomised study of the MabThera International Trial (MInT) Group. Lancet Oncol. 2011, 12, 1013–1022. [Google Scholar] [CrossRef]
- Habermann, T.M.; Weller, E.A.; Morrison, V.A.; Gascoyne, R.D.; Cassileth, P.A.; Cohn, J.B.; Dakhil, S.R.; Woda, B.; Fisher, R.I.; Peterson, B.A.; et al. Rituximab-CHOP versus CHOP alone or with maintenance rituximab in older patients with diffuse large B-cell lymphoma. J. Clin. Oncol. 2006, 24, 3121–3127. [Google Scholar] [CrossRef]
- Sehn, L.H.; Donaldson, J.; Chhanabhai, M.; Fitzgerald, C.; Gill, K.; Klasa, R.; MacPherson, N.; O’Reilly, S.; Spinelli, J.J.; Sutherland, J.; et al. Introduction of combined CHOP plus rituximab therapy dramatically improved outcome of diffuse large B-cell lymphoma in British Columbia. J. Clin. Oncol. 2005, 23, 5027–5033. [Google Scholar] [CrossRef] [PubMed]
- Pfreundschuh, M.; Schubert, J.; Ziepert, M.; Schmits, R.; Mohren, M.; Lengfelder, E.; Reiser, M.; Nickenig, C.; Clemens, M.; Peter, N.; et al. Six versus eight cycles of bi-weekly CHOP-14 with or without rituximab in elderly patients with aggressive CD20+ B-cell lymphomas: A randomised controlled trial (RICOVER-60). Lancet Oncol. 2008, 9, 105–116. [Google Scholar] [CrossRef]
- Rieger, M.; Österborg, A.; Pettengell, R.; White, D.; Gill, D.; Walewski, J.; Kuhnt, E.; Loeffler, M.; Pfreundschuh, M.; Ho, A.D. Primary mediastinal B-cell lymphoma treated with CHOP-like chemotherapy with or without rituximab: Results of the Mabthera International Trial Group study. Ann. Oncol. 2011, 22, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Vassilakopoulos, T.P.; Pangalis, G.A.; Katsigiannis, A.; Papageorgiou, S.G.; Constantinou, N.; Terpos, E.; Zorbala, A.; Vrakidou, E.; Repoussis, P.; Poziopoulos, C.; et al. Rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone with or without radiotherapy in primary mediastinal large B-cell lymphoma: The emerging standard of care. Oncologist 2012, 17, 239–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreri, A.J.; Cwynarski, K.; Pulczynski, E.; Ponzoni, M.; Deckert, M.; Politi, L.S.; Torri, V.; Fox, C.P.; Rosee, P.L.; Schorb, E.; et al. Chemoimmunotherapy with methotrexate, cytarabine, thiotepa, and rituximab (MATRix regimen) in patients with primary CNS lymphoma: Results of the first randomisation of the International Extranodal Lymphoma Study Group-32 (IELSG32) phase 2 trial. Lancet. Haematol. 2016, 3, e217–e227. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, N.L.; Wilson, W.H.; Jung, S.H.; Hsi, E.D.; Maurer, M.J.; Pederson, L.D.; Polley, M.C.; Pitcher, B.N.; Cheson, B.D.; Kahl, B.S.; et al. Dose-Adjusted EPOCH-R Compared With R-CHOP as Frontline Therapy for Diffuse Large B-Cell Lymphoma: Clinical Outcomes of the Phase III Intergroup Trial Alliance/CALGB 50303. J. Clin. Oncol. 2019, 37, 1790–1799. [Google Scholar] [CrossRef]
- Cunningham, D.; Hawkes, E.A.; Jack, A.; Qian, W.; Smith, P.; Mouncey, P.; Pocock, C.; Ardeshna, K.M.; Radford, J.A.; McMillan, A.; et al. Rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisolone in patients with newly diagnosed diffuse large B-cell non-Hodgkin lymphoma: A phase 3 comparison of dose intensification with 14-day versus 21-day cycles. Lancet 2013, 381, 1817–1826. [Google Scholar] [CrossRef] [Green Version]
- Delarue, R.; Tilly, H.; Mounier, N.; Petrella, T.; Salles, G.; Thieblemont, C.; Bologna, S.; Ghesquières, H.; Hacini, M.; Fruchart, C.; et al. Dose-dense rituximab-CHOP compared with standard rituximab-CHOP in elderly patients with diffuse large B-cell lymphoma (the LNH03-6B study): A randomised phase 3 trial. Lancet Oncol. 2013, 14, 525–533. [Google Scholar] [CrossRef]
- Pfreundschuh, M.; Muller, C.; Zeynalova, S.; Kuhnt, E.; Wiesen, M.H.; Held, G.; Rixecker, T.; Poeschel, V.; Zwick, C.; Reiser, M.; et al. Suboptimal dosing of rituximab in male and female patients with DLBCL. Blood 2014, 123, 640–646. [Google Scholar] [CrossRef] [Green Version]
- Pfreundschuh, M.; Murawski, N.; Zeynalova, S.; Ziepert, M.; Loeffler, M.; Hanel, M.; Dierlamm, J.; Keller, U.; Dreyling, M.; Truemper, L.; et al. Optimization of rituximab for the treatment of DLBCL: Increasing the dose for elderly male patients. Br. J. Haematol. 2017, 179, 410–420. [Google Scholar] [CrossRef] [Green Version]
- Pfreundschuh, M.; Poeschel, V.; Zeynalova, S.; Hanel, M.; Held, G.; Schmitz, N.; Viardot, A.; Dreyling, M.H.; Hallek, M.; Mueller, C.; et al. Optimization of rituximab for the treatment of diffuse large B-cell lymphoma (II): Extended rituximab exposure time in the SMARTE-R-CHOP-14 trial of the german high-grade non-Hodgkin lymphoma study group. J. Clin. Oncol. 2014, 32, 4127–4133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaeger, U.; Trneny, M.; Melzer, H.; Praxmarer, M.; Nawarawong, W.; Ben Yehuda, D.; Goldstein, D.; Mihaljevic, B.; Ilhan, O.; Ballova, V.; et al. Rituximab maintenance for patients with aggressive B-cell lymphoma in first remission: Results of the randomized NHL13 trial. Haematologica 2015, 100, 955–963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witzens-Harig, M.; Benner, A.; McClanahan, F.; Klemmer, J.; Brandt, J.; Brants, E.; Rieger, M.; Meissner, J.; Hensel, M.; Neben, K.; et al. Rituximab maintenance improves survival in male patients with diffuse large B-cell lymphoma. Results of the HD2002 prospective multicentre randomized phase III trial. Br. J. Haematol. 2015, 171, 710–719. [Google Scholar] [CrossRef] [Green Version]
- Vassilakopoulos, T.P.; Apostolidis, J.; Angelopoulou, M.K. Comment on “Rituximab maintenance for patients with aggressive B-cell lymphoma in first remission: Results of the randomized NHL13 trial”. Haematologica 2015, 100, e480–e481. [Google Scholar] [CrossRef] [PubMed]
- Gisselbrecht, C.; Schmitz, N.; Mounier, N.; Singh Gill, D.; Linch, D.C.; Trneny, M.; Bosly, A.; Milpied, N.J.; Radford, J.; Ketterer, N.; et al. Rituximab maintenance therapy after autologous stem-cell transplantation in patients with relapsed CD20(+) diffuse large B-cell lymphoma: Final analysis of the collaborative trial in relapsed aggressive lymphoma. J. Clin. Oncol. 2012, 30, 4462–4469. [Google Scholar] [CrossRef] [Green Version]
- Coiffier, B.; Radford, J.; Bosly, A.; Martinelli, G.; Verhoef, G.; Barca, G.; Davies, A.; Decaudin, D.; Gallop-Evans, E.; Padmanabhan-Iyer, S.; et al. A multicentre, phase II trial of ofatumumab monotherapy in relapsed/progressive diffuse large B-cell lymphoma. Br. J. Haematol. 2013, 163, 334–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galanina, N.; Jasielec, J.; Peace, D.; Smith, S.M.; Nabhan, C. Ofatumumab monotherapy in relapsed/refractory diffuse large B-cell non-Hodgkin lymphoma. Leuk. Lymphoma 2017, 58, 752–753. [Google Scholar] [CrossRef]
- van Imhoff, G.W.; McMillan, A.; Matasar, M.J.; Radford, J.; Ardeshna, K.M.; Kuliczkowski, K.; Kim, W.; Hong, X.; Goerloev, J.S.; Davies, A.; et al. Ofatumumab Versus Rituximab Salvage Chemoimmunotherapy in Relapsed or Refractory Diffuse Large B-Cell Lymphoma: The ORCHARRD Study. J. Clin. Oncol. 2017, 35, 544–551. [Google Scholar] [CrossRef]
- Peyrade, F.; Bologna, S.; Delwail, V.; Emile, J.F.; Pascal, L.; Fermé, C.; Schiano, J.M.; Coiffier, B.; Corront, B.; Farhat, H.; et al. Combination of ofatumumab and reduced-dose CHOP for diffuse large B-cell lymphomas in patients aged 80 years or older: An open-label, multicentre, single-arm, phase 2 trial from the LYSA group. Lancet. Haematol. 2017, 4, e46–e55. [Google Scholar] [CrossRef]
- Flinn, I.W.; Erter, J.; Daniel, D.B.; Mace, J.R.; Berdeja, J.G. Phase II Study of Bendamustine and Ofatumumab in Elderly Patients with Newly Diagnosed Diffuse Large B-Cell Lymphoma Who Are Poor Candidates for R-CHOP Chemotherapy. Oncologist 2019, 24, 1035.e623. [Google Scholar] [CrossRef] [Green Version]
- Morschhauser, F.A.; Cartron, G.; Thieblemont, C.; Solal-Céligny, P.; Haioun, C.; Bouabdallah, R.; Feugier, P.; Bouabdallah, K.; Asikanius, E.; Lei, G.; et al. Obinutuzumab (GA101) monotherapy in relapsed/refractory diffuse large b-cell lymphoma or mantle-cell lymphoma: Results from the phase II GAUGUIN study. J. Clin. Oncol. 2013, 31, 2912–2919. [Google Scholar] [CrossRef] [PubMed]
- Vitolo, U.; Trněný, M.; Belada, D.; Burke, J.M.; Carella, A.M.; Chua, N.; Abrisqueta, P.; Demeter, J.; Flinn, I.; Hong, X.; et al. Obinutuzumab or Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone in Previously Untreated Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. 2017, 35, 3529–3537. [Google Scholar] [CrossRef] [PubMed]
- Oestergaard, M.Z.; Bolen, C.; Mattiello, F.; Martelli, M.; Sehn, L.H.; Trněný, M.; Tzankov, A.; Vitolo, U.; Nielsen, T.; Morariu-Zamfir, R.; et al. Superiority of Obinutuzumab over Rituximab in a New Molecular Follicular Lymphoma-like Subgroup of DLBCL: Results from an Exploratory Analysis of the Phase 3 GOYA Trial. Blood 2017, 130, 1543. [Google Scholar] [CrossRef]
- Le Gouill, S.; Ghesquières, H.; Oberic, L.; Morschhauser, F.; Tilly, H.; Ribrag, V.; Lamy, T.; Thieblemont, C.; Maisonneuve, H.; Gressin, R.; et al. Obinutuzumab vs rituximab for advanced DLBCL: A PET-guided and randomized phase 3 study by LYSA. Blood 2021, 137, 2307–2320. [Google Scholar] [CrossRef]
- Kellner, C.; Zhukovsky, E.A.; Pötzke, A.; Brüggemann, M.; Schrauder, A.; Schrappe, M.; Kneba, M.; Repp, R.; Humpe, A.; Gramatzki, M.; et al. The Fc-engineered CD19 antibody MOR208 (XmAb5574) induces natural killer cell-mediated lysis of acute lymphoblastic leukemia cells from pediatric and adult patients. Leukemia 2013, 27, 1595–1598. [Google Scholar] [CrossRef] [Green Version]
- Jurczak, W.; Zinzani, P.L.; Gaidano, G.; Goy, A.; Provencio, M.; Nagy, Z.; Robak, T.; Maddocks, K.; Buske, C.; Ambarkhane, S.; et al. Phase IIa study of the CD19 antibody MOR208 in patients with relapsed or refractory B-cell non-Hodgkin’s lymphoma. Ann. Oncol. 2018, 29, 1266–1272. [Google Scholar] [CrossRef]
- Salles, G.; Duell, J.; González Barca, E.; Tournilhac, O.; Jurczak, W.; Liberati, A.M.; Nagy, Z.; Obr, A.; Gaidano, G.; André, M.; et al. Tafasitamab plus lenalidomide in relapsed or refractory diffuse large B-cell lymphoma (L-MIND): A multicentre, prospective, single-arm, phase 2 study. Lancet Oncol. 2020, 21, 978–988. [Google Scholar] [CrossRef]
- Düll, J.; Maddocks, K.J.; Gonzalez-Barca, E.; Jurczak, W.; Liberati, A.M.; Obr, A.; Gaidano, G.; Abrisqueta, P.; André, M.; Dreyling, M.H.; et al. Long-term analyses from L-MIND, a phase II study of tafasitamab (MOR208) combined with lenalidomide (LEN) in patients with relapsed or refractory diffuse large B-cell lymphoma (R/R DLBCL). J. Clin. Oncol. 2021, 39, 7513. [Google Scholar] [CrossRef]
- Maddocks, K.J.; Duell, J.; González-Barca, E.; Jurczak, W.; Liberati, A.M.; de Vos, S.; Nagy, Z.; Obr, A.; Gaidano, G.; Abrisqueta, P.; et al. Long-Term Subgroup Analyses from L-Mind, a Phase II Study of Tafasitamab (MOR208) Combined with Lenalidomide in Patients with Relapsed or Refractory Diffuse Large B-Cell Lymphoma. Blood 2020, 136, 19–21. [Google Scholar] [CrossRef]
- Belada, D.; Nowakowski, G.S.; Bergua Burgues, J.M.; André, M.; Kopeckova, K.; Stevens, D.A.; Trněný, M.; Pérez Persona, E.; Pichler, P.; Klöpfer, P.; et al. A Phase Ib, Open-Label, Randomized Study to Assess Safety and Preliminary Efficacy of Tafasitamab (MOR208) or Tafasitamab + Lenalidomide in Addition to R-CHOP in Patients with Newly Diagnosed Diffuse Large B-Cell Lymphoma: Analysis of the Safety Run-in Phase. Blood 2020, 136, 27–28. [Google Scholar] [CrossRef]
- Smith, S.D.; Till, B.G.; Shadman, M.S.; Lynch, R.C.; Cowan, A.J.; Wu, Q.V.; Voutsinas, J.; Rasmussen, H.A.; Blue, K.; Ujjani, C.S.; et al. Pembrolizumab with R-CHOP in previously untreated diffuse large B-cell lymphoma: Potential for biomarker driven therapy. Br. J. Haematol. 2020, 189, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Younes, A.; Burke, J.M.; Cheson, B.D.; Diefenbach, C.; Ferrari, S.; Hahn, U.H.; Hawkes, E.A.; Khan, C.; Lossos, I.S.; Musuraca, G.; et al. Safety and Efficacy of Atezolizumab in Combination with Rituximab Plus CHOP in Previously Untreated Patients with Diffuse Large B-Cell Lymphoma (DLBCL): Updated Analysis of a Phase I/II Study. Blood 2019, 134, 2874. [Google Scholar] [CrossRef]
- Hawkes, E.A.; Chong, G.; Smith, C.; Lee, S.-T.; Churilov, L.; McKendrick, J.; Renwick, W.; Blombery, P.; Nelson, N.E.; Fancourt, T.; et al. Safety and Efficacy of Induction and Maintenance Avelumab Plus R-CHOP in Patients with Diffuse Large B-Cell Lymphoma (DLBCL): Analysis of the Phase II Avr-CHOP Study. Blood 2020, 136, 43–44. [Google Scholar] [CrossRef]
- Budde, L.E.; Halwani, A.; Yasenchak, C.A.; Farber, C.M.; Burke, J.M.; Fayad, L.E.; Holkova, B.; Knapp, M.; Kolibaba, K.S.; Advani, R.H.; et al. Results of an Ongoing Phase 2 Study of Brentuximab Vedotin with Rchp As Frontline Therapy in Patients with High-Intermediate/High-Risk Diffuse Large B Cell Lymphoma (DLBCL). Blood 2016, 128, 104. [Google Scholar] [CrossRef]
- Svoboda, J.; Bair, S.M.; Landsburg, D.J.; Nasta, S.D.; Nagle, S.J.; Barta, S.K.; Khan, N.; Filicko-O’Hara, J.; Gaballa, S.; Strelec, L.; et al. Brentuximab vedotin in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone as frontline treatment for patients with CD30-positive B-cell lymphomas. Haematologica 2020, 106, 1705–1713. [Google Scholar] [CrossRef]
- Reagan, P.M.; Portell, C.A.; Casulo, C.; Baran, A.M.; Magnuson, A.; Barr, P.M.; Lerman, Y.; French, K.N.; Friedberg, J.W. A Pilot Study of Brentuximab Vedotin, Rituximab and Dose Attenuated CHP in Patients 75 Years and Older with Diffuse Large B-Cell Lymphoma. Blood 2020, 136, 5–6. [Google Scholar] [CrossRef]
- Tilly, H.; Morschhauser, F.; Bartlett, N.L.; Mehta, A.; Salles, G.; Haioun, C.; Munoz, J.; Chen, A.I.; Kolibaba, K.; Lu, D.; et al. Polatuzumab vedotin in combination with immunochemotherapy in patients with previously untreated diffuse large B-cell lymphoma: An open-label, non-randomised, phase 1b–2 study. Lancet Oncol. 2019, 20, 998–1010. [Google Scholar] [CrossRef]
- Tilly, H.; Morschhauser, F.; Sehn, L.H.; Friedberg, J.W.; Trneny, M.; Sharman, J.P.; Herbaux, C.; Burke, J.M.; Matasar, M.; Rai, S.; et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2022, 386, 351–363. [Google Scholar] [CrossRef]
- Olszewski, A.J.; Avigdor, A.; Babu, S.; Levi, I.; Eradat, H.; Abadi, U.; Holmes, H.; McKinney, M.; Woszczyk, D.; Giannopoulos, K.; et al. Mosunetuzumab monotherapy in elderly/unfit pts with first-line diffuse large b-cell lymphoma (dlbcl): Safety and efficacy remain promising with durable complete responses. Hematol. Oncol. 2021, 39, 328–329. [Google Scholar] [CrossRef]
- Phillips, T.J.; Olszewski, A.J.; Munoz, J.; Kim, T.M.; Yoon, D.H.; Greil, R.; Westin, J.; Jaeger, U.; Canales, M.; Chen, C.; et al. Mosunetuzumab, a Novel CD20/CD3 Bispecific Antibody, in Combination with CHOP Confers High Response Rates in Patients with Diffuse Large B-Cell Lymphoma. Blood 2020, 136, 37–38. [Google Scholar] [CrossRef]
- Chen, R.; Zinzani, P.L.; Fanale, M.A.; Armand, P.; Johnson, N.A.; Brice, P.; Radford, J.; Ribrag, V.; Molin, D.; Vassilakopoulos, T.P.; et al. Phase II Study of the Efficacy and Safety of Pembrolizumab for Relapsed/Refractory Classic Hodgkin Lymphoma. J. Clin. Oncol. 2017, 35, 2125–2132. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Zinzani, P.L.; Lee, H.J.; Armand, P.; Johnson, N.A.; Brice, P.; Radford, J.; Ribrag, V.; Molin, D.; Vassilakopoulos, T.P.; et al. Pembrolizumab in relapsed or refractory Hodgkin lymphoma: 2-year follow-up of KEYNOTE-087. Blood 2019, 134, 1144–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassilakopoulos, T.P.; Chatzidimitriou, C.; Asimakopoulos, J.V.; Arapaki, M.; Tzoras, E.; Angelopoulou, M.K.; Konstantopoulos, K. Immunotherapy in Hodgkin Lymphoma: Present Status and Future Strategies. Cancers 2019, 11, 1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansell, S.M.; Bröckelmann, P.J.; von Keudell, G.; Lee, H.J.; Santoro, A.; Zinzani, P.L.; Collins, G.P.; Cohen, J.B.; De Boer, J.P.; Kuruvilla, J.; et al. Nivolumab for relapsed or refractory (r/r) classical hodgkin lymphoma (chl) after autologous transplantation: 5-year overall survival from the phase 2 checkmate 205 study. Hematol. Oncol. 2021, 39, 122–125. [Google Scholar] [CrossRef]
- Armand, P.; Zinzani, P.L.L.; Lee, H.J.; Johnson, N.; Brice, P.; Radford, J.; Ribrag, V.; Molin, D.; Vassilakopoulos, T.P.; Tomita, A.; et al. Five-Year Follow-up of Keynote-087: Pembrolizumab Monotherapy in Relapsed/Refractory Classical Hodgkin Lymphoma (R/R cHL). Blood 2021, 138, 1366. [Google Scholar] [CrossRef]
- Lesokhin, A.M.; Ansell, S.M.; Armand, P.; Scott, E.C.; Halwani, A.; Gutierrez, M.; Millenson, M.M.; Cohen, A.D.; Schuster, S.J.; Lebovic, D.; et al. Nivolumab in Patients With Relapsed or Refractory Hematologic Malignancy: Preliminary Results of a Phase Ib Study. J. Clin. Oncol. 2016, 34, 2698–2704. [Google Scholar] [CrossRef] [Green Version]
- Ansell, S.M.; Minnema, M.C.; Johnson, P.; Timmerman, J.M.; Armand, P.; Shipp, M.A.; Rodig, S.J.; Ligon, A.H.; Roemer, M.G.M.; Reddy, N.; et al. Nivolumab for Relapsed/Refractory Diffuse Large B-Cell Lymphoma in Patients Ineligible for or Having Failed Autologous Transplantation: A Single-Arm, Phase II Study. J. Clin. Oncol. 2019, 37, 481–489. [Google Scholar] [CrossRef]
- Smith, S.D.; Fromm, J.R.; Fang, M.; Till, B.G.; Shadman, M.; Lynch, R.C.; Cowan, A.J.; Wu, Q.V.; Voutsinas, J.; Rasmussen, H.A.; et al. Pembrolizumab with R-CHOP in Previously Untreated Diffuse Large B-Cell Lymphoma: Long Term Follow up and Analysis of the Mechanism of Pdl-1 Tumor Expression. Blood 2020, 136, 13–14. [Google Scholar] [CrossRef]
- Frigault, M.J.; Armand, P.; Redd, R.A.; Jeter, E.; Merryman, R.W.; Coleman, K.C.; Herrera, A.F.; Dahi, P.; Nieto, Y.; LaCasce, A.S.; et al. PD-1 blockade for diffuse large B-cell lymphoma after autologous stem cell transplantation. Blood Adv. 2020, 4, 122–126. [Google Scholar] [CrossRef]
- Armand, P.; Rodig, S.; Melnichenko, V.; Thieblemont, C.; Bouabdallah, K.; Tumyan, G.; Ozcan, M.; Portino, S.; Fogliatto, L.; Caballero, M.D.; et al. Pembrolizumab in Relapsed or Refractory Primary Mediastinal Large B-Cell Lymphoma. J. Clin. Oncol. 2019, 37, 3291–3299. [Google Scholar] [CrossRef]
- Kim, D.; Wang, J.; Willingham, S.B.; Martin, R.; Wernig, G.; Weissman, I.L. Anti-CD47 antibodies promote phagocytosis and inhibit the growth of human myeloma cells. Leukemia 2012, 26, 2538–2545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Advani, R.; Flinn, I.; Popplewell, L.; Forero, A.; Bartlett, N.L.; Ghosh, N.; Kline, J.; Roschewski, M.; LaCasce, A.; Collins, G.P.; et al. CD47 Blockade by Hu5F9-G4 and Rituximab in Non-Hodgkin’s Lymphoma. N. Engl. J. Med. 2018, 379, 1711–1721. [Google Scholar] [CrossRef] [PubMed]
- Dimou, M.; Bitsani, A.; Bethge, W.; Panayiotidis, P.; Vassilakopoulos, T.P. Pembrolizumab-induced Remission after Failure of Axicabtagene Ciloleucel: Case Report and Literature Review. In Vivo 2021, 35, 3401–3406. [Google Scholar] [CrossRef] [PubMed]
- Zinzani, P.L.; Tani, M.; Fanti, S.; Stefoni, V.; Musuraca, G.; Castellucci, P.; Marchi, E.; Farsad, M.; Fina, M.; Pellegrini, C.; et al. A phase II trial of CHOP chemotherapy followed by yttrium 90 ibritumomab tiuxetan (Zevalin) for previously untreated elderly diffuse large B-cell lymphoma patients. Ann. Oncol. 2008, 19, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Zinzani, P.L.; Rossi, G.; Franceschetti, S.; Botto, B.; Di Rocco, A.; Cabras, M.G.; Petti, M.C.; Stefoni, V.; Broccoli, A.; Fanti, S.; et al. Phase II trial of short-course R-CHOP followed by 90Y-ibritumomab tiuxetan in previously untreated high-risk elderly diffuse large B-cell lymphoma patients. Clin. Cancer Res. 2010, 16, 3998–4004. [Google Scholar] [CrossRef] [Green Version]
- Karmali, R.; Larson, M.L.; Shammo, J.M.; Gregory, S.A.; O’Brien, T.; Venugopal, P. Phase 2 study of CHOP-R-14 followed by (90)Y-ibritumomab tiuxetan in patients with previously untreated diffuse large B-cell lymphoma. Mol. Clin. Oncol. 2017, 6, 627–633. [Google Scholar] [CrossRef]
- Friedberg, J.W.; Unger, J.M.; Burack, W.R.; Gopal, A.K.; Raju, R.N.; Nademanee, A.P.; Kaminski, M.S.; Li, H.; Press, O.W.; Miller, T.P.; et al. R-CHOP with iodine-131 tositumomab consolidation for advanced stage diffuse large B-cell lymphoma (DLBCL): SWOG S0433. Br. J. Haematol. 2014, 166, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Kraeber-Bodere, F.; Pallardy, A.; Maisonneuve, H.; Campion, L.; Moreau, A.; Soubeyran, I.; Le Gouill, S.; Tournilhac, O.; Daguindau, E.; Jardel, H.; et al. Consolidation anti-CD22 fractionated radioimmunotherapy with (90)Y-epratuzumab tetraxetan following R-CHOP in elderly patients with diffuse large B-cell lymphoma: A prospective, single group, phase 2 trial. Lancet. Haematol. 2017, 4, e35–e45. [Google Scholar] [CrossRef]
- Nejadmoghaddam, M.-R.; Minai-Tehrani, A.; Ghahremanzadeh, R.; Mahmoudi, M.; Dinarvand, R.; Zarnani, A.-H. Antibody-Drug Conjugates: Possibilities and Challenges. Avicenna J. Med. Biotechnol. 2019, 11, 3–23. [Google Scholar]
- Hu, S.; Xu-Monette, Z.Y.; Balasubramanyam, A.; Manyam, G.C.; Visco, C.; Tzankov, A.; Liu, W.-m.; Miranda, R.N.; Zhang, L.; Montes-Moreno, S.; et al. CD30 expression defines a novel subgroup of diffuse large B-cell lymphoma with favorable prognosis and distinct gene expression signature: A report from the International DLBCL Rituximab-CHOP Consortium Program Study. Blood 2013, 121, 2715–2724. [Google Scholar] [CrossRef]
- Jacobsen, E.D.; Sharman, J.P.; Oki, Y.; Advani, R.H.; Winter, J.N.; Bello, C.M.; Spitzer, G.; Palanca-Wessels, M.C.; Kennedy, D.A.; Levine, P.; et al. Brentuximab vedotin demonstrates objective responses in a phase 2 study of relapsed/refractory DLBCL with variable CD30 expression. Blood 2015, 125, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, N.L.; Smith, M.R.; Siddiqi, T.; Advani, R.H.; O’Connor, O.A.; Sharman, J.P.; Feldman, T.; Savage, K.J.; Shustov, A.R.; Diefenbach, C.S.; et al. Brentuximab vedotin activity in diffuse large B-cell lymphoma with CD30 undetectable by visual assessment of conventional immunohistochemistry. Leuk. Lymphoma 2017, 58, 1607–1616. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Yoon, D.H.; Kim, J.S.; Kang, H.J.; Lee, H.W.; Eom, H.-S.; Hong, J.Y.; Cho, J.; Ko, Y.H.; Huh, J.; et al. Efficacy of Brentuximab Vedotin in Relapsed or Refractory High-CD30–Expressing Non-Hodgkin Lymphomas: Results of a Multicenter, Open-Labeled Phase II Trial. J. Korean Cancer Assoc. 2020, 52, 374–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinzani, P.L.; Pellegrini, C.; Chiappella, A.; Di Rocco, A.; Salvi, F.; Cabras, M.G.; Argnani, L.; Stefoni, V. Brentuximab vedotin in relapsed primary mediastinal large B-cell lymphoma: Results from a phase 2 clinical trial. Blood 2017, 129, 2328–2330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, J.; Berrien-Elliott, M.M.; Gomez, F.; Luo, J.; Becker-Hapak, M.; Cashen, A.F.; Wagner-Johnston, N.D.; Maddocks, K.; Mosior, M.; Foster, M.; et al. Phase I/Dose Expansion Trial of Brentuximab vedotin/Lenalidomide in Relapsed or Refractory Diffuse Large B-cell Lymphoma. Blood 2021, 139, 1999–2010. [Google Scholar] [CrossRef] [PubMed]
- Zinzani, P.L.; Santoro, A.; Gritti, G.; Brice, P.; Barr, P.M.; Kuruvilla, J.; Cunningham, D.; Kline, J.; Johnson, N.A.; Mehta-Shah, N.; et al. Nivolumab Combined With Brentuximab Vedotin for Relapsed/Refractory Primary Mediastinal Large B-Cell Lymphoma: Efficacy and Safety From the Phase II CheckMate 436 Study. J. Clin. Oncol. 2019, 37, 3081–3089. [Google Scholar] [CrossRef] [PubMed]
- Zinzani, P.L.; Santoro, A.; Gritti, G.; Brice, P.; Barr, P.M.; Kuruvilla, J.; Cunningham, D.; Kline, J.; Johnson, N.A.; Mehta-Shah, N.; et al. Nivolumab plus brentuximab vedotin for relapsed/refractory primary mediastinal large b-cell lymphoma: Extended follow-up from the phase 2 checkmate 436 study. Hematol. Oncol. 2021, 39, 93–95. [Google Scholar] [CrossRef]
- Advani, A.; Coiffier, B.; Czuczman, M.S.; Dreyling, M.; Foran, J.; Gine, E.; Gisselbrecht, C.; Ketterer, N.; Nasta, S.; Rohatiner, A.; et al. Safety, Pharmacokinetics, and Preliminary Clinical Activity of Inotuzumab Ozogamicin, a Novel Immunoconjugate for the Treatment of B-Cell Non-Hodgkin’s Lymphoma: Results of a Phase I Study. J. Clin. Oncol. 2010, 28, 2085–2093. [Google Scholar] [CrossRef]
- Fayad, L.; Offner, F.; Smith, M.R.; Verhoef, G.; Johnson, P.; Kaufman, J.L.; Rohatiner, A.; Advani, A.; Foran, J.; Hess, G.; et al. Safety and clinical activity of a combination therapy comprising two antibody-based targeting agents for the treatment of non-Hodgkin lymphoma: Results of a phase I/II study evaluating the immunoconjugate inotuzumab ozogamicin with rituximab. J. Clin. Oncol. 2013, 31, 573–583. [Google Scholar] [CrossRef]
- Wagner-Johnston, N.D.; Goy, A.; Rodriguez, M.A.; Ehmann, W.C.; Hamlin, P.A.; Radford, J.; Thieblemont, C.; Suh, C.; Sweetenham, J.; Huang, Y.; et al. A phase 2 study of inotuzumab ozogamicin and rituximab, followed by autologous stem cell transplant in patients with relapsed/refractory diffuse large B-cell lymphoma. Leuk. Lymphoma 2015, 56, 2863–2869. [Google Scholar] [CrossRef]
- Dang, N.H.; Ogura, M.; Castaigne, S.; Fayad, L.E.; Jerkeman, M.; Radford, J.; Pezzutto, A.; Bondarenko, I.; Stewart, D.A.; Shnaidman, M.; et al. Randomized, phase 3 trial of inotuzumab ozogamicin plus rituximab versus chemotherapy plus rituximab for relapsed/refractory aggressive B-cell non-Hodgkin lymphoma. Br. J. Haematol. 2018, 182, 583–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogura, M.; Tobinai, K.; Hatake, K.; Davies, A.; Crump, M.; Ananthakrishnan, R.; Ishibashi, T.; Paccagnella, M.L.; Boni, J.; Vandendries, E.; et al. Phase I Study of Inotuzumab Ozogamicin Combined with R-CVP for Relapsed/Refractory CD22+ B-cell Non-Hodgkin Lymphoma. Clin. Cancer Res. 2016, 22, 4807–4816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangha, R.; Davies, A.; Dang, N.H.; Ogura, M.; MacDonald, D.A.; Ananthakrishnan, R.; Paccagnella, M.L.; Vandendries, E.; Boni, J.; Goh, Y.T. Phase 1 study of inotuzumab ozogamicin combined with R-GDP for the treatment of patients with relapsed/refractory CD22+ B-cell non-Hodgkin lymphoma. J. Drug Assess. 2017, 6, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Palanca-Wessels, M.C.A.; Czuczman, M.; Salles, G.; Assouline, S.; Sehn, L.H.; Flinn, I.; Patel, M.R.; Sangha, R.; Hagenbeek, A.; Advani, R.; et al. Safety and activity of the anti-CD79B antibody–drug conjugate polatuzumab vedotin in relapsed or refractory B-cell non-Hodgkin lymphoma and chronic lymphocytic leukaemia: A phase 1 study. Lancet Oncol. 2015, 16, 704–715. [Google Scholar] [CrossRef]
- Morschhauser, F.; Flinn, I.W.; Advani, R.; Sehn, L.H.; Diefenbach, C.; Kolibaba, K.; Press, O.W.; Salles, G.; Tilly, H.; Chen, A.I.; et al. Polatuzumab vedotin or pinatuzumab vedotin plus rituximab in patients with relapsed or refractory non-Hodgkin lymphoma: Final results from a phase 2 randomised study (ROMULUS). Lancet Haematol. 2019, 6, e254–e265. [Google Scholar] [CrossRef]
- Phillips, T.; Brunvand, M.; Chen, A.; Press, O.; Essell, J.; Chiappella, A.; Diefenbach, C.; Jones, S.; Hirata, J.; Flinn, I.W. Polatuzumab Vedotin Combined with Obinutuzumab for Patients with Relapsed or Refractory Non-Hodgkin Lymphoma: Preliminary Safety and Clinical Activity of a Phase Ib/II Study. Blood 2016, 128, 622. [Google Scholar] [CrossRef]
- Sehn, L.H.; Hertzberg, M.; Opat, S.; Herrera, A.F.; Assouline, S.E.; Flowers, C.; Kim, T.M.; McMillan, A.; Ozcan, M.; Safar, V.; et al. Polatuzumab Vedotin Plus Bendamustine and Rituximab in Relapsed/Refractory Diffuse Large B-Cell Lymphoma: Updated Results of a Phase Ib/II Randomized Study and Preliminary Results of a Single-Arm Extension. Blood 2020, 136, 17–19. [Google Scholar] [CrossRef]
- Sehn, L.H.; Hertzberg, M.; Opat, S.S.; Herrera, A.F.; Assouline, S.; Flowers, C.R.; Kim, T.M.; McMillan, A.K.; Özcan, M.; Safar, V.; et al. Polatuzumab vedotin plus bendamustine and rituximab in relapsed/refractory DLBCL: Survival update and new extension cohort. Blood Adv. 2022, 6, 533–543. [Google Scholar] [CrossRef]
- Hamadani, M.; Radford, J.; Carlo-Stella, C.; Caimi, P.F.; Reid, E.G.; O’Connor, O.A.; Feingold, J.; Ardeshna, K.M.; Townsend, W.M.; Solh, M.; et al. Final Results of a Phase 1 Study of Loncastuximab Tesirine in Relapsed/Refractory B-Cell Non-Hodgkin Lymphoma. Blood 2021, 137, 2634–2645. [Google Scholar] [CrossRef]
- Caimi, P.F.; Ai, W.; Alderuccio, J.P.; Ardeshna, K.M.; Hamadani, M.; Hess, B.; Kahl, B.S.; Radford, J.; Solh, M.; Stathis, A.; et al. Loncastuximab tesirine in relapsed or refractory diffuse large B-cell lymphoma (LOTIS-2): A multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2021, 22, 790–800. [Google Scholar] [CrossRef]
- Vassilakopoulos, T.P.; Michail, M.; Papageorgiou, S.; Kourti, G.; Angelopoulou, M.K.; Panitsas, F.; Sachanas, S.; Kalpadakis, C.; Katodritou, E.; Leonidopoulou, T.; et al. Identification of Very Low-Risk Subgroups of Patients with Primary Mediastinal Large B-Cell Lymphoma Treated with R-CHOP. Oncologist 2021, 26, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Zhang, M.; Wu, K.; Zhu, J.; He, Z.; Li, J.; Chen, C.; Qiu, K.; Yu, X.; Wu, J. Risk of adverse events in lymphoma patients treated with brentuximab vedotin: A systematic review and meta-analysis. Expert Opin. Drug Saf. 2020, 19, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Wynne, J.; Wright, D.; Stock, W. Inotuzumab: From preclinical development to success in B-cell acute lymphoblastic leukemia. Blood Adv. 2019, 3, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Lamb, Y.N. Inotuzumab Ozogamicin: First Global Approval. Drugs 2017, 77, 1603–1610. [Google Scholar] [CrossRef]
- Kebriaei, P.; Cutler, C.; de Lima, M.; Giralt, S.; Lee, S.J.; Marks, D.; Merchant, A.; Stock, W.; van Besien, K.; Stelljes, M. Management of important adverse events associated with inotuzumab ozogamicin: Expert panel review. Bone Marrow Transplant. 2018, 53, 449–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sehn, L.H.; Herrera, A.F.; Flowers, C.R.; Kamdar, M.K.; McMillan, A.; Hertzberg, M.; Assouline, S.; Kim, T.M.; Kim, W.S.; Ozcan, M.; et al. Polatuzumab Vedotin in Relapsed or Refractory Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. 2020, 38, 155–165. [Google Scholar] [CrossRef]
- Liebers, N.; Duell, J.; Fitzgerald, D.; Kerkhoff, A.; Noerenberg, D.; Kaebisch, E.; Acker, F.; Fuhrmann, S.; Leng, C.; Welslau, M.; et al. Polatuzumab vedotin as a salvage and bridging treatment in relapsed or refractory large B-cell lymphomas. Blood Adv. 2021, 5, 2707–2716. [Google Scholar] [CrossRef]
- Gouni, S.; Rosenthal, A.C.; Crombie, J.L.; Ip, A.; Kamdar, M.; Hess, B.T.; Feng, L.; Watson, G.; Ayers, A.; Neelapu, S.S.; et al. A Multi-Center Retrospective Study of Polatuzumab for Patients with Large B-Cell Lymphoma Relapsed after Standard of Care CAR T-Cell Therapy. Blood 2021, 138, 2495. [Google Scholar] [CrossRef]
- Dimou, M.; Papageorgiou, S.; Stavroyianni, N. Real-life experience with the combination of polatuzumab vedotin, rituximab and bendamustine in aggressive b-cell lymphomas. Hematol. Oncol. 2021, 39, 336–348. [Google Scholar] [CrossRef]
- Segman, Y.; Ribakovsky, E.; Avigdor, A.; Goldhecht, Y.; Vainstein, V.; Goldschmidt, N.; Harlev, S.; Horwitz, N.; Gutwein, O.; Gurion, R.; et al. Outcome of relapsed/refractory diffuse large B-cell lymphoma patients treated with polatuzumab vedotin-based therapy: Real-life experience. Leuk. Lymphoma 2021, 62, 118–124. [Google Scholar] [CrossRef]
- Smith, S.D.; Lopedote, P.; Samara, Y.; Mei, M.; Herrera, A.F.; Winter, A.M.; Hill, B.T.; Shadman, M.; Ujjani, C.; Lynch, R.C.; et al. Polatuzumab Vedotin for Relapsed/Refractory Aggressive B-cell Lymphoma: A Multicenter Post-marketing Analysis. Clin. Lymphoma Myeloma Leuk. 2020, 21, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Northend, M.; Wilson, W.; Osborne, W.; Fox, C.P.; Davies, A.J.; El-Sharkawi, D.; Phillips, E.H.; Sim, H.W.; Sadullah, S.; Shah, N.; et al. Polatuzumab vedotin with bendamustine and rituximab for relapsed/refractory high-grade b-cell lymphoma: The uk experience. Hematol. Oncol. 2021, 39, 248–249. [Google Scholar] [CrossRef]
- Vodicka, P.; Benesova, K.; Janikova, A.; Prochazka, V.; Belada, D.; Mocikova, H.; Steinerova, K.; Duras, J.; Karban, J.; Hanackova, V.; et al. Polatuzumab vedotin plus bendamustine and rituximab in patients with relapsed/refractory diffuse large b-cell lymphoma in the real world. Hematol. Oncol. 2021, 39, 419–420. [Google Scholar] [CrossRef]
- Thapa, B.; Caimi, P.F.; Ardeshna, K.M.; Solh, M.; Carlo-Stella, C.; Kahl, B.S.; Hamadani, M. CD19 antibody-drug conjugate therapy in DLBCL does not preclude subsequent responses to CD19-directed CAR T-cell therapy. Blood Adv. 2020, 4, 3850–3852. [Google Scholar] [CrossRef]
- Moskowitz, C.H.; Fanale, M.A.; Shah, B.D.; Advani, R.H.; Chen, R.; Kim, S.; Kostic, A.; Liu, T.; Peng, J.; Forero-Torres, A. A Phase 1 Study of Denintuzumab Mafodotin (SGN-CD19A) in Relapsed/Refactory B-Lineage Non-Hodgkin Lymphoma. Blood 2015, 126, 182. [Google Scholar] [CrossRef]
- Trnĕný, M.; Verhoef, G.; Dyer, M.J.; Ben Yehuda, D.; Patti, C.; Canales, M.; Lopez, A.; Awan, F.T.; Montgomery, P.G.; Janikova, A.; et al. A phase II multicenter study of the anti-CD19 antibody drug conjugate coltuximab ravtansine (SAR3419) in patients with relapsed or refractory diffuse large B-cell lymphoma previously treated with rituximab-based immunotherapy. Haematologica 2018, 103, 1351–1358. [Google Scholar] [CrossRef]
- Coiffier, B.; Thieblemont, C.; de Guibert, S.; Dupuis, J.; Ribrag, V.; Bouabdallah, R.; Morschhauser, F.; Navarro, R.; Le Gouill, S.; Haioun, C.; et al. A phase II, single-arm, multicentre study of coltuximab ravtansine (SAR3419) and rituximab in patients with relapsed or refractory diffuse large B-cell lymphoma. Br. J. Haematol. 2016, 173, 722–730. [Google Scholar] [CrossRef] [Green Version]
- Advani, R.H.; Lebovic, D.; Chen, A.; Brunvand, M.; Goy, A.; Chang, J.E.; Hochberg, E.; Yalamanchili, S.; Kahn, R.; Lu, D.; et al. Phase I Study of the Anti-CD22 Antibody-Drug Conjugate Pinatuzumab Vedotin with/without Rituximab in Patients with Relapsed/Refractory B-cell Non-Hodgkin Lymphoma. Clin. Cancer Res. 2017, 23, 1167–1176. [Google Scholar] [CrossRef] [Green Version]
- Hamadani, M.; Collins, G.P.; Caimi, P.F.; Samaniego, F.; Spira, A.; Davies, A.; Radford, J.; Menne, T.; Karnad, A.; Zain, J.M.; et al. Camidanlumab tesirine in patients with relapsed or refractory lymphoma: A phase 1, open-label, multicentre, dose-escalation, dose-expansion study. Lancet. Haematol. 2021, 8, e433–e445. [Google Scholar] [CrossRef]
- Stathis, A.; Flinn, I.W.; Madan, S.; Maddocks, K.; Freedman, A.; Weitman, S.; Zucca, E.; Munteanu, M.C.; Lia Palomba, M. Safety, tolerability, and preliminary activity of IMGN529, a CD37-targeted antibody-drug conjugate, in patients with relapsed or refractory B-cell non-Hodgkin lymphoma: A dose-escalation, phase I study. Investig. New Drugs 2018, 36, 869–876. [Google Scholar] [CrossRef] [Green Version]
- Hicks, S.W.; Lai, K.C.; Gavrilescu, L.C.; Yi, Y.; Sikka, S.; Shah, P.; Kelly, M.E.; Lee, J.; Lanieri, L.; Ponte, J.F.; et al. The Antitumor Activity of IMGN529, a CD37-Targeting Antibody-Drug Conjugate, Is Potentiated by Rituximab in Non-Hodgkin Lymphoma Models. Neoplasia 2017, 19, 661–671. [Google Scholar] [CrossRef]
- Levy, M.Y.; Jagadeesh, D.; Grudeva-Popova, Z.; Trněný, M.; Jurczak, W.; Pylypenko, H.; André, M.; Dwivedy Nasta, S.; Rechavi-Robinson, D.; Toffanin, S.; et al. Safety and Efficacy of CD37-Targeting Naratuximab Emtansine PLUS Rituximab in Diffuse Large B-Cell Lymphoma and Other NON-Hodgkin’S B-Cell Lymphomas—A Phase 2 Study. Blood 2021, 138, 526. [Google Scholar] [CrossRef]
- Sawas, A.; Savage, K.J.; Perez, R.P.; Advani, R.H.; Zaine, J.M.; Lackey, J.M.; Trave, F.; Anand, B.; Chu, R.; Reyno, L.M.; et al. A phase 1 study of the anti-cd37 antibody-drug conjugate ags67e in advanced lymphoid malignancies. Interim results. Hematol. Oncol. 2017, 35, 49. [Google Scholar] [CrossRef] [Green Version]
- Phillips, T.; Barr, P.M.; Park, S.I.; Kolibaba, K.; Caimi, P.F.; Chhabra, S.; Kingsley, E.C.; Boyd, T.; Chen, R.; Carret, A.-S.; et al. A phase 1 trial of SGN-CD70A in patients with CD70-positive diffuse large B cell lymphoma and mantle cell lymphoma. Investig. New Drugs 2019, 37, 297–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tannir, N.M.; Forero-Torres, A.; Ramchandren, R.; Pal, S.K.; Ansell, S.M.; Infante, J.R.; de Vos, S.; Hamlin, P.A.; Kim, S.K.; Whiting, N.C.; et al. Phase I dose-escalation study of SGN-75 in patients with CD70-positive relapsed/refractory non-Hodgkin lymphoma or metastatic renal cell carcinoma. Investig. New Drugs 2014, 32, 1246–1257. [Google Scholar] [CrossRef]
- Owonikoko, T.K.; Hussain, A.; Stadler, W.M.; Smith, D.C.; Kluger, H.; Molina, A.M.; Gulati, P.; Shah, A.; Ahlers, C.M.; Cardarelli, P.M.; et al. First-in-human multicenter phase I study of BMS-936561 (MDX-1203), an antibody-drug conjugate targeting CD70. Cancer Chemother. Pharmacol. 2016, 77, 155–162. [Google Scholar] [CrossRef]
- Herrera, A.F.; Patel, M.R.; Burke, J.M.; Advani, R.; Cheson, B.D.; Sharman, J.P.; Penuel, E.; Polson, A.G.; Liao, C.D.; Li, C.; et al. Anti-CD79B Antibody-Drug Conjugate DCDS0780A in Patients with B-Cell Non-Hodgkin Lymphoma: Phase 1 Dose-Escalation Study. Clin. Cancer Res. 2022, 28, 1294–1301. [Google Scholar] [CrossRef]
- Wang, M.; Mei, M.; Barr, P.M.; Barrientos, J.; de Vos, S.; Furman, R.; Patel, K.; Thompson, P.A.; Choi, M.; Kallam, A.; et al. Phase 1 Dose Escalation and Cohort Expansion Study of the Anti-ROR1 Antibody-Drug Conjugate Zilovertamab Vedotin (MK-2140) for the Treatment of Non-Hodgkin Lymphoma. Blood 2021, 138, 528. [Google Scholar] [CrossRef]
- Kontermann, R.E.; Brinkmann, U. Bispecific antibodies. Drug Discov. Today 2015, 20, 838–847. [Google Scholar] [CrossRef] [Green Version]
- Brinkmann, U.; Kontermann, R.E. The making of bispecific antibodies. MAbs 2017, 9, 182–212. [Google Scholar] [CrossRef]
- Labrijn, A.F.; Meesters, J.I.; Priem, P.; de Jong, R.N.; van den Bremer, E.T.; van Kampen, M.D.; Gerritsen, A.F.; Schuurman, J.; Parren, P.W. Controlled Fab-arm exchange for the generation of stable bispecific IgG1. Nat. Protoc. 2014, 9, 2450–2463. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.A.; Goldenberg, D.M.; Cardillo, T.M.; McBride, W.J.; Sharkey, R.M.; Chang, C.H. Stably tethered multifunctional structures of defined composition made by the dock and lock method for use in cancer targeting. Proc. Natl. Acad. Sci. USA 2006, 103, 6841–6846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchings, M.; Morschhauser, F.; Iacoboni, G.; Carlo-Stella, C.; Offner, F.C.; Sureda, A.; Salles, G.; Martínez-Lopez, J.; Crump, M.; Thomas, D.N.; et al. Glofitamab, a Novel, Bivalent CD20-Targeting T-Cell-Engaging Bispecific Antibody, Induces Durable Complete Remissions in Relapsed or Refractory B-Cell Lymphoma: A Phase I Trial. J. Clin. Oncol. 2021, 39, 1959–1970. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, M.; Mous, R.; Clausen, M.R.; Johnson, P.; Linton, K.M.; Chamuleau, M.E.D.; Lewis, D.J.; Sureda Balari, A.; Cunningham, D.; Oliveri, R.S.; et al. Dose escalation of subcutaneous epcoritamab in patients with relapsed or refractory B-cell non-Hodgkin lymphoma: An open-label, phase 1/2 study. Lancet 2021, 398, 1157–1169. [Google Scholar] [CrossRef]
- Bannerji, R.; Allan, J.N.; Arnason, J.E.; Brown, J.R.; Advani, R.; Ansell, S.M.; O’Brien, S.M.; Duell, J.; Martin, P.; Joyce, R.M.; et al. Odronextamab (REGN1979), a Human CD20 x CD3 Bispecific Antibody, Induces Durable, Complete Responses in Patients with Highly Refractory B-Cell Non-Hodgkin Lymphoma, Including Patients Refractory to CAR T Therapy. Blood 2020, 136, 42–43. [Google Scholar] [CrossRef]
- Budde, L.E.; Assouline, S.; Sehn, L.H.; Schuster, S.J.; Yoon, S.S.; Yoon, D.H.; Matasar, M.J.; Bosch, F.; Kim, W.S.; Nastoupil, L.J.; et al. Single-Agent Mosunetuzumab Shows Durable Complete Responses in Patients With Relapsed or Refractory B-Cell Lymphomas: Phase I Dose-Escalation Study. J. Clin. Oncol. 2021, 40, 481–491. [Google Scholar] [CrossRef]
- Patel, K.; Michot, J.-M.; Chanan-Khan, A.; Ghesquieres, H.; Bouabdallah, K.; Byrd, J.C.; Cartron, G.; Portell, C.A.; Solh, M.; Tilly, H.; et al. Safety and Anti-Tumor Activity of Plamotamab (XmAb13676), an Anti-CD20 x Anti-CD3 Bispecific Antibody, in Subjects with Relapsed/Refractory Non-Hodgkin’s Lymphoma. Blood 2021, 138, 2494. [Google Scholar] [CrossRef]
- Goebeler, M.E.; Knop, S.; Viardot, A.; Kufer, P.; Topp, M.S.; Einsele, H.; Noppeney, R.; Hess, G.; Kallert, S.; Mackensen, A.; et al. Bispecific T-Cell Engager (BiTE) Antibody Construct Blinatumomab for the Treatment of Patients With Relapsed/Refractory Non-Hodgkin Lymphoma: Final Results From a Phase I Study. J. Clin. Oncol. 2016, 34, 1104–1111. [Google Scholar] [CrossRef]
- Viardot, A.; Goebeler, M.E.; Hess, G.; Neumann, S.; Pfreundschuh, M.; Adrian, N.; Zettl, F.; Libicher, M.; Sayehli, C.; Stieglmaier, J.; et al. Phase 2 study of the bispecific T-cell engager (BiTE) antibody blinatumomab in relapsed/refractory diffuse large B-cell lymphoma. Blood 2016, 127, 1410–1416. [Google Scholar] [CrossRef]
- Coyle, L.; Morley, N.J.; Rambaldi, A.; Mason, K.D.; Verhoef, G.; Furness, C.; Zhang, A.; Jung, A.S.; Franklin, J.L. Open-Label, Phase 2 Study of Blinatumomab as Second Salvage Therapy in Adults with Relapsed/Refractory Aggressive B-Cell Non-Hodgkin Lymphoma. Blood 2018, 132, 2103–2112. [Google Scholar] [CrossRef]
- Schuster, S.J.; Bartlett, N.L.; Assouline, S.; Yoon, S.-S.; Bosch, F.; Sehn, L.H.; Cheah, C.Y.; Shadman, M.; Gregory, G.P.; Ku, M.; et al. Mosunetuzumab Induces Complete Remissions in Poor Prognosis Non-Hodgkin Lymphoma Patients, Including Those Who Are Resistant to or Relapsing After Chimeric Antigen Receptor T-Cell (CAR-T) Therapies, and Is Active in Treatment through Multiple Lines. Blood 2019, 134, 6. [Google Scholar] [CrossRef]
- Bartlett, N.L.; Giri, P.; Budde, L.E.; Schuster, S.J.; Assouline, S.; Matasar, M.J.; Yoon, S.-S.; Canales, M.; Gutierrez, N.C.; Fay, K.; et al. Subcutaneous (SC) Administration of Mosunetuzumab with Cycle 1 Step-up Dosing Is Tolerable and Active in Patients with Relapsed/Refractory B-Cell Non-Hodgkin Lymphomas (R/R B-NHL): Initial Results from a Phase I/II Study. Blood 2021, 138, 3573. [Google Scholar] [CrossRef]
- Brouwer-Visser, J.; Fiaschi, N.; Deering, R.P.; Dhanik, A.; Cygan, K.J.; Zhang, W.; Jeong, S.; Pourpe, S.; Boucher, L.; Hamon, S.; et al. Baseline Biomarkers of T-Cell Function Correlate with Clinical Responses to Odronextamab (REGN1979), and Loss of CD20 Target Antigen Expression Identified As a Mechanism of Treatment Resistance. Blood 2020, 136, 10–11. [Google Scholar] [CrossRef]
- Popplewell, L.; Verhoef, G.; Kuruvilla, J.; Tuglus, C.; Kischel, R.; Stieglmaier, J.; Ghobadi, A. A first-in-human study of a half-life extended cd19-targeting bite in relapsed/refractory diffuse large b cell lymphoma, mantle cell lymphoma or follicular lymphoma. Hematol. Oncol. 2019, 37, 566–567. [Google Scholar] [CrossRef]
- CUI, Y.; Huang, Z.; Zhang, X.; Shen, W.; Chen, H.; Wen, Z.; Qi, B.; Luo, L.; Tan, Y.; Wu, Y.; et al. CD3-Activating Bi-Specific Antibody Targeting CD19 on B Cells in Mono- and Bi-Valent Format. Blood 2018, 132, 4169. [Google Scholar] [CrossRef]
- Reusch, U.; Duell, J.; Ellwanger, K.; Herbrecht, C.; Knackmuss, S.H.; Fucek, I.; Eser, M.; McAleese, F.; Molkenthin, V.; Gall, F.L.; et al. A tetravalent bispecific TandAb (CD19/CD3), AFM11, efficiently recruits T cells for the potent lysis of CD19(+) tumor cells. MAbs 2015, 7, 584–604. [Google Scholar] [CrossRef] [Green Version]
- Izhak, L.; Cullen, D.E.; Elgawly, M.; Luistro, L.; Johnson, S.; Bald, J.; Sasser, A.K.; Balasubramanian, S. Abstract 3636: Potent antitumor activity of duvortuxizumab, a CD19 x CD3 DART® molecule, in lymphoma models. Cancer Res. 2017, 77, 3636. [Google Scholar] [CrossRef] [Green Version]
- Buatois, V.; Johnson, Z.; Salgado-Pires, S.; Papaioannou, A.; Hatterer, E.; Chauchet, X.; Richard, F.; Barba, L.; Daubeuf, B.; Cons, L.; et al. Preclinical Development of a Bispecific Antibody that Safely and Effectively Targets CD19 and CD47 for the Treatment of B-Cell Lymphoma and Leukemia. Mol. Cancer Ther. 2018, 17, 1739–1751. [Google Scholar] [CrossRef] [Green Version]
- van Bommel, P.E.; He, Y.; Schepel, I.; Hendriks, M.A.J.M.; Wiersma, V.R.; van Ginkel, R.J.; van Meerten, T.; Ammatuna, E.; Huls, G.; Samplonius, D.F.; et al. CD20-selective inhibition of CD47-SIRPα "don’t eat me" signaling with a bispecific antibody-derivative enhances the anticancer activity of daratumumab, alemtuzumab and obinutuzumab. Oncoimmunology 2017, 7, e1386361. [Google Scholar] [CrossRef] [Green Version]
- Vallera, D.A.; Chen, H.; Sicheneder, A.R.; Panoskaltsis-Mortari, A.; Taras, E.P. Genetic alteration of a bispecific ligand-directed toxin targeting human CD19 and CD22 receptors resulting in improved efficacy against systemic B cell malignancy. Leuk. Res. 2009, 33, 1233–1242. [Google Scholar] [CrossRef] [Green Version]
- Bachanova, V.; Cao, Q.; Weisdorf, D.J.; Curtsinger, J.M.; Cooley, S.A.; Miller, J.; Vallera, D. Bispecific ligand-directed toxin targeting CD22 and CD19 (DT2219) for refractory B-cell malignancies: Results of phase I-II trial. J. Clin. Oncol. 2019, 37, e19066. [Google Scholar] [CrossRef]
- Parker, K.R.; Migliorini, D.; Perkey, E.; Yost, K.E.; Bhaduri, A.; Bagga, P.; Haris, M.; Wilson, N.E.; Liu, F.; Gabunia, K.; et al. Single-Cell Analyses Identify Brain Mural Cells Expressing CD19 as Potential Off-Tumor Targets for CAR-T Immunotherapies. Cell 2020, 183, 126–142.e117. [Google Scholar] [CrossRef] [PubMed]
- Shadman, M.; Yeung, C.; Redman, M.; Lee, S.Y.; Lee, D.H.; Ra, S.; Ujjani, C.S.; Dezube, B.J.; Poh, C.; Warren, E.H.; et al. Safety and Efficacy of Third Generation CD20 Targeted CAR-T (MB-106) for Treatment of Relapsed/Refractory B-NHL and CLL. Blood 2021, 138, 3872. [Google Scholar] [CrossRef]
- Liang, A.; Ye, S.; Li, P.; Huang, J.; Zhu, S.; Yao, X.; Zhou, L.; Xu, Y.; Zhu, J.; Zheng, C.; et al. Safety and efficacy of a novel anti-CD20 chimeric antigen receptor (CAR)-T cell therapy in relapsed/refractory (r/r) B-cell non-Hodgkin lymphoma (B-NHL) patients after failing CD19 CAR-T therapy. J. Clin. Oncol. 2021, 39, 2508. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Name of Antibody | Target | Approved for Newly Diagnosed DLBCL | Approved for R/R DLBCL | Commercially Available (Off-Label for DLBCL) | Investigational |
|---|---|---|---|---|---|
| Naked Antibodies | |||||
| Rituximab | CD20 | √ | |||
| Ofatumumab | √ | ||||
| Obinutuzumab | √ | ||||
| Enhanced antibodies | |||||
| Tafasitamab | CD19 | √ † | |||
| Radioimmunotherapy | |||||
| 90Y epratuzumab | CD22 | √ | |||
| 90Y ibritumomab tiuxetan | CD20 | √ | |||
| 131I tositumomab | √ | ||||
| Immune checkpoint inhibitors | |||||
| Nivolumab | PD-1 | √ | |||
| Pembrolizumab | √ *,† | ||||
| Avelumab | PD-L1 | √ | |||
| Atezolizumab | √ | ||||
| Durvalumab | √ | ||||
| Magrolimab | CD47 | √ | |||
| Antibody-drug conjugates | |||||
| Brentuximab vedotin | CD30 | √ | |||
| Inotuzumab ozogamicin | CD22 | √ | |||
| Pinatuzumab vedotin | √ | ||||
| Polatuzumab vedotin | CD79b | √ | |||
| Iladatuzumab vedotin | √ | ||||
| Loncastuximab tesirine | CD19 | √ † | |||
| Denintuzumab mafodotin | √ | ||||
| Coltuximab ravtansine | √ | ||||
| Camidanlumab tesirine | CD25 | √ | |||
| Naratuximab emtansine | CD37 | √ | |||
| Vorsetuzumab mafodotin | CD70 | √ | |||
| Zilovertamab vedotin | ROR1 | √ | |||
| Bispecific antibodies | |||||
| Glofitamab | CD3xCD20 | √ | |||
| Epcoritamab | √ | ||||
| Mosunetuzumab | √ | ||||
| Plamotamab | √ | ||||
| Odronextamab | √ | ||||
| Blinatumomab | CD3xCD19 | √ | |||
| Chimeric antigen receptor T-cells | |||||
| Axicabtagene ciloleucel | CD19 | √ | |||
| Tisagenlecleucel | √ | ||||
| Lisocabtagene maraleucel | √ † | ||||
| Reference | Study ID | Study Phase | Study Population | Treatment Protocol | Status | ORR (CR), % | PFS | OS |
|---|---|---|---|---|---|---|---|---|
| Tafasitamab | ||||||||
| Belada (2020) [40] | First-MIND NCT04134936 | Ib | 66 (IPI 2–5, ECOG PS: 0–2) | Tafasitamab (12 mg/kg d1, 8, 15) + R-CHOP (C1–6) | Active, not recruiting | 76 (NR) | NR | NR |
| Tafasitamab + R2-CHOP (C1–6) | 82 (NR) | |||||||
| Front-MIND NCT04824092 | III | IPI 3–5 (>60 y) or aaIPI 2–3 (≤60 y) ECOG PS: 0–2 | Tafasitamab (12 mg/kg d1, 8, 15) + R2-CHOP (C1–6) | Recruiting | ||||
| R-CHOP (C1–6) | ||||||||
| Pembrolizumab | ||||||||
| Smith (2020) [41] | NCT02541565 | I | 24 (ECOG PS 0–1) | Pembrolizumab (200 mg q3w) + R-CHOP (C1–6) | Completed | 90 (77) | 83% (2 y) | 84% (2 y) |
| Atezolizumab | ||||||||
| Younes (2019) [42] | NCT02596971 | I/II | 42 (ECOG PS 0–2) | Atezolizumab (1200 mg d1 C2–8) + R-CHOP Consolidation: atezolizumab 1200 mg q3w C9–25 | Completed | 88 (79) | 75% (2 y) | 86% (2 y) |
| Durvalumab | ||||||||
| Nowakowski (2021) | NCT03003520 | II | 46 (IPI ≥ 3, NCCN-IPI ≥ 4, ECOG PS 0–2) | Durvalumab (1125 mg d1 C1–8) + R-CHOP Consolidation: durvalumab 1500 mg q4w × 12 cycles | Active, not recruiting | 97 (68) | 68% (1 y) | NR |
| Durvalumab + R2-CHOP Consolidation: durvalumab q4w × 12 cycles | 100 (67) | 67% (1 y) | NR | |||||
| Avelumab | ||||||||
| Hawkes (2020) [43] | NCT03244176 | ΙΙ | 28 (Stage II-IV, ECOG: 0–2) | Avelumab (10 mg/kg) + rituximab q2w for two cycles followed by R-CHOP-21 × 6 cycles. Consolidation: avelumab q2w × 6 cycles | Recruiting | 89 (89) | 76% (1 y) | 89% (1 y) |
| Brentuximab vedotin | ||||||||
| Budde (2016) [44] | NCT01925612 | II | 51 (IPI 3–5 or aaIPI 2–3 | BV (1.2 or 1.8 mg/kg) + R-CHOP q3w | Terminated (portfolio prioritization) | NR (69) | CD30+: 79% CD30-: 58% (1.5 y) | CD30+: 92% CD30-: 71% (1.5 y) |
| 11 (IPI 3–5 or aaIPI 2–3) | BV 1.8 mg/kg + R-CHP q3w | 91 (82) | NR | NR | ||||
| Svoboda (2020) [45] | NCT01994850 | II | 29 (5 DLBCL, 22 PMLBL, 2 GZL) | BV 1.8 mg/kg + R-CHP q3w | Completed | 100 (86) | Not reached 85% (2 y) | Not reached 100% (2 y) |
| Reagan (2020) [46] | NCT02734771 | II | 22 (age ≥ 75 years) | BV 1.8 mg/kg + R-miniCHP q3w | Active, not recruiting | 86 (67) | Not reached 61% (2 y) | Not reached 74% (2 y) |
| Polatuzumab vedotin | ||||||||
| Tilly (2019) [47] | NCT01992653 | Ib/II | 66 (ECOG PS 0–2) | PolaV 1.8 mg/kg + R-CHP or G-CHP | Completed | 89 (77) | 83% (2 y) | 94% (1 y) |
| Tilly (2021) [48] | POLARIX NCT01992653 | III | 879 (IPI 2–5, ECOG PS 0–2) | PolaV 1.8 mg/kg + R-CHP | Completed | 86 (78) | 77% (2 y) * | 89% (2 y) |
| R-CHOP | 84 (74) | 70 (2 y) * | 89% (2 y) | |||||
| NCT04231877 | I | DLBCL, High-grade BCL | PolaV + R-da-EPOCH q3w | Active, not recruiting | ||||
| NCT04479267 | II | Double or triple-hit high-grade BCL | PolaV 1.8 mg/kg + R-CHP | Recruiting | ||||
| Glofitamab | ||||||||
| NCT03467373 | I | ECOG PS: 0–3 | Glofitamab + R-CHOP | Recruiting | ||||
| Epcoritamab | ||||||||
| NCT04663347 | I/II | DLBCL | Epcoritamab + R-CHOP | Recruiting | ||||
| Mosunetuzumab | ||||||||
| Olszewski (2021) [49] | NCT03677141 | I/II | 40 DLBCL (elderly or unfit patients) | Monotherapy (d1, d8, and d15 of C1, then q3w for eight cycles) | Recruiting | 68 (42) | NR | NR |
| Phillips (2020) [50] | NCT03677141 | I/II | 43 DLBCL | Mosunetuzumab + CHOP | Recruiting | 96 (85) | NR | NR |
| ADC | Antibody | Linker | Payload Release † | Payload | Target | DAR | Mode of Action § | Payload Specific Toxicities |
|---|---|---|---|---|---|---|---|---|
| Brentuximab vedotin (BV) | Chimeric IgG1 | Cleavable, MC-VC-PAB | I | MMAE | CD30 | 4 | A | Peripheral neuropathy, neutropenia |
| Inotuzumab ozogamicin (InO) | Humanized IgG4 | Cleavable, AcBut | II | N-acetyl gamma calicheamicin | CD22 | 6 | B | Hepatotoxicity, veno-occlusive liver disease, thrombocytopenia |
| Polatuzumab vedotin (PolaV) | Humanized IgG1 | Cleavable MC-VC-PAB | I | MMAE | CD79b | 3.5 | A | Peripheral neuropathy, neutropenia |
| Loncastuximab tesirine | Humanized IgG1 | Cleavable, MC-PEG-VA | I | SG3199, PBD | CD19 | 2.3 | C | Photosensitivity, increased GGT, myelosuppression, effusions, edema |
| Denintuzumab mafodotin (SGN-CD19A) | Humanized IgG1 | Non-cleavable maleimidocaproyl linker | III | MMAF | CD19 | NA | A | Ocular toxicity, Keratopathy |
| Coltuximab ravtansine (SAR3419) | Humanized IgG1 | Cleavable, SPDB | IV | Maytansinoid DM4 | CD19 | 3.5 | A | Ocular toxicity |
| Pinatuzumab vedotin (DCDT2980S) | Humanized IgG1 | Cleavable, MC-VC-PAB | I | MMAE | CD22 | 3.6 | A | Peripheral neuropathy, neutropenia |
| Camidanlumab tesirine (ADCT-301) | Humanized IgG1 | Cleavable MC-PEG-VA | I | SG3199, PBD | CD25 | 2.3 | C | Photosensitivity, increased GGT, myelosuppression, effusions, edema |
| Naratuximab emtansine (IMGN529) | Humanized IgG1 | Non-cleavableSMCC | III | Maytansinoid DM1 | CD37 | 3–4 | A | Thrombocytopenia, elevated liver transaminases, peripheral neuropathy |
| AGS67E | Humanized IgG2 | Cleavable, MC-VC-PAB | I | MMAE | CD37 | 3.7 | A | Peripheral neuropathy, neutropenia |
| MDX-1203 | Humanized IgG1 | Cleavable, MC-VC | I | MED-A Duocarmycin carbamate prodrug | CD70 | 1.25 | C | Hypersensitivity, Effusions, edema |
| Vorsetuzumab mafodotin (SGN-75) | Humanized IgG1 | Non-cleavable Maleimidocaproyl linker | III | MMAF | CD70 | NA | A | Thrombocytopenia, Ocular toxicity |
| SGN-CD70A | Humanized IgG1 | Cleavable, MC-VA | I | SGD-1882 PBD | CD70 | 2 | C | Thrombocytopenia |
| Iladatuzumab vedotin (DCDS0780A) | Humanized IgG1 | Cleavable, MC-VC-PAB | I | MMAE | CD79b | 2 | A | Ocular toxicity, neutropenia |
| Zilovertamab Vedotin (MK-2140) | Humanized IgG1 | Cleavable, MC-VC-PAB | I | MMAE | ROR1 | 4 | A | Peripheral neuropathy, neutropenia |
| Reference | Study Phase | Patients | Age, Median (Range) | Prior Treatment Lines Median (Range) | Treatment Protocol | ORR (CR), % | mDOR (Months) | Median PFS (Months) |
|---|---|---|---|---|---|---|---|---|
| Brentuximab vedotin | ||||||||
| Jacobsen (2015) [71] | II | 49 (CD30+, ECOG PS: 0–2) | 62 (17–85) | 3 (1–6) | BV 1.8 mg/kg q3w | 44 (17) | 5.6 | 4.0 |
| 16 (CD30+, ECOG PS: 0–2) | 62 (22–78) | 3 (1–5) | BV 1.8 mg/kg q3w + rituximab q3w | 46 (15) | NR | NR | ||
| Bartlett (2017) [72] | II | 52 CD30u, ECOG PS: 0–2) | 65 (21–91) | 2 (1–4) | BV 1.8 mg/kg q3w | 31 (12) | 4.7 | 1.4 |
| Kim (2019) [73] | II | 12 (CD30 > 30%, ECOG PS: 0–2) | 56 (27–73) | 3 (2–10) | BV 1.8 mg/kg q3w | 50 (17) | 6.0 | 1.9 |
| Zinzani (2017) [74] | II | 15 PMLBCL (CD30+, ECOG PS: 0–1) | 29 (20–73) | 3 (1–4) | BV 1.8 mg/kg q3w | 13 (0) | <3 | NR |
| Ward (2021) [75] | I | 37 (ECOG PS: 0–2) | 65 (51–79) | 3 (1–6) | BV 1.8 mg/kg q3w + lenalidomide 20 mg per day | 57 (35) | 13.1 | 10.2 |
| Zinzani (2019) [76] | I/II | 30 PMLBCL (CD30+, ECOG PS: 0–1) | 36 (19–83) | 2 (2–5) | BV 1.8 mg/kg q3w + nivolumab q3w | 73 (37) | 31.6 | 26.0 |
| Inotuzumab ozogamicin | ||||||||
| Advani (2010) [78] | I | 35 (CD22+, ECOG PS: 0–2) | 60 (26–82) | ≥4: 61% | InO 1.8 mg/m2 q3w | 15 (8) | NR | 1.6 |
| Fayad (2013) [79] | I/II | 47 (CD22+, ECOG PS: 0–2) | 72 (32–85) | ≥3: 9% | InO 1.8 mg/m2 + rituximab q4w | 74 (50) | 17.7 | 17.1 |
| Wagner-Johnston (2015) [80] | II | 63 (CD22+, ECOG PS: 0–2, Prior Tx lines ≤ 2) | 60 (19–75) | ≥2: 52 | InO 1.8 mg/m2 + rituximab 375 mg/m2 q3w ± ASCT | 30 (14) | NR | 3.0 |
| Dang (2018) [81] | III | 338 (CD22+, ECOG PS: 0–3, ASCT ineligible) | 70 (18–92) | 2 (1–3) | InO 1.8 mg/m2 + rituximab q4w | 41 (16) | 11.6 | 3.7 |
| BR or R-G | 44 (16) | 6.9 | 3.5 | |||||
| Ogura (2016) [82] | I | 21 (CD22+, ECOG PS: 0–2) | 63 (42–81) | 2 (1–6) | InO 0.8 mg/m2 + R-CVP q3w | 57 (10) | 11 | 4 |
| Sangha (2017) [83] | I | 21 (CD22+, ECOG PS: 0–2) | 65 (25–81) | 2 (1–6) | InO 0.8 mg/m2 + R-GDP q3w | 33 (19) | 9.3 | 6.1 |
| Polatuzumab vedotin | ||||||||
| Palanca-Wessels (2015) [84] | I/II | 25 (ECOG PS: 0–2) | 67 (20–81) | ≥3: 88% | PolaV 2.4 mg/kg q3w | 56 (16) | 5.2 | 5.0 |
| PolaV 2.4 mg/kg + rituximab q3w | 78 (22) | 12.3 | 12.5 | |||||
| Morschhauser (2019) [85] | Ib/II | 39 (ECOG PS: 0–2) | 68 (55–77) | 3 (2–6) | PolaV 2.4 mg/kg + rituximab q3w | 54 (21) | 13.4 | 5.6 |
| Phillips (2016) [86] | Ib/II | 38 (ECOG PS: 0–2) | 71 (27–84) | 2 (1–7) | PolaV 2.4 mg/kg + obinutuzumab q3w | 52 (29) | NR | NR |
| Sehn (2020) [87] | Ib/II | 40 (ECOG PS: 0–2) | 67 (33–86) | 2 (1–7) | PolaV 1.8 mg/kg + BR q3w | 45 (40) | 12.5 | 9.5 |
| Sehn (2021) [88] | Ib/II | 106 (ECOG PS: 0–2) | 70 (24–94) | 2 (1–7) | PolaV 1.8 mg/kg + BR q3w | 42 (39) | 9.5 | 6.6 |
| Loncastuximab tesirine | ||||||||
| Hamadani (2020) [89] | I | 139 DLBCL | 63 (20–86) | 3 (1–10) | 0.15 mg/kg q3w | 42 (23) | 4.5 | 2.8 |
| Caimi (2021) [90] | II | 145 DLBCL | 66 (56–71) | 3 (2–4) | 0.15 mg/kg q3w for 2 cycles and then 0.075 mg/kg for one year | 48 (24) | 12.6 | 4.9 |
| Dimou et al. [99] | Segman et al. [100] | Smith et al. [101] | Northend et al. [102] | Liebers et al. [97] | Vodicka et al. [103] | Sehn et al. [88] | |
|---|---|---|---|---|---|---|---|
| Patients (n) | 49 | 32 | 69 | 133 | 54 | 21 | 106 |
| Age, median (range) | 63 (67–85) | 66 (37–77) | 62 (17–88) | 72 (18–88) | 74 (37–87) | 67 (35–85) | 70 (24–94) |
| Gender (male %) | 53 | 60 | 62 | 65.4 | 68.5 | NA | 49 |
| Median prior treatment lines (range) | 2 (1–9) | 3 (2–3) | 3 (1–9) | ≥2: 64.7 | 3 (2–8) | 3 (2–7) | 2 (1–7) |
| Refractory to 1st treatment line (%) | 67 | 53 | NA | NA | NA | NA | 69 |
| Refractory to last treatment line (%) | 38 (78) | 23 (72) | NA | 68.4 | 87 | NA | 76 |
| Performance status, % | 0–1: 61 2: 20 3–4: 20 | ≥2: 53 | >1: 33 | ≥2: 30 | NA | ≥2: 76 | 0: 28 1: 59 2: 13 |
| Ann-Arbor stage III/IV (%) | 57 | 88 | NA | NA | NA | 48 | 79 |
| Prior ASCT, % | 16 | 31 | 16 | NA | 9 | 29 | 18 |
| Prior CAR-T cell therapy, % | 0 | 3 | 26 | NA | 9 | NA | 1 |
| ORR, % | 43 | 63 | 50 | 57 | 48 | 33 | 42 |
| CR, % | 25 | 38 | 24 | 33 | 15 | 24 | 39 |
| Median PFS (95% CI) (months) | 4 (2.3–5.8) | 5.6 (2.97–7.97) | 2 (NA) | 4.8 (3.7–9.3) | 1 y: 8.0% (1.7–38.3) | 8.7 (NA) | 6.6 (5.1–9.2) |
| Median OS (95% CI) (months) | 8.5 (3.1–13.8) | 8.3 (5.4–14.8) | 5.3 (NA) | 8.2 (5.9–14.3) | 1 y: 12.6 (4.1–38.9) | 3.8 (NA) | 12.5 (8.3–23.1) |
| Median DoR (95% CI) (months) | 8.7 (4–16) | 12.6 (NA) | 5 (NA) | NA | NA | NA | 9.5 (7.9–23.1) |
| Glofitamab Hutchings et al. [123] | Epcoritamab Hutchings et al. [124] | Odronextamab Bannerji et al. [125] | Mosunetuzumab Budde et al. [126] | |
|---|---|---|---|---|
| Structure | IgG-like Humanized IgG1 CrossMab (2:1) | IgG-like Humanized IgG1 DuoBody (1:1) | IgG-like Humanized IgG4 Common light chains (1:1) | IgG-like Humanized IgG1 Knobs-in-holes (1:1) |
| Route of administration | IV | SC | IV | IV or SC |
| Plasma half-life | 6–11 days | 8.67 days | 14 days | 6–11 days |
| Recommended phase 2 dose (RP2D) | 2.5/10/30 mg | 48 mg | 160/320 mg | 1/2/60/60/30 mg (IV) 5/45/45 mg (SC) |
| Treatment Schedule | C1d1: Obinutuzumab 1000 mg C1d8: Glofitamab 2.5 mg C1d15: Glofitamab 10 mg C2d1-C12d1: Glofitamab 30 mg (Cycles of 21 days) | C1-2: qw C3-6: q2w C7-: q4w (Cycles of 28 days) | 160 mg qw for 12 weeks 320 mg q2w onwards Week 1: Initial dose split in two days Week 2: Intermediate dose split in two days | C1d1: 1 mg (IV) 5 mg (SC) C1d8: 2 mg (IV) 45 mg (SC) C1d15: 60 mg (IV) 45 mg (SC) C2d1: 60 mg (IV) 45 mg (SC) C3d1-: 30 mg (IV) 45 mg (SC) (Cycles of 21 days) |
| Duration of treatment | Maximum of 12 cycles unless disease progression or unacceptable toxicity | Until disease progression or unacceptable toxicity | Until disease progression or unacceptable toxicity In patients with durable CR: q4w | Maximum of 17 cycles unless disease progression or unacceptable toxicity Discontinuation after 8 cycles in case of CR |
| Bispecific Antibody | Study PHASE | Patients | Age, Median (Range) | Prior Treatment Lines, Median (Range) | Treatment Protocol | Efficacy | Adverse Events (Grade ≥ 3) |
|---|---|---|---|---|---|---|---|
| CD3xCD20 | |||||||
| Glofitamab [123] | I | 258 (98 DLBCL) | 64 (22–86) | 3 (1–12) | Fixed dosing: 0.6–25 mg q2w or q3w Step-up dosing: 2.5/10/16 mg or 2.5/10/30 mg q3w | ORR: 54% CR: 39% mDOR: 29.4 months mPFS: 2.9 months | Neutropenia (25%) Thrombocytopenia (8%) Anemia (8%) CRS (5%) |
| Epcoritamab [124] | I/II | 68 (46 DLBCL) | 68 (55–74) | 3 (2–4) | 0.76–48 mg q1w: cycle 1–2; q2w: cycle 3–6; q4w thereafter | ORR: 68%; CR: 46% | Anemia (13%) Fatigue (6%) Hypotension (6%) Neurotoxicity (3%) |
| Mosunetuzumab [126] | I | 129 (82 DLBCL) | 63 (19–91) | 3 (1–14) | 1/2/60/60/30 mg q3w | ORR 35%; CR 19% mDOR: 7.6 months mPFS: 1.4 months | Neutropenia (25%) Hypophosphatemia (15%) Anemia (9%) CRS (1%) Neurotoxicity (4%) |
| Odronextamab [125] | I | 127 (71 DLBCL) | NR | 3 (1–11) | 0.03–320 mg q1w for 12w followed by q2w | No prior CAR-T: ORR: 60% CR: 60% mDOR: 10.3 months mPFS: 11.2 months Prior CAR-T: ORR: 33% CR: 23.8% mDOR: 2.8 months mPFS: 2.5 months | CRS (7%) Neurotoxicity (2%) |
| Plamotamab [127] | I | 47 (27 DLBCL) | 62 (32–89) | 4 (1–10) | 20–125 μg/kg q1w | ORR 41% CR: 26% | Neutropenia (14%) Thrombocytopenia (8%) Hypokalemia (6%) CRS (3%) |
| CD3xCD19 | |||||||
| Blinatumomab [128] | I | 76 (14 DLBCL) | 65 (20–80) | 3 (1–10) | 60 μg/m2/d Continuous IV 4–8 weeks followed by a 4-week consolidation | ORR: 55% CR: 36% mDOR: 13.5 months | Lymphopenia (79%) Neurologic (22%) Increase CRP (20%) Leukopenia (20%) Neutropenia (17%) Thrombocytopenia (12%) Hyperglycemia (12%) |
| Blinatumomab [129] | II | 25 DLBCL | 66 (34–85) | 3 (1–7) | 112 μg/d Continuous IV infusion for 8 weeks followed by 4-week consolidation | ORR 43% CR 19% mDoR 11.6 months mPFS 3.7 months | Thrombocytopenia (17%) Leukopenia: 17% Neurotoxicity (22%) |
| Blinatumomab [130] | II/III | 41 (34 DLBCL) | 59 (19–75) | NR | 9 μg/d for 7 d 28 μg/d for 7 d, 112 μg/d for 42 d followed by an optional 4-week cycle. | ORR: 37%; CR: 22% mPFS: 2.5 months mOS: Not reached | Neutropenia (10%) Neurotoxicity (24%) |
| Glofitamab Hutchings et al. [123] | Epcoritamab Hutchings et al. [124] | Odronextamab Bannerji et al. [125] | Mosunetuzumab Budde et al. [126] | |||
|---|---|---|---|---|---|---|
| Study Phase | Ι | I/II | Ι | I | ||
| Patients (n) | 258 98 DLBCL 31 tFL, 26 MCL, 11 RT 75 iNHL | 68 46 DLBCL 12 FL 4 MCL | 127 71 DLBCL 37 FL 11 MCL 6 MZL 2 Β-NHL | 129 82 DLBCL 26 tFL 13 MCL 5 RT 1 FL gr 3B | ||
| Age, median (range) | 64 (22–86) | 68 (55–74) | ΝR | 63 (19–91) | ||
| Eligibility criteria | R/R B-NHL, ECOG PS ≤ 1 | R/R B-NHL, ECOG PS ≤ 1 (after at least one Tx with anti-CD20 mAb) | R/R B-NHL, ECOG PS ≤ 1 (after at least one Tx with anti-CD20 mAb) | R/R B-NHL, ECOG PS ≤ 1 | ||
| Prior treatment lines, median (range) | 3 (1–12) | 3 (2–4) | 3 (1–11) | 3 (1–14) | ||
| Prior CAR-T cells (#) | 3 (1.8%) | 5 DLBCL | 29 (23%) (25 DLBCL) | 15 (11.6%) | ||
| Median follow-up (months) | 13.5 | 10.2 | 3.9 | 11.9 | ||
| Premedication (CRS prophylaxis) | 1000 mg obinutuzumab on day -7 | Corticosteroids | Dexamethasone | Corticosteroids | ||
| Dose | 2.5/10/16 mg 2.5/10/30 mg | ≥12 mg (n = 18) | ≥48 mg (n = 7) | Dose ≥ 80 mg | 1/2/60/60/30 mg | |
| Prior CAR-T (n = 21) | No prior CAR-T) (n = 10) | |||||
| ORR (%) | 54 | 68 | 91 | 33 | 60 | 35 |
| CR (%) | 39 | 45 | 55 | 24 | 60 | 19 |
| Median DOR (months) | 29.4 | ΝR | ΝR | 2.8 DoCR: 4.4 | 10.3 DoCR: 9.5 | 7.6 DoCR: 22.8 |
| Median PFS (months) | 2.9 | 9.1 | Not reached | 2.5 | 11.1 | 1.4 |
| CRS (%) (grade 3 + 4) | 5.1% | 0 | 7.1% (6.3 + 0.8) | 1% | ||
| Neurotoxicity (grade 3 + 4) | 0 | 3% | 2.3% (2.3 + 0) | 4.1% | ||
| Treatment discontinuation | 2.9% | 0 | 5.5% | 3.6% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papageorgiou, S.G.; Thomopoulos, T.P.; Liaskas, A.; Vassilakopoulos, T.P. Monoclonal Antibodies in the Treatment of Diffuse Large B-Cell Lymphoma: Moving beyond Rituximab. Cancers 2022, 14, 1917. https://doi.org/10.3390/cancers14081917
Papageorgiou SG, Thomopoulos TP, Liaskas A, Vassilakopoulos TP. Monoclonal Antibodies in the Treatment of Diffuse Large B-Cell Lymphoma: Moving beyond Rituximab. Cancers. 2022; 14(8):1917. https://doi.org/10.3390/cancers14081917
Chicago/Turabian StylePapageorgiou, Sotirios G., Thomas P. Thomopoulos, Athanasios Liaskas, and Theodoros P. Vassilakopoulos. 2022. "Monoclonal Antibodies in the Treatment of Diffuse Large B-Cell Lymphoma: Moving beyond Rituximab" Cancers 14, no. 8: 1917. https://doi.org/10.3390/cancers14081917