
Cost-Effectiveness of Genetic Testing for All Women Diagnosed with Breast Cancer in China

 , , , ,
, , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
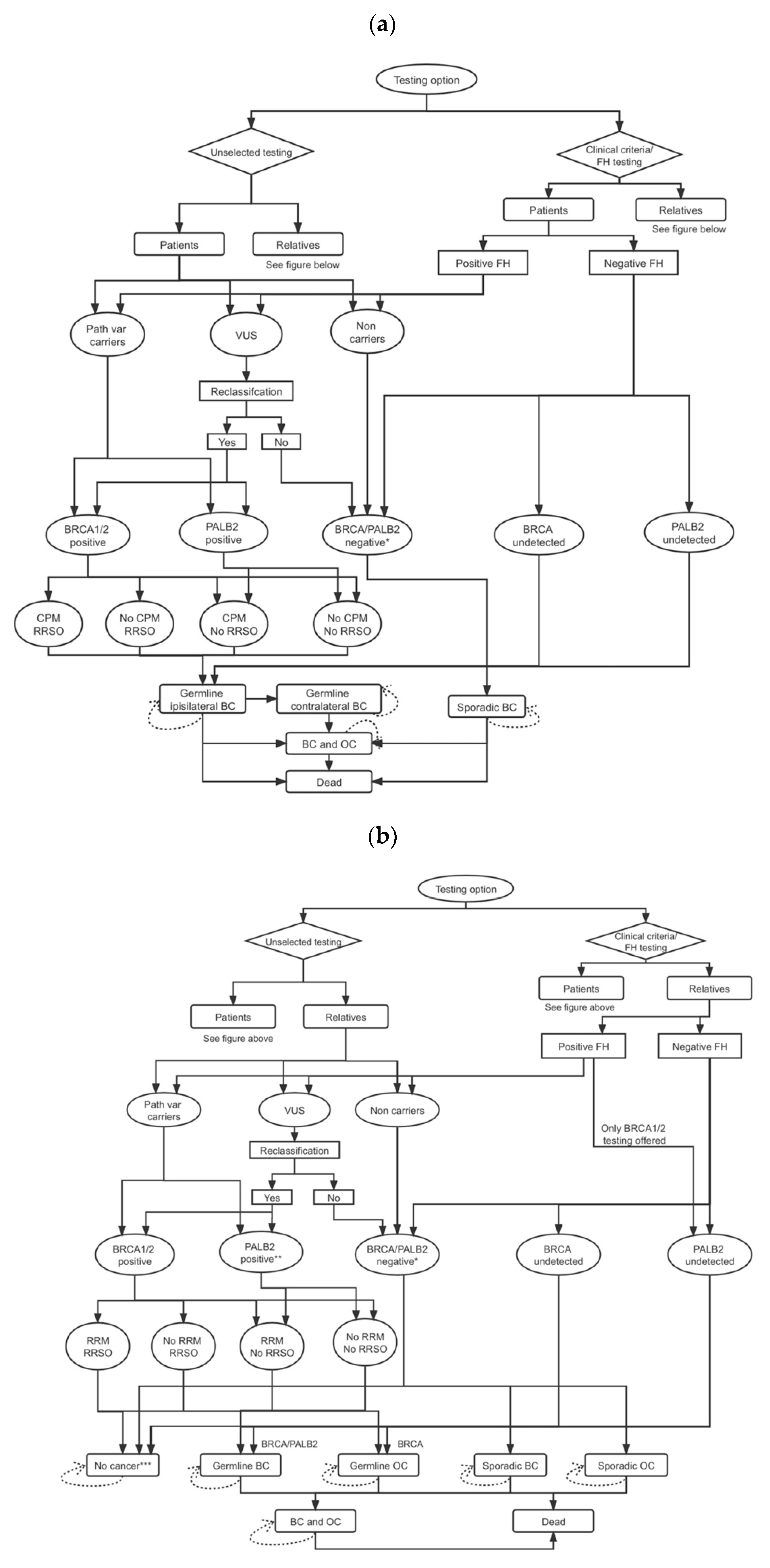
2.1. Model and Genetic Testing Strategy
2.2. Probabilities
2.3. Relatives: Number and Age Distribution
2.4. Costs
2.5. Life-Years
2.6. Quality-Adjusted Life-Years (QALYs)
2.7. Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- NICE. Familial Breast Cancer: Classification, Care and Managing Breast Cancer and Related Risks in People with a Family History of Breast Cancer; NICE Clinical Guideline CG164, Updated 2017 ed.; National Institute for Health and Care Excellence: London, UK, 2017; Available online: https://www.nice.org.uk/guidance/cg164 (accessed on 10 June 2021).
- Manchanda, R.; Burnell, M.; Abdelraheim, A.; Johnson, M.; Sharma, A.; Benjamin, E.; Brunell, C.; Saridogan, E.; Gessler, S.; Oram, D.; et al. Factors influencing uptake and timing of risk reducing salpingo-oophorectomy in women at risk of familial ovarian cancer: A competing risk time to event analysis. BJOG 2012, 119, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.A.; Eisen, A.; Poll, A.; Candib, A.; McCready, D.; Cil, T.; Wright, F.; Demsky, R.; Mancuso, T.; Sun, P.; et al. Frequency of Contralateral Prophylactic Mastectomy in Breast Cancer Patients with a Negative BRCA1 and BRCA2 Rapid Genetic Test Result. Ann. Surg. Oncol. 2021, 28, 4967–4973. [Google Scholar] [CrossRef]
- Childers, C.P.; Childers, K.K.; Maggard-Gibbons, M.; Macinko, J. National Estimates of Genetic Testing in Women With a History of Breast or Ovarian Cancer. J. Clin. Oncol. 2017, 35, 3800–3806. [Google Scholar] [CrossRef] [PubMed]
- Kurian, A.W.; Ward, K.C.; Howlader, N.; Deapen, D.; Hamilton, A.S.; Mariotto, A.; Miller, D.; Penberthy, L.S.; Katz, S.J. Genetic Testing and Results in a Population-Based Cohort of Breast Cancer Patients and Ovarian Cancer Patients. J. Clin. Oncol. 2019, 37, 1305–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, L.; Strasser-Weippl, K.; Li, J.-J.; Louis, J.S.; Finkelstein, D.M.; Yu, K.-D.; Chen, W.-Q.; Shao, Z.-M.; Goss, P.E. Breast Cancer in China. Lancet Oncol. 2014, 15, e279–e289. [Google Scholar]
- Li, J.; Zhang, B.N.; Fan, J.H.; Pang, Y.; Zhang, P.; Wang, S.L.; Zheng, S.; Zhang, B.; Yang, H.J.; Xie, X.M.; et al. A nation-wide multicenter 10-year (1999–2008) retrospective clinical epidemiological study of female breast cancer in China. BMC Cancer 2011, 11, 364. [Google Scholar] [CrossRef] [Green Version]
- Fan, L.; Strasser-Weippl, K.; Li, J.J.; St Louis, J.; Finkelstein, D.M.; Yu, K.D.; Chen, W.Q.; Shao, Z.M.; Goss, P.E. Breast cancer in China. Lancet. Oncol. 2014, 15, e279–e289. [Google Scholar] [CrossRef]
- Sun, L.; Brentnall, A.; Patel, S.; Buist, D.S.M.; Bowles, E.J.A.; Evans, D.G.R.; Eccles, D.; Hopper, J.; Li, S.; Southey, M.; et al. A Cost-effectiveness Analysis of Multigene Testing for All Patients With Breast Cancer. JAMA Oncol. 2019, 5, 1718–1730. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics. Main Data of the Seventh National Population Census. Available online: http://www.stats.gov.cn/tjsj/zxfb/202105/t20210510_1817176.html (accessed on 31 October 2021).
- Sun, J.; Meng, H.; Yao, L.; Lv, M.; Bai, J.; Zhang, J.; Wang, L.; Ouyang, T.; Li, J.; Wang, T.; et al. Germline Mutations in Cancer Susceptibility Genes in a Large Series of Unselected Breast Cancer Patients. Clin. Cancer Res. 2017, 23, 6113–6119. [Google Scholar] [CrossRef] [Green Version]
- Beitsch, P.D.; Whitworth, P.W.; Hughes, K.; Patel, R.; Rosen, B.; Compagnoni, G.; Baron, P.; Simmons, R.; Smith, L.A.; Grady, I.; et al. Underdiagnosis of Hereditary Breast Cancer: Are Genetic Testing Guidelines a Tool or an Obstacle? J. Clin. Oncol. 2019, 37, 453–460. [Google Scholar] [CrossRef]
- Metcalfe, K.A.; Eisen, A.; Poll, A.; Candib, A.; McCready, D.; Cil, T.; Wright, F.; Lerner-Ellis, J.; McCuaig, J.; Graham, T.; et al. Rapid Genetic Testing for BRCA1 and BRCA2 Mutations at the Time of Breast Cancer Diagnosis: An Observational Study. Ann. Surg. Oncol. 2021, 28, 2219–2226. [Google Scholar] [CrossRef] [PubMed]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoniou, A.C.; Casadei, S.; Heikkinen, T.; Barrowdale, D.; Pylkas, K.; Roberts, J.; Lee, A.; Subramanian, D.; De Leeneer, K.; Fostira, F.; et al. Breast-cancer risk in families with mutations in PALB2. N. Engl. J. Med. 2014, 371, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Leslie, G.; Doroszuk, A.; Schneider, S.; Allen, J.; Decker, B.; Dunning, A.M.; Redman, J.; Scarth, J.; Plaskocinska, I.; et al. Cancer Risks Associated with Germline PALB2 Pathogenic Variants: An International Study of 524 Families. J. Clin. Oncol. 2019, 38, 674–685. [Google Scholar] [CrossRef] [PubMed]
- Asphaug, L.; Melberg, H.O. The Cost-Effectiveness of Multigene Panel Testing for Hereditary Breast and Ovarian Cancer in Norway. MDM Policy Pract. 2019, 4, 2381468318821103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koldehoff, A.; Danner, M.; Civello, D.; Rhiem, K.; Stock, S.; Müller, D. Cost-Effectiveness of Targeted Genetic Testing for Breast and Ovarian Cancer: A Systematic Review. Value Health 2021, 24, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Manahan, E.R.; Kuerer, H.M.; Sebastian, M.; Hughes, K.S.; Boughey, J.C.; Euhus, D.M.; Boolbol, S.K.; Taylor, W.A. Consensus Guidelines on Genetic‘ Testing for Hereditary Breast Cancer from the American Society of Breast Surgeons. Ann. Surg. Oncol. 2019, 26, 3025–3031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Easton, D.F.; Pharoah, P.D.; Antoniou, A.C.; Tischkowitz, M.; Tavtigian, S.V.; Nathanson, K.L.; Devilee, P.; Meindl, A.; Couch, F.J.; Southey, M.; et al. Gene-panel sequencing and the prediction of breast-cancer risk. N. Engl. J. Med. 2015, 372, 2243–2257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddow, J.; Palomaki, G. ACCE: A Model Process for Evaluating Data on Emerging Genetic Tests. In Human Genome Epidemiology: A Scientific Foundation for Using Genetic Information to Improve Health and Prevent Disease; Khoury, M., Little, J., Burke, W., Eds.; Oxford University Press: Oxford, UK, 2003; pp. 217–233. [Google Scholar]
- International Agency for Research on Cancer. Estimated Number of New Cases in 2018, Worldwide, Females, All Ages. Available online: http://gco.iarc.fr/today/online-analysis-table (accessed on 21 June 2021).
- Van Marcke, C.; Collard, A.; Vikkula, M.; Duhoux, F.P. Prevalence of pathogenic variants and variants of unknown significance in patients at high risk of breast cancer: A systematic review and meta-analysis of gene-panel data. Crit. Rev. Oncol. Hematol. 2018, 132, 138–144. [Google Scholar] [CrossRef]
- Mersch, J.; Brown, N.; Pirzadeh-Miller, S.; Mundt, E.; Cox, H.C.; Brown, K.; Aston, M.; Esterling, L.; Manley, S.; Ross, T. Prevalence of Variant Reclassification Following Hereditary Cancer Genetic Testing. JAMA 2018, 320, 1266–1274. [Google Scholar] [CrossRef]
- Chai, X.; Domchek, S.; Kauff, N.; Rebbeck, T.; Chen, J. RE: Breast Cancer Risk After Salpingo-Oophorectomy in Healthy BRCA1/2 Mutation Carriers: Revisiting the Evidence for Risk Reduction. J. Natl. Cancer Inst. 2015, 107, djv217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domchek, S.M.; Friebel, T.M.; Singer, C.F.; Evans, D.G.; Lynch, H.T.; Isaacs, C.; Garber, J.E.; Neuhausen, S.L.; Matloff, E.; Eeles, R.; et al. Association of risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA 2010, 304, 967–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebbeck, T.R.; Kauff, N.D.; Domchek, S.M. Meta-analysis of risk reduction estimates associated with risk-reducing salpingo-oophorectomy in BRCA1 or BRCA2 mutation carriers. J. Natl. Cancer Inst. 2009, 101, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Heemskerk-Gerritsen, B.A.; Seynaeve, C.; van Asperen, C.J.; Ausems, M.G.; Collee, J.M.; van Doorn, H.C.; Gomez Garcia, E.B.; Kets, C.M.; van Leeuwen, F.E.; Meijers-Heijboer, H.E.; et al. Breast cancer risk after salpingo-oophorectomy in healthy BRCA1/2 mutation carriers: Revisiting the evidence for risk reduction. J. Natl. Cancer Inst. 2015, 107, djv033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breast Cancer Treatment—National Cancer Institute. Available online: https://www.cancer.gov/types/breast/hp/breast-treatment-pdq (accessed on 22 November 2021).
- Parker, W.H.; Feskanich, D.; Broder, M.S.; Chang, E.; Shoupe, D.; Farquhar, C.M.; Berek, J.S.; Manson, J.E. Long-term mortality associated with oophorectomy compared with ovarian conservation in the nurses’ health study. Obstet. Gynecol. 2013, 121, 709–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivera, C.M.; Grossardt, B.R.; Rhodes, D.J.; Brown, R.D., Jr.; Roger, V.L.; Melton, L.J., 3rd; Rocca, W.A. Increased cardiovascular mortality after early bilateral oophorectomy. Menopause 2009, 16, 15–23. [Google Scholar] [CrossRef] [Green Version]
- Edejer, T.; Baltussen, R.; Adam, T.; Hutubessy, R.; Acharya, A.; Evans, D.; Murray, C. WHO Guide to Cost-Effectiveness Analysis; WHO, Ed.; World Health Organisation: Geneva, Switzerland, 2003. [Google Scholar]
- United Nations Department of Economic and Social Affairs. World Population Prospects 2019. Available online: https://population.un.org/wpp/ (accessed on 10 June 2021).
- Chen, H.; Chen, Y.; Cui, B. The association of multimorbidity with healthcare expenditure among the elderly patients in Beijing, China. Arch. Gerontol. Geriatr. 2018, 79, 32–38. [Google Scholar] [CrossRef]
- The World Bank. PPP Conversion Factor, GDP. The World Bank: 2019. Available online: https://data.worldbank.org/indicator/PA.NUS.PPP (accessed on 15 June 2021).
- Peking University; Fudan University; China Pharmaceutical University; Tianjin University; Ministry of Human Resources and Social Security; PLA 306 Hospital. China Guidelines for Pharmacoeconomic Evaluations. Available online: http://www.ispor.org/peguidelines/index.asp (accessed on 9 August 2021).
- Sanders, G.D.; Neumann, P.J.; Basu, A.; Brock, D.W.; Feeny, D.; Krahn, M.; Kuntz, K.M.; Meltzer, D.O.; Owens, D.K.; Prosser, L.A.; et al. Recommendations for Conduct, Methodological Practices, and Reporting of Cost-effectiveness Analyses: Second Panel on Cost-Effectiveness in Health and Medicine. JAMA 2016, 316, 1093–1103. [Google Scholar] [CrossRef]
- World Health Organisation. Life Tables; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Evans, D.G.; Lalloo, F.; Ashcroft, L.; Shenton, A.; Clancy, T.; Baildam, A.D.; Brain, A.; Hopwood, P.; Howell, A. Uptake of risk-reducing surgery in unaffected women at high risk of breast and ovarian cancer is risk, age, and time dependent. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2318–2324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Niksic, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Esteve, J.; et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Hammerschmidt, T.; Goertz, A.; Wagenpfeil, S.; Neiss, A.; Wutzler, P.; Banz, K. Validation of health economic models: The example of EVITA. Value Health 2003, 6, 551–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The World Bank. GDP per Capita (Current US$). Available online: http://data.worldbank.org/indicator/NY.GDP.PCAP.CD (accessed on 15 June 2021).
- Health Economics Resource Center. U.S. Department of Veterans Affairs. Cost-Effectiveness Analysis. Available online: https://www.herc.research.va.gov/include/page.asp?id=cost-effectiveness-analysis (accessed on 16 February 2021).
- Briggs, A. Probabilistic analysis of cost-effectiveness models: Statistical representation of parameter uncertainty. Value Health 2005, 8, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A Population-Based Study of Genes Previously Implicated in Breast Cancer. N. Engl. J. Med. 2021, 384, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Breast Cancer Association, C.; Dorling, L.; Carvalho, S.; Allen, J.; Gonzalez-Neira, A.; Luccarini, C.; Wahlstrom, C.; Pooley, K.A.; Parsons, M.T.; Fortuno, C.; et al. Breast Cancer Risk Genes—Association Analysis in More than 113,000 Women. N. Engl. J. Med. 2021, 384, 428–439. [Google Scholar] [CrossRef]
- NICE. NICE Health Technology Evaluations: The Manual. Available online: https://www.nice.org.uk/process/pmg36/chapter/introduction-to-health-technology-evaluation (accessed on 16 February 2022).
- Metcalfe, K.A.; Birenbaum-Carmeli, D.; Lubinski, J.; Gronwald, J.; Lynch, H.; Moller, P.; Ghadirian, P.; Foulkes, W.D.; Klijn, J.; Friedman, E.; et al. International variation in rates of uptake of preventive options in BRCA1 and BRCA2 mutation carriers. Int. J. Cancer 2008, 122, 2017–2022. [Google Scholar] [CrossRef] [Green Version]
- Kong, Y.; Yang, L.; Tang, H.; Lv, N.; Xie, X.; Li, J.; Guo, J.; Li, L.; Wu, M.; Gao, J.; et al. A nation-wide multicenter retrospective study of the epidemiological, pathological and clinical characteristics of breast cancer in situ in Chinese women in 1999–2008. PLoS ONE 2013, 8, e81055. [Google Scholar] [CrossRef] [Green Version]
- Xuan, Q.; Gao, K.; Song, Y.; Zhao, S.; Dong, L.; Zhang, Z.; Zhang, Q.; Wang, J. Adherence to Needed Adjuvant Therapy Could Decrease Recurrence Rates for Rural Patients With Early Breast Cancer. Clin. Breast Cancer 2016, 16, e165–e173. [Google Scholar] [CrossRef]
- Payne, K.; Gavan, S.P.; Wright, S.J.; Thompson, A.J. Cost-effectiveness analyses of genetic and genomic diagnostic tests. Nat. Rev. Genet. 2018, 19, 235–246. [Google Scholar] [CrossRef]
- Lowry, K.P.; Geuzinge, H.A.; Stout, N.K.; Alagoz, O.; Hampton, J.; Kerlikowske, K.; de Koning, H.J.; Miglioretti, D.L.; van Ravesteyn, N.T.; Schechter, C.; et al. Breast Cancer Screening Strategies for Women With ATM, CHEK2, and PALB2 Pathogenic Variants: A Comparative Modeling Analysis. JAMA Oncol. 2022. [Google Scholar] [CrossRef]
- Francken, A.B.; Schouten, P.C.; Bleiker, E.M.; Linn, S.C.; Rutgers, E.J. Breast cancer in women at high risk: The role of rapid genetic testing for BRCA1 and -2 mutations and the consequences for treatment strategies. Breast 2013, 22, 561–568. [Google Scholar] [CrossRef]
- Pal, T.; Agnese, D.; Daly, M.; La Spada, A.; Litton, J.; Wick, M.; Klugman, S.; Esplin, E.D.; Jarvik, G.P.; Professional, P.; et al. Points to consider: Is there evidence to support BRCA1/2 and other inherited breast cancer genetic testing for all breast cancer patients? A statement of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 2020, 22, 681–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, X.; Wang, P.; Tao, X.; Zhong, N. Genetic services and testing in China. J. Community Genet. 2013, 4, 379–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrasekaran, D.; Sobocan, M.; Blyuss, O.; Miller, R.E.; Evans, O.; Crusz, S.M.; Mills-Baldock, T.; Sun, L.; Hammond, R.F.L.; Gaba, F.; et al. Implementation of Multigene Germline and Parallel Somatic Genetic Testing in Epithelial Ovarian Cancer: SIGNPOST Study. Cancers 2021, 13, 4344. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Interventions | Health Effects | Costs (USD) | ICER (Cost/QALY) | ||||
|---|---|---|---|---|---|---|---|
| LYGs | QALYs | Payer | Societal | Payer | Societal | ||
| Testing all BC patients | 14.164 | 13.483 | 4686 | 6808 | Testing all BC patients vs. testing based on FH/clinical criteria | 6848 | 4152 |
| Testing based on FH/clinical criteria | 14.149 | 13.470 | 4596 | 6753 | Testing all BC patients vs. no testing | 8340 | 5416 |
| No testing | 14.144 | 13.465 | 4554 | 6726 | - | - | - |
| Testing all BC Patients | No Testing | ICER | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Health Effects | Costs (USD) | Health Effects | Costs (USD) | Cost/LYG | Cost/QALY | ||||||
| LYGs | QALYs | Payer | Societal | LYGs | QALYs | Payer | Societal | Payer | Societal | Payer | Societal |
| Baseline | |||||||||||
| 14.164 | 13.483 | 4686 | 6808 | 14.144 | 13.465 | 4554 | 6726 | 6509 | 4037 | 7266 | 4506 |
| Scenario: No reduction in BC risk from RRSO b | |||||||||||
| 14.164 | 13.483 | 4686 | 6808 | 14.144 | 13.465 | 4554 | 6726 | 6508 | 4060 | 7308 | 4558 |
| Scenario: No HRT Adherence c | |||||||||||
| 14.163 | 13.483 | 4687 | 6809 | 14.144 | 13.465 | 4554 | 6726 | 6730 | 4201 | 7576 | 4729 |
| Scenario: Half RRM uptake in unaffected relatives d | |||||||||||
| 14.164 | 13.483 | 4687 | 6811 | 14.144 | 13.465 | 4554 | 6726 | 6546 | 4198 | 7449 | 4777 |
| Scenario: Half RRSO uptake in unaffected relatives e | |||||||||||
| 14.163 | 13.482 | 4682 | 6807 | 14.144 | 13.465 | 4554 | 6726 | 6425 | 4090 | 7439 | 4735 |
| Scenario: Half RRM and half RRSO uptake in unaffected relatives f | |||||||||||
| 14.164 | 13.482 | 4685 | 6813 | 14.144 | 13.465 | 4554 | 6726 | 6514 | 4342 | 7802 | 5201 |
| Scenario: Half CPM uptake in patients g | |||||||||||
| 14.160 | 13.481 | 4683 | 6812 | 14.144 | 13.465 | 4554 | 6726 | 7857 | 5243 | 8310 | 5546 |
| Scenario: Half RRSO uptake in patients h | |||||||||||
| 14.160 | 13.481 | 4672 | 6800 | 14.144 | 13.465 | 4554 | 6726 | 7014 | 4412 | 7588 | 4773 |
| Scenario: Lower uptake rate of genetic testing in patients and relatives i (70%) | |||||||||||
| 14.158 | 13.477 | 4644 | 6787 | 14.144 | 13.465 | 4554 | 6726 | 6229 | 4233 | 7575 | 5148 |
| Scenario: Lower uptake rate of genetic testing in patients and relatives i (50%) | |||||||||||
| 14.153 | 13.473 | 4607 | 6762 | 14.144 | 13.465 | 4554 | 6726 | 5449 | 3731 | 6922 | 4739 |
| Scenario: No VUS management j | |||||||||||
| 14.162 | 13.479 | 4629 | 6766 | 14.144 | 13.465 | 4554 | 6726 | 3943 | 2097 | 5355 | 2848 |
| IMPACT | Testing All BC Patients | Testing Based on Family History | No Testing | Difference (Testing All vs. No Testing) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Patients | Relatives | Patients | Relatives | Patients | Relatives | Patients | Relatives | Total | |
| Germline BC cases | 2075 a | 7658 | 3806 a | 10,493 | 4515 a | 11,576 | 2440 | 3918 | 6358 |
| Germline OC cases | 737 | 2144 | 1263 | 2640 | 1487 | 2904 | 750 | 760 | 1510 |
| Germline BC/OC deaths | 4873 | 3679 | 7237 | 4968 | 8247 | 5469 | 3374 | 1790 | 5164 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, L.; Cui, B.; Wei, X.; Sadique, Z.; Yang, L.; Manchanda, R.; Legood, R. Cost-Effectiveness of Genetic Testing for All Women Diagnosed with Breast Cancer in China. Cancers 2022, 14, 1839. https://doi.org/10.3390/cancers14071839
Sun L, Cui B, Wei X, Sadique Z, Yang L, Manchanda R, Legood R. Cost-Effectiveness of Genetic Testing for All Women Diagnosed with Breast Cancer in China. Cancers. 2022; 14(7):1839. https://doi.org/10.3390/cancers14071839
Chicago/Turabian StyleSun, Li, Bin Cui, Xia Wei, Zia Sadique, Li Yang, Ranjit Manchanda, and Rosa Legood. 2022. "Cost-Effectiveness of Genetic Testing for All Women Diagnosed with Breast Cancer in China" Cancers 14, no. 7: 1839. https://doi.org/10.3390/cancers14071839