
Uptake Rates of Risk-Reducing Surgeries for Women at Increased Risk of Hereditary Breast and Ovarian Cancer Applied to Cost-Effectiveness Analyses: A Scoping Systematic Review


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Review
2.2. Value of Information (VOI) Analysis
3. Results
3.1. Strategies Being Compared
3.2. Study Population
3.3. Uptake Rates Applied to the Models
3.4. Sources of Uptake Rates
3.5. Impact of Varying Uptake Rates in Sensitivity Analyses
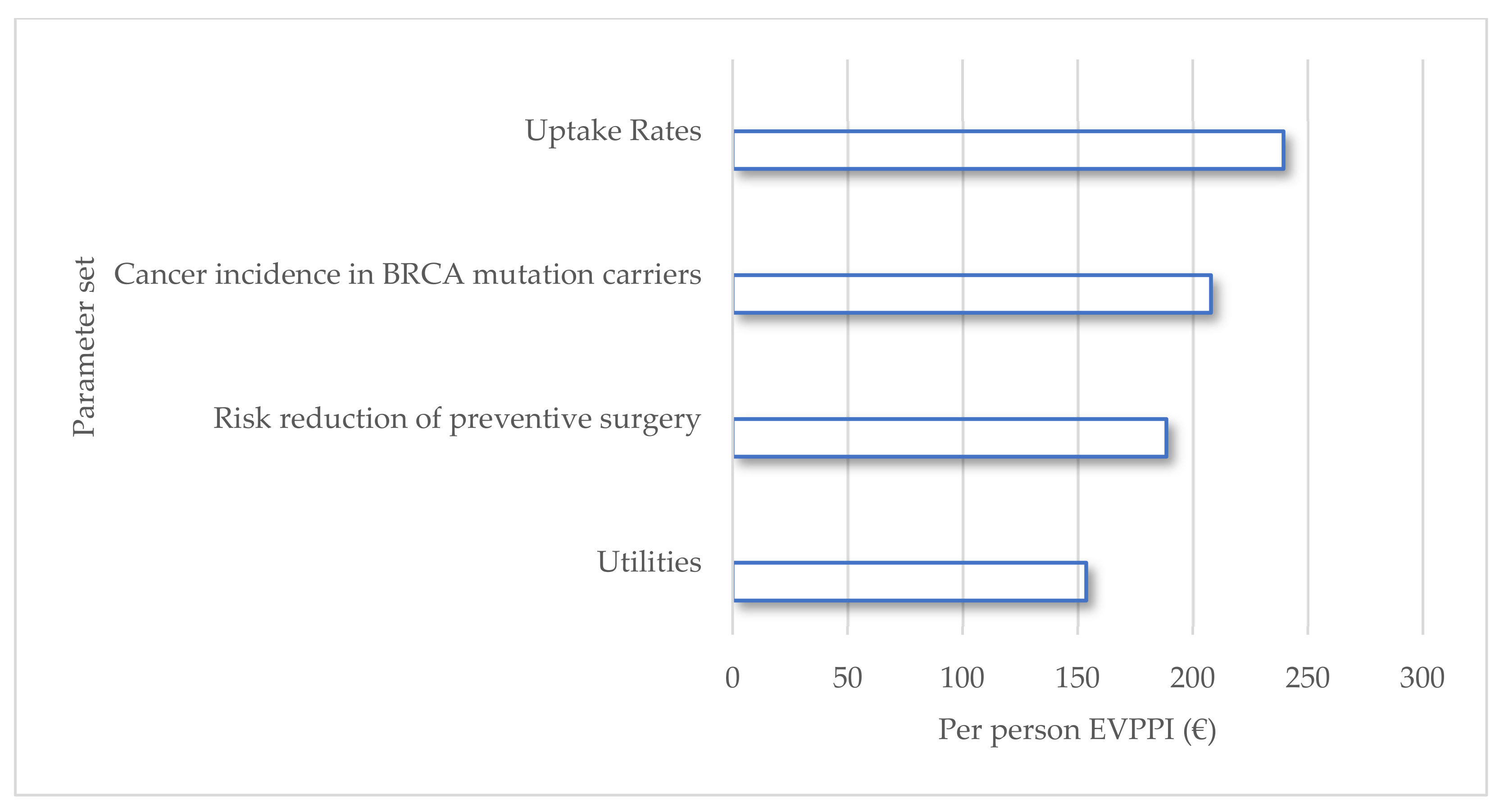
3.6. VOI Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Heemskerk-Gerritsen, B.A.M.; Jager, A.; Koppert, L.B.; Obdeijn, A.I.; Collée, M.; Meijers-Heijboer, H.E.J.; Jenner, D.J.; Oldenburg, H.S.A.; van Engelen, K.; de Vries, J.; et al. Survival after bilateral risk-reducing mastectomy in healthy BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 2019, 177, 723–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domchek, S.M.; Friebel, T.M.; Singer, C.F.; Evans, D.G.; Lynch, H.T.; Isaacs, C.; Garber, J.E.; Neuhausen, S.L.; Matloff, E.; Eeles, R.; et al. Association of risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA 2010, 304, 967–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotsopoulos, J.; Huzarski, T.; Gronwald, J.; Singer, C.F.; Moller, P.; Lynch, H.T.; Armel, S.; Karlan, B.; Foulkes, W.D.; Neuhausen, S.L.; et al. Bilateral Oophorectomy and Breast Cancer Risk in BRCA1 and BRCA2 Mutation Carriers. J. Natl. Cancer Inst. 2017, 109, djw177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavaddat, N.; Antoniou, A.C.; Mooij, T.M.; Hooning, M.J.; Heemskerk-Gerritsen, B.A.; Noguès, C.; Gauthier-Villars, M.; Caron, O.; Gesta, P.; Pujol, P.; et al. Risk-reducing salpingo-oophorectomy, natural menopause, and breast cancer risk: An international prospective cohort of BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. 2020, 22, 8. [Google Scholar] [CrossRef] [Green Version]
- Manchanda, R.; Abdelraheim, A.; Johnson, M.; Rosenthal, A.N.; Benjamin, E.; Brunell, C.; Burnell, M.; Side, L.; Gessler, S.; Saridogan, E.; et al. Outcome of risk-reducing salpingo-oophorectomy in BRCA carriers and women of unknown mutation status. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.D.; Pappas, M.; Zakher, B.; Mitchell, J.P.; Okinaka-Hu, L.; Fu, R. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: A systematic review to update the U.S. Preventive Services Task Force recommendation. Ann. Intern. Med. 2014, 160, 255–266. [Google Scholar] [CrossRef] [Green Version]
- Koldehoff, A.; Danner, M.; Civello, D.; Rhiem, K.; Stock, S.; Muller, D. Cost-Effectiveness of Targeted Genetic Testing for Breast and Ovarian Cancer: A Systematic Review. Value Health 2021, 24, 303–312. [Google Scholar] [CrossRef]
- Metcalfe, K.; Eisen, A.; Senter, L.; Armel, S.; Bordeleau, L.; Meschino, W.S.; Pal, T.; Lynch, H.T.; Tung, N.M.; Kwong, A.; et al. International trends in the uptake of cancer risk reduction strategies in women with a BRCA1 or BRCA2 mutation. Br. J. Cancer 2019, 121, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Muller, D.; Danner, M.; Schmutzler, R.; Engel, C.; Wassermann, K.; Stollenwerk, B.; Stock, S.; Rhiem, K. Economic modeling of risk-adapted screen-and-treat strategies in women at high risk for breast or ovarian cancer. Eur. J. Health Econ. 2019, 20, 739–750. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Ficarazzi, F.; Vecchi, M.; Ferrari, M.; Pierotti, M.A. Towards population-based genetic screenings for breast and ovarian cancer: A comprehensive review from economic evaluations to patient perspectives. Breast 2021, 58, 121–129. [Google Scholar] [CrossRef]
- Jayasekera, J.; Mandelblatt, J.S. Systematic Review of the Cost Effectiveness of Breast Cancer Prevention, Screening, and Treatment Interventions. J. Clin. Oncol. 2020, 38, 332–350. [Google Scholar] [CrossRef] [PubMed]
- Meshkani, Z.; Aboutorabi, A.; Moradi, N.; Langarizadeh, M.; Motlagh, A.G. Population or family history based BRCA gene tests of breast cancer? A systematic review of economic evaluations. Hered. Cancer Clin. Pract. 2021, 19, 35. [Google Scholar] [CrossRef] [PubMed]
- Sroczynski, G.; Gogollari, A.; Kuehne, F.; Hallsson, L.R.; Widschwendter, M.; Pashayan, N.; Siebert, U. A Systematic Review on Cost-effectiveness Studies Evaluating Ovarian Cancer Early Detection and Prevention Strategies. Cancer Prev. Res. 2020, 13, 429–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenwick, E.; Steuten, L.; Knies, S.; Ghabri, S.; Basu, A.; Murray, J.F.; Koffijberg, H.E.; Strong, M.; Sanders Schmidler, G.D.; Rothery, C. Value of Information Analysis for Research Decisions-An Introduction: Report 1 of the ISPOR Value of Information Analysis Emerging Good Practices Task Force. Value Health 2020, 23, 139–150. [Google Scholar] [CrossRef] [Green Version]
- Rothery, C.; Strong, M.; Koffijberg, H.E.; Basu, A.; Ghabri, S.; Knies, S.; Murray, J.F.; Sanders Schmidler, G.D.; Steuten, L.; Fenwick, E. Value of Information Analytical Methods: Report 2 of the ISPOR Value of Information Analysis Emerging Good Practices Task Force. Value Health 2020, 23, 277–286. [Google Scholar] [CrossRef]
- Strong, M.; Oakley, J.E.; Brennan, A. Estimating multiparameter partial expected value of perfect information from a probabilistic sensitivity analysis sample: A nonparametric regression approach. Med. Decis. Mak. 2014, 34, 311–326. [Google Scholar] [CrossRef] [Green Version]
- Developed for NICE by the National Collaborating Centre for Cancer. Familial Breast Cancer: Full Cost Effectiveness Evidence Review & Reports. Available online: https://www.nice.org.uk/guidance/cg164/update/CG164/documents/familial-breast-cancer-update-full-evidence-review-reports-for-health-economics2 (accessed on 1 June 2021).
- Asphaug, L.; Melberg, H.O. The Cost-Effectiveness of Multigene Panel Testing for Hereditary Breast and Ovarian Cancer in Norway. MDM Policy Pract. 2019, 4, 2381468318821103. [Google Scholar] [CrossRef] [Green Version]
- Breheny, N.; Geelhoed, E.; Goldblatt, J.; O’Leary, P. Cost-Effectiveness of Predictive Genetic Tests for Familial Breast and Ovarian Cancer. Available online: https://lsspjournal.biomedcentral.com/track/pdf/10.1186/1746-5354-1-2-67.pdf (accessed on 1 June 2021).
- Eccleston, A.; Bentley, A.; Dyer, M.; Strydom, A.; Vereecken, W.; George, A.; Rahman, N. A Cost-Effectiveness Evaluation of Germline BRCA1 and BRCA2 Testing in UK Women with Ovarian Cancer. Value Health 2017, 20, 567–576. [Google Scholar] [CrossRef] [Green Version]
- Guzauskas, G.F.; Garbett, S.; Zhou, Z.; Spencer, S.J.; Smith, H.S.; Hao, J.; Hassen, D.; Snyder, S.R.; Graves, J.A.; Peterson, J.F.; et al. Cost-effectiveness of Population-Wide Genomic Screening for Hereditary Breast and Ovarian Cancer in the United States. JAMA Netw. Open 2020, 3, e2022874. [Google Scholar] [CrossRef]
- Holland, M.L.; Huston A Fau-Noyes, K.; Noyes, K. Cost-effectiveness of testing for breast cancer susceptibility genes. Value Health 2009, 12, 207–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurry, M.; Eccleston, A.; Dyer, M.; Hoskins, P. Canadian cost-effectiveness model of BRCA-driven surgical prevention of breast/ovarian cancers compared to treatment if cancer develops. Int. J. Technol. Assess. Health Care 2020, 36, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Kemp, Z.; Turnbull, A.; Yost, S.; Seal, S.; Mahamdallie, S.; Poyastro-Pearson, E.; Warren-Perry, M.; Eccleston, A.; Tan, M.M.; Teo, S.H.; et al. Evaluation of Cancer-Based Criteria for Use in Mainstream BRCA1 and BRCA2 Genetic Testing in Patients with Breast Cancer. JAMA Netw. Open 2019, 2, e194428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, J.S.; Gutierrez-Barrera, A.M.; Young, D.; Sun, C.C.; Daniels, M.S.; Lu, K.H.; Arun, B. Expanding the criteria for BRCA mutation testing in breast cancer survivors. J. Clin. Oncol. 2010, 28, 4214–4220. [Google Scholar] [CrossRef]
- Kwon, J.S.; Tinker, A.V.; Hanley, G.E.; Pansegrau, G.; Sun, S.; Carey, M.S.; Schrader, I. BRCA mutation testing for first-degree relatives of women with high-grade serous ovarian cancer. Gynecol. Oncol. 2019, 152, 459–464. [Google Scholar] [CrossRef]
- Li, Y.; Arellano, A.R.; Bare, L.A.; Bender, R.A.; Strom, C.M.; Devlin, J.J. A Multigene Test Could Cost-Effectively Help Extend Life Expectancy for Women at Risk of Hereditary Breast Cancer. Value Health 2017, 20, 547–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manchanda, R.; Sun, L.; Patel, S.; Evans, O.; Wilschut, J.; de Freitas Lopes, A.C.; Gaba, F.; Brentnall, A.; Duffy, S.; Cui, B.; et al. Economic Evaluation of Population-Based BRCA1/BRCA2 Mutation Testing across Multiple Countries and Health Systems. Cancers 2020, 12, 1929. [Google Scholar] [CrossRef]
- Moya-Alarcon, C.; Gonzalez-Dominguez, A.; Simon, S.; Perez-Roman, I.; Gonzalez-Martin, A.; Bayo-Lozano, E.; Sanchez-Heras, A.B. Cost-utility analysis of germline BRCA1/2 testing in women with high-grade epithelial ovarian cancer in Spain. Clin. Transl. Oncol. 2019, 21, 1076–1084. [Google Scholar] [CrossRef] [Green Version]
- Petelin, L.; Hossack, L.; Shanahan, M.; Mitchell, G.; Liew, D.; James, P.A.; Trainer, A.H. Cost-effectiveness of long-term clinical management of BRCA pathogenic variant carriers. Genet. Med. 2020, 22, 831–839. [Google Scholar] [CrossRef]
- Ramos, M.C.A.; Folgueira, M.; Maistro, S.; Campolina, A.G.; Soarez, P.C.; Bock, G.H.; Novaes, H.M.D.; Diz, M. Cost effectiveness of the cancer prevention program for carriers of the BRCA1/2 mutation. Rev. Saude Publica 2018, 52, 94. [Google Scholar] [CrossRef] [Green Version]
- Simoes Correa-Galendi, J.; del Pilar Estevez Diz, M.; Stock, S.; Müller, D. Economic Modelling of Screen-and-Treat Strategies for Brazilian Women at Risk of Hereditary Breast and Ovarian Cancer. Appl. Health Econ. Health Policy 2021, 19, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Brentnall, A.; Patel, S.; Buist, D.S.M.; Bowles, E.J.A.; Evans, D.G.R.; Eccles, D.; Hopper, J.; Li, S.; Southey, M.; et al. A Cost-effectiveness Analysis of Multigene Testing for All Patients with Breast Cancer. JAMA Oncol. 2019, 5, 1718–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuffaha, H.W.; Mitchell, A.; Ward, R.L.; Connelly, L.; Butler, J.R.G.; Norris, S.; Scuffham, P.A. Cost-effectiveness analysis of germ-line BRCA testing in women with breast cancer and cascade testing in family members of mutation carriers. Genet. Med. 2018, 20, 985–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norum, J.; Grindedal, E.M.; Heramb, C.; Karsrud, I.; Ariansen, S.L.; Undlien, D.E.; Schlichting, E.; Maehle, L. BRCA mutation carrier detection. A model-based cost-effectiveness analysis comparing the traditional family history approach and the testing of all patients with breast cancer. ESMO Open 2018, 3, e000328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoskins, P.; Eccleston, A.; Hurry, M.; Dyer, M. Targeted surgical prevention of epithelial ovarian cancer is cost effective and saves money in BRCA mutation carrying family members of women with epithelial ovarian cancer. A Canadian model. Gynecol. Oncol. 2019, 153, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Tengs, T.O.; Berry, D.A. The Cost Effectiveness of Testing for the BRCA1 and BRCA2 Breast-Ovarian Cancer Susceptibility Genes. Available online: http://www.scopus.com/inward/record.url?scp=0033997009&partnerID=8YFLogxK (accessed on 2 June 2021).
- Carbonara, N.; la Forgia, D.; Pellegrino, R.; Ressa, C.; Tommasi, S. A Cost Decision Model Supporting Treatment Strategy Selection in BRCA1/2 Mutation Carriers in Breast Cancer. J. Pers. Med. 2021, 11, 847. [Google Scholar] [CrossRef] [PubMed]
- Meijers-Heijboer, E.J.; Verhoog, L.C.; Brekelmans, C.T.M.; Seynaeve, C.; Tilanus-Linthorst, M.M.A.; Wagner, A.; Dukel, L.; Devilee, P.; van den Ouweland, A.M.W.; van Geel, A.N.; et al. Presymptomatic DNA testing and prophylactic surgery in families with a BRCA1 or BRCA2 mutation. Lancet 2000, 355, 2015–2020. [Google Scholar] [CrossRef]
- Esteban, I.; Linossi, L.M.C.; Carrasco, E.; Gadea, N.; Bonache, S.; Enriquez, S.G.; Cruz, C.; Diez, O.; Balmaña, J. Evolución del Test Genético de BRCA1 y BRCA2 en Pacientes con Cáncer de Mama u Ovario a lo Largo de una Década. Available online: http://www.postersessiononline.es/312191188_es/congresos/15seom/aula/-P_192_15seom.pdf (accessed on 25 October 2017).
- Chai, X.; Friebel, T.M.; Singer, C.F.; Evans, D.G.; Lynch, H.T.; Isaacs, C.; Garber, J.E.; Neuhausen, S.L.; Matloff, E.; Eeles, R.; et al. Use of risk-reducing surgeries in a prospective cohort of 1,499 BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 2014, 148, 397–406. [Google Scholar] [CrossRef]
- McAlpine, J.N.; Hanley, G.E.; Woo, M.M.; Tone, A.A.; Rozenberg, N.; Swenerton, K.D.; Gilks, C.B.; Finlayson, S.J.; Huntsman, D.G.; Miller, D.M.; et al. Opportunistic salpingectomy: Uptake, risks, and complications of a regional initiative for ovarian cancer prevention. Am. J. Obstet. Gynecol. 2014, 210, 471.e1–471.e11. [Google Scholar] [CrossRef]
- Singh, K.; Lester, J.; Karlan, B.; Bresee, C.; Geva, T.; Gordon, O. Impact of family history on choosing risk-reducing surgery among BRCA mutation carriers. Am. J. Obstet. Gynecol. 2013, 208, 329.e1–329.e6. [Google Scholar] [CrossRef]
- Wainberg, S.; Husted, J. Utilization of screening and preventive surgery among unaffected carriers of a BRCA1 or BRCA2 gene mutation. Cancer Epidemiol. Prev. Biomark. 2004, 13, 1989–1995. [Google Scholar]
- Friebel, T.M.; Domchek, S.M.; Neuhausen, S.L.; Wagner, T.; Evans, D.G.; Isaacs, C.; Garber, J.E.; Daly, M.B.; Eeles, R.; Matloff, E.; et al. Bilateral prophylactic oophorectomy and bilateral prophylactic mastectomy in a prospective cohort of unaffected BRCA1 and BRCA2 mutation carriers. Clin. Breast Cancer 2007, 7, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.; Lynch, H.T.; Ghadirian, P.; Tung, N.; Olivotto, I.; Warner, E.; Olopade, O.I.; Eisen, A.; Weber, B.; McLennan, J.; et al. Contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. J. Clin. Oncol. 2004, 22, 2328–2335. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.A.; Birenbaum-Carmeli, D.; Lubinski, J.; Gronwald, J.; Lynch, H.; Moller, P.; Ghadirian, P.; Foulkes, W.D.; Klijn, J.; Friedman, E.; et al. International variation in rates of uptake of preventive options in BRCA1 and BRCA2 mutation carriers. Int. J. Cancer 2008, 122, 2017–2022. [Google Scholar] [CrossRef] [Green Version]
- Metcalfe, K.A.; Lubinski, J.; Ghadirian, P.; Lynch, H.; Kim-Sing, C.; Friedman, E.; Foulkes, W.D.; Domchek, S.; Ainsworth, P.; Isaacs, C.; et al. Predictors of contralateral prophylactic mastectomy in women with a BRCA1 or BRCA2 mutation: The Hereditary Breast Cancer Clinical Study Group. J. Clin. Oncol. 2008, 26, 1093–1097. [Google Scholar] [CrossRef] [Green Version]
- Uyei, A.; Peterson, S.K.; Erlichman, J.; Broglio, K.; Yekell, S.; Schmeler, K.; Lu, K.; Meric-Bernstam, F.; Amos, C.; Strong, L.; et al. Association between clinical characteristics and risk-reduction interventions in women who underwent BRCA1 and BRCA2 testing: A single-institution study. Cancer 2006, 107, 2745–2751. [Google Scholar] [CrossRef]
- Evans, D.G.; Ingham, S.L.; Baildam, A.; Ross, G.L.; Lalloo, F.; Buchan, I.; Howell, A. Contralateral mastectomy improves survival in women with BRCA1/2-associated breast cancer. Breast Cancer Res. Treat. 2013, 140, 135–142. [Google Scholar] [CrossRef]
- Manchanda, R.; Burnell, M.; Abdelraheim, A.; Johnson, M.; Sharma, A.; Benjamin, E.; Brunell, C.; Saridogan, E.; Gessler, S.; Oram, D.; et al. Factors influencing uptake and timing of risk reducing salpingo-oophorectomy in women at risk of familial ovarian cancer: A competing risk time to event analysis. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 527–536. [Google Scholar] [CrossRef]
- Sidon, L.; Ingham, S.; Clancy, T.; Clayton, R.; Clarke, A.; Jones, E.A.; Lalloo, F.; Evans, D.G. Uptake of risk-reducing salpingo-oophorectomy in women carrying a BRCA1 or BRCA2 mutation: Evidence for lower uptake in women affected by breast cancer and older women. Br. J. Cancer 2012, 106, 775–779. [Google Scholar] [CrossRef] [Green Version]
- Collins, I.M.; Milne, R.L.; Weideman, P.C.; McLachlan, S.A.; Friedlander, M.L.; Hopper, J.L.; Phillips, K.A. Preventing breast and ovarian cancers in high-risk BRCA1 and BRCA2 mutation carriers. Med. J. Aust. 2013, 199, 680–683. [Google Scholar] [CrossRef]
- Metcalfe, K.; Gershman, S.; Ghadirian, P.; Lynch, H.T.; Snyder, C.; Tung, N.; Kim-Sing, C.; Eisen, A.; Foulkes, W.D.; Rosen, B.; et al. Contralateral mastectomy and survival after breast cancer in carriers of BRCA1 and BRCA2 mutations: Retrospective analysis. BMJ 2014, 348, g226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metcalfe, K.A.; Ghadirian, P.; Rosen, B.; Foulkes, W.; Kim-Sing, C.; Eisen, A.; Ainsworth, P.; Horsman, D.; Maugard, C.; Provencher, D.; et al. Variation in rates of uptake of preventive options by Canadian women carrying the BRCA1 or BRCA2 genetic mutation. Open Med. 2007, 1, e92–e98. [Google Scholar] [PubMed]
- Petelin, L.; Hossack, L.; Mitchell, G.; Liew, D.; Trainer, A.H.; James, P.A. A Microsimulation Model for Evaluating the Effectiveness of Cancer Risk Management for BRCA Pathogenic Variant Carriers: miBRovaCAre. Value Health 2019, 22, 854–862. [Google Scholar] [CrossRef]
- Evans, D.G.; Lalloo, F.; Ashcroft, L.; Shenton, A.; Clancy, T.; Baildam, A.D.; Brain, A.; Hopwood, P.; Howell, A. Uptake of risk-reducing surgery in unaffected women at high risk of breast and ovarian cancer is risk, age, and time dependent. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2318–2324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, M.B.; Pilarski, R.; Berry, M.; Buys, S.S.; Farmer, M.; Friedman, S.; Garber, J.E.; Kauff, N.D.; Khan, S.; Klein, C.; et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Breast and Ovarian, Version 2.2017. J. Natl. Compr. Canc. Netw. 2017, 15, 9–20. [Google Scholar] [CrossRef]
- Rhiem, K.; Auber, B.; Briest, S.; Dikow, N.; Ditsch, N.; Dragicevic, N.; Grill, S.; Hahnen, E.; Horvath, J.; Jaeger, B.; et al. Consensus Recommendations of the German Consortium for Hereditary Breast and Ovarian Cancer. Breast Care 2021, 1–9. [Google Scholar] [CrossRef]
- Flippo-Morton, T.; Walsh, K.; Chambers, K.; Amacker-North, L.; White, B.; Sarantou, T.; Boselli, D.M.; White, R.L., Jr. Surgical Decision Making in the BRCA-Positive Population: Institutional Experience and Comparison with Recent Literature. Breast J. 2016, 22, 35–44. [Google Scholar] [CrossRef]
- Balmana, J.; Sanz, J.; Bonfill, X.; Casado, A.; Rue, M.; Gich, I.; Diez, O.; Sabate, J.M.; Baiget, M.; Alonso, M.C. Genetic counseling program in familial breast cancer: Analysis of its effectiveness, cost and cost-effectiveness ratio. Int. J. Cancer 2004, 112, 647–652. [Google Scholar] [CrossRef]
- Gamble, C.; Havrilesky, L.J.; Myers, E.R.; Chino, J.P.; Hollenbeck, S.; Plichta, J.K.; Kelly Marcom, P.; Shelley Hwang, E.; Kauff, N.D.; Greenup, R.A. Cost Effectiveness of Risk-Reducing Mastectomy versus Surveillance in BRCA Mutation Carriers with a History of Ovarian Cancer. Ann. Surg. Oncol. 2017, 24, 3116–3123. [Google Scholar] [CrossRef]
- Patel, S.; Legood, R.; Evans, D.G.; Turnbull, C.; Antoniou, A.C.; Menon, U.; Jacobs, I.; Manchanda, R. Cost effectiveness of population based BRCA1 founder mutation testing in Sephardi Jewish women. Am. J. Obstet. Gynecol. 2018, 218, 431.e1–431.e12. [Google Scholar] [CrossRef]
- Rubinstein, W.S.; Jiang, H.; Dellefave, L.; Rademaker, A.W. Cost-effectiveness of population-based BRCA1/2 testing and ovarian cancer prevention for Ashkenazi Jews: A call for dialogue. Genet. Med. 2009, 11, 629–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manchanda, R.; Legood, R.; Pearce, L.; Menon, U. Defining the risk threshold for risk reducing salpingo-oophorectomy for ovarian cancer prevention in low risk postmenopausal women. Gynecol. Oncol. 2015, 139, 487–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manchanda, R.; Legood, R.; Antoniou, A.C.; Gordeev, V.S.; Menon, U. Specifying the ovarian cancer risk threshold of ‘premenopausal risk-reducing salpingo-oophorectomy’ for ovarian cancer prevention: A cost-effectiveness analysis. J. Med. Genet. 2016, 53, 591–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manchanda, R.; Patel, S.; Antoniou, A.C.; Levy-Lahad, E.; Turnbull, C.; Evans, D.G.; Hopper, J.L.; Macinnis, R.J.; Menon, U.; Jacobs, I.; et al. Cost-effectiveness of population based BRCA testing with varying Ashkenazi Jewish ancestry. Am. J. Obstet. Gynecol. 2017, 217, 578.e1–578.e12. [Google Scholar] [CrossRef]
- Manchanda, R.; Patel, S.; Gordeev, V.S.; Antoniou, A.C.; Smith, S.; Lee, A.; Hopper, J.L.; MacInnis, R.J.; Turnbull, C.; Ramus, S.J.; et al. Cost-effectiveness of Population-Based BRCA1, BRCA2, RAD51C, RAD51D, BRIP1, PALB2 Mutation Testing in Unselected General Population Women. J. Natl. Cancer Inst. 2018, 110, 714–725. [Google Scholar] [CrossRef]
- Zhang, L.; Bao, Y.; Riaz, M.; Tiller, J.; Liew, D.; Zhuang, X.; Amor, D.J.; Huq, A.; Petelin, L.; Nelson, M.; et al. Population genomic screening of all young adults in a health-care system: A cost-effectiveness analysis. Genet. Med. 2019, 21, 1958–1968. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author/Year | Country | Strategies Being Compared | Model Population | RRM Uptake Rate (Age, in Years) | RRSO Uptake Rate (Age, in Years) | Combined RRM and RRSO |
|---|---|---|---|---|---|---|
| Müller 2018 † [9] | Germany | Testing (sequencing of BRCA1/2) vs. no testing | Women at risk for hereditary BC or OC due to family history, entering the model at age 35 | 0.06 (35) | 0.42 (35) | 0.45 (35) |
| Simões Correa Galendi 2020 [33] | Brazil | Testing (sequencing of BRCA1/2) vs. no testing | First-degree relatives of index patients (BC or OC) with BRCA1/2 mutations, entering the model at age 30 | 0.10 (30–34) 0.11 (35–39) 0.07 (40) | 0.27 (30–34) 0.23 (35–39) 0.17 (40) | Not considered |
| Petelin 2020 [31] | Australia | Risk management strategy (including risk-reducing surgeries) vs. population-based breast screening program | BRCA1/2 mutation carriers entering the model at age 20 | 0.31(39) | 0.41 (45) | |
| Manchanda 2020 [29] | United Kingdom/USA/Netherlands China/Brazil India | Testing (sequencing of BRCA1/2) all general population women ≥ 30 years vs. clinical criteria/FH-based testing | Women at risk for having mutations based on clinical and FH, entering the model at age 30 | 0.47 | 0.55 | Not considered |
| Hurry 2020 [24] | Canada | Testing (sequencing of BRCA1/2) vs. no testing | Index patients aged 50; first- and second-degree relatives (daughters entered the model at age 20, sisters at 50) | 0.21 (44) | 0.44 (54) | Not considered |
| Guzauskas 2020 [22] | United States | Population-based testing (sequencing of BRCA1/2) vs. testing based on FH or clinical risk | Women at risk for having mutations based on clinical and FH, entering the model at age 30 or 45 | 0.10 (30–34) 0.11 (35–39) 0.07 (40) | 0.27 (30–34) 0.23 (35–39) 0.17 (40) | Not considered |
| Sun 2019 [34] | United Stated and United Kingdom | Testing (sequencing of BRCA1/2) for all women with BC vs. based on FH or clinical risk | Index patients (BC); first-degree relatives of index patients with BRCA1/2 mutations, entering the model at different ages ¥ | 0.47(30) | 0.55 (30) | Not considered |
| Moya-Alarcón 2019 [30] | Spain | Testing (sequencing of BRCA1/2) vs. no testing | Index patients at age 51 (OC); first- and second-degree relatives (daughters, nephews and nieces entered the model at age 23) | 0.25 (45–55) | 0.65 (45–55) | Not considered |
| Kwon 2019 [27] | Canada | Testing followed by RRSO (Sequencing of BRCA1/2) vs. no testing vs. RRSO for all (without testing) | First-degree relatives of index patients (OC), entering the model at age 40 | Not considered | 0.54 (40–50) | 0.33 (40–50) |
| Kemp 2019 [25] | United Kingdom | Testing (sequencing of BRCA1/2) vs. no testing | Index patients aged 50 years (BC); first- and second-degree relatives (daughters entered the model at age 20, sisters at 50) | BRCA1 0.34 (40) BRCA2 0.25 (40) | BRCA1 0.88 (40) BRCA2 0.87 (40) | Not considered |
| Asphaug 2019 [19] | Norway | Full sequencing of BRCA1/2 vs. seven-gene panel vs. 14-gene panel | Index patients aged 55 years (BC); first-degree relatives (daughters entered the model at age 25 and sisters at 55) | 0.12 (25–34) 0.11 (35–60) | 0.10 (25–34) 0.28 (35–39) 0.35 (40–60) | Not considered |
| Tuffaha 2018 [35] | Australia | Testing (sequencing of BRCA1/2) vs. no testing | Index patients at age 40 (BC) with 10% probability for BRCA1/2 mutations; first- and second-degree relatives (children entered the model at age 10, siblings at age 40) | 0.3 (40) | 0.54 (40) | 0.16 (40) |
| Ramos 2018 [32] | Brazil | Testing (sequencing of BRCA1/2) vs. no testing | First-degree female relatives of index patients (OC) with BRCA1/2 mutations, entering the model at age 30 | 0.18 (30) | 0.57 (30) | Not considered |
| Li 2017 [28] | United States | Full sequencing of BRCA1/2 vs. five-gene panel | Women at risk for hereditary BC or OC due to family history or other hereditary syndromes, entering the model at age 40 or 50 | 0.42 (50) | Not considered | Not considered |
| Eccleston 2017 [21] | United Kingdom | Testing (sequencing of BRCA1/2) vs. no testing | Index patients age 50 years (OC) First- and second-degree relatives (daughters entered the model at age 20, sisters at 50) | BRCA1 0.34 (40) BRCA2 0.25 (40) | BRCA1 0.88 (40) BRCA2 0.87 (40) | Not considered |
| NICE 2013 [18] | United Kingdom | Testing (sequencing of BRCA1/2) vs. no testing | First-degree female relatives of index patients (BC or OC) with BRCA1/2 mutations, entering the model at different ages 20–70 | 0.42 (30) | 0.54 (35) | 0.15 |
| Kwon 2010 [26] | Canada | Testing (different criteria for sequencing of BRCA1/2) vs. no testing | Subgroups of women with BC before age 40 or 50, regardless of ethnicity of family history | 0.20 (50–55) § | 0.55 (50–55) | Not considered |
| Holland 2009 [23] | United States | Testing (sequencing of BRCA1/2) vs. no testing | Women with 10% pre-test probability of having a mutation, ‡ who entered the model at age 35 | 0.15 (35) | 0.25 (35) | Not considered |
| Breheny 2005 [20] | Australia | Testing (sequencing of BRCA1/2) vs. no testing | First-degree relatives of individuals with BRCA1/2 mutations, entering the model at age 25 | 0.30 (38) | - | Not considered |
| Author/Year | Source of Uptake Rate (Year) | Study Design | Country | Number of Participants | Follow-Up |
|---|---|---|---|---|---|
| Müller 2018 † [9] | Unpublished | Cross-sectional (single-center, hypothetical responses of women in a counseling situation) | Germany | 136 women at different ages following individual genetic counseling | - |
| Simões Correa Galendi 2020 [33] | Chai (2014) [42] | Prospective, multi-center (post-testing counseling) | United States, United Kingdom | 1499 healthy women with inherited BRCA1/2 mutations | At least 0.5 years |
| Petelin 2020 [31] | Petelin (2019) [57] | Prospective and retrospective collected clinical data from a single specialized cancer center | Australia | 983 women with BRCA1/2 mutations (302 had BC at diagnosis) | 6.5 years |
| Manchanda 2020 [29] | Evans (2009) [58] | Matched controls (regional cancer registries) | United Kingdom | 221 healthy women with known BRCA1/2 mutations | 7 years |
| Hurry 2020 [24] | RRM: Metcalfe (2007) [56] RRSO: McAlpine (2014) [43] | Retrospective (databases of mutation carriers Hospital discharges (RRSO) | Canada | RRM: 342 women with BRCA mutations, healthy and previous BC RRSO: 2119 who underwent hysterectomy (with or without BSO) or BSO or sterilization | RRM: 4 years RRSO: |
| Guzauskas 2020 [22] | Chai (2014) [42] | Prospective, multi-center (post-testing counseling) | United States, United Kingdom | 1499 healthy women with inherited BRCA1/2 mutations | At least 6 months |
| Sun 2019 [34] | RRM: Evans (2009) [58] RRSO: Manchanda (2012) [52] | Matched controls (regional cancer registries) Prospective observational cohort | United Kingdom | RRM: 105 women with BRCA mutations (healthy and BC) RRSO: 1133 women at high risk, less than 50% had BRCA mutations | 7 years 6 years |
| Moya-Alarcón 2019 [30] | Esteban (2015) [41] | Retrospective (hospital data) | Spain | 969 women from 682 families | |
| Kwon 2019 [27] | Metcalfe (2008) [48] | Retrospective (multicenter study, questionnaire after receiving genetic test) | United States | RRSO: 703 women, healthy and with previous BC with BRCA mutations | 3.9 years |
| Kemp 2019 [25] | - | Retrospective (unpublished single hospital data) | United Kingdom. | 858 women with BRCA mutations (unclear if previous cancer diagnosis) | - |
| Asphaug 2019 [19] | Metcalfe (2008) [48] | Retrospective (multi-center, questionnaire after receiving genetic test) | Austria, Canada, France, Israel, Italy, Norway, Poland, United States | RRM: 1290 RRSO: 177 women, healthy and with previous BC with BRCA mutations | 3.9 years |
| Tuffaha 2018 [35] | Collins (2013) [54] | Prospective (multicenter, interviewer-administered questionnaire, surgery confirmed from pathology and medical records) | Australia | 325 healthy women with inherited BRCA mutations | 3 years |
| Ramos 2018 [32] | Metcalfe (2008) [48] | Retrospective (multicenter, questionnaire after receiving genetic test) | Various, Canada | RRM: 766/RRSO: 1383 women, healthy and with previous BC, with BRCA mutations | 3.9 years |
| Li 2017 [28] | Singh (2013) [44] | Retrospective (registry data) | United States | 136 women with inherited BRCA mutations without previous cancer diagnosis | 1–11 years |
| Eccleston 2017 [21] | - | Retrospective (unpublished single hospital data) | United Kingdom | 858 women with BRCA mutations (unclear if previous cancer diagnosis) | - |
| NICE 2013 [18] | RRM: Evans (2009) [58] RRSO: Sidon (2012) [53] RRSO/RRM: Uyei (2006) [50] | Matched controls (regional cancer registries) Retrospective (regional cancer registries) Retrospective (medical records) | United Kingdom | RRM: 105 RRSO: 314 RRM/RRSO: 554 All women with BRCA mutations, healthy or with BC | 7 years 5 years 6 years |
| Kwon 2010 [26] | RRM: Metcalfe (2004) [47] | Retrospective (medical records) | United States, the Netherlands | Metcalfe (2004): 390 women with early-stage BC, who are known carriers or are likely to carry BRCA1/2 mutations and were treated with unilateral mastectomy Other studies: healthy women with BRCA mutations and diagnosis of BC | 9 years |
| RRSO: Friebel (2007) [46] | Prospective (questionnaire, medical records) | ||||
| Meijers-Heijboer (2000) [40] | Prospective (single-center, hospital data) | ||||
| Metcalfe (2008) [48] | Retrospective (multicenter, questionnaire after receiving genetic test) | ||||
| Metcalfe (2008) [49] | Prospective (multicenter, questionnaires) | ||||
| Holland 2009 [23] | Weinberg (2004) [45] | Meta-analysis (five studies for uptake of BC, six studies for uptake of OC) | Various | 354 healthy, pre-symptomatic women who knew their mutation status and who had no prior history of BC or OC | |
| Breheny 2005 [20] | - | Provided abbreviation not identifiable | - | - |
| Author/Year | Strategies Being Compared | ICER | Deterministic Sensitivity Analysis (Impact on the ICER by Varying the Uptake Rates) |
|---|---|---|---|
| Müller 2018 † [9] | Testing vs. no testing | EUR 17,027/QALY | 5% lower uptake of RRSO and RRSO combined with RRM increased ICER by 70%. |
| Simões Correa Galendi 2020 [33] | Testing vs. no testing | BRL 24,264/QALY (USD 11,726/QALY) | 10% lower uptake rates of all risk-reducing surgeries increased the ICER by 10%; 20% lower uptake rates of all RR surgeries increased the ICER by 30%. |
| Petelin 2020 [31] | Risk management strategy vs. population-based breast screening program | AUD 32,359/QALY (BRCA1) AUD 48,263/QALY (BRCA2) | At a 75% reduced uptake of RRSO, the ICER increased by 25% and 15% for BRCA1 and BRCA2 mutation carriers, respectively. At a 75% reduced uptake of RRM, the ICER decreased by 1% and 17% for BRCA1 and BRCA2 mutation carriers, respectively. |
| Manchanda 2020 [29] | Populational testing vs. clinical criteria/FH-based testing | UK: USD 21,191/QALY USA: USD 16,552/QALY NL: USD 25,215/QALY China: USD 23,485/QALY Brazil: USD 20,995/QALY India: USD 32,217/QALY | Half the uptake rate for RRM or RRSO increased the ICER by about 5%. |
| Hurry 2020 [24] | Testing vs. no testing | CAD 14,294/QALY (USD 10,555/QALY) | 50% increase in RRS uptake rates (RRSO 0.66 and RRM 0.32), and mean age of RRSO 50 years reduced the ICER 85%. |
| Guzauskas 2020 [22] | Population-based testing vs. testing based on FH or clinical risk | USD 87,700/QALY | Considering an uptake rate of RRSO or RRM of 50% lower (or 50% higher) increased (or reduced) the ICER by 10%. |
| Sun 2019 [34] | Testing for all women with BC vs. based on FH or clinical risk | UK: GBP 10,464/QALY USA: USD 65,661/QALY | 10% higher uptake of RRSO reduced the ICER by 10%, and 10% lower uptake increase the ICER by 10% (for the UK payer perspective); 10% higher uptake of RRSO increased the ICER by 5%, 10% lower uptake decreased the ICER by 40% (for the US payer perspective). |
| Moya-Alarcón 2019 [30] | Testing vs. no testing | EUR 31,621/QALY | Considering an uptake rate of RRSO or RRM 25% lower (or 25% higher) increased (or reduced) the ICER by 5%. |
| Kwon 2019 [27] | Testing followed by RRSO vs. no testing | USD 7888 per QALY | Not reported |
| Kemp 2019 [25] | Testing vs. no testing | USD 1330/QALY | Not reported |
| Asphaug 2019 [19] | Full sequencing of BRCA1/2 vs. seven-gene panel vs. 14-gene panel | USD 53,310/QALY | Considered negligible by the author. |
| Tuffaha 2018 [35] | Testing vs. no testing | AUD 18,900 | Significant Reducing the uptake rates by 10%, the ICER increased 40–50%. |
| Ramos 2018 [32] | Testing vs. no testing | BRL 908/case of cancer avoided | Not reported |
| Li 2017 [28] | Full sequencing of BRCA1/2 vs. five-gene panel | USD 69,920/QALY | Considering an uptake rate of RRM 50% lower (or 50% higher) increased the ICER by 50% (or reduced the ICER by 40%). |
| Eccleston 2017 [21] | Testing vs. no testing | GBP 4339/QALY | Considering an uptake rate of RRSO 75% lower increased the ICER by 40%. Considering an uptake rate of RRM 50% higher decreased the ICER by 23%. |
| NICE 2013 [18] | Testing vs. no testing | GBP 18,114/QALY § | Considered negligible by the author. |
| Kwon 2010 [26] | Testing vs. no testing | USD 9084/QALY | The ICER increased about 30% when applying a realistic scenario (40% choose no procedure) over an ideal scenario (100% uptake). |
| Holland 2009 [23] | Testing vs. no testing | USD 9000/QALY | The ICER decreased as the rate of RRM increased and dominated above an 80% RRM rate. Higher rates (until 60%) of RRSO also decreased the ICER, and higher than 60%, the incremental benefits decreased faster than the incremental costs, increasing the ICER. |
| Breheny 2005 [20] | Testing (sequencing of BRCA1/2) vs. no testing | USD 477/cancer-free year gained (BRCA1) USD 2150/cancer-free year gained (BRCA2) | Varying the uptake rate of RRM from 0% to 50%, the latter reduced the ICER by 10%. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simões Corrêa Galendi, J.; Kautz-Freimuth, S.; Stock, S.; Müller, D. Uptake Rates of Risk-Reducing Surgeries for Women at Increased Risk of Hereditary Breast and Ovarian Cancer Applied to Cost-Effectiveness Analyses: A Scoping Systematic Review. Cancers 2022, 14, 1786. https://doi.org/10.3390/cancers14071786
Simões Corrêa Galendi J, Kautz-Freimuth S, Stock S, Müller D. Uptake Rates of Risk-Reducing Surgeries for Women at Increased Risk of Hereditary Breast and Ovarian Cancer Applied to Cost-Effectiveness Analyses: A Scoping Systematic Review. Cancers. 2022; 14(7):1786. https://doi.org/10.3390/cancers14071786
Chicago/Turabian StyleSimões Corrêa Galendi, Julia, Sibylle Kautz-Freimuth, Stephanie Stock, and Dirk Müller. 2022. "Uptake Rates of Risk-Reducing Surgeries for Women at Increased Risk of Hereditary Breast and Ovarian Cancer Applied to Cost-Effectiveness Analyses: A Scoping Systematic Review" Cancers 14, no. 7: 1786. https://doi.org/10.3390/cancers14071786