1. Introduction
Diffuse large B-cell lymphoma (DLBCL) is the commonest subtype of non-Hodgkin lymphoma (NHL), accounting for approximately 30–40% of adult cases [
1]. The gold standard treatment is immunochemotherapy with rituximab, cyclophosphamide, doxorubicin hydrochloride, vincristine (Oncovin) and prednisolone (RCHOP) [
2]. Radiotherapy can be added if there is bulky or residual disease. Prophylactic intrathecal methotrexate or intravenous treatment with chemotherapy that crosses the blood-brain barrier may be included if there is high risk for central nervous system (CNS) involvement [
3]. Even with current therapy regimes, approximately 20–30% of patients will recur following treatment [
4,
5]. Staging and response assessment is performed using 2-deoxy-2-[fluorine18]-fluoro-D-glucose (FDG) positron emission tomography/computed tomography (PET/CT). Treatment stratification based on mid-treatment (interim) PET/CT is commonly used in the management of patients with Hodgkin lymphoma but is less established in DLBCL due to the reduced ability to accurately predict treatment outcome in this lymphoma subtype mid-treatment [
6,
7]. There is increasing interest in the use of PET/CT derived metrics for treatment stratification at baseline in lymphoma to improve patient outcome. A number of groups have explored the potential utility of baseline metabolic tumour volume (MTV) for predicting event free survival (EFS) with promising results, but this has yet to be adopted clinically [
8,
9,
10,
11,
12,
13,
14,
15,
16,
17]. Others have explored the potential utility of radiomic features extracted from PET/CT for modelling purposes [
8,
18]. Initial results are promising, however, the published studies with relatively small numbers of patients are heterogenous
This aim of this study was to develop and test models combining baseline clinical information and radiomic features extracted from PET/CT imaging in DLBCL patients to predict 2-year EFS (2-EFS) using data from our tertiary centre. The secondary aim was to compare model performance to the predictive ability of baseline MTV.
2. Materials and Methods
The transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD) guidelines were adhered to as part of this study (
Supplementary Material).
2.1. Patient Selection
Radiological and clinical databases were retrospectively reviewed to identify patients who underwent baseline PET/CT for DLBCL at our institution between January 2008 and January 2018. A cut-off of January 2018 was chosen to allow a minimum of 2 years follow up without interference or confounding factors introduced by the COVID-19 pandemic. Patients were excluded if they did not have DLBCL, were under 16 years of age, had no measurable disease on PET/CT, had hepatic involvement, had a concurrent malignancy, were not treated with R-CHOP or if the images were degraded or incomplete. A 2-EFS event was defined as disease progression, recurrence or death from any cause within the 2-year follow up period.
2.2. PET/CT Acquisition
All imaging was performed as part of routine clinical practice. Patients fasted for 6 h prior to administration of intravenous Fluorine-18 FDG (4 MBq/kg). PET acquisition and reconstruction parameters for the four scanners used at our institution are detailed in
Table 1. Attenuation correction was performed using a low-dose unenhanced diagnostic CT component acquired using the following settings: 3.75 mm slice thickness; pitch 6; 140 kV; 80 mAs.
2.3. Image Segmentation
All PET/CT images were reviewed and contoured using a specialised multimodality imaging software package (RTx v1.8.2, Mirada Medical, Oxford, UK). FDG-positive disease segmentation was performed by either a clinical radiologist with six years’ experience or a research radiographer with two years’ experience. Contours were then reviewed by dual-certified Radiology and Nuclear Medicine Physicians with >15 years’ experience of oncological PET/CT interpretation. Any discrepancies were agreed by consensus.
Two different semi-automated segmentation techniques were used. The first applied a fixed standardised uptake value (SUV) threshold of 4.0, and the second used a threshold derived from 1.5 times mean liver SUV. The 4.0 SUV threshold was selected based on previous work assessing different segmentation techniques in a cohort of DLBCL patients by Burggraaff et al. which found it had a higher interobserver reliability [
19] and requires less adaption than techniques such as 41% SUVmax. The 1.5 times mean liver SUV threshold was chosen as an adaptive threshold technique which has been used in different cancer types [
20,
21], and allows for adaptive thresholding which takes into consideration background SUV uptake which can vary between individuals. Mean liver SUV was calculated by placing a 110 cm
3 spherical region of interest (ROI) in the right lobe of the liver. The PET image contour was translated to the CT component of the study with the contours matched to soft tissue with a value of −10 to 100 Hounsfield units (HU). Contours were saved and exported as digital imaging and communications in medicine (DICOM) radiotherapy (RT) structures. Both the images and contours were converted to Neuroimaging Informatics Technology Initiative (NIfTI) files using the python library Simple ITK (v2.0.2) (
https://simpleitk.org/, accessed on 1 December 2021).
2.4. Feature Extraction
Feature extraction was performed using PyRadiomics (v2.2.0) (
https://pyradiomics.readthedocs.io/en/latest/index.html, accessed on 1 December 2021). Both the CT and PET images were resampled to a uniform voxel size of 2 mm
3. Radiomic features were extracted from the entire segmented disease for each patient. A fixed bin width of 2.5 HU was used for the CT component. Two different bin-widths were used when extracting the radiomic features from the PET component. The first being derived by finding the contour with the maximum range of SUVs and dividing this by 130, the second being derived by dividing the maximum range by 64. This methodology was based on previous work by Orlhac et al. and on PyRadiomics documentation [
22]. The first and second order features were extracted from both the PET and CT components. Further higher order features were explored by extracting the first and second order features following application of wavelet, log-sigma, square, square root, logarithm, exponential, gradient and local binary pattern (lbp)-3D filters to the images. All the features extracted and the filters applied are detailed in
Table S1. The mathematical definition of each of the radiomic features can be found within the PyRadiomics documentation [
23]. PyRadiomics deviates from the image biomarker standardisation initiative (IBSI) by applying a fixed bin width from 0 and not the minimum segmentation value, and the calculation of first order kurtosis being +3 [
24,
25]. Otherwise, PyRadiomics adheres to IBSI guidelines. Patient age, disease stage and sex were also included as clinical features in the models. Disease stage and sex were dummy encoded using Pandas (v1.2.4) (
https://pandas.pydata.org/pandas-docs/stable/whatsnew/v1.2.4.html, accessed on 1 December 2021). This resulted in a total of 3935 features extracted per patient. ComBat harmonisation was applied to account for the different scanners used within the study (
https://github.com/Jfortin1/ComBatHarmonization, accessed on 1 December 2021) [
26].
2.5. Machine Learning
The dataset was split into a training and test set stratified around 2-EFS, disease stage, age and sex with an 80:20 split using scikit-learn (v0.24.2) (
https://scikit-learn.org/stable/whats_new/v0.24.html, accessed on 1 December 2021). Concordance between the demographics of the training and test groups was assessed using a
t-test for continuous data and a χ
2 test for categorical data. A
p-value of <0.05 was regarded as significant. Continuous data was normalised using a standard scaler (scikit-learn v0.24.2) which was trained and fit on the training set and subsequently applied to the test set. Highly correlated features were removed from the training and test sets if they had a Pearson coefficient over 0.8. This reduced the number of features from 3935 down to 130 for each patient.
Six different machine learning (ML) classifiers were used: logistic regression with lasso, ridge and elasticnet penalties, support vector machine (SVM), random forest and k-nearest neighbour. A maximum number of five features were included within each model, apart from in the lasso and elasticnet models where these classifiers determined the optimum number of features. To avoid false discoveries (Type 1 errors), a maximum number of five features was chosen guided by the rule of 1 feature per 10 events within the training set. Feature selection for the remaining models was performed using three different methods: a forward wrapper method (mlxtend 0.18.0), a univariate analysis method (scikit-learn v0.24.2), and a recursive feature extraction method (where applicable) (scikitlearn v0.24.2). Each method was used to create a list of features from two to the maximum five features which were to be explored in the training phase. The features selected were based on the highest mean receiver operating characteristic (ROC) curve area under the curve (AUC) in a four-fold stratified cross validation with 25 repeats.
Training of the ML models and the tuning of hyperparameters was performed using a grid search with a stratified four-fold cross validation stratified around 2-EFS with 25 repeats. The list of hyperparameters explored within the grid search are detailed in
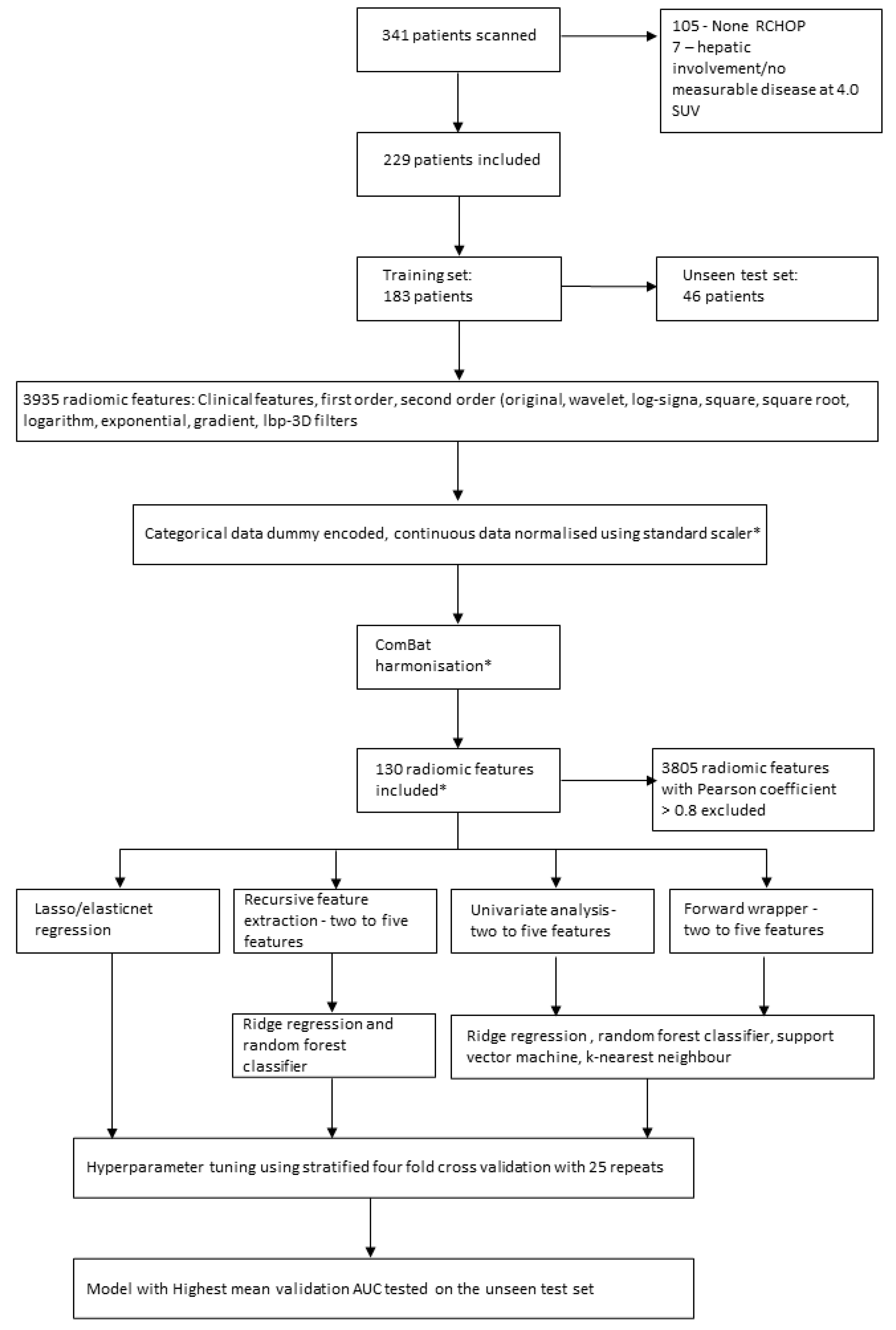
Table S2. Features and hyperparameters with the highest mean validation AUC which was within 0.05 of the mean training AUC were selected. A 0.05 cut-off was chosen to try and minimise selection of an overfitted model. The model which had the highest mean validation AUC overall was tested once on the unseen test set. The Youden index was used to discover the optimum cut-off value from the ROC curve and the accuracy, sensitivity, specificity, negative predictive value (NPV) and positive predictive value (PPV) were calculated from this for the unseen test set. The pipeline for patient inclusion, feature selection and predictive model creation and testing is depicted in
Figure 1.
Given the growing evidence surrounding MTV as a predictor of outcome, two further logistic regression models were derived from the MTVs using the different segmentation. A comparison between results from the different cross validation splits between the radiomic model with the mean highest AUC and the MTV model with the mean higher AUC was performed using a Wilcoxon signed ranked test.
3. Results
A total of 229 DLBCL patients met the inclusion criteria (136 male, 93 female) with 62 2-EFS events. There were 183 patients within the training cohort and 46 patients in the unseen test cohort. No statistically significant differences were identified between the training and test sets (
Table 2).
None of the machine learning models created using elasticnet regression, lasso regression or k-nearest neighbour algorithms had a mean validation AUC within 0.05 of the mean training AUC. The remaining model results are presented in
Table 3 and
Table 4.
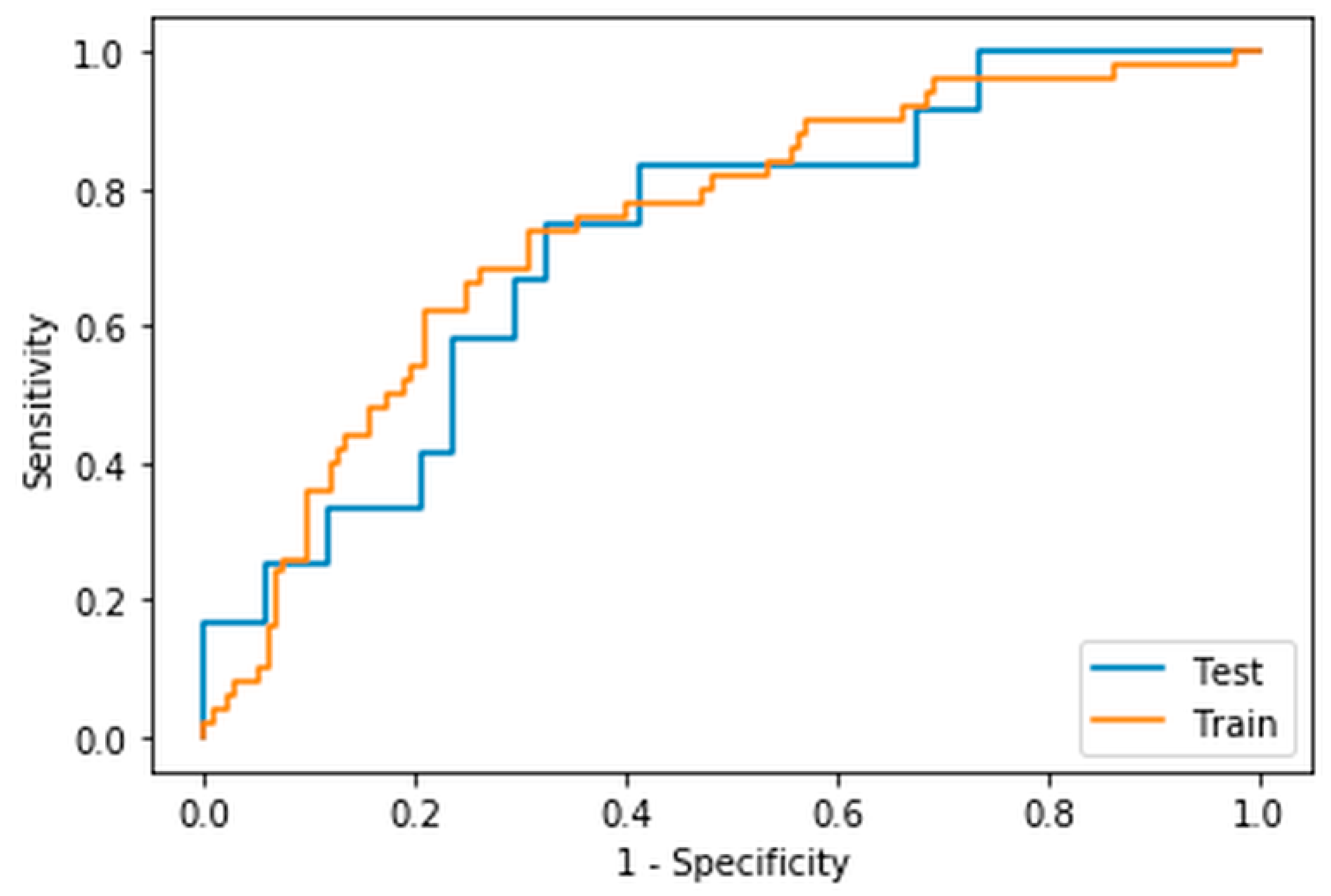
The model within the highest mean validation ROC AUC was the ridge regression model created using radiomic features extracted from a fixed threshold of 4.0 SUV segmentation using a bin width of the maximum range of SUVs divided by 64. The mean training AUC was 0.77 ± 0.02, the mean validation AUC was 0.75 ± 0.06 and the AUC when tested on the unseen dataset was 0.73 (
Figure 2). The features selected with their coefficients and intercept are presented in
Table 5. A threshold of 0.5 was chosen and led to an accuracy of 0.70, sensitivity of 0.44, specificity of 0.86, positive predictive value of 0.67, and a negative predictive value of 0.71. The confusion matrix is presented in
Table 6.
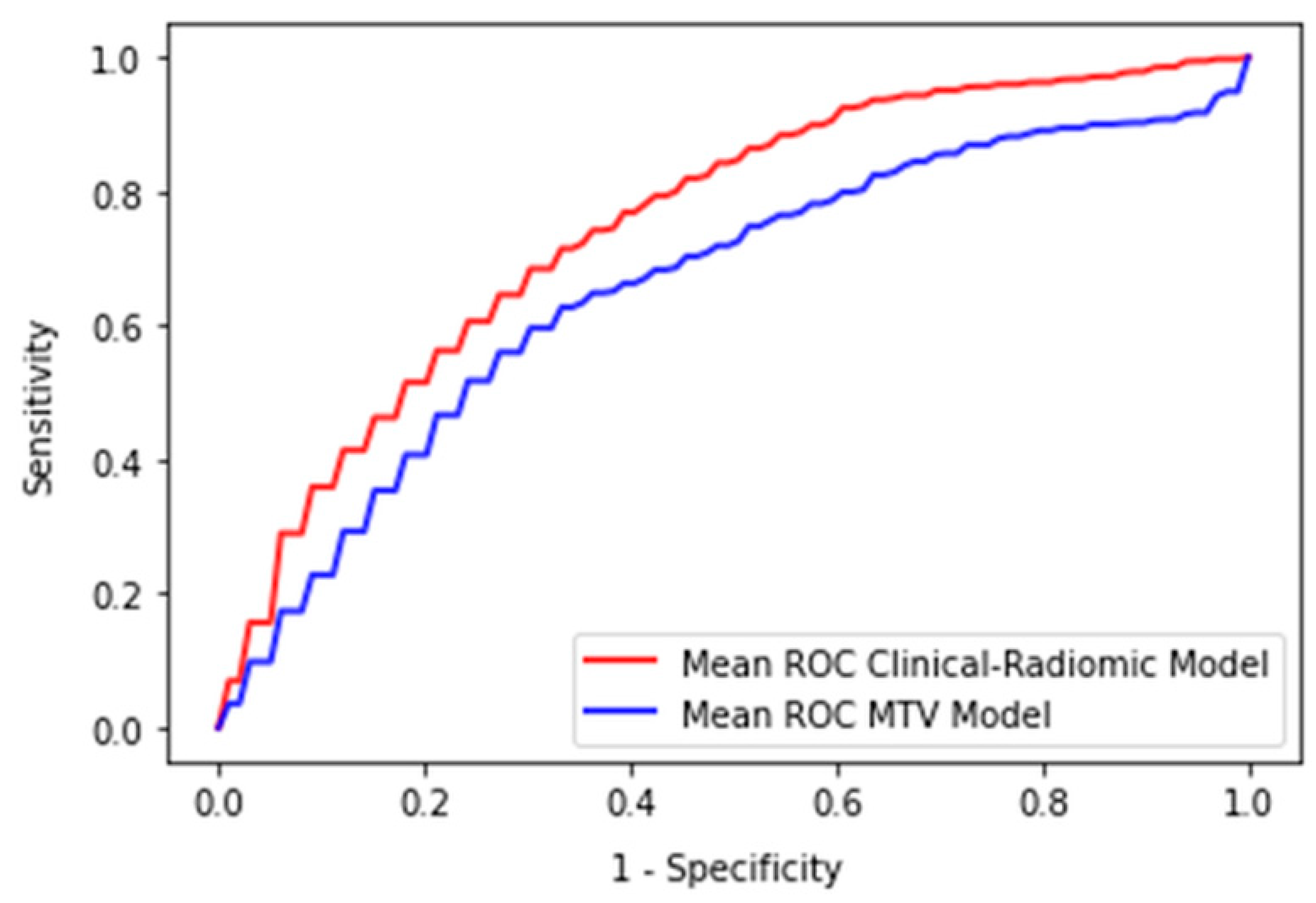
The logistic regression model created solely from MTV using the 4.0 SUV fixed threshold segmentation technique had a mean training AUC of 0.66 ± 0.03 and a mean validation AUC of 0.66 ± 0.08. The logistic regression model derived from MTV using the 1.5 times mean liver SUV segmentation technique had a mean training AUC of 0.67 ± 0.03 and a mean validation AUC of 0.67 ± 0.08. There was a statistically significant difference when comparing the cross validation AUCs for the 100 splits between the highest performing MTV-based model and the radiomic-based ridge regression model,
p < 0.001 (
Figure 3).
4. Discussion
Our study found that a prediction model combining clinical and radiomic features derived from pretreatment PET/CT using a ridge regression model had the highest mean validation AUC when predicting 2-EFS in DLBCL patients. This model had significantly higher validation AUCs than those achieved by a model solely derived from MTV and achieved an AUC of 0.73 on the unseen test set. The radiomic features used within the model that led to the highest mean validation AUC were extracted from a segmentation derived from a fixed threshold of 4.0 SUV using a bin-width calculated from the maximum range of SUVs divided by 64. The model was formed using five features (Stage Four, PET original GLSZM large area emphasis, PET wavelet-HHL GLSZM Small Area Emphasis, PET wavelet-HHH GLSZM Grey Level Non-Uniformity normalised, PET square 10th percentile).
The biological correlate of radiomic features and how these relate to the lesion or disease process can often be overlooked, and can become more complex when image filtering is involved [
27]. Three of the radiomic features included in the best model were derived from GLSZM which is a matrix formed by the number of connected voxels with the same grey level intensity. The first was the PET GLSZM Large Area Emphasis, which is a measure of distribution of large area size zones, and was extracted from the PET data without any filter applied. This feature is higher in lesions which have a coarser texture based on the original image. The other two GLZMs are calculated after applying a wavelet filter. Wavelet filters highlight or suppress certain spatial frequencies within an image. In PyRadiomics a combination of high and low filters is passed in each of the different dimensions, which results in eight different decompositions. PET wavelet-HHL GLSZM Small Area Emphasis is a measure of the distribution of small size zones, which are higher in lesions with fine textures following the application of the wavelet filter. PET wavelet-HHH GLSZM Grey Level Non-Uniformity is a measure of the variability of the grey level intensity within the image. A lower value indicates a higher number of similar SUVs on the wavelet filtered image. The last radiomic feature included was PET square 10th percentile which is the 10th percentile value of the SUV after a square of the image SUVs has been taken and normalised to the original SUV range. Interestingly, none of the CT-derived radiomic features were selected as part of the best performing radiomic models. This is likely due to the transposition of the segmentations from the PET on to the unenhanced CT including more areas of non-lymphomatous tissue.
Other studies which have explored the use of radiomic features in outcome prediction in DLBCL are not always directly comparable [
12,
28,
29,
30,
31,
32]. This is mainly due to differences in segmentation methodology, modelling techniques and outcome measures between groups. Aide et al. studied the use of radiomic features in predicting 2-EFS in 132 patients (training = 105, validation = 27) and found that MTV as well as four second-order metrics and five third-order metrics were selected from ROC analyses. However, long-zone high-grey level emphasis was the only independent predictor when analysed with the international prognostic index (IPI) and MTV [
29]. In our study long-zone high-grey level emphasis was discarded when checking for multicollinearity. This highlights a potential issue of radiomic model development when applying a methodology on different datasets. It may be that the same features would be chosen between the different datasets, but each method removes the alternate correlated feature and, therefore, appears to create an entirely new model. Both Zhang et al. and Ceriani et al. used lasso in their cox regression models to select the most appropriate features [
31,
32]. Zhang et al. in a study of 152 patients (training = 100, validation = 52) treated with R-CHOP or R-EPOCH (rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin) found that a survival model created with radiomic features and MTV had a validation time dependent ROC AUC of 0.748 (95% CI 0.596–0.886). A model created with radiomic features and metabolic bulk volume had a validation time dependent ROC AUC 0.759 (95% CI 0.595–0.888). Ceriani et al. reported that a radiomic score derived from a training set of 133 patients and tested on an external dataset of 107 patients had an AUC of 0.71 in both the test and validation datasets. The features selected within their cox regression model were GLCM sum squares, maximum 3D diameter and GLDM grey level variance, GLSZM grey level non-uniformity normalised.
In our study both lasso and elasticnet methods failed to produce a model that achieved mean training and validation scores within 0.05 of each other. Even when allowing for a more generous difference between the training and validation scores, mean validation scores remained below 0.65. This 0.05 cut-off is arbitrary and was applied to try and reduce the impact of overfitting on the dataset and allow selection of a potentially more generalisable model. Despite this, there is still a risk that both training and validation datasets are overfitted and the model would need external validation on an external dataset.
One of the largest published studies by Decazes et al. in 215 DLBCL patients, explored use of tumour volume surface ratio and total tumour surface as outcome predictors for 5-year progression free survival (PFS), but found that MTV outperformed both features with MTV having an AUC of 0.67 [
12]. This AUC for MTV is similar to the findings in our study, with the mean validation AUC for MTV prediction of 2-EFS being 0.66 for the 4.0 SUV threshold and 0.67 for the 1.5 times liver threshold segmentation techniques, respectively. Although, there is growing interest in the use of MTV as an imaging biomarker, Adams et al. reported, in a study of 73 DLBCL patients, that the prognostic ability of MTV does not add anything to the prognostic ability of the clinical scoring system National Comprehensive Cancer Network-International Prognostic Index (NCCN-IPI) [
33]. Unfortunately, due to missing clinical data it was not possible to compare IPI performance in our patient cohort. However, this does highlight the potential impact of confounders on the generalisability of predictive models. Although, causality is not generally considered in predictive modelling, its use in future models could allow for greater transparency of a model. The issues of generalisability may be compounded by learnt biases towards groups of patients in the training process.
The TRIPOD checklist was completed to increase transparency of model development [
34,
35]. However, there are limitations to our study including its retrospective nature and uncertainty surrounding the exact timing and recording of recurrence. Use of 2-EFS partially mitigates against this by allowing a wider window for the relapse to be recorded, however, it does mean that data which could have been included in a time to survival type model is lost. 2-EFS was chosen as the majority of patients relapse within the first 2 years. Time to event ML models could be used in future studies to reduce the need to exclude data. The lesions were not re-segmented as part of the study, and therefore, calculations of inter or intra-reliability, as well as robustness of the features have not been performed. ComBat harmonization was used to help mitigate against scanner variation in the extracted feature extraction. However, this limits the ability to apply this model prospectively to patients not scanned using a protocol used to train the model. Lack of clinical data surrounding the IPI and cell of origin (COO) information, meant that these could not be used as direct comparators to radiomic models created.


 ,
, 



{kind=link}
{kind=link}
{kind=link}