
Hyperspectral Imaging for Tissue Classification after Advanced Stage Ovarian Cancer Surgery—A Pilot Study

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
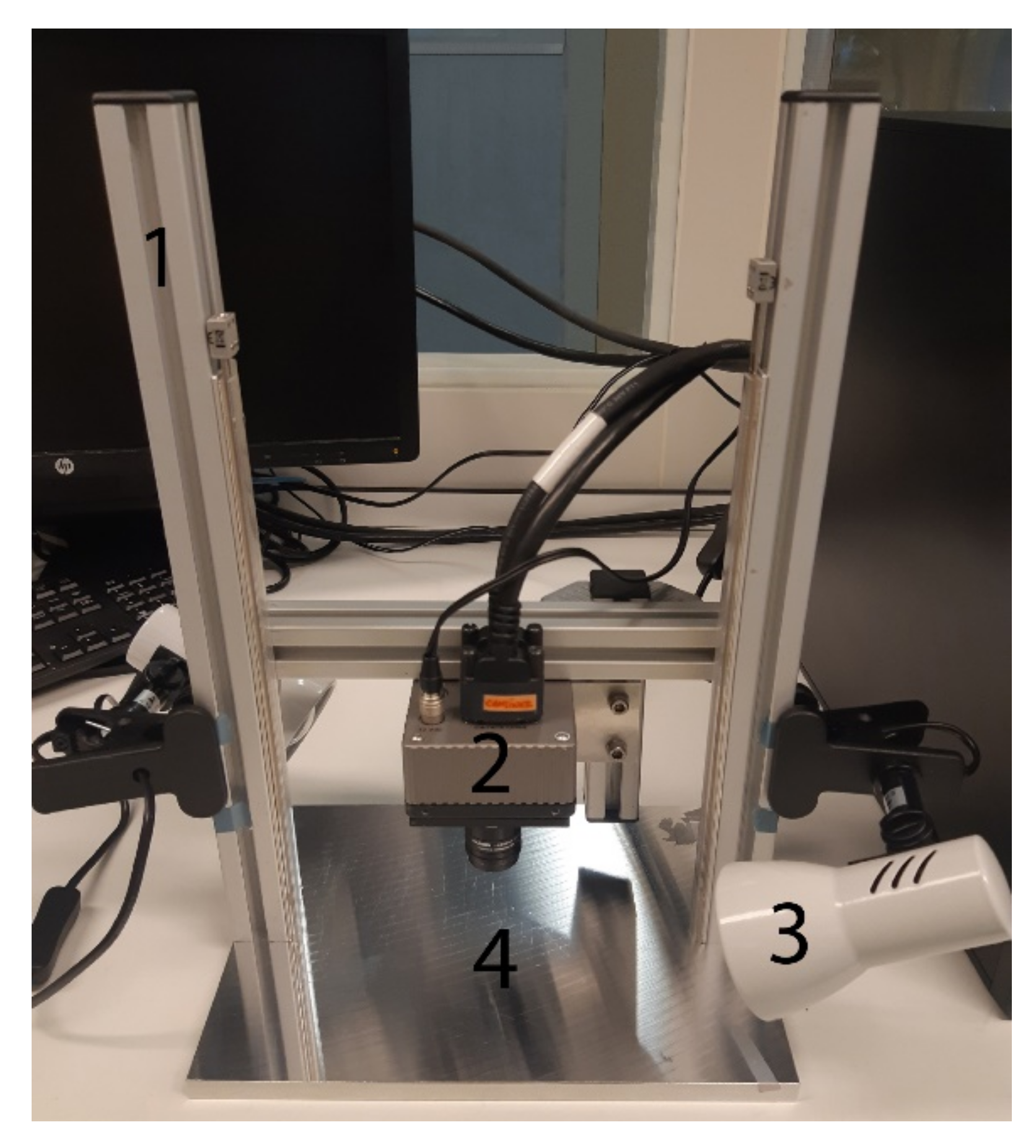
2.2. Instrumentation
2.3. Data Acquisition
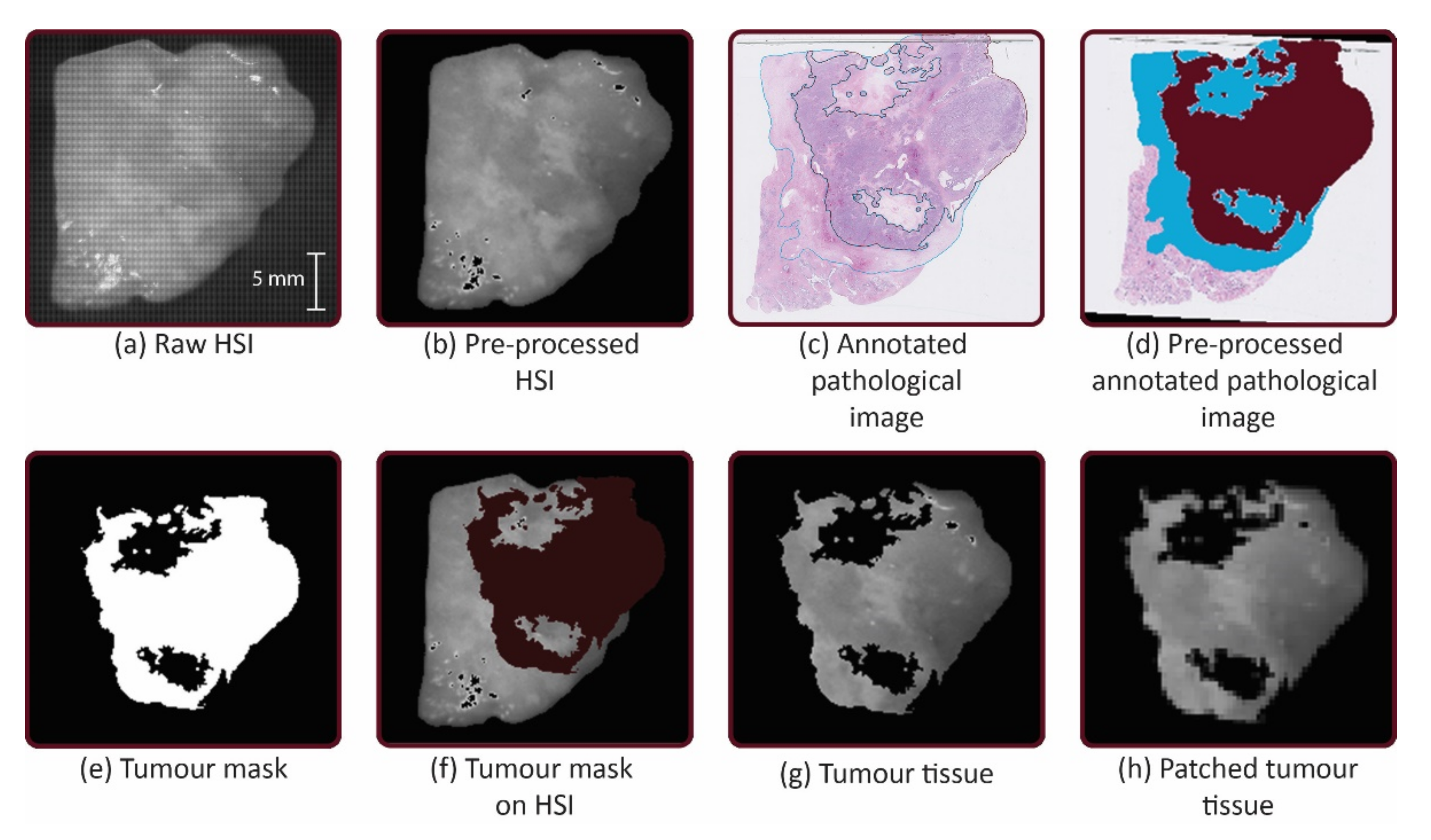
2.4. Data Pre-Processing
2.4.1. Image Calibration
2.4.2. Normalization
2.4.3. Image Data Selection
2.5. Pathological Annotation
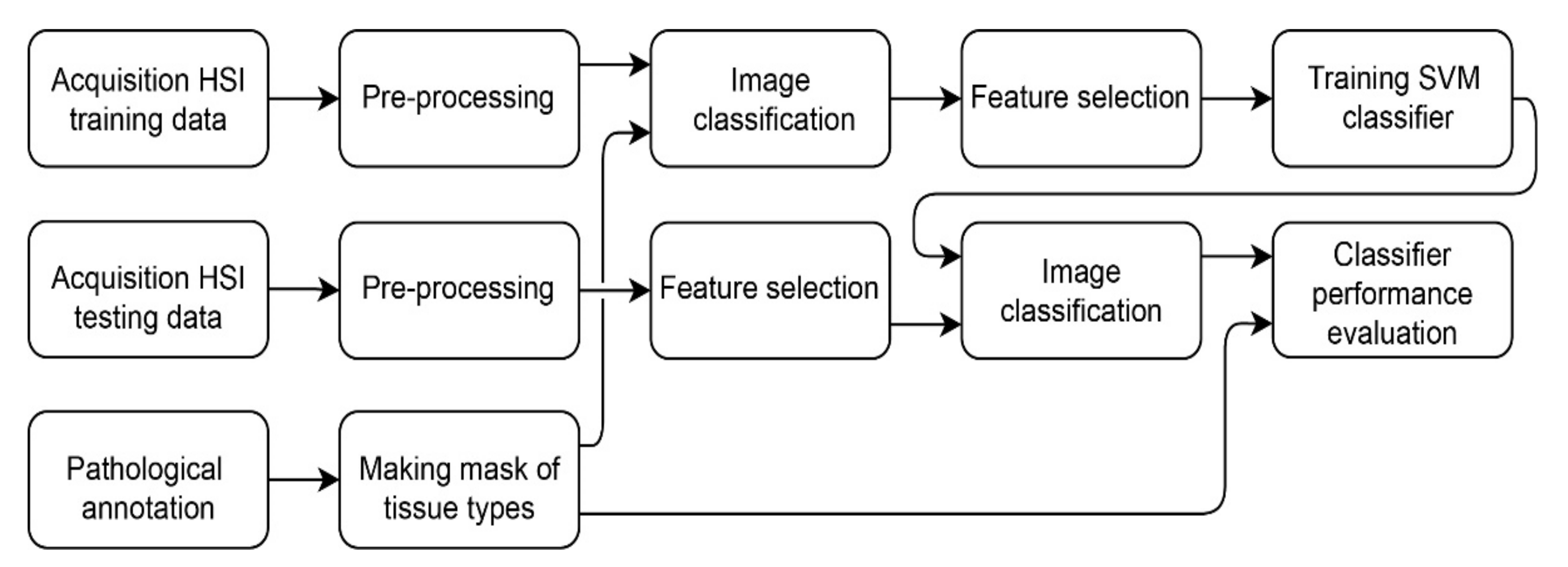
2.6. Classification of Hyperspectral Data
2.6.1. Image Classification
2.6.2. Feature Extraction
2.6.3. Support Vector Machine Classifier
2.7. Classifier Performance Evaluation
3. Results
3.1. Participants and Pathologies
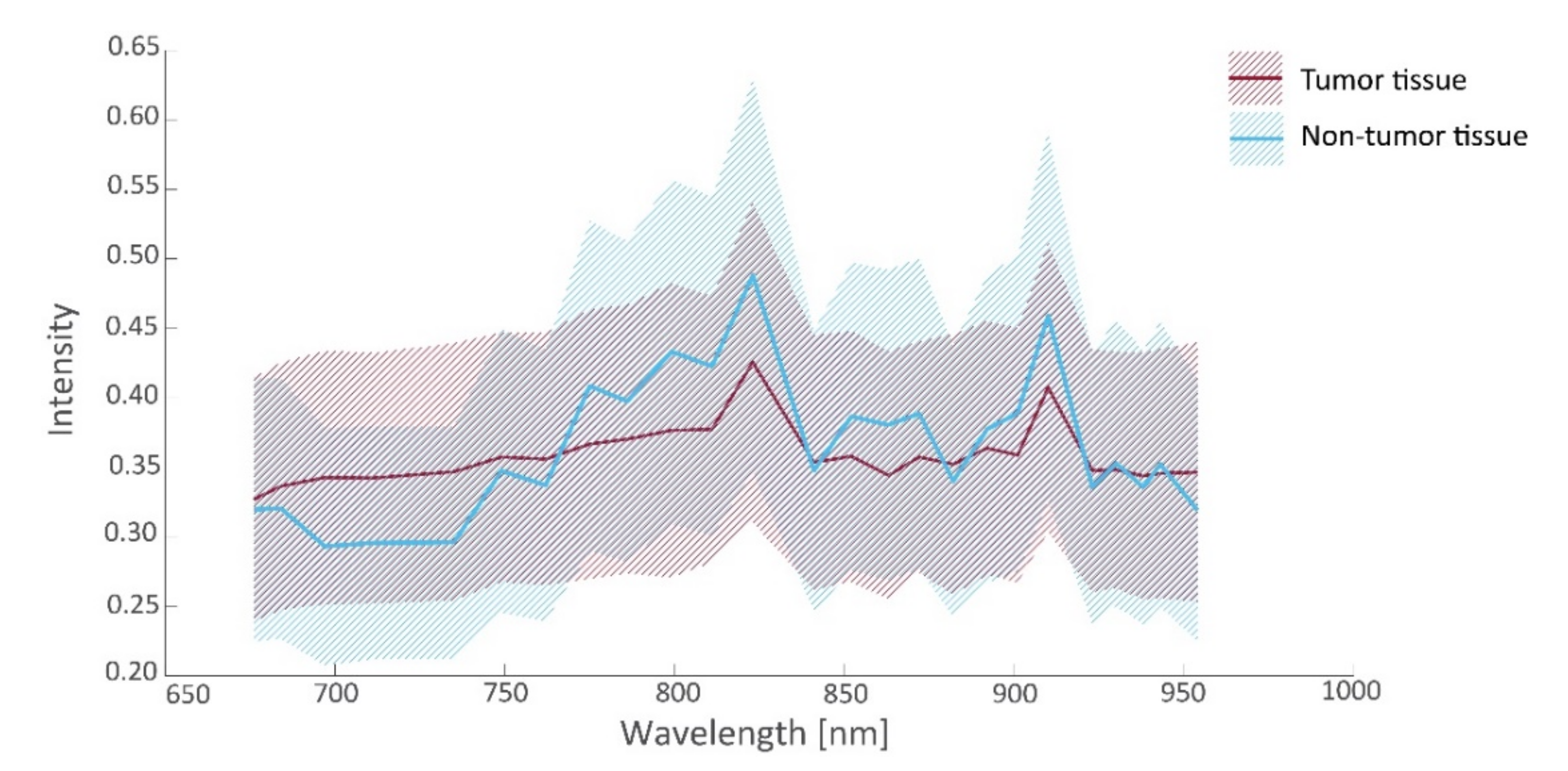
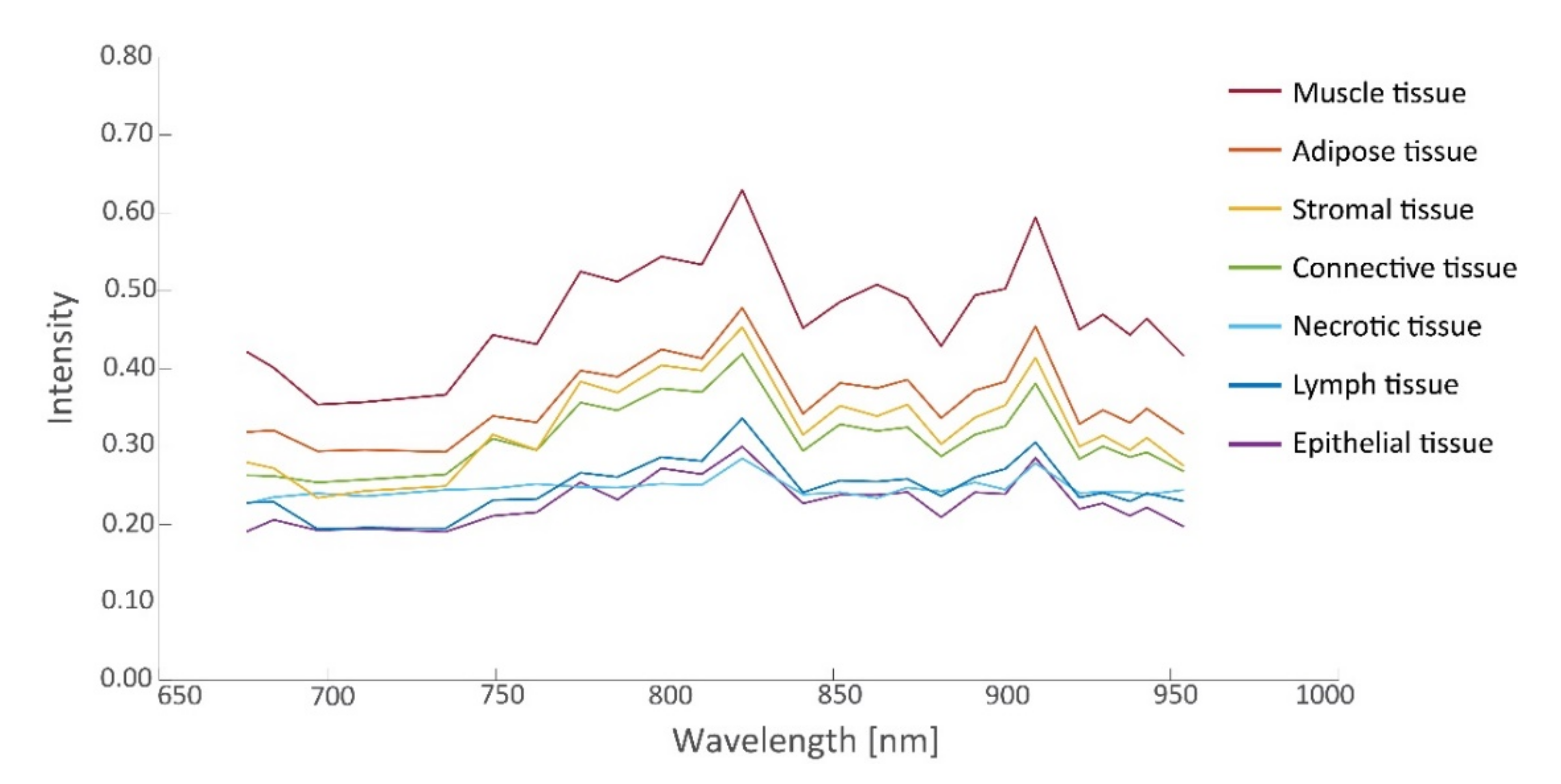
3.2. Spectral Signatures
3.3. Tissue Classification
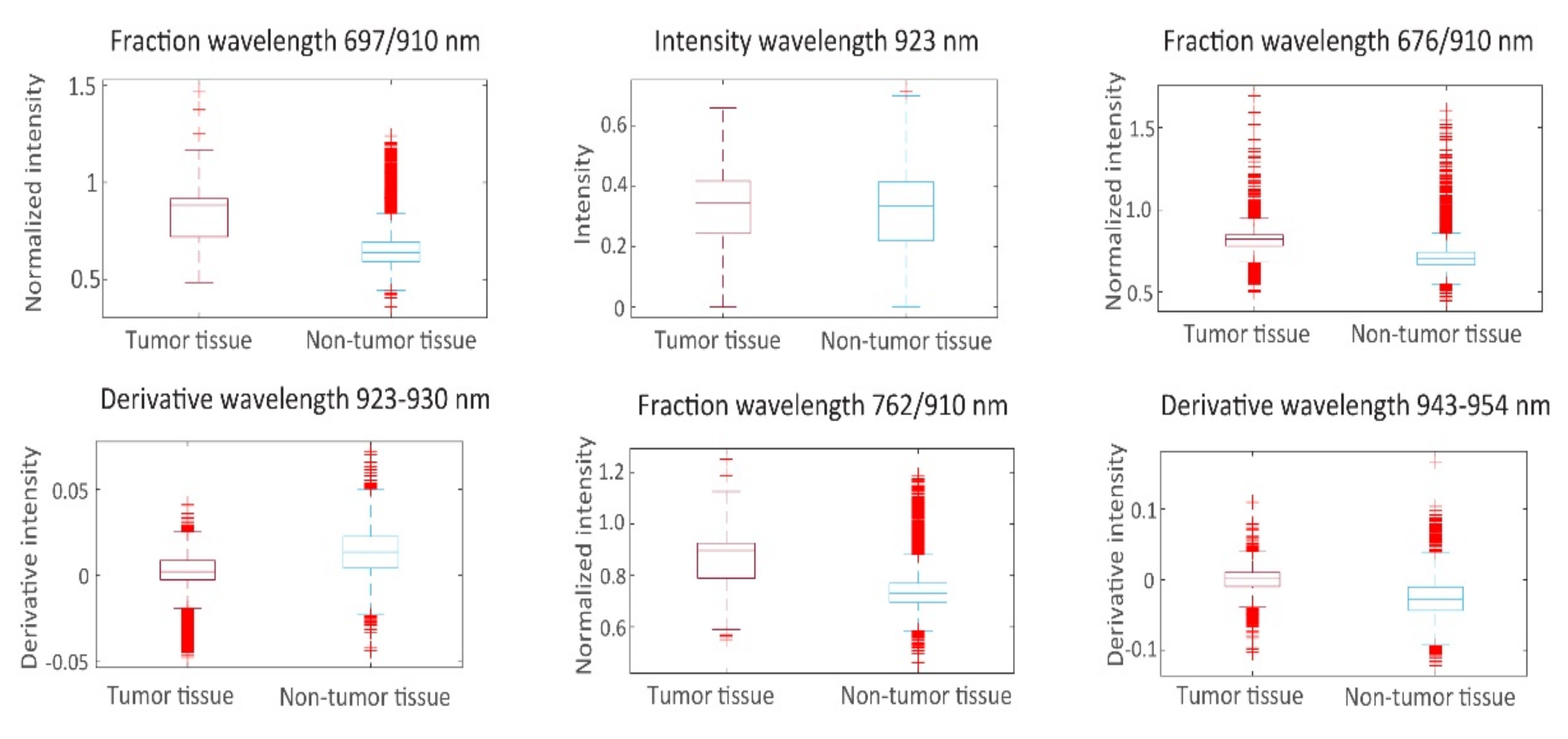
3.3.1. Feature Selection
3.3.2. Classifier Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Mutch, D.G.; Prat, J. 2014 FIGO Staging for Ovarian, Fallopian Tube and Peritoneal Cancer. Gynecol. Oncol. 2014, 133, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Orr, B.; Edwards, R.P. Diagnosis and Treatment of Ovarian Cancer. Hematol. Clin. North Am. 2018, 32, 943–964. [Google Scholar] [CrossRef]
- Wright, A.A.; Bohlke, K.; Armstrong, D.K.; Bookman, M.A.; Cliby, W.A.; Coleman, R.L.; Dizon, D.S.; Kash, J.J.; Meyer, L.A.; Moore, K.N.; et al. Neoadjuvant Chemotherapy for Newly Diagnosed, Advanced Ovarian Cancer: Society of Gynecologic Oncology and American Society of Clinical Oncology Clinical Practice Guideline. Gynecol. Oncol. 2016, 143, 3–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, M.C.; Seo, S.-S.; Kang, S.; Kim, S.K.; Kim, S.H.; Yoo, C.W.; Park, S.-Y. Intraoperative Image-Guided Surgery for Ovarian Cancer. Quant. Imaging Med. Surg. 2012, 2, 114–117. [Google Scholar] [CrossRef]
- Esbona, K.; Li, Z.; Wilke, L.G. Intraoperative Imprint Cytology and Frozen Section Pathology for Margin Assessment in Breast Conservation Surgery: A Systematic Review. Ann. Surg. Oncol. 2012, 19, 3236–3245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dam, G.M.; Themelis, G.; Crane, L.M.; Harlaar, N.J.; Pleijhuis, R.G.; Kelder, W.; Sarantopoulos, A.; De Jong, J.S.; Arts, H.J.; Van Der Zee, A.G.; et al. Intraoperative Tumor-Specific Fluorescence Imaging in Ovarian Cancer by Folate Receptor-α Targeting: First in-Human Results. Nat. Med. 2011, 17, 1315–1319. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Endo, Y.; Fujita, T.; Ishibashi, H.; Nishioka, T.; Canbay, E.; Li, Y.; Ogura, S.-I.; Yonemura, Y. Cytoreductive Surgery Under Aminolevulinic Acid-Mediated Photodynamic Diagnosis Plus Hyperthermic Intraperitoneal Chemotherapy in Patients with Peritoneal Carcinomatosis from Ovarian Cancer and Primary Peritoneal Carcinoma: Results of a Phase I Trial. Ann. Surg. Oncol. 2014, 21, 4256–4262. [Google Scholar] [CrossRef] [Green Version]
- Yonemura, Y.; Canbay, E.; Ishibashi, H.; Nishino, E.; Endou, Y.; Sako, S.; Ogura, S.-I. 5-Aminolevulinic Acid Fluorescence in Detection of Peritoneal Metastases. Asian Pac. J. Cancer Prev. 2016, 17, 2271–2275. [Google Scholar] [CrossRef] [Green Version]
- Hoogstins, C.E.; Tummers, Q.R.; Gaarenstroom, K.; De Kroon, C.D.; Trimbos, J.B.M.; Bosse, T.; Smit, V.T.; Vuyk, J.; Van De Velde, C.J.; Cohen, A.F.; et al. A Novel Tumor-Specific Agent for Intraoperative Near-Infrared Fluorescence Imaging: A Translational Study in Healthy Volunteers and Patients with Ovarian Cancer. Clin. Cancer Res. 2016, 22, 2929–2938. [Google Scholar] [CrossRef] [Green Version]
- Randall, L.M.; Wenham, R.M.; Low, P.S.; Dowdy, S.C.; Tanyi, J.L. A Phase II, Multicenter, Open-Label Trial of OTL38 Injection for the Intra-Operative Imaging of Folate Receptor-Alpha Positive Ovarian Cancer. Gynecol. Oncol. 2019, 155, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Halicek, M.; Fabelo, H.; Ortega, S.; Callico, G.M.; Fei, B. In-Vivo and Ex-Vivo Tissue Analysis through Hyperspectral Imaging Techniques: Revealing the Invisible Features of Cancer. Cancers 2019, 11, 756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacques, S.L. Optical Properties of Biological Tissues: A Review. Phys. Med. Biol. 2013, 58, R37. [Google Scholar] [CrossRef] [PubMed]
- Halicek, M.; Dormer, J.D.; Little, J.V.; Chen, A.Y.; Myers, L.; Sumer, B.D.; Fei, B. Hyperspectral Imaging of Head and Neck Squamous Cell Carcinoma for Cancer Margin Detection in Surgical Specimens from 102 Patients Using Deep Learning. Cancers 2019, 11, 1367. [Google Scholar] [CrossRef] [Green Version]
- Maktabi, M.; Köhler, H.; Ivanova, M.; Jansen-Winkeln, B.; Takoh, J.; Niebisch, S.; Rabe, S.M.; Neumuth, T.; Gockel, I.; Chalopin, C. Tissue Classification of Oncologic Esophageal Resectates Based on Hyperspectral Data. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1651–1661. [Google Scholar] [CrossRef]
- Kho, E.; Dashtbozorg, B.; De Boer, L.L.; Van De Vijver, K.K.; Sterenborg, H.J.C.M.; Ruers, T.J.M. Broadband Hyperspectral Imaging for Breast Tumor Detection Using Spectral and Spatial Information. Biomed. Opt. Express 2019, 10, 4496–4515. [Google Scholar] [CrossRef] [Green Version]
- Halicek, M.; Little, J.V.; Wang, X.; Chen, A.Y.; Fei, B. Optical Biopsy of Head and Neck Cancer Using Hyperspectral Imaging and Convolutional Neural Networks. J. Biomed. Opt. 2019, 24, 036007. [Google Scholar] [CrossRef] [Green Version]
- Lu, G.; Little, J.V.; Wang, X.; Zhang, H.; Patel, M.R.; Griffith, C.C.; El-Deiry, M.W.; Chen, A.Y.; Fei, B. Detection of Head and Neck Cancer in Surgical Specimens Using Quantitative Hyperspectral Imaging. Clin. Cancer Res. 2017, 23, 5426–5436. [Google Scholar] [CrossRef] [Green Version]
- De Koning, S.G.B.; Weijtmans, P.; Karakullukcu, M.B.; Shan, C.; Baltussen, E.J.M.; Smit, L.A.; van Veen, R.L.P.; Hendriks, B.H.W.; Sterenborg, H.J.C.M.; Ruers, T.J.M. Toward Assessment of Resection Margins Using Hyperspectral Diffuse Reflection Imaging (400–1700 nm) during Tongue Cancer Surgery. Lasers Surg. Med. 2019, 52, 496–502. [Google Scholar] [CrossRef]
- Kho, E.; De Boer, L.L.; Van De Vijver, K.K.; Van Duijnhoven, F.; Peeters, M.-J.T.V.; Sterenborg, H.J.; Ruers, T.J. Hyperspectral Imaging for Resection Margin Assessment during Cancer Surgery. Clin. Cancer Res. 2019, 25, 3572–3580. [Google Scholar] [CrossRef] [Green Version]
- Fabelo, H.; Halicek, M.; Ortega, S.; Shahedi, M.; Szolna, A.; Piñeiro, J.F.; Sosa, C.; O’Shanahan, A.J.; Bisshopp, S.; Espino, C.; et al. Deep Learning-Based Framework for In Vivo Identification of Glioblastoma Tumor using Hyperspectral Images of Human Brain. Sensors 2019, 19, 920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouri, D.; Lucas, Y.; Treuillet, S. Calibration and Test of a Hyperspectral Imaging Prototype for Intra-Operative Surgical Assistance. In Proceedings of the Medical Imaging 2013: Digital Pathology, Lake Buena Vista, FL, USA, 29 March 2013; Volume 8676, pp. 229–237. [Google Scholar] [CrossRef] [Green Version]
- Singh, B.K.; Verma, K.; Thoke, A. Investigations on Impact of Feature Normalization Techniques on Classifier’s Performance in Breast Tumor Classification. Int. J. Comput. Appl. 2015, 116, 11–15. [Google Scholar]
- Lu, G.; Wang, N.; Qin, X.; Muller, S.; Wang, X.; Chen, A.Y.; Chen, Z.G.; Fei, B. Detection and Delineation of Squamous Neoplasia with Hyperspectral Imaging in a Mouse Model of Tongue Carcinogenesis. J. Biophotonics 2017, 11, e201700078. [Google Scholar] [CrossRef] [PubMed]
- Manni, F.; van der Sommen, F.; Zinger, S.; Kho, E.; De Koning, S.G.B.; Ruers, T.J.M.; Shan, C.; Schleipen, J.; De With, P.H.N. Automated Tumor Assessment of Squamous Cell Carcinoma on Tongue Cancer Patients with Hyperspectral Imaging. In Proceedings of the Medical Imaging 2019: Image-Guided Procedures, Robotic Interventions, and Modeling, San Diego, CA, USA, 8 March 2019; Volume 10951, pp. 676–682. [Google Scholar] [CrossRef] [Green Version]
- Lu, G.; Fei, B. Medical Hyperspectral Imaging: A Review. J. Biomed. Opt. 2014, 19, 010901. [Google Scholar] [CrossRef]
- Tummers, Q.R.J.G.; Hoogstins, C.E.S.; Peters, A.A.W.; De Kroon, C.D.; Trimbos, J.B.M.Z.; Van De Velde, C.J.H.; Frangioni, J.V.; Vahrmeijer, A.L.; Gaarenstroom, K. The Value of Intraoperative Near-Infrared Fluorescence Imaging Based on Enhanced Permeability and Retention of Indocyanine Green: Feasibility and False-Positives in Ovarian Cancer. PLoS ONE 2015, 10, e0129766. [Google Scholar] [CrossRef]
- Pop, C.F.; Veys, I.; Galdon, M.G.; Moreau, M.; Larsimont, D.; Donckier, V.; Bourgeois, P.; Liberale, G. Ex Vivo Indocyanine Green Fluorescence Imaging for the Detection of Lymph Node Involvement in Advanced-Stage Ovarian Cancer. J. Surg. Oncol. 2018, 118, 1163–1169. [Google Scholar] [CrossRef]
- Veys, I.; Pop, C.F.; Vankerckhove, S.; Barbieux, R.; Chintinne, M.; Moreau, M.; Nogaret, J.-M.; Larsimont, D.; Donckier, V.; Bourgeois, P.; et al. ICG-Fluorescence Imaging for Detection of Peritoneal Metastases and Residual Tumoral Scars in Locally Advanced Ovarian Cancer: A Pilot Study. J. Surg. Oncol. 2017, 117, 228–235. [Google Scholar] [CrossRef]
- Baltussen, E.J.M.; Kok, E.N.; De Koning, S.G.B.; Sanders, J.; Aalbers, A.G.J.; Kok, N.F.M.; Beets, G.L.; Flohil, C.C.; Bruin, S.C.; Kuhlmann, K.F.D.; et al. Hyperspectral Imaging for Tissue Classification, a Way toward Smart Laparoscopic Colorectal Surgery. J. Biomed. Opt. 2019, 24, 1–9. [Google Scholar] [CrossRef]
- Beaulieu, R.J.; Goldstein, S.; Singh, J.; Safar, B.; Banerjee, A.; Ahuja, N. Automated Diagnosis of Colon Cancer Using Hyperspectral Sensing. Int. J. Med Robot. Comput. Assist. Surg. 2018, 14, e1897. [Google Scholar] [CrossRef]
- Halicek, M.; Fabelo, H.; Ortega, S.; Little, J.V.; Wang, X.; Chen, A.Y.; Callico, G.M.; Myers, L.; Sumer, B.D.; Fei, B. Hyperspectral Imaging for Head and Neck Cancer Detection: Specular Glare and Variance of the Tumor Margin in Surgical Specimens. J. Med Imaging 2019, 6, 035004. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, B.H.W.; Balthasar, A.J.R.; Lucassen, G.W.; Van Der Voort, M.; Mueller, M.; Pully, V.V.; Bydlon, T.M.; Reich, C.; Van Keersop, A.T.M.H.; Kortsmit, J.; et al. Nerve Detection with Optical Spectroscopy for Regional Anesthesia Procedures. J. Transl. Med. 2015, 13, 380. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Primary Location | Histology | Grade | FIGO Stage | Procedure | Tissue Type |
|---|---|---|---|---|---|---|
| 1 | Ovarian | Serous adenocarcinoma | 3 | IIIC | PDS a | A: Ovarian B: Ovarian C: Ovarian D: Omentum |
| 2 | Ovarian | Serous carcinoma | 3 | IV | IDS b | A: Mesenterium |
| 3 | Ovarian | Serous adenocarcinoma | 1/3 | IV | IDS b | A: Omentum B: Ovarian |
| 4 | Ovarian | Serous adenocarcinoma | 3 | IV | IDS b | A: Omentum B: Omentum C: Intestines |
| 5 | Mucinous adenocarcinoma | 3 | IV | PDS a | A: Omentum | |
| 6 | Ovarian | Serous adenocarcinoma | 3 | IIIC | IDS b | A: Ovarian B: Ovarian C: Intestines D: Omentum E: Omentum |
| 7 | Ovarian | Serous adenocarcinoma | 3 | IV | IDS b | A: Omentum B: Ovarian C: Ovarian |
| 8 | Ovarian | Serous adenocarcinoma | 3 | IIIC | IDS b | A: Omentum B: Ovarian |
| 9 | Ovarian | Serous adenocarcinoma | 3 | IV | IDS b | A: Ovarian B: Ovarian |
| 10 | Ovarian | Serous adenocarcinoma | 3 | IV | IDS b | A: Ovarian B: Omentum C: Ovarian |
| 11 | Ovarian | Serous adenocarcinoma | 1 | IV | PDS a | A: Omentum |
| Patient | 1 | 2 | 3 | 4 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|
| Total | 7819 | 123 | 1678 | 3134 | 7102 | 1236 | 1663 | 1564 | 1382 | 745 |
| Tumor | 5065 | 0 | 0 | 0 | 1012 | 440 | 0 | 31 | 80 | 688 |
| Non-tumor | 2754 | 123 | 1678 | 3134 | 6090 | 796 | 1663 | 1533 | 1302 | 57 |
| Patient | Sensitivity | Specificity | PPV a. | NPV b. | AUC c. | MCC d. |
|---|---|---|---|---|---|---|
| 1 | 0.91 | 0.55 | 0.79 | 0.77 | 0.76 | 0.51 |
| 2 | - | 0.00 | 0 * | - | - | - |
| 3 | - | 0.55 | 0 * | 1.00 * | - | - |
| 4 | - | 0.99 | 0 * | 1.00 * | - | - |
| 6 | 0.55 | 0.87 | 0.42 | 0.92 | 0.79 | 0.38 |
| 7 | 0.66 | 0.79 | 0.64 | 0.81 | 0.78 | 0.45 |
| 8 | - | 1.00 | 0 * | 1.00 * | ||
| 9 | 0.95 | 0.67 | 0.05 | 1.00 | 0.84 | 0.18 |
| 10 | 0.85 | 0.88 | 0.30 | 0.99 | 0.89 | 0.46 |
| 11 | 0.91 | 0.72 | 0.98 | 0.40 | 0.89 | 0.49 |
| Mean | 0.81 | 0.70 | 0.53 | 0.82 | 0.83 | 0.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Vliet-Pérez, S.M.; van de Berg, N.J.; Manni, F.; Lai, M.; Rijstenberg, L.; Hendriks, B.H.W.; Dankelman, J.; Ewing-Graham, P.C.; Nieuwenhuyzen-de Boer, G.M.; van Beekhuizen, H.J. Hyperspectral Imaging for Tissue Classification after Advanced Stage Ovarian Cancer Surgery—A Pilot Study. Cancers 2022, 14, 1422. https://doi.org/10.3390/cancers14061422
van Vliet-Pérez SM, van de Berg NJ, Manni F, Lai M, Rijstenberg L, Hendriks BHW, Dankelman J, Ewing-Graham PC, Nieuwenhuyzen-de Boer GM, van Beekhuizen HJ. Hyperspectral Imaging for Tissue Classification after Advanced Stage Ovarian Cancer Surgery—A Pilot Study. Cancers. 2022; 14(6):1422. https://doi.org/10.3390/cancers14061422
Chicago/Turabian Stylevan Vliet-Pérez, Sharline M., Nick J. van de Berg, Francesca Manni, Marco Lai, Lucia Rijstenberg, Benno H. W. Hendriks, Jenny Dankelman, Patricia C. Ewing-Graham, Gatske M. Nieuwenhuyzen-de Boer, and Heleen J. van Beekhuizen. 2022. "Hyperspectral Imaging for Tissue Classification after Advanced Stage Ovarian Cancer Surgery—A Pilot Study" Cancers 14, no. 6: 1422. https://doi.org/10.3390/cancers14061422