
A Novel Predictive Scoring System for 90-Day Mortality among Patients with Hepatocellular Cell Carcinoma Receiving Major Hepatectomy

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Database
2.2. Selection of Study Participants
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Patients with HCC Receiving Major Hepatectomy
3.2. 90-Day Mortality Risk Assessment after Major Hepatectomy
3.3. Stepwise Selection for 90-Day Mortality after Major Hepatectomy
3.4. 90-Day Mortality Assessment Using the Chang Gung-PohAi Mortality Predictive Scoring System
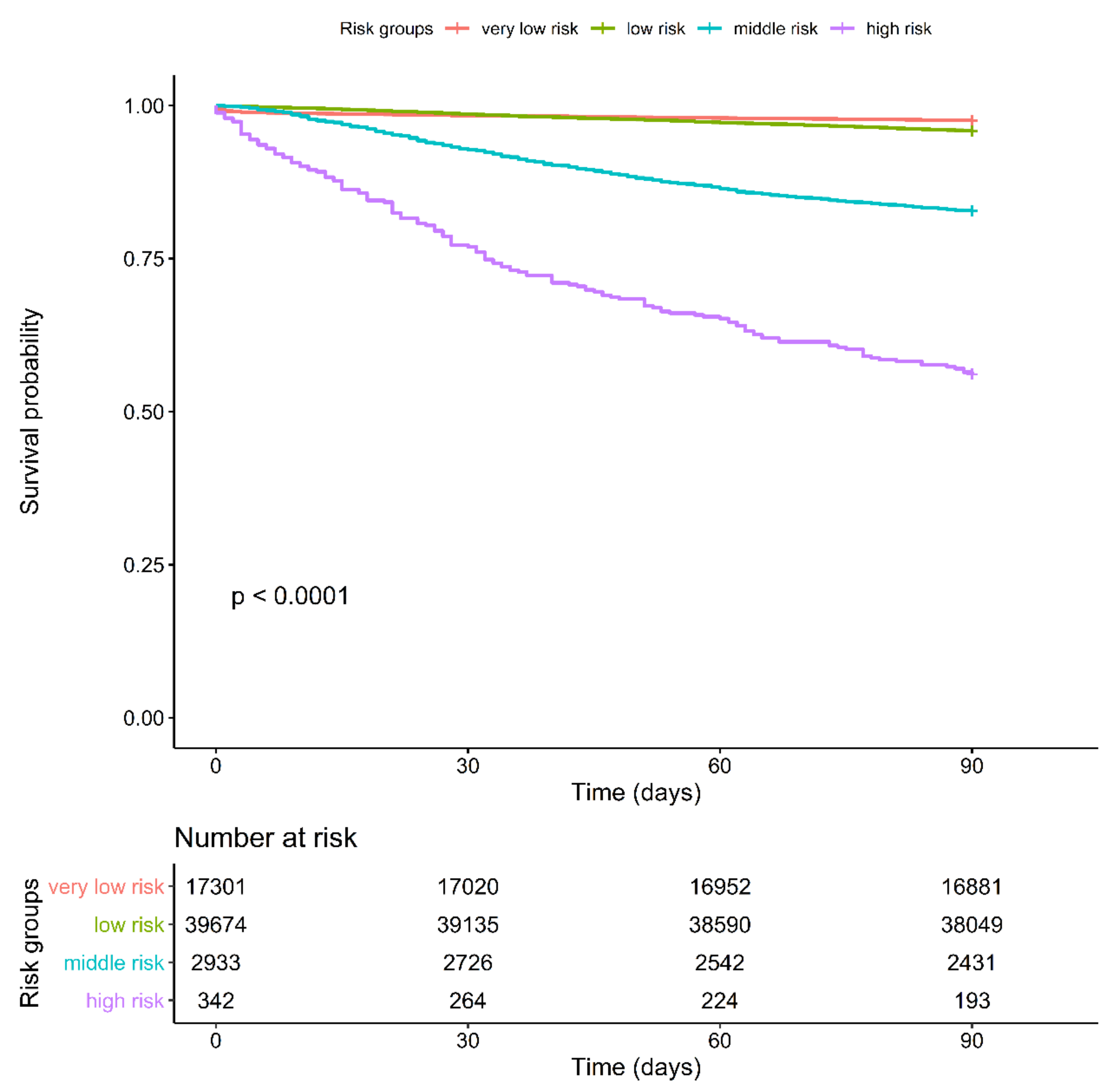
3.5. Kaplan–Meier Survival Curve for 90-Day Mortality Determined Using Chang Gung-PohAi, American Society of Anesthesiologists, or CCI Scores
3.6. Kaplan–Meier Curve for 5-Year Overall Survival Determined Using Chang Gung-PohAi, ASA, and CCI Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Llovet, J.M.; Villanueva, A.; Marrero, J.A.; Schwartz, M.; Meyer, T.; Galle, P.R.; Lencioni, R.; Greten, T.F.; Kudo, M.; Mandrekar, S.J.; et al. Trial Design and Endpoints in Hepatocellular Carcinoma: AASLD Consensus Conference. Hepatology 2021, 73 (Suppl. 1), 158–191. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Singal, A.G. Surveillance for Hepatocellular Carcinoma: Current Best Practice and Future Direction. Gastroenterology 2019, 157, 54–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seale, A.C.; Blencowe, H.; Zaidi, A.; Ganatra, H.; Syed, S.; Engmann, C.; Newton, C.R.; Vergnano, S.; Stoll, B.J.; Cousens, S.N.; et al. Neonatal severe bacterial infection impairment estimates in South Asia, sub-Saharan Africa, and Latin America for 2010. Pediatr. Res. 2013, 74, 73–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulik, L.; El-Serag, H.B. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology 2019, 156, 477–491.e1. [Google Scholar] [CrossRef]
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of hepatocellular carcinoma. Hepatology 2021, 73, 4–13. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.W.; Yong, C.C.; Lin, C.C.; Wang, C.C.; Chen, C.L.; Cheng, Y.F.; Wang, J.H.; Yen, Y.H.; Chen, C.H. Liver resection of hepatocellular carcinoma within and beyond the Barcelona Clinic Liver Cancer guideline recommendations: Results from a high-volume liver surgery center in East Asia. J. Surg. Oncol. 2020, 122, 1587–1594. [Google Scholar] [CrossRef]
- Wei, A.C.; Tung-Ping Poon, R.; Fan, S.T.; Wong, J. Risk factors for perioperative morbidity and mortality after extended hepatectomy for hepatocellular carcinoma. J. Br. Surg. 2003, 90, 33–41. [Google Scholar] [CrossRef]
- Imamura, H.; Sano, K.; Sugawara, Y.; Kokudo, N.; Makuuchi, M. Assessment of hepatic reserve for indication of hepatic resection: Decision tree incorporating indocyanine green test. J. Hepato-Biliary-Pancreat. Surg. 2005, 12, 16–22. [Google Scholar] [CrossRef]
- Wu, T.; Wang, F.; Lin, Y.; Chan, K.; Yu, M.; Lee, W. Right hepatectomy by the anterior method with liver hanging versus conventional approach for large hepatocellular carcinomas. J. Br. Surg. 2010, 97, 1070–1078. [Google Scholar] [CrossRef]
- Pamecha, V.; Gurusamy, K.S.; Sharma, D.; Davidson, B.R. Techniques for liver parenchymal transection: A meta-analysis of randomized controlled trials. HPB 2009, 11, 275–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.-M.; Lei, L.-M.; Zhu, J.; Li, G.-L.; Min, J. Risk factor analysis of perioperative mortality after ruptured bleeding in hepatocellular carcinoma. World J. Gastroenterol. WJG 2014, 20, 14921. [Google Scholar] [CrossRef]
- Ferrero, A.; Viganò, L.; Polastri, R.; Muratore, A.; Eminefendic, H.; Regge, D.; Capussotti, L. Postoperative liver dysfunction and future remnant liver: Where is the limit? World J. Surg. 2007, 31, 1643–1651. [Google Scholar] [CrossRef] [PubMed]
- Regimbeau, J.M.; Abdalla, E.K.; Vauthey, J.N.; Lauwers, G.Y.; Durand, F.; Nagorney, D.M.; Ikai, I.; Yamaoka, Y.; Belghiti, J. Risk factors for early death due to recurrence after liver resection for hepatocellular carcinoma: Results of a multicenter study. J. Surg. Oncol. 2004, 85, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, L.S. Surgery in the patient with liver disease. Trans. Am. Clin. Clim. Assoc. 2010, 121, 192–204; discussion 205. [Google Scholar] [CrossRef]
- Zacharias, T.; Ferreira, N. Nutritional risk screening 2002 and ASA score predict mortality after elective liver resection for malignancy. Arch. Med. Sci. 2017, 13, 361. [Google Scholar] [CrossRef] [Green Version]
- Aronson, W.L.; McAuliffe, M.S.; Miller, K. Variability in the American Society of Anesthesiologists physical status classification scale. AANA J. 2003, 71, 265–276. [Google Scholar]
- Fong, Y.; Brennan, M.; Cohen, A.; Heffernan, N.; Freiman, A.; Blumgart, L. Liver resection in the elderly. J. Br. Surg. 1997, 84, 1386–1390. [Google Scholar]
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef]
- Hall, W.H.; Ramachandran, R.; Narayan, S.; Jani, A.B.; Vijayakumar, S. An electronic application for rapidly calculating Charlson comorbidity score. BMC Cancer 2004, 4, 94. [Google Scholar] [CrossRef] [Green Version]
- Frenkel, W.J.; Jongerius, E.J.; Mandjes-van Uitert, M.J.; van Munster, B.C.; de Rooij, S.E. Validation of the Charlson Comorbidity Index in acutely hospitalized elderly adults: A prospective cohort study. J. Am. Geriatr. Soc. 2014, 62, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Laor, A.; Tal, S.; Guller, V.; Zbar, A.P.; Mavor, E. The Charlson Comorbidity Index (CCI) as a mortality predictor after surgery in elderly patients. Am. Surg. 2016, 82, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Chen, T.-M.; Kao, Y.-W.; Lin, K.-C.; Yuan, K.S.-P.; Wu, A.T.H.; Shia, B.-C.; Wu, S.-Y. Predicting 90-Day Mortality in Locoregionally Advanced Head and Neck Squamous Cell Carcinoma after Curative Surgery. Cancers 2018, 10, 392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, K.C.; Chen, T.M.; Yuan, K.S.; Wu, A.T.H.; Wu, S.Y. Assessment of Predictive Scoring System for 90-Day Mortality Among Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma Who Have Completed Concurrent Chemoradiotherapy. JAMA Netw. Open 2020, 3, e1920671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, S.Y.; Chiang, C.J.; Yang, Y.W.; Lee, W.C. Secular trends in liver cancer incidence from 1997 to 2014 in Taiwan and projection to 2035: An age-period-cohort analysis. J. Formos. Med. Assoc. 2019, 118, 444–449. [Google Scholar] [CrossRef]
- Chiang, C.J.; You, S.L.; Chen, C.J.; Yang, Y.W.; Lo, W.C.; Lai, M.S. Quality assessment and improvement of nationwide cancer registration system in Taiwan: A review. Jpn. J. Clin. Oncol. 2015, 45, 291–296. [Google Scholar] [CrossRef]
- Wen, C.P.; Tsai, S.P.; Chung, W.S. A 10-year experience with universal health insurance in Taiwan: Measuring changes in health and health disparity. Ann. Intern Med. 2008, 148, 258–267. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.Y.; Fang, S.C.; Hwang, O.R.; Shih, H.J.; Shao, Y.J. Influence of Baseline Cardiovascular Comorbidities on Mortality after Androgen Deprivation Therapy for Metastatic Prostate Cancer. Cancers 2020, 12, 189. [Google Scholar] [CrossRef] [Green Version]
- Shia, B.C.; Qin, L.; Lin, K.C.; Fang, C.Y.; Tsai, L.L.; Kao, Y.W.; Wu, S.Y. Outcomes for Elderly Patients Aged 70 to 80 Years or Older with Locally Advanced Oral Cavity Squamous Cell Carcinoma: A Propensity Score-Matched, Nationwide, Oldest Old Patient-Based Cohort Study. Cancers 2020, 12, 258. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.C.; Liu, H.E.; Kao, Y.W.; Qin, L.; Lin, K.C.; Fang, C.Y.; Tsai, L.L.; Shia, B.C.; Wu, S.Y. Definitive radiotherapy or surgery for early oral squamous cell carcinoma in old and very old patients: A propensity-score-matched, nationwide, population-based cohort study. Radiother. Oncol. 2020, 151, 214–221. [Google Scholar] [CrossRef]
- Yu, J.M.; Hsieh, M.C.; Qin, L.; Zhang, J.; Wu, S.Y. Metformin reduces radiation-induced cardiac toxicity risk in patients having breast cancer. Am. J. Cancer Res. 2019, 9, 1017–1026. [Google Scholar] [PubMed]
- Wu, S.-Y.; Huang, E.-Y.; Lin, H. Optimal Treatments for Cervical Adenocarcinoma. Am. J. Cancer Res. 2019, 9, 1224. [Google Scholar] [PubMed]
- Reddy, S.K.; Barbas, A.S.; Turley, R.S.; Steel, J.L.; Tsung, A.; Marsh, J.W.; Geller, D.A.; Clary, B.M. A standard definition of major hepatectomy: Resection of four or more liver segments. HPB 2011, 13, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Mellemgaard, A.; Luchtenborg, M.; Iachina, M.; Jakobsen, E.; Green, A.; Krasnik, M.; Moller, H. Role of comorbidity on survival after radiotherapy and chemotherapy for nonsurgically treated lung cancer. J. Thorac. Oncol. 2015, 10, 272–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sogaard, M.; Thomsen, R.W.; Bossen, K.S.; Sorensen, H.T.; Norgaard, M. The impact of comorbidity on cancer survival: A review. Clin. Epidemiol. 2013, 5, 3–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, L.; Cheung, W.Y.; Atkinson, E.; Krzyzanowska, M.K. Impact of comorbidity on chemotherapy use and outcomes in solid tumors: A systematic review. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 106–117. [Google Scholar] [CrossRef]
- Kuo, C.N.; Liao, Y.M.; Kuo, L.N.; Tsai, H.J.; Chang, W.C.; Yen, Y. Cancers in Taiwan: Practical insight from epidemiology, treatments, biomarkers, and cost. J. Formos. Med. Assoc. 2020, 119, 1731–1741. [Google Scholar] [CrossRef]
- Zheng, R.; Qu, C.; Zhang, S.; Zeng, H.; Sun, K.; Gu, X.; Xia, C.; Yang, Z.; Li, H.; Wei, W.; et al. Liver cancer incidence and mortality in China: Temporal trends and projections to 2030. Chin. J. Cancer Res. 2018, 30, 571–579. [Google Scholar] [CrossRef]
- Poon, R.T.; Fan, S.T.; Ng, I.O.; Wong, J. Significance of resection margin in hepatectomy for hepatocellular carcinoma: A critical reappraisal. Ann. Surg. 2000, 231, 544–551. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef]
- Wang, Y.Y.; Zhao, X.H.; Ma, L.; Ye, J.Z.; Wu, F.X.; Tang, J.; You, X.M.; Xiang, B.D.; Li, L.Q. Comparison of the ability of Child-Pugh score, MELD score, and ICG-R15 to assess preoperative hepatic functional reserve in patients with hepatocellular carcinoma. J. Surg. Oncol. 2018, 118, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.W.; Qu, Z.; Wu, B.Q.; Sun, D.L.; Jiang, Y. The preoperative fibrosis score 4 predicts posthepatectomy liver failure in patients with hepatocellular carcinoma. Ann. Hepatol. 2019, 18, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.-A.; Petrowsky, H.; DeOliveira, M.L.; Graf, R. Strategies for safer liver surgery and partial liver transplantation. N. Engl. J. Med. 2007, 356, 1545–1559. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Chen, B.; Miao, X.Y.; Zhou, J.J.; Xiong, L.; Wen, Y.; Zou, H. Comparison of FIB-4 Index and Child-Pugh Score in Predicting the Outcome of Hepatic Resection for Hepatocellular Carcinoma. J. Gastrointest. Surg. 2020, 24, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Cieslak, K.P.; Runge, J.H.; Heger, M.; Stoker, J.; Bennink, R.J.; Van Gulik, T.M. New perspectives in the assessment of future remnant liver. Dig. Surg. 2014, 31, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Petrowsky, H.; Fritsch, R.; Guckenberger, M.; De Oliveira, M.L.; Dutkowski, P.; Clavien, P.-A. Modern therapeutic approaches for the treatment of malignant liver tumours. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 755–772. [Google Scholar] [CrossRef]
- Zaydfudim, V.M.; Turrentine, F.E.; Smolkin, M.E.; Bauer, T.B.; Adams, R.B.; McMurry, T.L. The impact of cirrhosis and MELD score on postoperative morbidity and mortality among patients selected for liver resection. Am. J. Surg. 2020, 220, 682–686. [Google Scholar] [CrossRef]
- Rahnemai-Azar, A.A.; Cloyd, J.M.; Weber, S.M.; Dillhoff, M.; Schmidt, C.; Winslow, E.R.; Pawlik, T.M. Update on Liver Failure Following Hepatic Resection: Strategies for Prediction and Avoidance of Post-operative Liver Insufficiency. J. Clin. Transl. Hepatol. 2018, 6, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.-Y.; Xiang, B.-D.; Ma, L.; Zhong, J.-H.; Ye, J.-Z.; Wang, K.; Xing, B.-C.; Li, L.-Q. Development and validation of a nomogram to preoperatively estimate post-hepatectomy liver dysfunction risk and long-term survival in patients with hepatocellular carcinoma. Ann. Surg. 2021, 274, e1209–e1217. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Nomi, T.; Hokuto, D.; Kamitani, N.; Matsuo, Y.; Sho, M. Outcomes in Patients with Chronic Kidney Disease After Liver Resection for Hepatocellular Carcinoma. World J. Surg. 2021, 45, 598–606. [Google Scholar] [CrossRef]
- Bolder, U.; Brune, A.; Schmidt, S.; Tacke, J.; Jauch, K.W.; Lohlein, D. Preoperative assessment of mortality risk in hepatic resection by clinical variables: A multivariate analysis. Liver Transpl. Surg. 1999, 5, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S. Grading of patients for surgical procedures. Anesthesiology 1941, 2, 281–284. [Google Scholar]
- Daabiss, M. American Society of Anaesthesiologists physical status classification. Indian J. Anaesth. 2011, 55, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, L.L.; Kashiwagi, D.T.; Burton, M.C.; Cha, S.; Varkey, P. The Charlson Comorbidity Index Score as a predictor of 30-day mortality after hip fracture surgery. Am. J. Med. Qual. 2011, 26, 461–467. [Google Scholar] [CrossRef]
- Volk, M.L.; Hernandez, J.C.; Lok, A.S.; Marrero, J.A. Modified Charlson comorbidity index for predicting survival after liver transplantation. Liver Transplant. 2007, 13, 1515–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.-Y.; Chang, C.-L.; Chen, C.-I.; Huang, C.-C. Comparison of Acute and Chronic Surgical Complications Following Robot-Assisted, Laparoscopic, and Traditional Open Radical Prostatectomy Among Men in Taiwan. JAMA Netw. Open 2021, 4, e2120156. [Google Scholar] [CrossRef]
- Kao, W.H.; Hong, J.H.; See, L.C.; Yu, H.P.; Hsu, J.T.; Chou, I.J.; Chou, W.C.; Chiou, M.J.; Wang, C.C.; Kuo, C.F. Validity of cancer diagnosis in the National Health Insurance database compared with the linked National Cancer Registry in Taiwan. Pharmacoepidemiol. Drug Saf. 2018, 27, 1060–1066. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | 90-Day Survival No. (%) | 90-Day Mortality No. (%) | p Value | |
|---|---|---|---|---|
| n | 57,525 (95.5%) | 2725 (4.5%) | ||
| Sex | Female | 20,859 (36.3) | 885 (32.5) | <0.001 |
| Male | 36,666 (63.7) | 1840 (67.5) | ||
| Age, mean (SD) | 58.39 (13.72) | 61.61 (16.43) | <0.001 | |
| Age (years) | 20–29 | 1653 (2.9) | 172 (6.3) | <0.001 |
| 30–39 | 3499 (6.1) | 112 (4.1) | ||
| 40–49 | 8402 (14.6) | 263 (9.7) | ||
| 50–59 | 15,023 (26.1) | 441 (16.2) | ||
| 60–69 | 16,316 (28.4) | 719 (26.4) | ||
| ≥70 | 12,632 (22.0) | 1018 (37.4) | ||
| Comorbidities | ||||
| Diabetes mellitus | Yes | 12,731 (22.1) | 812 (29.8) | <0.001 |
| Pneumonia | Yes | 2859 (5.0) | 320 (11.7) | <0.001 |
| COPD | Yes | 2686 (4.7) | 224 (8.2) | <0.001 |
| Hepatitis B | Yes | 18,659 (32.4) | 492 (18.1) | <0.001 |
| Hepatitis C | Yes | 10,065 (17.5) | 447 (16.4) | 0.149 |
| Heart valve dysfunction | Yes | 976 (1.7) | 56 (2.1) | 0.182 |
| Sepsis | Yes | 2278 (4.0) | 505 (18.5) | <0.001 |
| Heart failure | Yes | 1330 (2.3) | 151 (5.5) | <0.001 |
| Disseminated intravascular coagulation | Yes | 27 (0.0) | 46 (1.7) | <0.001 |
| ARDS | Yes | 41 (0.1) | 25 (0.9) | <0.001 |
| Aortic aneurysm | Yes | 96 (0.2) | 15 (0.6) | <0.001 |
| Peripheral vascular disease | Yes | 566 (1.0) | 43 (1.6) | 0.003 |
| Peptic ulcer disease | Yes | 12,853 (22.3) | 775 (28.4) | <0.001 |
| Dementia | Yes | 511 (0.9) | 59 (2.2) | <0.001 |
| Chronic pulmonary disease | Yes | 2617 (4.5) | 179 (6.6) | <0.001 |
| Connective tissue disease | Yes | 512 (0.9) | 20 (0.7) | 0.455 |
| Mild liver disease | Yes | 27,019 (47.0) | 1100 (50.4) | <0.001 |
| Hemiplegia | Yes | 1456 (2.5) | 123 (4.5) | <0.001 |
| Moderate or severe liver disease | Yes | 8362 (14.5) | 413 (17.2) | <0.001 |
| Coronal arterial disease | Yes | 4390 (7.6) | 278 (10.2) | <0.001 |
| Myocardial infarction | Yes | 164 (0.3) | 42 (1.5) | <0.001 |
| HTN | Yes | 20,474 (35.6) | 993 (36.4) | 0.377 |
| Angina | Yes | 868 (1.5) | 72 (2.6) | <0.001 |
| CKD | Yes | 250 (0.4) | 26 (1.0) | <0.001 |
| Moderate or severe renal disease | Yes | 1622 (2.8) | 425 (15.6) | <0.001 |
| End-stage renal disease | Yes | 1904 (3.3) | 175 (6.4) | <0.001 |
| Cerebral vascular accident | Yes | 1738 (3.0) | 165 (6.1) | <0.001 |
| Transient ischemic attack | Yes | 846 (1.5) | 89 (3.3) | <0.001 |
| Implanted pacemaker | Yes | 11 (0.0) | 3 (0.1) | 0.016 |
| Cancer status | ||||
| Any other cancers | Yes | 14,632 (25.4) | 746 (27.4) | 0.025 |
| Leukemia | Yes | 44 (0.1) | 3 (0.1) | 0.793 |
| Lymphoma | Yes | 194 (0.3) | 17 (0.6) | 0.021 |
| Metastatic solid tumor for other cancers | Yes | 1229 (2.1) | 72 (2.6) | <0.001 |
| Surgical techniques | 0.948 | |||
| Open | 54,591 (94.9) | 2589 (95.0) | ||
| Laparoscopic surgery | 2934 (5.1) | 136 (5.0) | ||
| Hepatocellular cell carcinoma stages | ||||
| BCLC classification | 36,768 (63.9) | 1970 (72.3) | <0.001 | |
| 0 | 11,038 (19.2) | 217 (8.0) | ||
| A | 3312 (5.8) | 134 (4.9) | ||
| B | 3544 (6.2) | 249 (9.1) | ||
| C | 2863 (5.0) | 155 (5.7) | ||
| AJCC Clinical T stages | 36,767 (63.9) | 1970 (72.3) | <0.001 | |
| cT1 | 11,143 (19.4) | 229 (8.4) | ||
| cT2 | 3569 (6.2) | 151 (5.5) | ||
| cT3 | 4496 (7.8) | 273 (10.0) | ||
| cT4 | 1550 (2.7) | 102 (3.7) | ||
| Clinical N stages | 36,767 (63.9) | 1970 (72.3) | <0.001 | |
| cN0 | 17,957 (31.2) | 620 (22.8) | ||
| cN1 | 2801 (4.9) | 135 (5.0) | ||
| Clinical M stages | 36,767 (63.9) | 1970 (72.3) | <0.001 | |
| cM0 | 18,265 (31.8) | 636 (23.3) | ||
| cM1 | 2493 (4.3) | 119 (4.4) |
| Factor | aHR * | 95% CI | p Value |
|---|---|---|---|
| Age (years) | |||
| 20–29 | Reference | ||
| 30–39 | 0.745 | 0.302, 1.837 | 0.5228 |
| 40–49 | 0.756 | 0.328, 1.746 | 0.5129 |
| 50–59 | 0.857 | 0.379, 1.938 | 0.7103 |
| 60–69 | 1.139 | 0.506, 2.563 | 0.7536 |
| ≧70 | 2.117 | 0.944, 4.749 | 0.0689 |
| Sex | |||
| Female | Reference | ||
| Male | 1.015 | 0.865, 1.191 | 0.8537 |
| Comorbidities | |||
| Diabetes mellitus | 1.689 | 1.458, 1.957 | <0.001 |
| Pneumonia | 2.896 | 2.338, 3.588 | <0.001 |
| COPD | 1.903 | 1.481, 2.445 | <0.001 |
| Hepatitis B | 1.021 | 0.429, 1.585 | 0.4010 |
| Hepatitis C | 0.975 | 0.824, 1.153 | 0.7632 |
| Heart valve dysfunction | 1.817 | 1.219, 2.706 | 0.0033 |
| Sepsis | 8.688 | 7.275, 10.376 | <0.001 |
| Heart failure | 2.898 | 2.202, 3.813 | <0.001 |
| Disseminated intravascular coagulation | 35.258 | 15.789, 78.733 | <0.001 |
| ARDS | 3.948 | 0.556, 28.059 | 0.1699 |
| Aortic aneurysm | 2.278 | 0.734, 7.064 | 0.1540 |
| Peripheral vascular disease | 2.376 | 1.54, 3.667 | <0.001 |
| Peptic ulcer disease | 1.53 | 1.31, 1.786 | <0.001 |
| Dementia | 2.649 | 1.699, 4.13 | <0.001 |
| Chronic pulmonary disease | 1.353 | 1.004, 1.822 | 0.0471 |
| Connective tissue disease | 1.086 | 0.361, 1.799 | 0.5979 |
| Mild liver disease | 1.050 | 0.650, 1.085 | 0.7461 |
| Hemiplegia | 2.291 | 1.700, 3.087 | <0.001 |
| Moderate or severe liver disease | 1.169 | 0.981, 1.394 | 0.0804 |
| Coronal arterial disease | 1.197 | 0.944, 1.517 | 0.1372 |
| Myocardial infarction | 6.275 | 3.824, 10.296 | <0.001 |
| HTN | 1.144 | 0.991, 1.321 | 0.0661 |
| Angina | 2.058 | 1.445, 2.933 | <0.001 |
| CKD | 2.439 | 1.307, 4.551 | 0.0051 |
| Moderate or severe renal disease | 7.185 | 5.98, 8.633 | <0.001 |
| End-stage renal disease | 2.051 | 1.579, 2.664 | <0.001 |
| Cerebral vascular accident | 2.251 | 1.718, 2.949 | <0.001 |
| Transient ischemic attack | 2.516 | 1.792, 3.532 | <0.001 |
| Implanted pacemaker | 1.000 | 0.999, 1.001 | 0.9990 |
| Cancer status | |||
| Any other cancers | 1.029 | 0.858, 1.235 | 0.7565 |
| Leukemia | 1.000 | 0.991, 1.001 | 0.9977 |
| Lymphoma | 2.672 | 0.376, 18.993 | 0.3259 |
| Other metastatic solid tumor | 1.525 | 1.295, 1.797 | <0.001 |
| Surgical techniques | |||
| Open | Reference | ||
| Laparoscopic surgery | 0.996 | 0.782, 3.124 | 0.8697 |
| Hepatocellular cell carcinoma stages | |||
| BCLC classification 0 | Reference | ||
| BCLC classification A | 2.043 | 1.647, 2.534 | <0.001 |
| BCLC classification B | 3.490 | 2.908, 4.187 | <0.001 |
| BCLC classification C | 2.705 | 2.201, 3.325 | <0.001 |
| AJCC cT1 | Reference | ||
| AJCC cT2 | 2.042 | 1.663, 2.508 | <0.001 |
| AJCC cT3 | 2.898 | 2.431, 3.455 | <0.001 |
| AJCC cT4 | 3.126 | 2.475, 3.948 | <0.001 |
| AJCC cN0 | Reference | ||
| AJCC cN1 | 3.015 | 1.471, 4.579 | <0.001 |
| AJCC cM0 | Reference | ||
| AJCC cM1 | 1.361 | 1.119, 1.655 | 0.002 |
| Factor | HR * | Score |
|---|---|---|
| Age: 30–39 years | 0.854 | 0 |
| Age: 40–49 years | 0.974 | 0 |
| Age: 50–59 years | 0.817 | 0 |
| Age: 60–69 years | 0.967 | 0 |
| Age: ≧70 years | 1.462 | 1 |
| Comorbidities | ||
| Diabetes mellitus | 1.426 | 1 |
| Pneumonia | 1.703 | 2 |
| Hepatitis B | 0.910 | 0 |
| Sepsis | 4.762 | 5 |
| Heart failure | 1.604 | 2 |
| Disseminated intravascular coagulation | 14.055 | 14 |
| Peptic ulcer disease | 1.336 | 1 |
| Dementia | 1.703 | 2 |
| Myocardial infarction | 3.624 | 4 |
| HTN | 0.998 | 0 |
| Moderate or severe renal disease | 4.477 | 4 |
| Cerebral vascular accident | 1.48 | 1 |
| Transient ischemic attack | 1.582 | 2 |
| Cancer status | ||
| Any other cancers | 0.942 | 0 |
| Other metastatic solid tumor | 1.421 | 1 |
| Hepatocellular cell carcinoma status | ||
| BCLC classification A | 1.929 | 2 |
| BCLC classification B | 3.557 | 4 |
| BCLC classification C | 4.024 | 4 |
| AJCC cN1 | 3.272 | 3 |
| Chang Gung-Poh Ai Cumulative Score | Survivors | Deaths | 90-Day Mortality Rate after Major Hepatectomy |
|---|---|---|---|
| 0 | 17,301 | 422 | 2.44% |
| 1 | 16,552 | 445 | 2.69% |
| 2 | 8651 | 337 | 3.90% |
| 3 | 4067 | 207 | 5.09% |
| 4 | 3398 | 186 | 5.47% |
| 5 | 4287 | 250 | 5.83% |
| 6 | 2719 | 224 | 8.24% |
| 7 | 1257 | 147 | 11.69% |
| 8 | 676 | 100 | 14.79% |
| 9 | 438 | 94 | 21.46% |
| 10 | 344 | 103 | 29.94% |
| 11 | 218 | 60 | 27.52% |
| 12 | 112 | 34 | 30.36% |
| 13 | 71 | 23 | 32.39% |
| 14 | 61 | 32 | 52.46% |
| 15 | 25 | 13 | 52.00% |
| 16 | 24 | 17 | 70.83% |
| 17 | 6 | 3 | 50.00% |
| 18+ | 43 | 28 | 65.12% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soong, R.-S.; Chen, Y.-C.; Chou, T.-C.; Chiang, P.-H.; Chen, W.-M.; Chiang, M.-F.; Shia, B.-C.; Wu, S.-Y. A Novel Predictive Scoring System for 90-Day Mortality among Patients with Hepatocellular Cell Carcinoma Receiving Major Hepatectomy. Cancers 2022, 14, 1398. https://doi.org/10.3390/cancers14061398
Soong R-S, Chen Y-C, Chou T-C, Chiang P-H, Chen W-M, Chiang M-F, Shia B-C, Wu S-Y. A Novel Predictive Scoring System for 90-Day Mortality among Patients with Hepatocellular Cell Carcinoma Receiving Major Hepatectomy. Cancers. 2022; 14(6):1398. https://doi.org/10.3390/cancers14061398
Chicago/Turabian StyleSoong, Ruey-Shyang, Yi-Chan Chen, Ta-Chun Chou, Po-Hsing Chiang, Wan-Ming Chen, Ming-Feng Chiang, Ben-Chang Shia, and Szu-Yuan Wu. 2022. "A Novel Predictive Scoring System for 90-Day Mortality among Patients with Hepatocellular Cell Carcinoma Receiving Major Hepatectomy" Cancers 14, no. 6: 1398. https://doi.org/10.3390/cancers14061398