
High Expression of NT5DC2 Is a Negative Prognostic Marker in Pulmonary Adenocarcinoma

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Collective
2.2. Protein Expression Analysis and Immunohistochemistry
2.3. Gene Expression Analysis
2.4. Post-Hoc Correlations with Cancer Associated Fibroblasts
2.5. Statistical Analysis
3. Results
3.1. Protein Expression Cohort Analysis
3.2. Gene Expression Cohort Analysis
3.3. NT5DC2 Protein and Gene Expression
3.4. p53 Clinical Characterization in the Context of NT5DC2
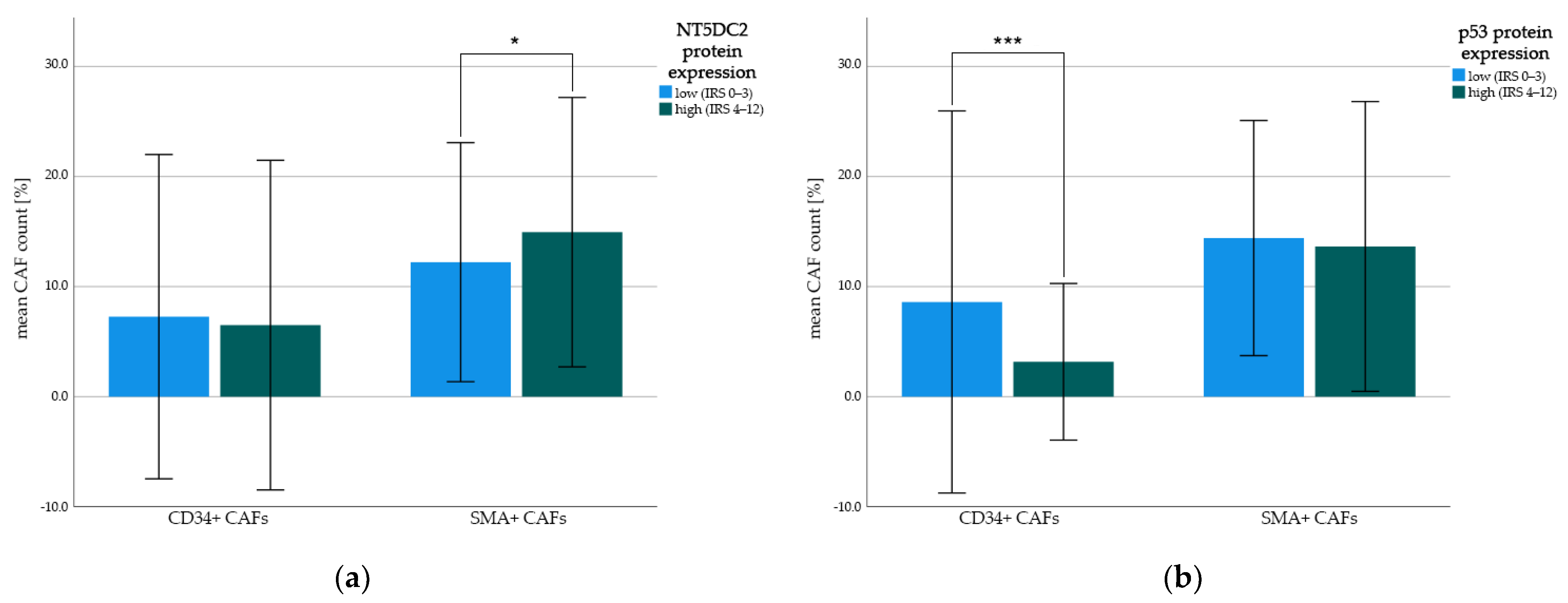
3.5. Post-Hoc Correlation of NT5DC2 and p53 Protein Expression with Cancer Associated Fibroblasts (CAFs)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulze, A.B.; Evers, G.; Kerkhoff, A.; Mohr, M.; Schliemann, C.; Berdel, W.E.; Schmidt, L.H. Future Options of Molecular-Targeted Therapy in Small Cell Lung Cancer. Cancers 2019, 11, 690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, J.; Lim, J.S.; Jang, S.J.; Cun, Y.; Ozretia, L.; Kong, G.; Leenders, F.; Lu, X.; Fernández-Cuesta, L.; Bosco, G.; et al. Comprehensive genomic profiles of small cell lung cancer. Nature 2015, 524, 47–53. [Google Scholar] [CrossRef] [PubMed]
- König, D.; Savic Prince, S.; Rothschild, S.I. Targeted Therapy in Advanced and Metastatic Non-Small Cell Lung Cancer. An Update on Treatment of the Most Important Actionable Oncogenic Driver Alterations. Cancers 2021, 13, 804. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Li, B.T.; Dy, G.K.; Price, T.J.; Falchook, G.S.; Wolf, J.; Italiano, A.; Schuler, M.; Borghaei, H.; Barlesi, F.; et al. Sotorasib for Lung Cancers with KRAS p.G12C Mutation. N. Engl. J. Med. 2021, 384, 2371–2381. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR -Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.-W.; Kato, T.; et al. Osimertinib in Resected EGFR-Mutated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef]
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.-W.; Ou, S.-H.I.; Pérol, M.; Dziadziuszko, R.; Rosell, R.; et al. Alectinib versus Crizotinib in Untreated ALK-Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 829–838. [Google Scholar] [CrossRef]
- Planchard, D.; Besse, B.; Groen, H.J.M.; Souquet, P.-J.; Quoix, E.; Baik, C.S.; Barlesi, F.; Kim, T.M.; Mazieres, J.; Novello, S.; et al. Dabrafenib plus trametinib in patients with previously treated BRAFV600E-mutant metastatic non-small cell lung cancer: An open-label, multicentre phase 2 trial. Lancet Oncol. 2016, 17, 984–993. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Smit, E.F.; Groen, H.J.M.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M.; Zhang, P.; Mookerjee, B.; et al. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: An open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1307–1316. [Google Scholar] [CrossRef]
- Drilon, A.; Oxnard, G.R.; Tan, D.S.W.; Loong, H.H.F.; Johnson, M.; Gainor, J.; McCoach, C.E.; Gautschi, O.; Besse, B.; Cho, B.C.; et al. Efficacy of Selpercatinib in RET Fusion–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Ou, S.-H.I.; Bang, Y.-J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-Rearranged Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2014, 371, 1963–1971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doebele, R.C.; Drilon, A.; Paz-Ares, L.; Siena, S.; Shaw, A.T.; Farago, A.F.; Blakely, C.M.; Seto, T.; Cho, B.C.; Tosi, D.; et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: Integrated analysis of three phase 1–2 trials. Lancet Oncol. 2020, 21, 271–282. [Google Scholar] [CrossRef]
- Passaro, A.; Attili, I.; Rappa, A.; Vacirca, D.; Ranghiero, A.; Fumagalli, C.; Guarize, J.; Spaggiari, L.; de Marinis, F.; Barberis, M.; et al. Genomic Characterization of Concurrent Alterations in Non-Small Cell Lung Cancer (NSCLC) Harboring Actionable Mutations. Cancers 2021, 13, 2172. [Google Scholar] [CrossRef]
- Peng, P.; Lv, G.; Hu, J.; Wang, K.; Lv, J.; Guo, G. Co-mutations of epidermal growth factor receptor and BRAF in Chinese non-small cell lung cancer patients. Ann. Transl. Med. 2021, 9, 1321. [Google Scholar] [CrossRef]
- Nagasaka, M.; Singh, V.; Baca, Y.; Sukari, A.; Kim, C.; Mamdani, H.; Spira, A.I.; Uprety, D.; Bepler, G.; Kim, E.S.; et al. The Effects of HER2 Alterations in EGFR Mutant Non-small Cell Lung Cancer. Clin. Lung Cancer 2022, 23, 52–59. [Google Scholar] [CrossRef]
- Fumagalli, C.; Vacirca, D.; Rappa, A.; Passaro, A.; Guarize, J.; Rafaniello Raviele, P.; de Marinis, F.; Spaggiari, L.; Casadio, C.; Viale, G.; et al. The long tail of molecular alterations in non-small cell lung cancer: A single-institution experience of next-generation sequencing in clinical molecular diagnostics. J. Clin. Pathol. 2018, 71, 767–773. [Google Scholar] [CrossRef]
- Freire Boullosa, L.; Van Loenhout, J.; Flieswasser, T.; De Waele, J.; Hermans, C.; Lambrechts, H.; Cuypers, B.; Laukens, K.; Bartholomeus, E.; Siozopoulou, V.; et al. Auranofin reveals therapeutic anticancer potential by triggering distinct molecular cell death mechanisms and innate immunity in mutant p53 non-small cell lung cancer. Redox Biol. 2021, 42, 101949. [Google Scholar] [CrossRef]
- Jin, X.; Liu, X.; Zhang, Z.; Xu, L. NT5DC2 suppression restrains progression towards metastasis of non-small-cell lung cancer through regulation p53 signaling. Biochem. Biophys. Res. Commun. 2020, 533, 354–361. [Google Scholar] [CrossRef]
- Zhu, Z.; Hou, Q.; Guo, H. NT5DC2 knockdown inhibits colorectal carcinoma progression by repressing metastasis, angiogenesis and tumor-associated macrophage recruitment: A mechanism involving VEGF signaling. Exp. Cell Res. 2020, 397, 112311. [Google Scholar] [CrossRef]
- Hu, B.; Zhou, S.; Hu, X.; Zhang, H.; Lan, X.; Li, M.; Wang, Y.; Hu, Q. NT5DC2 promotes leiomyosarcoma tumour cell growth via stabilizing unpalmitoylated TEAD4 and generating a positive feedback loop. J. Cell. Mol. Med. 2021, 25, 5976–5987. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Ran, H.; Xiao, D.; Huang, H.; Mi, L.; Wang, X.; Chen, L.; Li, D.; Zhang, S.; Han, Q.; et al. NT5DC2 promotes tumorigenicity of glioma stem-like cells by upregulating fyn. Cancer Lett. 2019, 454, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Cao, J.; Wang, P.; He, X. NT5DC2 is a novel prognostic marker in human hepatocellular carcinoma. Oncol. Lett. 2020, 20, 70. [Google Scholar] [CrossRef] [PubMed]
- Tsim, S.; O’Dowd, C.A.; Milroy, R.; Davidson, S. Staging of non-small cell lung cancer (NSCLC): A review. Respir. Med. 2010, 104, 1767–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boeckx, B.; Shahi, R.B.; Smeets, D.; De Brakeleer, S.; Decoster, L.; Van Brussel, T.; Galdermans, D.; Vercauter, P.; Decoster, L.; Alexander, P.; et al. The genomic landscape of nonsmall cell lung carcinoma in never smokers. Int. J. Cancer 2020, 146, 3207–3218. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-M. Update of epidermal growth factor receptor-tyrosine kinase inhibitors in non-small-cell lung cancer. J. Chin. Med. Assoc. 2013, 76, 249–257. [Google Scholar] [CrossRef] [Green Version]
- Kwak, E.L.; Bang, Y.-J.; Camidge, D.R.; Shaw, A.T.; Solomon, B.; Maki, R.G.; Ou, S.-H.I.; Dezube, B.J.; Jänne, P.A.; Costa, D.B.; et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 1693–1703. [Google Scholar] [CrossRef] [Green Version]
- Jurmeister, P.; Lenze, D.; Berg, E.; Mende, S.; Schäper, F.; Kellner, U.; Herbst, H.; Sers, C.; Budczies, J.; Dietel, M.; et al. Lung Cancer Parallel screening for ALK, MET and ROS1 alterations in non-small cell lung cancer with implications for daily routine testing. Lung Cancer 2015, 87, 122–129. [Google Scholar] [CrossRef]
- Shea, M.; Costa, D.B.; Rangachari, D. Management of advanced non-small cell lung cancers with known mutations or rearrangements: Latest evidence and treatment approaches. Ther. Adv. Respir. Dis. 2016, 10, 113–129. [Google Scholar] [CrossRef] [Green Version]
- Győrffy, B.; Surowiak, P.; Budczies, J.; Lánczky, A. Online Survival Analysis Software to Assess the Prognostic Value of Biomarkers Using Transcriptomic Data in Non-Small-Cell Lung Cancer. PLoS ONE 2013, 8, e82241. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, L.H.; Biesterfeld, S.; Kümmel, A.; Faldum, A.; Sebastian, M.; Taube, C.; Buhll, R.; Wiewrodt, R. Tissue microarrays are reliable tools for the clinicopathological characterization of lung cancer tissue. Anticancer Res. 2009, 29, 201–209. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19331151 (accessed on 3 March 2022). [PubMed]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. Available online: http://www.ncbi.nlm.nih.gov/pubmed/3303008 (accessed on 5 February 2022). [PubMed]
- Fedchenko, N.; Reifenrath, J. Different approaches for interpretation and reporting of immunohistochemistry analysis results in the bone tissue—A review. Diagn. Pathol. 2014, 9, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Wang, X.; Huang, S.; Wang, L.; Han, L.; Yu, S. Prognostic roles of Notch receptor mRNA expression in human ovarian cancer. Oncotarget 2017, 8, 32731–32740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulze, A.B.; Schmidt, L.H.; Heitkötter, B.; Huss, S.; Mohr, M.; Marra, A.; Hillejan, L.; Görlich, D.; Barth, P.J.; Rehkämper, J.; et al. Prognostic impact of CD34 and SMA in cancer-associated fibroblasts in stage I–III NSCLC. Thorac. Cancer 2020, 11, 120–129. [Google Scholar] [CrossRef]
- Schröder, M.S.; Culhane, A.C.; Quackenbush, J.; Haibe-Kains, B. survcomp: An R/Bioconductor package for performance assessment and comparison of survival models. Bioinformatics 2011, 27, 3206–3208. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.; Lin, J. Δ133p53 decreases the chemosensitivity of carcinoma cell line H1299. Cell Biol. Int. 2019, 43, 960–964. [Google Scholar] [CrossRef]
- Roth, I.; Campbell, H.; Rubio, C.; Vennin, C.; Wilson, M.; Wiles, A.; Williams, G.; Woolley, A.; Timpson, P.; Berridge, M.V.; et al. The Δ133p53 isoform and its mouse analogue Δ122p53 promote invasion and metastasis involving pro-inflammatory molecules interleukin-6 and CCL2. Oncogene 2016, 35, 4981–4989. [Google Scholar] [CrossRef]
- Chen, J.; Wu, X.; Lin, J.; Levine, A.J. mdm-2 inhibits the G1 arrest and apoptosis functions of the p53 tumor suppressor protein. Mol Cell Biol. 1996, 16, 2445–2452. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Qi, F.; Zhao, F.; Li, G.; Shao, S.; Zhang, X.; Yuan, L.; Feng, Y. Cancer-associated fibroblasts enhance tumor-associated macrophages enrichment and suppress NK cells function in colorectal cancer. Cell Death Dis. 2019, 10, 273. [Google Scholar] [CrossRef] [Green Version]
- Pape, J.; Magdeldin, T.; Stamati, K.; Nyga, A.; Loizidou, M.; Emberton, M.; Cheema, U. Cancer-associated fibroblasts mediate cancer progression and remodel the tumouroid stroma. Br. J. Cancer 2020, 123, 1178–1190. [Google Scholar] [CrossRef] [PubMed]
- Barth, P.J.; Ebrahimsade, S.; Hellinger, A.; Moll, R.; Ramaswamy, A. CD34+ fibrocytes in neoplastic and inflammatory pancreatic lesions. Virchows Arch. 2002, 440, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Barth, P.J.; Schenck zu Schweinsberg, T.; Ramaswamy, A.; Moll, R. CD34 + fibrocytes, a-smooth muscle antigen-positive myofibroblasts, and CD117 expression in the stroma of invasive squamous cell carcinomas of the oral cavity, pharynx, and larynx. Virchows Arch. 2004, 444, 231–234. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total Cohort | NT5DC2 Low | NT5DC2 High | |||||
|---|---|---|---|---|---|---|---|---|
| ntotal = 252 | % * | n = 107 | % * | n = 145 | % * | p-Value | ||
| Age (Years) | Mean (±SD) | 65.9 (±8.5) | 64.8 (±7.6) | 66.8 (±9.0) | 0.059 a | |||
| Sex | male | 206 | 81.7 | 86 | 80.4 | 120 | 58.3 | 0.625 c |
| female | 46 | 18.3 | 21 | 19.6 | 25 | 17.2 | ||
| ECOG | 0 | 33 | 13.1 | 16 | 15.0 | 17 | 11.7 | 0.253 b |
| I | 200 | 79.4 | 85 | 79.4 | 115 | 79.3 | ||
| II–III | 19 | 7.5 | 6 | 5.6 | 13 | 9.0 | ||
| FEV1 (% pred.) | mean (±SD) | 80.5 (±20.3) | 80.6 (±20.8) | 80.4 (±20.0) | 0.950 a | |||
| median (Q1–Q3) | 81 (65–96) | 82 (64–95.5) | 81 (65.5–96.0) | 0.999 b | ||||
| Smoking status | non-smoker | 54 | 21.5 | 20 | 18.7 | 34 | 23.6 | 0.438 c |
| (* n = 251) | smoker | 197 | 78.5 | 87 | 81.3 | 110 | 76.4 | |
| Histopathology | squamous cell (SCC) | 121 | 48.0 | 55 | 51.4 | 66 | 45.5 | 0.534 d |
| adeno (ADC) | 89 | 35.3 | 37 | 34.6 | 52 | 35.9 | ||
| large cell (LCC) | 42 | 16.7 | 15 | 14.0 | 27 | 18.6 | ||
| p53 IHC | low (IRS 0–3) | 151 | 64.3 | 70 | 73.7 | 81 | 57.9 | 0.018 c |
| (* n = 235) | high (IRS 4–12) | 84 | 35.7 | 25 | 26.3 | 59 | 42.1 | |
| p53 IHC | mean (±SD) | 2.8 (±3.4) | 2.1 (±3.2) | 3.3 (±3.5) | 0.009 a | |||
| (* n = 235) | median (Q1–Q3) | 1.0 (0.0–5.0) | 0.0 (0.0–4.0) | 1.8 (0.0–6.0) | 0.002 b | |||
| Grade (* n = 249) | G1 | 1 | 0.4 | 1 | 0.9 | 0 | 0.0 | 0.080 b |
| G2 | 78 | 31.0 | 41 | 38.3 | 37 | 26.1 | ||
| G3 | 135 | 53.6 | 50 | 46.7 | 85 | 59.9 | ||
| G4 | 35 | 13.9 | 15 | 14.0 | 20 | 14.1 | ||
| Resection | R0 | 237 | 94.0 | 98 | 91.6 | 139 | 95.9 | 0.159 b |
| R1 | 13 | 5.2 | 8 | 7.5 | 5 | 3.4 | ||
| R2 | 2 | 0.8 | 1 | 0.9 | 1 | 0.7 | ||
| UICC6 pT | pT1 | 163 | 27.4 | 36 | 33.6 | 33 | 22.8 | 0.251 b |
| pT2 | 55 | 58.3 | 54 | 50.5 | 93 | 64.1 | ||
| pT3 | 34 | 10.3 | 13 | 12.1 | 13 | 9.0 | ||
| pT4 | 10 | 4.0 | 4 | 3.7 | 6 | 4.1 | ||
| UICC6 pN | pN0 | 163 | 64.7 | 73 | 68.2 | 90 | 62.1 | 0.372 b |
| pN1 | 55 | 21.8 | 20 | 18.7 | 35 | 24.1 | ||
| pN2 | 34 | 13.5 | 14 | 13.1 | 20 | 13.8 | ||
| UICC6 cM | cM0 | 252 | 100.0 | 107 | 100.0 | 145 | 100.0 | 1.000 b |
| UICC6 pTNM | stage I | 140 | 55.6 | 64 | 59.8 | 76 | 52.4 | 0.331 b |
| stage II | 66 | 26.2 | 24 | 22.4 | 42 | 29.0 | ||
| stage III | 46 | 18.3 | 19 | 17.8 | 27 | 18.6 | ||
| PFS (months) | median (95% CI) | 32.7 (22.4–42.9) | 44.3 (9.2–79.4) | 30.8 (22.0–39.5) | 0.144 e | |||
| OS (months) | median (95% CI) | 43.9 (32.2–55.5) | 58.1 (32.6–83.6) | 38.6 (29.0–48.1) | 0.146 e | |||
| Follow up (months) | median (95% CI) | 89.4 (84.1–94.7) | 94.7 (86.8–102.6) | 85.3 (82.5–88.1) | 0.206 e | |||
| Variables | Total Cohort | NT5DC2 mRNA Low | NT5DC2 mRNA High | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| ntotal = 1925 | % * | n = 963 | % * | n = 962 | % * | |||
| Sex (* n = 1814) | male | 1100 | 60.6 | 550 | 60.6 | 550 | 60.7 | # |
| female | 714 | 39.4 | 358 | 39.4 | 356 | 39.3 | ||
| unknown | 111 | 55 | 56 | |||||
| Smoking status (* n = 1025) | non-smoker | 205 | 20.0 | 102 | 19.9 | 103 | 20.1 | # |
| smoker | 820 | 80.0 | 410 | 80.1 | 410 | 79.9 | ||
| unknown | 900 | 451 | 449 | |||||
| Histopathology (* n = 1243) | squamous cell (SCC) | 524 | 42.2 | 262 | 42.1 | 262 | 42.1 | 1.000 c |
| adeno (ADC) | 719 | 57.8 | 360 | 57.9 | 359 | 57.9 | ||
| unknown | 682 | 341 | 341 | |||||
| TP53 mRNA | low (<median expr.) | 962 | 50.0 | 666 | 69.2 | 296 | 30.8 | <0.001 c |
| high (≥median expr.) | 963 | 50.0 | 297 | 30.8 | 666 | 69.2 | ||
| TP53 mRNA | mean (±SD) | 584.2 (±428.4) | 423.2 (±346.2) | 745.4 (±442.1) | <0.001 a <0.001 b | |||
| median (Q1–Q3) | 488.0 (253.0–795.0) | 303.0 (101.0–570.0) | 681.5 (432.8–972.0) | |||||
| Grade (* n = 588) | G1 | 201 | 34.2 | 100 | 34.1 | 101 | 34.2 | # |
| G2 | 310 | 52.7 | 155 | 52.9 | 155 | 52.5 | ||
| G3 | 77 | 13.1 | 38 | 13.0 | 39 | 23.2 | ||
| unknown | 1337 | 670 | 667 | |||||
| Resection (* n = 726) | R0 | 726 | 100.0 | 363 | 100.0 | 363 | 100.0 | - |
| unknown | 1199 | 0 | 600 | 0 | 599 | |||
| AJCC pT (* n = 1153) | pT1 | 437 | 37.9 | 218 | 37.9 | 219 | 37.9 | # |
| pT2 | 589 | 51.1 | 294 | 51.1 | 295 | 51.0 | ||
| pT3 | 81 | 7.0 | 40 | 7.0 | 41 | 7.1 | ||
| pT4 | 46 | 4.0 | 23 | 4.0 | 23 | 4.0 | ||
| unknown | 772 | 388 | 384 | |||||
| AJCC pN (* n = 1144) | pN0 | 781 | 68.3 | 392 | 68.3 | 389 | 68.2 | # |
| pN1 | 252 | 22.0 | 126 | 22.0 | 126 | 22.1 | ||
| pN2 | 111 | 9.7 | 56 | 9.8 | 55 | 9.6 | ||
| unknown | 781 | 389 | 392 | |||||
| AJCC pM1 (* n = 691) | pM0 | 681 | 98.6 | 341 | 98.6 | 340 | 98.6 | # |
| pM1 | 10 | 1.4 | 5 | 1.4 | 5 | 1.4 | ||
| unknown | 1234 | 617 | 617 | |||||
| AJCC pTNM (* n = 895) | stage I | 577 | 64.5 | 288 | 64.4 | 289 | 64.5 | # |
| stage II | 244 | 27.3 | 122 | 27.3 | 122 | 27.2 | ||
| stage III | 70 | 7.8 | 35 | 7.8 | 35 | 7.8 | ||
| stage IV | 4 | 0.4 | 2 | 0.4 | 2 | 0.4 | ||
| unknown | 1030 | 516 | 514 | |||||
| PFS (months) (* n = 982) | median (95% CI) | 88.7 (n.e.–n.e.) | n.e. (n.e.–n.e.) | 53.2 (36.1–70.2) | <0.001 d | |||
| OS (months) | median (95% CI) | 69.0 (62.9–75.1) | 77.8 (67.4–88.1) | 59.0 (50.5–67.5) | <0.001 d | |||
| Follow up (months) | median (95% CI) | 69.4 (66.9–71.9) | 69.0 (65.7–72.3) | 71.8 (68.0–75.6) | 0.081 d | |||
| NT5DC2 Protein Expression | Mean (±SD) IHC IRS | p-Value | Median (Q1–Q3) IHC IRS | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| Overall | 4.21 (±3.03) | 4.0 (2.0–6.0) | ||||||
| Histology | ||||||||
| SCC | 3.95 (±2.88) | 0.221 a | 4.0 (2.0–5.0) | 0.328 b | ||||
| ADC | 4.49 (±3.37) | 4.0 (2.0–8.0) | ||||||
| UICC 6 pT | 0.181 c | 0.122 d | ||||||
| pT1 | 3.78 (±2.96) | 0.073 a | 3.0 (2.0–6.0) | 0.045 b | ||||
| pT2 | 4.57 (±3.04) | 0.157 a | 4.0 (2.0–6.0) | 0.092 b | ||||
| pT3 | 3.62 (±3.11) | 0.988 a | 3.5 (1.8–4.0) | 0.718 b | ||||
| pT4 | 3.60 (±2.63) | 4.0 (1.5–6.0) | ||||||
| UICC 6 pN | 0.114 c | 0.345 d | ||||||
| pN0 | 3.95 (±2.78) | 0.259 a | 4.0 (2.0–6.0) | 0.282 b | ||||
| pN1 | 4.49 (±3.13) | 0.467 a | 4.0 (2.0–8.0) | 0.706 b | ||||
| pN2 | 5.06 (±3.80) | 4.0 (2.0–8.0) | ||||||
| Grading | 0.342 c | 0.259 d | ||||||
| G1 | 1.00 (±n.e.) | 0.333 a | 1.0 (1.0–1.0) | 0.221 b | ||||
| G2 | 3.79 (±2.85) | 0.132 a | 3.0 (2.0–6.0) | 0.140 b | ||||
| G3 | 4.44 (±3.21) | 0.607 a | 4.0 (2.0–6.0) | 0.814 b | ||||
| G4 | 4.17 (±2.56) | 4.0 (2.0–6.0) | ||||||
| p53 IHC | ||||||||
| low (IRS 0–3) | 4.02 (±3.13) | 0.071 a | 4.0 (2.0–6.0) | 0.073 b | ||||
| high (IRS 4–12) | 4.75 (±2.85) | 4.0 (3.0–6.0) | ||||||
| NT5DC2 Gene Expression | Mean (±SD) mRNA Count | p-Value | Median (Q1–Q3) mRNA Count | p-Value | ||||
| Overall | 636.2 (±454.6) | 547.0 (330.0–835.0) | ||||||
| Histology | ||||||||
| SCC | 641.7 (±434.4) | <0.001 a | 570.5 (335.3–858.5) | <0.001 b | ||||
| ADC | 478.3 (±355.6) | 387.0 (257.0–613.0) | ||||||
| AJCC pT | 0.568 c | 0.647 d | ||||||
| pT1 | 706.0 (±431.6) | 0.485 a | 635.0 (464.5–866.0) | 0.981 b | ||||
| pT2 | 725.0 (±427.9) | 0.554 a | 621.0 (434.5–902.0) | 0.829 b | ||||
| pT3 | 698.5 (±370.7) | 0.244 a | 652.0 (384.0–972.0) | 0.321 b | ||||
| pT4 | 791.2 (±457.2) | 705.5 (470.5–1071.3) | ||||||
| AJCC pN | 0.001 c | 0.001 d | ||||||
| pN0 | 707.5 (±426.5) | 0.354 a | 636.0 (449.0–870.0) | 0.183 b | ||||
| pN1 | 680.5 (±392.4) | 0.001 a | 576.5 (407.5–886.3) | <0.001 b | ||||
| pN2 | 848.9 (±436.4) | 770.0 (528.0–1122.0) | ||||||
| Grading | 0.273 c | 0.821 d | ||||||
| G1 | 844.8 (±580.2) | 0.364 a | 736.0 (479.0–1066.0) | 0.898 b | ||||
| G2 | 802.9 (±374.9) | 0.190 a | 722.0 (558.0–947.0) | 0.521 b | ||||
| G3 | 751.8 (±284.0) | 695.0 (563.0–888.0) | ||||||
| TP53 mRNA | ||||||||
| low (<median) | 501.1 (±380.8) | <0.001 a | 390.5 (251.0–635.3) | <0.001 b | ||||
| high (≥median) | 771.2 (±481.5) | 679.0 (484.0–952.0) | ||||||
| (A) Protein Expression Cohort | ||||||
| Histology | p53 Expression (IRS) 1 | NT5DC2 Expression (IRS) 1 | Median OS (95% CI) (Months) | p4 | Hazard Ratio (95% CI) | p5 |
| SCC | Low | Low | 23.8 (15.3–32.3) | 0.402 | * | 0.403 |
| High | 29.4 (17.1–41.7) | 0.78 (0.44–1.39) | ||||
| High | Low | 43.9 (3.8–83.9) | 0.466 | * | 0.467 | |
| High | 38.6 (15.6–61.5) | 0.78 (0.39–1.54) | ||||
| ADC | Low | Low | n.e. (n.e.) 3 | 0.021 | * | 0.025 |
| High | 48.7 (33.0–64.3) | 2.35 (1.12–4.97) | ||||
| High | Low | 10.4 (5.8–15.0) | 0.017 | * | 0.032 | |
| High | 90.9 (30.4–151.3) | 0.19 (0.04–0.86) | ||||
| (B) Gene Expression Cohort | ||||||
| Histology | TP53 Expression (mRNA) 2 | NT5DC2 Expression (mRNA) 2 | Median OS (95% CI) (Months) | p4 | Hazard Ratio (95% CI) | p5 |
| SCC | Low | Low | 51.5 (31.5–71.6) | 0.200 | * | 0.201 |
| High | 62.2 (39.7–84.7) | 0.78 (0.53–1.14) | ||||
| High | Low | 37.6 (23.0–52.2) | 0.307 | * | 0.308 | |
| High | 64.1 (35.8–92.4) | 0.84 (0.59–1.18) | ||||
| ADC | Low | Low | 136.3 (n.e.) 3 | <0.001 | * | 0.001 |
| High | 63.0 (23.6–102.4) | 1.86 (1.31–2.64) | ||||
| High | Low | 109.0 (101.6–116.4) | 0.106 | * | 0.108 | |
| High | 75.4 (58.3–92.6) | 1.35 (0.94–1.93) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulze, A.B.; Kuntze, A.; Schmidt, L.H.; Mohr, M.; Marra, A.; Hillejan, L.; Schulz, C.; Görlich, D.; Hartmann, W.; Bleckmann, A.; et al. High Expression of NT5DC2 Is a Negative Prognostic Marker in Pulmonary Adenocarcinoma. Cancers 2022, 14, 1395. https://doi.org/10.3390/cancers14061395
Schulze AB, Kuntze A, Schmidt LH, Mohr M, Marra A, Hillejan L, Schulz C, Görlich D, Hartmann W, Bleckmann A, et al. High Expression of NT5DC2 Is a Negative Prognostic Marker in Pulmonary Adenocarcinoma. Cancers. 2022; 14(6):1395. https://doi.org/10.3390/cancers14061395
Chicago/Turabian StyleSchulze, Arik Bernard, Anna Kuntze, Lars Henning Schmidt, Michael Mohr, Alessandro Marra, Ludger Hillejan, Christian Schulz, Dennis Görlich, Wolfgang Hartmann, Annalen Bleckmann, and et al. 2022. "High Expression of NT5DC2 Is a Negative Prognostic Marker in Pulmonary Adenocarcinoma" Cancers 14, no. 6: 1395. https://doi.org/10.3390/cancers14061395