
Impact of Dose Escalation on the Efficacy of Salvage Radiotherapy for Recurrent Prostate Cancer—A Risk-Adjusted, Matched-Pair Analysis

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bartkowiak, D.; Siegmann, A.; Bohmer, D.; Budach, V.; Wiegel, T. The impact of prostate-specific antigen persistence after radical prostatectomy on the efficacy of salvage radiotherapy in patients with primary N0 prostate cancer. BJU Int. 2019, 124, 785–791. [Google Scholar] [CrossRef]
- Bartkowiak, D.; Thamm, R.; Bottke, D.; Siegmann, A.; Bohmer, D.; Budach, V.; Wiegel, T. Prostate-specific antigen after salvage radiotherapy for postprostatectomy biochemical recurrence predicts long-term outcome including overall survival. Acta Oncol. 2018, 57, 362–367. [Google Scholar] [CrossRef]
- Preisser, F.; Chun, F.K.H.; Pompe, R.S.; Heinze, A.; Salomon, G.; Graefen, M.; Huland, H.; Tilki, D. Persistent Prostate-Specific Antigen After Radical Prostatectomy and Its Impact on Oncologic Outcomes. Eur. Urol. 2019, 76, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Preisser, F.; Coxilha, G.; Heinze, A.; Oh, S.; Chun, F.K.; Sauter, G.; Pompe, R.S.; Huland, H.; Graefen, M.; Tilki, D. Impact of positive surgical margin length and Gleason grade at the margin on biochemical recurrence in patients with organ-confined prostate cancer. Prostate 2019, 79, 1832–1836. [Google Scholar] [CrossRef]
- Fendler, W.P.; Calais, J.; Eiber, M.; Flavell, R.R.; Mishoe, A.; Feng, F.Y.; Nguyen, H.G.; Reiter, R.E.; Rettig, M.B.; Okamoto, S.; et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol. 2019, 5, 856–863. [Google Scholar] [CrossRef] [Green Version]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Pisansky, T.M.; Thompson, I.M.; Valicenti, R.K.; D’Amico, A.V.; Selvarajah, S. Adjuvant and Salvage Radiotherapy after Prostatectomy: ASTRO/AUA Guideline Amendment 2018–2019. J. Urol. 2019, 202, 533–538. [Google Scholar] [CrossRef] [Green Version]
- National Comprehensive Cancer Network. Prostate Cancer (Version 3.2022). 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 3 March 2022).
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Expert Patient Advocate (European Prostate Cancer Coalition/Europa UOMO); De Santis, M.; Gillessen, S.; Grummet, J.; Henry, A.M.; van der Kwast, T.H.; Lam, T.B.; et al. EAU—EANM—ESTRO—ESUR—ISUP—SIOG Guidelines on Prostate Cancer; EAU Guidelines Office: Arnhem, The Netherlands, 2021. [Google Scholar]
- Carrie, C.; Magne, N.; Burban-Provost, P.; Sargos, P.; Latorzeff, I.; Lagrange, J.L.; Supiot, S.; Belkacemi, Y.; Peiffert, D.; Allouache, N.; et al. Short-term androgen deprivation therapy combined with radiotherapy as salvage treatment after radical prostatectomy for prostate cancer (GETUG-AFU 16): A 112-month follow-up of a phase 3, randomised trial. Lancet Oncol. 2019, 20, 1740–1749. [Google Scholar] [CrossRef]
- Shipley, W.U.; Seiferheld, W.; Lukka, H.R.; Major, P.P.; Heney, N.M.; Grignon, D.J.; Sartor, O.; Patel, M.P.; Bahary, J.P.; Zietman, A.L.; et al. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N. Engl. J. Med. 2017, 376, 417–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Broeck, T.; van den Bergh, R.C.N.; Arfi, N.; Gross, T.; Moris, L.; Briers, E.; Cumberbatch, M.; De Santis, M.; Tilki, D.; Fanti, S.; et al. Prognostic Value of Biochemical Recurrence Following Treatment with Curative Intent for Prostate Cancer: A Systematic Review. Eur. Urol. 2019, 75, 967–987. [Google Scholar] [CrossRef] [Green Version]
- Tendulkar, R.D.; Agrawal, S.; Gao, T.; Efstathiou, J.A.; Pisansky, T.M.; Michalski, J.M.; Koontz, B.F.; Hamstra, D.A.; Feng, F.Y.; Liauw, S.L.; et al. Contemporary Update of a Multi-Institutional Predictive Nomogram for Salvage Radiotherapy after Radical Prostatectomy. J. Clin. Oncol. 2016, 34, 3648–3654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishan, A.U.; Tendulkar, R.D.; Tran, P.T.; Parker, C.C.; Nguyen, P.L.; Stephenson, A.J.; Carrie, C. Optimizing the Timing of Salvage Postprostatectomy Radiotherapy and the Use of Concurrent Hormonal Therapy for Prostate Cancer. Eur. Urol. Oncol. 2018, 1, 3–18. [Google Scholar] [CrossRef]
- Michalski, J.M.; Moughan, J.; Purdy, J.; Bosch, W.; Bruner, D.W.; Bahary, J.P.; Lau, H.; Duclos, M.; Parliament, M.; Morton, G.; et al. Effect of Standard vs Dose-Escalated Radiation Therapy for Patients With Intermediate-Risk Prostate Cancer: The NRG Oncology RTOG 0126 Randomized Clinical Trial. JAMA Oncol. 2018, 4, e180039. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.L.; Schmidt, R.; Moiseenko, V.; Olsen, L.A.; Tan, J.; Xiao, Y.; Galvin, J.; Pugh, S.; Seider, M.J.; Dicker, A.P.; et al. Quantifying Unnecessary Normal Tissue Complication Risks due to Suboptimal Planning: A Secondary Study of RTOG 0126. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, X.; Li, H.Z.; Gao, X.S.; Qin, S.B.; Zhang, M.; Li, X.M.; Li, X.Y.; Ma, M.W.; Bai, Y.; Li, X.Y.; et al. Toxicity and Biochemical Outcomes of Dose-Intensified Postoperative Radiation Therapy for Prostate Cancer: Results of a Randomized Phase III Trial. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 282–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghadjar, P.; Hayoz, S.; Bernhard, J.; Zwahlen, D.R.; Holscher, T.; Gut, P.; Polat, B.; Hildebrandt, G.; Muller, A.C.; Plasswilm, L.; et al. Dose-intensified Versus Conventional-dose Salvage Radiotherapy for Biochemically Recurrent Prostate Cancer After Prostatectomy: The SAKK 09/10 Randomized Phase 3 Trial. Eur. Urol. 2021, 80, 306–315. [Google Scholar] [CrossRef]
- Cox, D.R. Regression Models and Life-Tables. J. R. Stat. Soc. 1972, 34, 187–220. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- King, C.R. The dose-response of salvage radiotherapy following radical prostatectomy: A systematic review and meta-analysis. Radiother. Oncol. 2016, 121, 199–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shelan, M.; Abo-Madyan, Y.; Welzel, G.; Bolenz, C.; Kosakowski, J.; Behnam, N.; Wenz, F.; Lohr, F. Dose-escalated salvage radiotherapy after radical prostatectomy in high risk prostate cancer patients without hormone therapy: Outcome, prognostic factors and late toxicity. Radiat. Oncol. 2013, 8, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Angelillo, R.M.; Fiore, M.; Trodella, L.E.; Sciuto, R.; Ippolito, E.; Carnevale, A.; Iurato, A.; Miele, M.; Trecca, P.; Trodella, L.; et al. 18F-choline PET/CT driven salvage radiotherapy in prostate cancer patients: Update analysis with 5-year median follow-up. Radiol. Med. 2020, 125, 668–673. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | <70 Gy (N = 225) | ≥70 Gy (N = 329) | All (N = 554) |
|---|---|---|---|
| Age at RP, years; median (IQR) | 63 (59–67) | 64 (60–68) | 64 (59–68) |
| Pre-RP PSA *, ng/mL; | 10.00 | 8.87 | 9.40 |
| median (IQR) | (7.00–15.16) | (5.98–14.4) | (6.28–14.7) |
| Tumor stage | |||
| pT2 | 107 (48%) | 182 (55%) | 289 (52%) |
| pT3 | 114 (50%) | 142 (43%) | 256 (46%) |
| pT4 | 4 (2%) | 5 (2%) | 9 (2%) |
| Gleason score * | |||
| GS ≤ 6 | 92 (41%) | 96 (29%) | 188 (34%) |
| GS = 7 | 87 (39%) | 167 (51%) | 254 (46%) |
| GS ≥ 8 | 46 (20%) | 66 (20%) | 112 (20%) |
| Surgical margins * | |||
| R0 | 101 (45%) | 201 (61%) | 302 (55%) |
| R1 | 124 (55%) | 128 (39%) | 252 (45%) |
| Pre-SRT PSA, ng/mL; | 0.294 | 0.290 | 0.292 |
| median (IQR) | (0.140–0.690) | (0.180–0.516) | (0.160–0.568) |
| Risk Factors | HR (95% CI) | p |
|---|---|---|
| Pre-RP PSA < 10 * vs. ≥10 ng/ml | 1.14 (0.88–1.47) | 0.3278 |
| pT2 * vs. pT3–4 | 2.13 (1.62–2.79) | <0.0001 |
| GS ≤ 7 * vs. GS 8–10 | 1.60 (1.20–2.14) | 0.0015 |
| Surgical margin R0 * vs. R1 | 0.68 (0.53–0.88) | 0.0031 |
| Pre-SRT PSA < 0.5 * vs. ≥0.5 ng/ml | 1.56 (1.21–2.02) | 0.0007 |
| SAKK 09/10 [18] | Chinese Trial [17] | Own Data | |
|---|---|---|---|
| Type of study | Open-label, multicenter Phase III trial | Randomized controlled Phase III trial | Retrospective cohort |
| Inclusion criteria | Biochemical failure after RP 3 PSA rises or 2 rises with last being 0.1 ng/mL Postoperative PSA-Nadir ≤ 0.4 ng/mL No ADT before or during SRT pT2a-3b No macroscopic relapse Nodal negative | Biochemical failure or PSA persistence after RP (ART/SRT = 48/96 Postoperative PSA-Nadir ≤ 0.4 ng/mL No ADT before or during SRT pT3–4 positive margin Nodal negative | Biochemical failure after RP PSA rise above 0.1 ng/mL No ADT before or during SRT pT3–4 positive margin Nodal negative |
| Treatment groups | 6400 cGy vs. 7000 cGy Target volume: prostatic bed Technique: 3D CRT (44%), IMRT (57%) Assignment to treatment by randomization | 6600 cGy vs. 7200 cGy Target volume: prostatic bed (RTOG-guideline) Technique: IG-IMRT/IG-VMAT High Risk patients: pelvic RT (88%) | <7000 cGy vs. ≥7000 cGy Target volume: prostatic bed +/− seminal vesicle bed (T3/4) Technique: 3D CRT (74.9%), IMRT (25.1%) Matched-Pair-Analysis |
| Primary endpoint | Freedom from biochemical Progression: Definition: PSA-increase ≥ 0.4 ng/mL beyond post-SRT-Nadir | Biochemical PFS: secondary therapy Definition: PSA-increase > 0.2 ng/mL beyond post-SRT-Nadir (x2), OS: death of any cause | PFS, secondary therapy Definition: PSA-increase > 0.2 ng/mL beyond post-SRT-Nadir OS: death of any cause |
| Secondary endpoints | Clinical PFS Time to hormonal therapy, OS Acute and late toxicity Quality of life | Acute and late toxicity Toxicity of hormonal treatment | n.s. |
| Number of patients | 350 Conv. D.: 175 (170 ITT) Escal. D.: 175 (174 ITT) | 144 Conv. D.: 71 Escal. D.: 73 | 554 low dose: 225 high dose: 329 |
| Pre-SRT-PSA-level | 0.3 ng/mL (0.03–1.61) | 0.2 ng/ml | 0.28 ng/mL (0.04–8.87) |
| Follow-Up | 6.2 years (IQR 5.5–7.2) | 48.5 months (14–79 months) | 6.8 years (IQR 4.2–9.2) |
| Time RP–SRT | 6400 cGy: 25.9 mo. (14.0–42.3) 7000 cGy: 30.3 mo. (15.8–50.8) | 8 mo. | 23 mo. (1.7–176) |
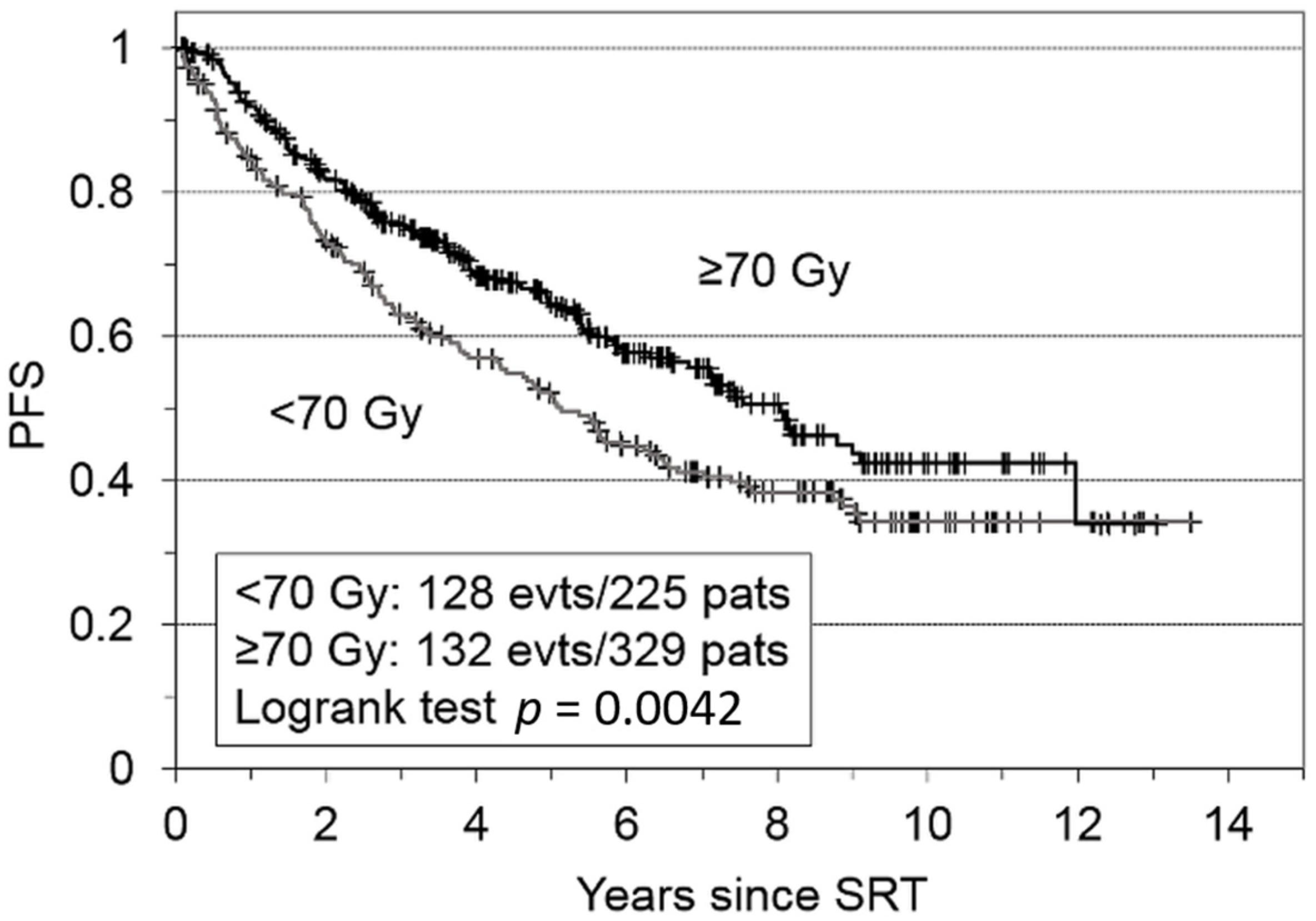
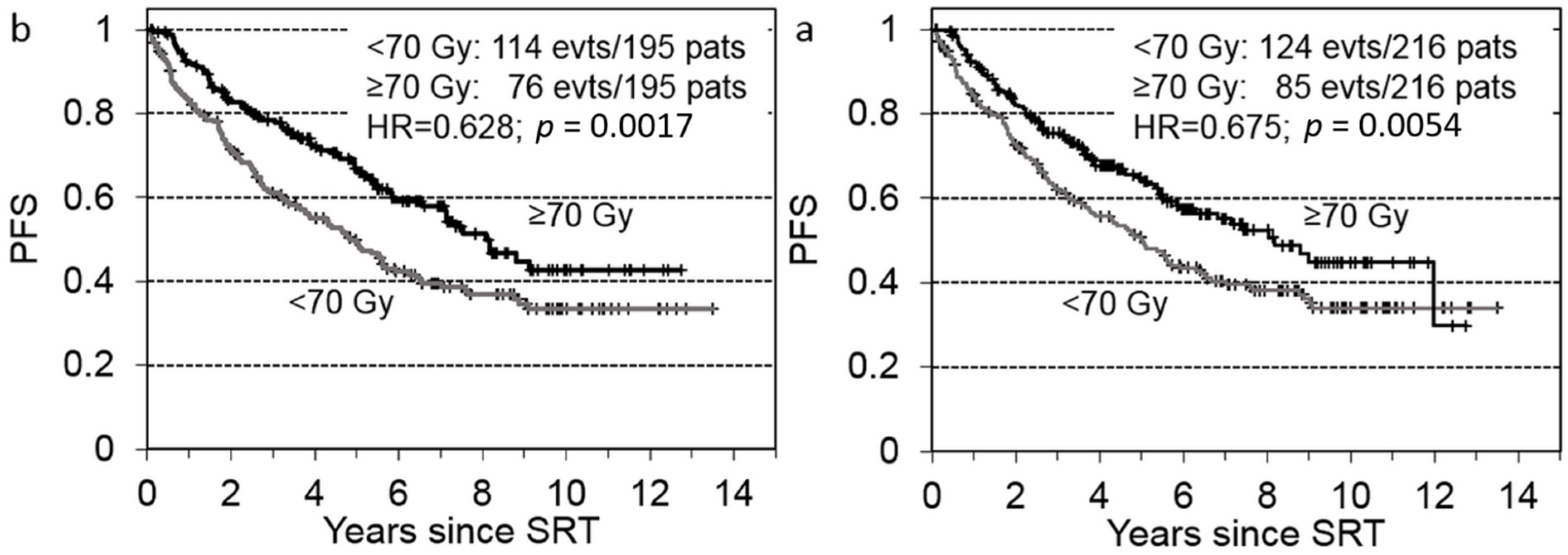
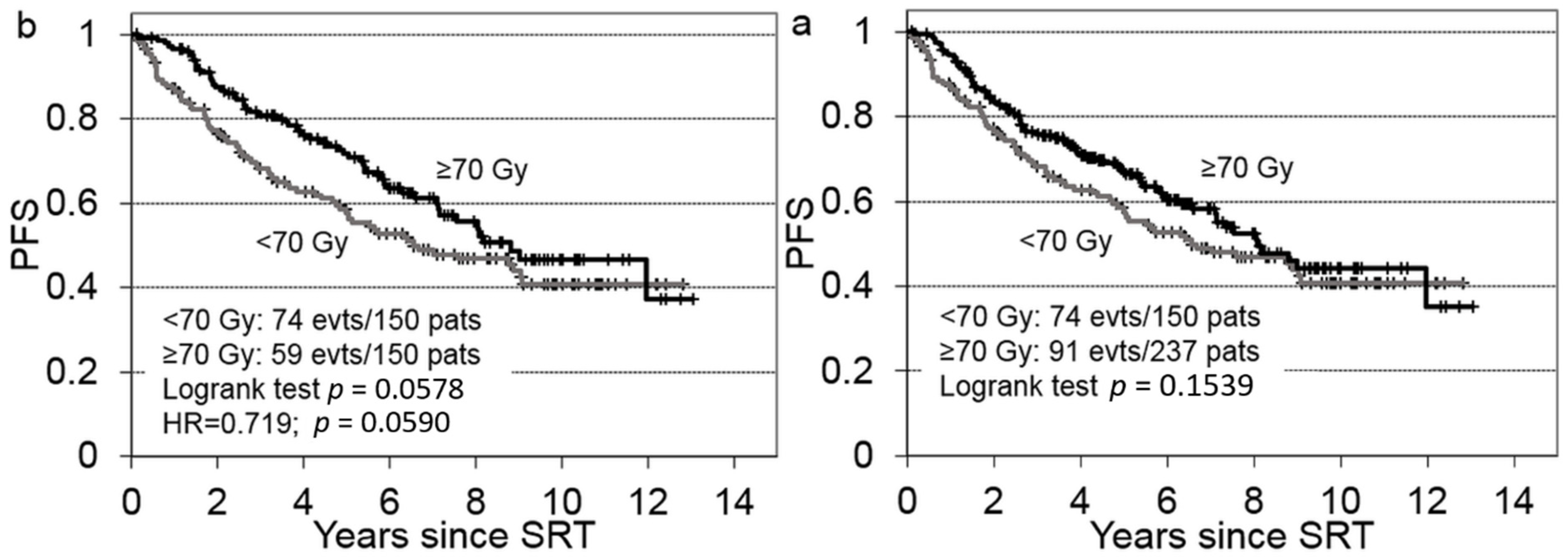
| Results | Reported: 6-year-results 6400 cGy: 62.3% (95% CI: 54.2–69.4) 7000 cGy: 61.3% (95% CI: 53.4–68.3) bPFS: p = 0.44 Hazard-ratio: 1.14 (95% CI: 0.82–1.6) | Reported: 4-year-results 66 Gy: 75.9%; 95% CI, 71.6–79.6% 72 Gy: 82.6%; 95% CI, 78.8–85.7% bPFS: p = 0.299 | Reported: 5-year-results Conventional dose: 52% Escalated dose: 65% PFS: p = 0.0042 Multivariate Analysis: significant improvement favoring: lower pT stage lower Gleason sum positive resection status lower-pre-SRT PSA level |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Böhmer, D.; Siegmann, A.; Scharl, S.; Ruf, C.; Wiegel, T.; Krafcsik, M.; Thamm, R. Impact of Dose Escalation on the Efficacy of Salvage Radiotherapy for Recurrent Prostate Cancer—A Risk-Adjusted, Matched-Pair Analysis. Cancers 2022, 14, 1320. https://doi.org/10.3390/cancers14051320
Böhmer D, Siegmann A, Scharl S, Ruf C, Wiegel T, Krafcsik M, Thamm R. Impact of Dose Escalation on the Efficacy of Salvage Radiotherapy for Recurrent Prostate Cancer—A Risk-Adjusted, Matched-Pair Analysis. Cancers. 2022; 14(5):1320. https://doi.org/10.3390/cancers14051320
Chicago/Turabian StyleBöhmer, Dirk, Alessandra Siegmann, Sophia Scharl, Christian Ruf, Thomas Wiegel, Manuel Krafcsik, and Reinhard Thamm. 2022. "Impact of Dose Escalation on the Efficacy of Salvage Radiotherapy for Recurrent Prostate Cancer—A Risk-Adjusted, Matched-Pair Analysis" Cancers 14, no. 5: 1320. https://doi.org/10.3390/cancers14051320