
Status of the Current Treatment Options and Potential Future Targets in Uterine Leiomyosarcoma: A Review

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
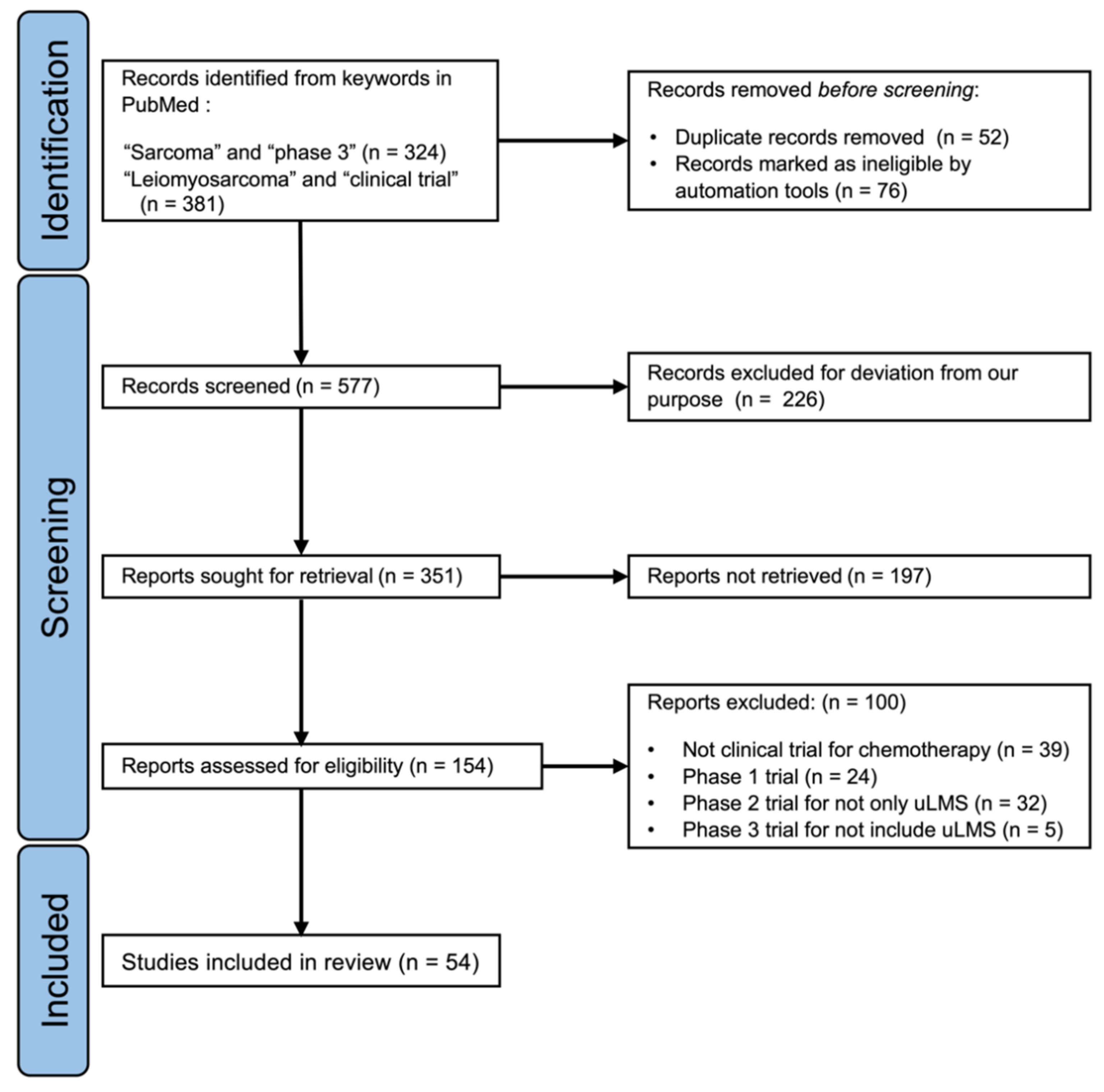
2. Literature Search and Selection
3. Standard Therapy for uLMS
3.1. uLMS Staging and the Overview of Prognosis
3.2. Surgical Procedures and Adjuvant Therapy for uLMS
3.3. First-Line Chemotherapy for Advanced or Recurrent uLMS

{kind=link}
{kind=link}
| Regimen | Year | Patients (n) | LMS (n) | uLMS (n) | ORR (%) | mPFS (Months) | mOS (Months) |
|---|---|---|---|---|---|---|---|
| Dox vs. Dox + CPA [16] | 1985 | 104 | 38 | 38 | 19 vs. 19 | 5.1 vs. 4.9 | 11.6 vs. 10.9 |
| Dox + DTIC bolus vs. infusion [17] | 1991 | 240 | 105 | 27 | 17 vs. 17 | NA | NA |
| GD + placebo vs. GD + Bev [12] | 2015 | 107 | 107 | 107 | 31.5 vs. 35.8 | 6.2 vs. 4.2 | 26.9 vs. 23.3 |
| Dox vs. GD [13] | 2017 | 257 | 118 | 71 | 19 vs. 20 | 5.8 vs. 5.9 | 19.1 vs. 16.8 |
| Dox + placebo vs. Dox + olaratumab [14] | 2020 | 506 | 234 | 94 | 18.3 vs. 14.0 | 6.8 vs. 5.4 | 19.7 vs. 20.4 |
3.4. Second-Line Chemotherapy for Advanced or Recurrent uLMS
| Regimen | Year | Patients (n) | LMS (n) | uLMS (n) | ORR (%) | mPFS (Months) | mOS (Months) |
|---|---|---|---|---|---|---|---|
| PTX [39] | 2003 | 48 | 48 | 48 | 8.4 | NA | NA |
| GEM [40] | 2004 | 42 | 42 | 42 | 20.5 | NA | NA |
| GD [30] | 2008 | 48 | 48 | 48 | 27 * | 6.7 | 14.7 |
| GEM vs. GD [29] | 2012 | 90 | 90 | 46 ** | 19 vs. 24 | 5.5 vs. 4.7 | NA |
| Ixabepilone [41] | 2014 | 23 | 23 | 23 | 0 | 1.4 | NA |
| Letrozole [31] | 2014 | 27 | 27 | 27 | 0 | 3 (PFS-12W 50% *) | NA |
| Nivolumab [32] | 2017 | 12 | 12 | 12 | 0 | 1.8 | NA |
| Alisertib [33] | 2017 | 23 | 23 | 23 | 0 | 1.7 | 14.5 |
| Trabectedin [42] | 2018 | 168 | 168 | 168 | 23.5 | 4.1 (PFS-6M 35.2% *) | 20.6 |
| Thalidomide [43] | 2007 | 29 | 29 | 29 | 0 | 1.9 | 8.3 |
| Sunitinib [34] | 2009 | 23 | 23 | 23 | 8.7 | 1.54 | 15.1 |
4. Homologous Recombination Deficiency in uLMS
4.1. Incidence of Homologous Recombination Deficiency in uLMS
| Authors | Patients (n) | Methods | Deletion | Truncating Mutation |
|---|---|---|---|---|
| Chudasama et al. [51] | 10 | WES | Total: 5 (50%) | 0 |
| Homozygous: 1 (10%) | ||||
| Hemizygous: 4 (40%) | ||||
| Rosenbaum et al. [54] | 121 | MSK-IMPACT™ | Total: 8 (7%) | 3 (2.5%) |
| Homozygous: 8 (7%) | ||||
| Hensley et al. [32] | 80 | MSK-IMPACT™ | Total: 4 (5%) | 2 (2.5%) |
| Homozygous: 4 (5%) | ||||
| Seligson et al. [52] | 61 | Database * | 6 (10%) | 0 |
4.2. Effect of PARP Inhibitors on uLMS
4.3. Clinical Trials for Unresectable Advanced or Recurrent uLMS
5. Designs for Future Clinical Trials
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Toro, J.R.; Travis, L.B.; Wu, H.J.; Zhu, K.; Fletcher, C.D.; Devesa, S.S. Incidence patterns of soft tissue sarcomas, regardless of primary site, in the surveillance, epidemiology and end results program, 1978–2001: An analysis of 26,758 cases. Int. J. Cancer 2006, 119, 2922–2930. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Kawai, A.; Yonemori, K.; Takahashi, S.; Araki, N.; Ueda, T. Systemic therapy for soft tissue sarcoma: Proposals for the optimal use of pazopanib, trabectedin, and eribulin. Adv. Ther. 2017, 34, 1556–1571. [Google Scholar] [CrossRef]
- Japanese Orthopaedic Association Committee on Musculoskeletal Tumor. Soft Tissue Tumor Registry in Japan 2015; Japanese Orthopaedic Association: Tokyo, Japan, 2015. [Google Scholar]
- Bell, S.W.; Kempson, R.L.; Hendrickson, M.R. Problematic uterine smooth muscle neoplasms. A clinicopathologic study of 213 cases. Am. J. Surg Pathol 1994, 18, 535–558. [Google Scholar] [CrossRef] [PubMed]
- Japan Society of Obstetrics and Gynecology, Gynecologic Oncology Committee. Patient Annual Report for 2012–2018; Japan Society of Obstetrics and Gynecology: Tokyo, Japan; Available online: http://plaza.umin.ac.jp/~jsog-go/new5.html (accessed on 26 June 2021).
- Takehara, K.; Yamashita, N.; Watanabe, R.; Teramoto, N.; Tsuda, H.; Motohashi, T.; Harano, K.; Nakanishi, T.; Tokunaga, H.; Susumu, N.; et al. Clinical status and prognostic factors in Japanese patients with uterine leiomyosarcoma. Gynecol. Oncol. 2020, 157, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Chae, S.H.; Shim, S.H.; Chang, M.; Choi, A.Y.; Kang, G.G.; Lee, S.J.; Kim, S.N. Effect of adjuvant therapy on the risk of recurrence in early-stage leiomyosarcoma: A meta-analysis. Gynecol. Oncol. 2019, 154, 638–650. [Google Scholar] [CrossRef]
- Reed, N.S.; Mangioni, C.; Malmstrom, H.; Scarfone, G.; Poveda, A.; Pecorelli, S.; Tateo, S.; Franchi, M.; Jobsen, J.J.; Coens, C.; et al. Phase III randomised study to evaluate the role of adjuvant pelvic radiotherapy in the treatment of uterine sarcomas stages I and II: An European Organisation for Research and Treatment of Cancer Gynaecological Cancer Group Study (protocol 55874). Eur. J. Cancer 2008, 44, 808–818. [Google Scholar] [CrossRef]
- Seagle, B.L.; Sobecki-Rausch, J.; Strohl, A.E.; Shilpi, A.; Grace, A.; Shahabi, S. Prognosis and treatment of uterine leiomyosarcoma: A National Cancer Database study. Gynecol. Oncol. 2017, 145, 61–70. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Uterine Neoplasms. NCCN Guidelines Version 3. 2021. Available online: https://www.nccn.org/login?ReturnURL=https://www.nccn.org/professionals/physician_gls/pdf/uterine.pdf (accessed on 21 June 2021).
- Hensley, M.L.; Miller, A.; O’Malley, D.M.; Mannel, R.S.; Behbakht, K.; Bakkum-Gamez, J.N.; Michael, H. Randomized phase III trial of gemcitabine plus docetaxel plus bevacizumab or placebo as first-line treatment for metastatic uterine leiomyosarcoma: An NRG Oncology/Gynecologic Oncology Group study. J. Clin. Oncol. 2015, 33, 1180–1185. [Google Scholar] [CrossRef]
- Seddon, B.; Strauss, S.J.; Whelan, J.; Leahy, M.; Woll, P.J.; Cowie, F.; Rothermundt, C.; Wood, Z.; Benson, C.; Ali, N.; et al. Gemcitabine and docetaxel versus doxorubicin as first-line treatment in previously untreated advanced unresectable or metastatic soft-tissue sarcomas (GeDDiS): A randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1397–1410. [Google Scholar] [CrossRef] [Green Version]
- Tap, W.D.; Wagner, A.J.; Schoffski, P.; Martin-Broto, J.; Krarup-Hansen, A.; Ganjoo, K.N.; Yen, C.C.; Abdul Razak, A.R.; Spira, A.; Kawai, A.; et al. Effect of doxorubicin plus olaratumab vs doxorubicin plus placebo on survival in patients with advanced soft tissue sarcomas: The ANNOUNCE randomized clinical trial. JAMA 2020, 323, 1266–1276. [Google Scholar] [CrossRef] [PubMed]
- Hensley, M.L.; Blessing, J.A.; Mannel, R.; Rose, P.G. Fixed-dose rate gemcitabine plus docetaxel as first-line therapy for metastatic uterine leiomyosarcoma: A Gynecologic Oncology Group phase II trial. Gynecol. Oncol. 2008, 109, 329–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muss, H.B.; Bundy, B.; DiSaia, P.J.; Homesley, H.D.; Fowler, W.C., Jr.; Creasman, W.; Yordan, E. Treatment of recurrent or advanced uterine sarcoma. A randomized trial of doxorubicin versus doxorubicin and cyclophosphamide (a phase III trial of the Gynecologic Oncology Group). Cancer 1985, 55, 1648–1653. [Google Scholar] [CrossRef]
- Zalupski, M.; Metch, B.; Balcerzak, S.; Fletcher, W.S.; Chapman, R.; Bonnet, J.D.; Weiss, G.R.; Ryan, J.; Benjamin, R.S.; Baker, L.H. Phase III comparison of doxorubicin and dacarbazine given by bolus versus infusion in patients with soft-tissue sarcomas: A Southwest Oncology Group study. J. Natl. Cancer Inst. 1991, 83, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Judson, I.; Verweij, J.; Gelderblom, H.; Hartmann, J.T.; Schöffski, P.; Blay, J.Y.; Kerst, J.M.; Sufliarsky, J.; Whelan, J.; Hohenberger, P.; et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: A randomised controlled phase 3 trial. Lancet Oncol. 2014, 15, 415–423. [Google Scholar] [CrossRef]
- D’Ambrosio, L.; Touati, N.; Blay, J.Y.; Grignani, G.; Flippot, R.; Czarnecka, A.M.; Piperno-Neumann, S.; Martin-Broto, J.; Sanfilippo, R.; Katz, D.; et al. Doxorubicin plus dacarbazine, doxorubicin plus ifosfamide, or doxorubicin alone as a first-line treatment for advanced leiomyosarcoma: A propensity score matching analysis from the European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group. Cancer 2020, 126, 2637–2647. [Google Scholar]
- Takahashi, N.; Li, W.W.; Banerjee, D.; Scotto, K.W.; Bertino, J.R. Sequence-dependent enhancement of cytotoxicity produced by ecteinascidin 743 (ET-743) with doxorubicin or paclitaxel in soft tissue sarcoma cells. Clin. Cancer Res. 2001, 7, 3251–3257. [Google Scholar]
- Pautier, P.; Floquet, A.; Chevreau, C.; Penel, N.; Guillemet, C.; Delcambre, C.; Cupissol, D.; Selle, F.; Isambert, N.; Piperno-Neumann, S.; et al. Trabectedin in combination with doxorubicin for first-line treatment of advanced uterine or soft-tissue leiomyosarcoma (LMS-02): A non-randomised, multicentre, phase 2 trial. Lancet Oncol. 2015, 16, 457–464. [Google Scholar] [CrossRef]
- Pautier, P.; Floquet, A.; Chevreau, C.; Penel, N.; Guillemet, C.; Delcambre, C.; Cupissol, D.; Selle, F.; Isambert, N.; Piperno-Neumann, S.; et al. A single-arm multicentre phase II trial of doxorubicin in combination with trabectedin in the first-line treatment for leiomyosarcoma with long-term follow-up and impact of cytoreductive surgery. ESMO Open 2021, 6, 100209. [Google Scholar] [CrossRef]
- Pautier, P.; Italiano, A.; Piperno-Neumann, S.; Chevreau, C.M.; Penel, N.; Cupissol, D.; Boudou-Rouquette, P.; Bertucci, F.; Balleyguier, C.; Lebrun-Ly, V.; et al. LBA59—LMS-04 study: A randomised, multicenter, phase III study comparing doxorubicin alone versus doxorubicin with trabectedin followed by trabectedin in non-progressive patients as first-line therapy, in patients with metastatic or unresectable leiomyosarcoma—A French Sarcoma Group study. Ann. Oncol. 2021, 32 (Suppl. 5), S1283–S1346. [Google Scholar]
- Van der Graaf, W.T.A.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef]
- Demetri, G.D.; von Mehren, M.; Jones, R.L.; Hensley, M.L.; Schuetze, S.M.; Staddon, A.; Milhem, M.; Elias, A.; Ganjoo, K.; Tawbi, H.; et al. Efficacy and safety of trabectedin or dacarbazine for metastatic liposarcoma or leiomyosarcoma after failure of conventional chemotherapy: Results of a phase III randomized multicenter clinical trial. J. Clin. Oncol. 2016, 34, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Schöffski, P.; Chawla, S.; Maki, R.G.; Italiano, A.; Gelderblom, H.; Choy, E.; Grignani, G.; Camargo, V.; Bauer, S.; Rha, S.Y.; et al. Eribulin versus dacarbazine in previously treated patients with advanced liposarcoma or leiomyosarcoma: A randomised, open-label, multicentre, phase 3 trial. Lancet 2016, 387, 1629–1637. [Google Scholar] [CrossRef]
- Demetri, G.D.; Chawla, S.P.; Ray-Coquard, I.; Le Cesne, A.; Staddon, A.P.; Milhem, M.M.; Penel, N.; Riedel, R.F.; Bui-Nguyen, B.; Cranmer, L.D.; et al. Results of an international randomized phase III trial of the mammalian target of rapamycin inhibitor ridaforolimus versus placebo to control metastatic sarcomas in patients after benefit from prior chemotherapy. J. Clin. Oncol. 2013, 31, 2485–2492. [Google Scholar] [CrossRef]
- Blay, J.-Y.; Pápai, Z.; Tolcher, A.W.; Italiano, A.; Cupissol, D.; López-Pousa, A.; Chawla, S.P.; Bompas, E.; Babovic, N.; Penel, N.; et al. Ombrabulin plus cisplatin versus placebo plus cisplatin in patients with advanced soft-tissue sarcomas after failure of anthracycline and ifosfamide chemotherapy: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2015, 16, 531–540. [Google Scholar] [CrossRef]
- Pautier, P.; Floquet, A.; Penel, N.; Piperno-Neumann, S.; Isambert, N.; Rey, A.; Bompas, E.; Cioffi, A.; Delcambre, C.; Cupissol, D.; et al. Randomized multicenter and stratified phase II study of gemcitabine alone versus gemcitabine and docetaxel in patients with metastatic or relapsed leiomyosarcomas: A Federation Nationale des Centres de Lutte Contre le Cancer (FNCLCC) French Sarcoma Group Study (TAXOGEM study). Oncologist 2012, 17, 1213–1220. [Google Scholar]
- Hensley, M.L.; Blessing, J.A.; Degeest, K.; Abulafia, O.; Rose, P.G.; Homesley, H.D. Fixed-dose rate gemcitabine plus docetaxel as second-line therapy for metastatic uterine leiomyosarcoma: A Gynecologic Oncology Group phase II study. Gynecol. Oncol. 2008, 109, 323–328. [Google Scholar] [CrossRef] [Green Version]
- George, S.; Feng, Y.; Manola, J.; Nucci, M.R.; Butrynski, J.E.; Morgan, J.A.; Ramaiya, N.; Quek, R.; Penson, R.T.; Wagner, A.J.; et al. Phase 2 trial of aromatase inhibition with letrozole in patients with uterine leiomyosarcomas expressing estrogen and/or progesterone receptors. Cancer 2014, 120, 738–743. [Google Scholar] [CrossRef]
- Ben-Ami, E.; Barysauskas, C.M.; Solomon, S.; Tahlil, K.; Malley, R.; Hohos, M.; Polson, K.; Loucks, M.; Severgnini, M.; Patel, T.; et al. Immunotherapy with single agent nivolumab for advanced leiomyosarcoma of the uterus: Results of a phase 2 study. Cancer 2017, 123, 3285–3290. [Google Scholar] [CrossRef] [Green Version]
- Hyman, D.M.; Sill, M.W.; Lankes, H.A.; Piekarz, R.; Shahin, M.S.; Ridgway, M.R.; Backes, F.; Tenney, M.E.; Mathews, C.A.; Hoffman, J.S.; et al. A phase 2 study of alisertib (MLN8237) in recurrent or persistent uterine leiomyosarcoma: An NRG Oncology/Gynecologic Oncology Group study 0231D. Gynecol. Oncol. 2017, 144, 96–100. [Google Scholar] [CrossRef] [Green Version]
- Hensley, M.L.; Sill, M.W.; Scribner, D.R., Jr.; Brown, J.; Debernardo, R.L.; Hartenbach, E.M.; McCourt, C.K.; Bosscher, J.R.; Gehrig, P.A. Sunitinib malate in the treatment of recurrent or persistent uterine leiomyosarcoma: A Gynecologic Oncology Group phase II study. Gynecol. Oncol. 2009, 115, 460–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hensley, M.L.; Chavan, S.S.; Solit, D.B.; Murali, R.; Soslow, R.; Chiang, S.; Jungbluth, A.A.; Bandlamudi, C.; Srinivasan, P.; Tap, W.D.; et al. Genomic landscape of uterine sarcomas defined through prospective clinical sequencing. Clin. Cancer Res. 2020, 26, 3881–3888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunderson, C.C.; Santin, A.; DelPriore, G.; Elvin, J.; Ramkissoon, S.; Ali, S.; McMahon, C.; Fabrizio, D.; Chalmers, Z.; Frampton, G.; et al. Comprehensive genomic profiling of uterine leiomyosarcomas identifies frequent clinically relevant genomic alterations and opportunities for personalized therapies. Gynecol. Oncol. 2016, 143, 208–209. [Google Scholar] [CrossRef]
- George, S.; Miao, D.; Demetri, G.D.; Adeegbe, D.; Rodig, S.J.; Shukla, S.; Lipschitz, M.; Amin-Mansour, A.; Raut, C.P.; Carter, S.L.; et al. Loss of PTEN is associated with resistance to anti-PD-1 checkpoint blockade therapy in metastatic uterine leiomyosarcoma. Immunity 2017, 46, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Wispelaere, W.; Annibali, D.; Tuyaerts, S.; Lambrechts, D.; Amant, F. Resistance to immune checkpoint blockade in uterine leiomyosarcoma: What can we learn from other cancer types? Cancers 2021, 13, 2040. [Google Scholar] [CrossRef] [PubMed]
- Gallup, D.G.; Blessing, J.A.; Andersen, W.; Morgan, M.A. Evaluation of paclitaxel in previously treated leiomyosarcoma of the uterus: A Gynecologic Oncology Group study. Gynecol. Oncol. 2003, 89, 48–51. [Google Scholar] [CrossRef]
- Look, K.Y.; Sandler, A.; Blessing, J.A.; Lucci, J.A., 3rd; Rose, P.G.; Gynecologic Oncology Group. Phase II trial of gemcitabine as second-line chemotherapy of uterine leiomyosarcoma: A Gynecologic Oncology Group (GOG) Study. Gynecol. Oncol. 2004, 92, 644–647. [Google Scholar] [CrossRef]
- Duska, L.R.; Blessing, J.A.; Rotmensch, J.; Mannel, R.S.; Hanjani, P.; Rose, P.G.; Dizon, D.S. A phase II evaluation of ixabepilone (IND #59699, NSC #710428) in the treatment of recurrent or persistent leiomyosarcoma of the uterus: An NRG Oncology/Gynecologic Oncology Group Study. Gynecol. Oncol. 2014, 135, 44–48. [Google Scholar]
- Gadducci, A.; Grosso, F.; Scambia, G.; Raspagliesi, F.; Colombo, N.; Grignani, G.; Casali, P.; Sanfilippo, R.; Buonadonna, A.; Santoro, A.; et al. A phase II randomised (calibrated design) study on the activity of the single-agent trabectedin in metastatic or locally relapsed uterine leiomyosarcoma. Br. J. Cancer 2018, 119, 565–571. [Google Scholar] [CrossRef] [Green Version]
- McMeekin, D.S.; Sill, M.W.; Darcy, K.M.; Stearns-Kurosawa, D.J.; Webster, K.; Waggoner, S.; Benbrook, D. A phase II trial of thalidomide in patients with refractory leiomyosarcoma of the uterus and correlation with biomarkers of angiogenesis: A Gynecologic Oncology Group study. Gynecol. Oncol. 2007, 106, 596–603. [Google Scholar] [CrossRef]
- Taylor, B.S.; Barretina, J.; Maki, R.G.; Antonescu, C.R.; Singer, S.; Ladanyi, M. Advances in sarcoma genomics and new therapeutic targets. Nat. Rev. Cancer 2011, 11, 541–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Genome Atlas Research Network. Comprehensive and integrated genomic characterization of adult soft tissue sarcomas. Cell 2017, 171, 950–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebbeck, T.R.; Friebel, T.M.; Friedman, E.; Hamann, U.; Huo, D.; Kwong, A.; Olah, E.; Olopade, O.I.; Solano, A.R.; Teo, S.-H.; et al. Mutational spectrum in a worldwide study of 29,700 families with BRCA1 or BRCA2 mutations. Hum. Mutat 2018, 39, 593–620. [Google Scholar] [CrossRef] [Green Version]
- Bhaskaran, S.P.; Huang, T.; Rajendran, B.K.; Guo, M.; Luo, J.; Qin, Z.; Zhao, B.; Chian, J.; Li, S.; Wang, S.M. Ethnic-specific BRCA1/2 variation within Asia population: Evidence from over 78 000 cancer and 40 000 non-cancer cases of Indian, Chinese, Korean and Japanese populations. J. Med. Genet. 2021, 58, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, P.; Bandlamudi, C.; Cheng, M.L.; Srinivasan, P.; Chavan, S.S.; Friedman, N.D.; Rosen, E.Y.; Richards, A.L.; Bouvier, N.; Selcuklu, S.D.; et al. Tumour lineage shapes BRCA-mediated phenotypes. Nature 2019, 571, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, E.; Jonsson, P.; Seier, K.; Qin, L.X.; Chi, P.; Dickson, M.; Gounder, M.; Kelly, C.; Keohan, M.L.; Nacev, B.; et al. Clinical outcome of leiomyosarcomas with somatic alteration in homologous recombination pathway genes. JCO Precis Oncol. 2020, 4, 1350–1360. [Google Scholar] [CrossRef]
- Chudasama, P.; Mughal, S.S.; Sanders, M.A.; Hubschmann, D.; Chung, I.; Deeg, K.I.; Wong, S.H.; Rabe, S.; Hlevnjak, M.; Zapatka, M.; et al. Integrative genomic and transcriptomic analysis of leiomyosarcoma. Nat. Commun. 2018, 9, 144. [Google Scholar] [CrossRef] [Green Version]
- Seligson, N.D.; Kautto, E.A.; Passen, E.N.; Stets, C.; Toland, A.E.; Millis, S.Z.; Meyer, C.F.; Hays, J.L.; Chen, J.L. BRCA1/2 functional loss defines a targetable subset in leiomyosarcoma. Oncologist 2019, 24, 973–979. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Tu, J.; Zhao, Z.; Chen, L.; Qu, Y.; Li, H.; Yao, H.; Wang, X.; Lee, D.F.; Shen, J.; et al. Molecular signatures of BRCAness analysis identifies PARP inhibitor niraparib as a novel targeted therapeutic strategy for soft tissue sarcomas. Theranostics 2020, 10, 9477–9494. [Google Scholar] [CrossRef]
- Rosenbaum, E.; Jonsson, P.; Seier, K.; Chi, P.; Dickson, M.A.; Gounder, M.M.; Kelly, C.M.; Keohan, M.L.; Qin, L.-X.; Hensley, M.L.; et al. DNA damage response pathway alterations and clinical outcome in leiomyosarcoma. J. Clin. Oncol. 2019, 37, 11048. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Ledermann, J.A.; Selle, F.; Gebski, V.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Poveda, A.; Pignata, S.; et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): A double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1274–1284. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef]
- Thomas, A.; Murai, J.; Pommier, Y. The evolving landscape of predictive biomarkers of response to PARP inhibitors. J. Clin. Invest. 2018, 128, 1727–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Martin, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in patients with newly diagnosed advanced ovarian cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Mirza, M.R.; Monk, B.J.; Herrstedt, J.; Oza, A.M.; Mahner, S.; Redondo, A.; Fabbro, M.; Ledermann, J.A.; Lorusso, D.; Vergote, I.; et al. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N. Engl. J. Med. 2016, 375, 2154–2164. [Google Scholar] [CrossRef]
- Moore, K.N.; Secord, A.A.; Geller, M.A.; Miller, D.S.; Cloven, N.; Fleming, G.F.; Wahner Hendrickson, A.E.; Azodi, M.; DiSilvestro, P.; Oza, A.M.; et al. Niraparib monotherapy for late-line treatment of ovarian cancer (QUADRA): A multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2019, 20, 636–648. [Google Scholar] [CrossRef]
- Van Glabbeke, M.; Verweij, J.; Judson, I.; Nielsen, O.S. Progression-free rate as the principal end-point for phase II trials in soft-tissue sarcomas. Eur. J. Cancer 2002, 38, 543–549. [Google Scholar] [CrossRef]


| FIGO 2008 | Primary Tumor | Distribution (%) [6] | 5-year OS (%) [7] |
|---|---|---|---|
| Stage I | Tumors limited to the uterus | 65.7 | 57.1 |
| IA | Tumor size ≤ 5 cm | ||
| IB | Tumor size > 5 cm | ||
| Stage II | Tumor extends beyond the uterus, within the pelvis | 9.8 | 44.6 |
| IIA | Tumor involves the adnexa | ||
| IIB | Tumor involves other pelvic tissues | ||
| Stage III | Tumors infiltrates abdominal tissues | 7.8 | 20.4 |
| IIIA | One site | ||
| IIIB | More than one site | ||
| IIIC | Regional lymph node metastasis | ||
| Stage IV | 16.7 | 23.2 | |
| IVA | Invasion of bladder and/or rectum | ||
| IVB | Distant metastases |
| Line | Regimen | Year | Patients (n) | LMS (n) | uLMS (n) | ORR (%) | mPFS (months) | mOS (months) |
|---|---|---|---|---|---|---|---|---|
| Third | Pazopanib vs. placebo [24] | 2012 | 369 | 165 | NA | 6 vs. 0 | 4.6 vs. 1.6 * | 12.5 vs. 10.7 |
| Second | Ridaforolimus vs. placebo [27] | 2013 | 711 | 231 | NA | (CBR: 40.6 vs. 28.6) | 4.4 vs. 3.65 * | 22.7 vs. 21.3 |
| Second | Ombrabulin + CDDP vs. placebo + CDDP [28] | 2015 | 355 | 95 | NA | 4 vs. 1 | 1.54 vs. 1.41 * | 11.44 vs. 9.33 |
| Second | Trabectedin vs. DTIC [25] | 2016 | 518 | 378 | 212 | 9 vs. 10 | 4.2 vs. 1.5 * | 12.4 vs. 12.9 |
| Third | Eribulin vs. DTIC [26] | 2016 | 452 | 297 | 131 | 4 vs. 5 | 2.6 vs. 2.6 | 13.5 vs. 11.5 * |
| Authors | Year | Patients (n) | Line of Previous Chemotherapy | Response |
|---|---|---|---|---|
| Seligson et al. [52] | 2019 | 4 | Third: 2 (50%) | PR: 1 (25%) |
| Fourth: 1 (25%) | SD: 3 (75%) | |||
| Fifth: 1 (25%) | ||||
| Hensley et al. [32] | 2020 | 6 | NA | CR: 1 (17%) PR: 1 (17%) All had at least some radiographic regression |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asano, H.; Isoe, T.; Ito, Y.M.; Nishimoto, N.; Watanabe, Y.; Yokoshiki, S.; Watari, H. Status of the Current Treatment Options and Potential Future Targets in Uterine Leiomyosarcoma: A Review. Cancers 2022, 14, 1180. https://doi.org/10.3390/cancers14051180
Asano H, Isoe T, Ito YM, Nishimoto N, Watanabe Y, Yokoshiki S, Watari H. Status of the Current Treatment Options and Potential Future Targets in Uterine Leiomyosarcoma: A Review. Cancers. 2022; 14(5):1180. https://doi.org/10.3390/cancers14051180
Chicago/Turabian StyleAsano, Hiroshi, Toshiyuki Isoe, Yoichi M. Ito, Naoki Nishimoto, Yudai Watanabe, Saki Yokoshiki, and Hidemichi Watari. 2022. "Status of the Current Treatment Options and Potential Future Targets in Uterine Leiomyosarcoma: A Review" Cancers 14, no. 5: 1180. https://doi.org/10.3390/cancers14051180