
Risk Stratification Using a Novel Nomogram for 2190 EGFR-Mutant NSCLC Patients Receiving the First or Second Generation EGFR-TKI

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Treatment and Response Evaluation
2.3. Statistical Analysis
2.4. Nomogram Creation and Statistical Software
3. Results
3.1. Patient Characteristics
3.2. Influence of Clinical Variables on PFS
3.3. Establishment of a Prognostic Nomogram Based on Pretreatment Variables
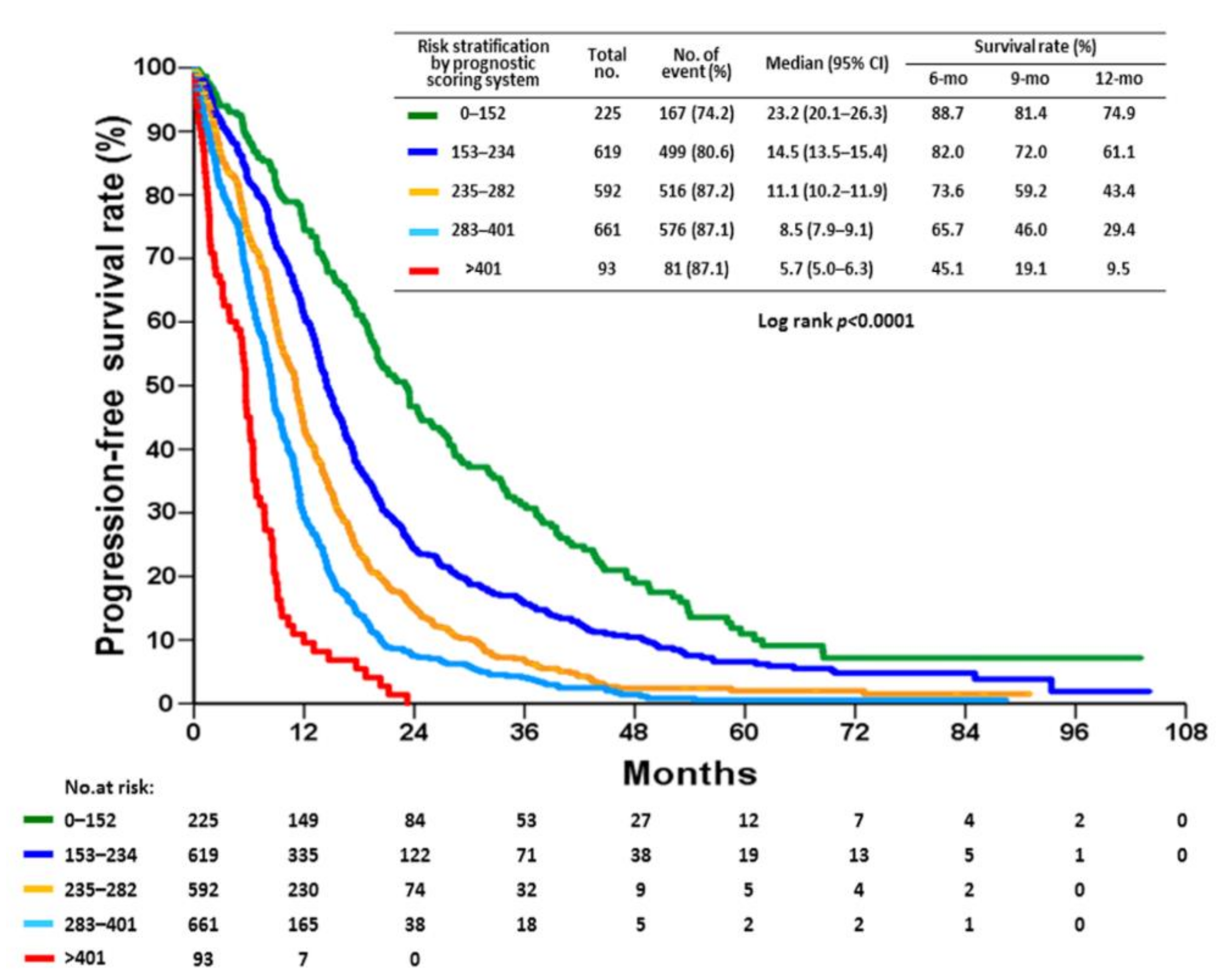
3.4. Risk Stratification by the Nomogram
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T.; et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): An open label, randomised phase 3 trial. Lancet Oncol. 2010, 11, 121–128. [Google Scholar] [CrossRef]
- Sequist, L.V.; Yang, J.C.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.M.; Boyer, M.; et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.L.; Zhou, C.; Hu, C.P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Lee, K.Y.; et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): An open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 213–222. [Google Scholar] [CrossRef]
- Park, K.; Tan, E.H.; O’Byrne, K.; Zhang, L.; Boyer, M.; Mok, T.; Hirsh, V.; Yang, J.C.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): A phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016, 17, 577–589. [Google Scholar] [CrossRef]
- Wu, Y.L.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Tsuji, F.; Linke, R.; Rosell, R.; Corral, J.; et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): A randomised, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 1454–1466. [Google Scholar] [CrossRef]
- Soria, J.C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Santoni-Rugiu, E.; Melchior, L.C.; Urbanska, E.M.; Jakobsen, J.N.; Stricker, K.; Grauslund, M.; Sørensen, J.B. Intrinsic resistance to EGFR-Tyrosine Kinase Inhibitors in EGFR-Mutant Non-Small Cell Lung Cancer: Differences and Similarities with Acquired Resistance. Cancers 2019, 11, 923. [Google Scholar] [CrossRef] [Green Version]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef]
- Stirrups, R. Osimertinib improves progression-free survival in NSCLC. Lancet Oncol. 2018, 19, e10. [Google Scholar] [CrossRef]
- Hosomi, Y.; Morita, S.; Sugawara, S.; Kato, T.; Fukuhara, T.; Gemma, A.; Takahashi, K.; Fujita, Y.; Harada, T.; Minato, K.; et al. Gefitinib Alone Versus Gefitinib Plus Chemotherapy for Non-Small-Cell Lung Cancer With Mutated Epidermal Growth Factor Receptor: NEJ009 Study. J. Clin. Oncol. 2020, 38, 115–123. [Google Scholar] [CrossRef]
- Saito, H.; Fukuhara, T.; Furuya, N.; Watanabe, K.; Sugawara, S.; Iwasawa, S.; Tsunezuka, Y.; Yamaguchi, O.; Okada, M.; Yoshimori, K.; et al. Erlotinib plus bevacizumab versus erlotinib alone in patients with EGFR-positive advanced non-squamous non-small-cell lung cancer (NEJ026): Interim analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Oncol. 2019, 20, 625–635. [Google Scholar] [CrossRef]
- Nakagawa, K.; Garon, E.B.; Seto, T.; Nishio, M.; Ponce Aix, S.; Paz-Ares, L.; Chiu, C.H.; Park, K.; Novello, S.; Nadal, E.; et al. Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 1655–1669. [Google Scholar] [CrossRef] [Green Version]
- Canale, M.; Petracci, E.; Delmonte, A.; Bronte, G.; Chiadini, E.; Ludovini, V.; Dubini, A.; Papi, M.; Baglivo, S.; De Luigi, N.; et al. Concomitant TP53 Mutation Confers Worse Prognosis in EGFR-Mutated Non-Small Cell Lung Cancer Patients Treated with TKIs. J. Clin. Med. 2020, 9, 1047. [Google Scholar] [CrossRef] [Green Version]
- Takeda, M.; Okamoto, I.; Fujita, Y.; Arao, T.; Ito, H.; Fukuoka, M.; Nishio, K.; Nakagawa, K. De novo resistance to epidermal growth factor receptor-tyrosine kinase inhibitors in EGFR mutation-positive patients with non-small cell lung cancer. J. Thorac. Oncol. 2010, 5, 399–400. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.S.; Lin, M.H.; Lee, C.P.; Yang, Y.H.; Chen, W.C.; Chang, G.H.; Tsai, Y.T.; Chen, P.C.; Tsai, Y.H. Chang Gung Research Database: A multi-institutional database consisting of original medical records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef]
- Wu, C.E.; Chang, C.F.; Huang, C.Y.; Yang, C.T.; Kuo, C.S.; Hsu, P.C.; Chang, J.W. Feasibility and effectiveness of afatinib for poor performance status patients with EGFR-mutation-positive non-small-cell lung cancer: A retrospective cohort study. BMC Cancer 2021, 21, 859. [Google Scholar] [CrossRef]
- Hothorn, T.; Hornik, K.; Zeileis, A. Unbiased recursive partitioning: A conditional inference framework. J. Comput. Graph. Stat. 2006, 15, 651–674. [Google Scholar] [CrossRef] [Green Version]
- Haratake, N.; Misumi, T.; Yamanaka, T.; Seto, T. Optimizing Sequential Treatment With EGFR Tyrosine Kinase Inhibitor With a Simulation of the T790M Mutation Rate in EGFR–Mutated Lung Cancer. JTO Clin. Res. Rep. 2020, 1, 100085. [Google Scholar] [CrossRef]
- Liang, H.; Pan, Z.; Wang, W.; Guo, C.; Chen, D.; Zhang, J.; Zhang, Y.; Tang, S.; He, J.; Liang, W.; et al. The alteration of T790M between 19 del and L858R in NSCLC in the course of EGFR-TKIs therapy: A literature-based pooled analysis. J. Thorac. Dis. 2018, 10, 2311–2320. [Google Scholar] [CrossRef] [Green Version]
- Chai, C.S.; Liam, C.K.; Poh, M.E.; Ong, D.B.; Pang, Y.K.; Cheah, P.L.; Ho, G.F.; Alip, A. Predictors of Acquired T790M Mutation in Patients Failing First- or Second-Generation Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitors. Cancer Manag. Res. 2020, 12, 5439–5450. [Google Scholar] [CrossRef]
- Wu, S.G.; Chiang, C.L.; Liu, C.Y.; Wang, C.C.; Su, P.L.; Hsia, T.C.; Shih, J.Y.; Chang, G.C. An Observational Study of Acquired EGFR T790M-Dependent Resistance to EGFR-TKI Treatment in Lung Adenocarcinoma Patients in Taiwan. Front. Oncol. 2020, 10, 1481. [Google Scholar] [CrossRef]
- Kawamura, T.; Kenmotsu, H.; Omori, S.; Nakashima, K.; Wakuda, K.; Ono, A.; Naito, T.; Murakami, H.; Omae, K.; Mori, K.; et al. Clinical Factors Predicting Detection of T790M Mutation in Rebiopsy for EGFR-Mutant Non-small-cell Lung Cancer. Clin. Lung Cancer 2018, 19, e247–e252. [Google Scholar] [CrossRef]
- Lin, Y.T.; Chen, J.S.; Liao, W.Y.; Ho, C.C.; Hsu, C.L.; Yang, C.Y.; Chen, K.Y.; Lee, J.H.; Lin, Z.Z.; Shih, J.Y.; et al. Clinical outcomes and secondary epidermal growth factor receptor (EGFR) T790M mutation among first-line gefitinib, erlotinib and afatinib-treated non-small cell lung cancer patients with activating EGFR mutations. Int. J. Cancer 2019, 144, 2887–2896. [Google Scholar] [CrossRef]
- Huang, Y.H.; Hsu, K.H.; Tseng, J.S.; Chen, K.C.; Hsu, C.H.; Su, K.Y.; Chen, J.; Chen, H.W.; Yu, S.L.; Yang, T.Y.; et al. The Association of Acquired T790M Mutation with Clinical Characteristics after Resistance to First-Line Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor in Lung Adenocarcinoma. Cancer Res. Treat. 2018, 50, 1294–1303. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.P.; Chen, Y.M.; Lai, C.H.; Lin, C.Y.; Fang, W.F.; Huang, C.H.; Li, S.H.; Chen, H.C.; Wang, C.C.; Lin, M.C. The impact of de novo liver metastasis on clinical outcome in patients with advanced non-small-cell lung cancer. PLoS ONE 2017, 12, e0178676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castanon, E.; Rolfo, C.; Vinal, D.; Lopez, I.; Fusco, J.P.; Santisteban, M.; Martin, P.; Zubiri, L.; Echeveste, J.I.; Gil-Bazo, I. Impact of epidermal growth factor receptor (EGFR) activating mutations and their targeted treatment in the prognosis of stage IV non-small cell lung cancer (NSCLC) patients harboring liver metastasis. J. Transl. Med. 2015, 13, 257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbate, M.I.; Cortinovis, D.L.; Tiseo, M.; Vavalà, T.; Cerea, G.; Toschi, L.; Canova, S.; Colonese, F.; Bidoli, P. Peritoneal carcinomatosis in non-small-cell lung cancer: Retrospective multicentric analysis and literature review. Future Oncol. 2019, 15, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Su, H.T.; Tsai, C.M.; Perng, R.P. Peritoneal carcinomatosis in lung cancer. Respirology 2008, 13, 465–467. [Google Scholar] [CrossRef]
- Zito Marino, F.; Bianco, R.; Accardo, M.; Ronchi, A.; Cozzolino, I.; Morgillo, F.; Rossi, G.; Franco, R. Molecular heterogeneity in lung cancer: From mechanisms of origin to clinical implications. Int. J. Med. Sci. 2019, 16, 981–989. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.Y.; Zhong, W.Z.; Zhang, X.C.; Su, J.; Yang, X.N.; Chen, Z.H.; Yang, J.J.; Zhou, Q.; Yan, H.H.; An, S.J.; et al. EGFR mutation heterogeneity and the mixed response to EGFR tyrosine kinase inhibitors of lung adenocarcinomas. Oncologist 2012, 17, 978–985. [Google Scholar] [CrossRef] [Green Version]
- Jin, R.; Peng, L.; Shou, J.; Wang, J.; Jin, Y.; Liang, F.; Zhao, J.; Wu, M.; Li, Q.; Zhang, B.; et al. EGFR-Mutated Squamous Cell Lung Cancer and Its Association With Outcomes. Front. Oncol. 2021, 11, 680804. [Google Scholar] [CrossRef]
- Tu, C.Y.; Chen, C.M.; Liao, W.C.; Wu, B.R.; Chen, C.Y.; Chen, W.C.; Hsia, T.C.; Cheng, W.C.; Chen, C.H. Comparison of the effects of the three major tyrosine kinase inhibitors as first-line therapy for non-small-cell lung cancer harboring epidermal growth factor receptor mutations. Oncotarget 2018, 9, 24237–24247. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Murotani, K.; Kubo, A.; Kunii, E.; Taniguchi, H.; Shindo, J.; Asada, K.; Imaizumi, K.; Tanaka, K.; Inui, N.; et al. Comparative analysis of overall survival using propensity score between first- and second-generation EGFR-TKI: Real world data of 1354 patients with EGFR mutant NSCLC. Ann. Oncol. 2018, 29, viii526–viii527. [Google Scholar] [CrossRef]
- Su, P.L.; Wu, Y.L.; Chang, W.Y.; Ho, C.L.; Tseng, Y.L.; Lai, W.W.; Su, W.C.; Lin, C.C.; Yang, S.C. Preventing and treating brain metastases with three first-line EGFR-tyrosine kinase inhibitors in patients with EGFR mutation-positive advanced non-small cell lung cancer. Ther. Adv. Med. Oncol. 2018, 10, 1758835918797589. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, S.H.; Ahn, J.S.; Ahn, M.J.; Park, K.; Sun, J.M. Efficacy and Safety of Afatinib for EGFR-mutant Non-small Cell Lung Cancer, Compared with Gefitinib or Erlotinib. Cancer Res. Treat. 2019, 51, 502–509. [Google Scholar] [CrossRef]
- Keam, B.; Kim, D.W.; Park, J.H.; Lee, J.O.; Kim, T.M.; Lee, S.H.; Chung, D.H.; Heo, D.S. Nomogram Predicting Clinical Outcomes in Non-small Cell Lung Cancer Patients Treated with Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors. Cancer Res. Treat. 2014, 46, 323–330. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, B.; Pang, Q.; Zhang, T.; Chen, X.; Er, P.; Wang, Y.; You, J.; Wang, P. A nomogram for predicting brain metastases of EGFR-mutated lung adenocarcinoma patients and estimating the efficacy of therapeutic strategies. J. Thorac. Dis. 2021, 13, 883–892. [Google Scholar] [CrossRef]
- Yang, B.; Ji, H.; Zhong, J.; Ma, L.; Zhong, J.; Dong, H.; Zhou, C.; Duan, S.; Zhu, C.; Tian, J.; et al. Value of 18F-FDG PET/CT-Based Radiomics Nomogram to Predict Survival Outcomes and Guide Personalized Targeted Therapy in Lung Adenocarcinoma With EGFR Mutations. Front. Oncol. 2020, 10, 567160. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Shen, G.; Mao, J.; Gao, B. CT Radiomics in Predicting EGFR Mutation in Non-small Cell Lung Cancer: A single Institutional Study. Front. Oncol. 2020, 10, 542957. [Google Scholar] [CrossRef] [PubMed]
- Sakata, Y.; Sakata, S.; Oya, Y.; Tamiya, M.; Suzuki, H.; Shibaki, R.; Okada, A.; Kobe, H.; Matsumoto, H.; Yokoi, T. Osimertinib as first-line treatment for advanced epidermal growth factor receptor mutation–positive non–small-cell lung cancer in a real-world setting (OSI-FACT). Eur. J. Cancer 2021, 159, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.C.; Lim, C.K.; Chang, L.Y.; Chen, K.Y.; Shih, J.Y.; Yu, C.J. (Non-small cell lung cancer harbouring non-resistant uncommon EGFR mutations: Mutation patterns, effectiveness of epidermal growth factor receptor-tyrosine kinase inhibitors and prognostic factors. Eur. J. Cancer 2019, 119, 77–86. [Google Scholar] [CrossRef]
- Yang, J.C.; Schuler, M.; Popat, S.; Miura, S.; Heeke, S.; Park, K.; Märten, A.; Kim, E.S. Afatinib for the Treatment of NSCLC Harboring Uncommon EGFR Mutations: A Database of 693 Cases. J. Thorac. Oncol. 2020, 15, 803–815. [Google Scholar] [CrossRef] [Green Version]
- Gristina, V.; Malapelle, U.; Galvano, A.; Pisapia, P.; Pepe, F.; Rolfo, C.; Tortorici, S.; Bazan, V.; Troncone, G.; Russo, A. The significance of epidermal growth factor receptor uncommon mutations in non-small cell lung cancer: A systematic review and critical appraisal. Cancer Treat. Rev. 2020, 85, 101994. [Google Scholar] [CrossRef]
- Ito, K.; Morise, M.; Wakuda, K.; Hataji, O.; Shimokawaji, T.; Takahashi, K.; Furuya, N.; Takeyama, Y.; Goto, Y.; Abe, T.; et al. A multicenter cohort study of osimertinib compared with afatinib as first-line treatment for EGFR-mutated non-small-cell lung cancer from practical dataset: CJLSG1903. ESMO Open 2021, 6, 100115. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 2190) | Response | p-Value | ||
|---|---|---|---|---|---|
| CR/PR (n = 1461) | SD (n = 324) | PD/NA (n = 405) | |||
| Basic data | |||||
| Age (years), mean ± SD | 67.0 ± 12.1 | 66.1 ± 12.0 | 67.5 ± 12.2 | 69.8 ± 12.0 | <0.0001 |
| ≤65 | 989 (45.2) | 695 (70.3) | 144 (14.6) | 150 (15.1) | 0.001 |
| >65 | 1201 (54.8) | 766 (63.8) | 180 (15.0) | 255 (21.2) | |
| Sex | |||||
| Male | 1321 (60.3) | 896 (67.8) | 186 (14.1) | 239 (18.1) | 0.357 |
| Female | 869 (39.7) | 565 (65.0) | 138 (15.9) | 166 (19.1) | |
| Performance score | |||||
| 0 | 360 (16.4) | 262 (72.8) | 53 (14.7) | 45 (12.5) | <0.0001 |
| 1 | 1350 (61.6) | 914 (67.7) | 221 (16.4) | 215 (15.9) | |
| 2 | 289 (13.2) | 181 (62.6) | 28 (9.7) | 80 (27.7) | |
| 3 | 130 (5.9) | 70 (53.8) | 17 (13.1) | 43 (33.1) | |
| 4 | 61 (2.8) | 34 (55.7) | 5 (8.2) | 22 (36.1) | |
| Smoking | |||||
| Yes | 508 (23.2) | 328 (64.6) | 79 (15.5) | 101 (19.9) | 0.831 |
| No | 1625 (74.2) | 1095 (67.4) | 236 (14.5) | 294 (18.1) | |
| Unknown | 57 (2.6) | 38 (66.7) | 9 (15.8) | 10 (17.5) | |
| Tumor characteristics | |||||
| Morphology | |||||
| Adenocarcinoma | 2151 (98.2) | 1443 (67.1) | 318 (14.8) | 390 (18.1) | 0.004 |
| Non-adenocarcinoma | 39 (1.8) | 18 (46.2) | 6 (15.3) | 15 (38.5) | |
| Mutation | |||||
| Exon 19 deletion | 1034 (47.2) | 724 (70.1) | 138 (13.3) | 172 (16.6) | 0.008 |
| L858R | 1156 (52.8) | 737 (63.8) | 186 (16.0) | 233 (20.2) | |
| Stage | |||||
| IIIB | 149 (6.8) | 109 (73.2) | 17 (11.4) | 23 (15.4) | 0.219 |
| IV | 2041 (93.2) | 1352 (66.3) | 307 (15.0) | 382 (18.7) | |
| TKI therapy | |||||
| Drug | |||||
| Afatinib | 635 (29.0) | 454 (71.5) | 89 (14.0) | 92 (14.5) | 0.005 |
| Erlotinib | 496 (22.6) | 313 (63.1) | 70 (14.1) | 113 (22.8) | |
| Gefitinib | 1059 (48.4) | 694 (65.5) | 165 (15.6) | 200 (18.9) | |
| Metastatic site | |||||
| Lung | |||||
| Yes | 857 (39.1) | 605 (70.6) | 113 (13.2) | 139 (16.2) | 0.008 |
| No | 1333 (60.9) | 856 (64.2) | 211 (15.8) | 266 (20.0) | |
| Liver | |||||
| Yes | 290 (13.2) | 187 (64.5) | 31 (10.7) | 72 (24.8) | 0.004 |
| No | 1900 (86.8) | 1274 (67.1) | 293 (15.4) | 333 (17.5) | |
| Brain | |||||
| Yes | 650 (29.7) | 433 (66.7) | 77 (11.8) | 140 (21.5) | 0.007 |
| No | 1540 (70.3) | 1028 (66.8) | 247 (16.0) | 265 (17.2) | |
| Bone | |||||
| Yes | 1012 (46.2) | 651 (64.3) | 150 (14.8) | 211 (20.8) | 0.027 |
| No | 1178 (53.8) | 810 (68.8) | 174 (14.7) | 194 (16.5) | |
| Pleura | |||||
| Yes | 986 (45.0) | 639 (64.8) | 153 (15.5) | 194 (19.7) | 0.227 |
| No | 1204 (55.0) | 822 (68.3) | 171 (14.2) | 211 (17.5) | |
| Adrenal | |||||
| Yes | 189 (8.6) | 117 (61.9) | 25 (13.2) | 47 (24.9) | 0.061 |
| No | 2001 (91.4) | 1344 (67.2) | 299 (14.9) | 358 (17.9) | |
| Distant lymph node | |||||
| Yes | 223 (10.2) | 144 (64.6) | 25 (11.2) | 54 (24.2) | 0.035 |
| No | 1967 (89.8) | 1317 (67.0) | 299 (15.2) | 351 (17.8) | |
| Pericardium | |||||
| Yes | 45 (2.1) | 27 (60.0) | 6 (13.3) | 12 (26.7) | 0.361 |
| No | 2145 (97.9) | 1434 (66.9) | 318 (14.8) | 393 (18.3) | |
| Peritoneum | |||||
| Yes | 6 (0.3) | 4 (66.7) | 0 | 2 (33.3) | 0.448 |
| No | 2184 (99.7) | 1457 (66.7) | 321 (14.8) | 403 (18.5) | |
| Parameters | Total n | n of Events (%) | Median (Months) | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Age (years) | ||||||||
| ≤65 | 989 | 873 (88.3) | 11.4 | 10.8–11.9 | 0.289 | - | ||
| >65 | 1201 | 966 (80.4) | 11.4 | 10.6–12.2 | ||||
| Sex | ||||||||
| Male | 869 | 749 (86.2) | 11.1 | 10.3–11.8 | 0.198 | - | ||
| Female | 1321 | 1090 (82.5) | 11.5 | 10.9–12.2 | ||||
| Performance score | - | |||||||
| 0 | 360 | 284 (78.9) | 14.4 | 12.8–16.0 | <0.0001 | 1 | - | - |
| 1/2 | 1639 | 1408 (85.9) | 11.3 | 10.8–11.8 | 1.271 | 1.117–1.446 | <0.001 | |
| 3/4 | 191 | 147 (77.0) | 6.4 | 5.3–7.6 | 1.627 | 1.326–1.997 | <0.0001 | |
| Smoking | ||||||||
| Yes | 508 | 437 (86.0) | 11.0 | 10.0–12.1 | 0.275 | - | ||
| No | 1625 | 1351 (83.1) | 11.5 | 10.9–12.1 | ||||
| Unknown | 57 | 51 (89.5) | 10.3 | 7.7–12.9 | ||||
| Morphology | ||||||||
| Adenocarcinoma | 2151 | 1807 (84.0) | 11.5 | 11.0–12.0 | 0.001 | 1 | - | - |
| Non-adenocarcinoma | 39 | 32 (82.1) | 5.3 | 4.4–6.2 | 1.614 | 1.132–2.301 | 0.010 | |
| Mutation | ||||||||
| Exon 19 deletion | 1034 | 884 (85.5) | 11.9 | 11.2–12.6 | 0.055 | 1 | - | - |
| L858R | 1156 | 955 (82.6) | 10.9 | 10.2–11.5 | 1.099 | 1.002–1.206 | 0.045 | |
| Stage | ||||||||
| IIIB | 149 | 112 (75.2) | 21.8 | 18.0–25.6 | <0.0001 | 1 | - | - |
| IV | 2041 | 1727 (84.6) | 11.1 | 10.6–11.6 | 1.454 | 1.179–1.793 | <0.001 | |
| TKI drug | ||||||||
| Afatinib | 635 | 503 (79.2) | 14.5 | 13.5–15.4 | <0.0001 | 1 | - | - |
| Erlotinib | 496 | 416 (83.9) | 10.6 | 9.8–11.5 | 1.274 | 1.117–1.454 | <0.001 | |
| Gefitinib | 1059 | 920 (86.9) | 10.2 | 9.4–10.9 | 1.461 | 1.307–1.633 | <0.0001 | |
| Lung metastasis | ||||||||
| Yes | 857 | 725 (84.6) | 11.1 | 10.4–11.9 | 0.032 | 1.029 | 0.935–1.132 | 0.561 |
| No | 1333 | 1114 (83.6) | 11.5 | 10.8–12.2 | 1 | - | - | |
| Liver metastasis | ||||||||
| Yes | 290 | 255 (87.9) | 8.5 | 7.8–9.3 | <0.0001 | 1.467 | 1.276–1.687 | <0.0001 |
| No | 1900 | 1584 (83.4) | 11.8 | 11.2–12.3 | 1 | - | - | |
| Brain metastasis | ||||||||
| Yes | 650 | 546 (84.0) | 9.4 | 8.6–10.3 | <0.0001 | 1.222 | 1.099–1.360 | <0.001 |
| No | 1540 | 1293 (84.0) | 11.9 | 11.3–12.5 | 1 | - | - | |
| Bone metastasis | ||||||||
| Yes | 1012 | 871 (82.2) | 9.9 | 9.2–10.6 | <0.0001 | 1.328 | 1.204–1.465 | <0.0001 |
| No | 1178 | 968 (86.1) | 12.9 | 12.1–13.7 | 1 | - | - | |
| Pleural metastasis | ||||||||
| Yes | 986 | 848 (86.0) | 10.8 | 10.1–11.5 | <0.0001 | 1.360 | 1.232–1.500 | <0.0001 |
| No | 1204 | 991 (82.3) | 12.4 | 11.5–13.2 | 1 | - | - | |
| Adrenal metastasis | ||||||||
| Yes | 189 | 26 (86.2) | 8.2 | 7.0–9.4 | <0.0001 | 1.283 | 1.085–1.516 | 0.004 |
| No | 2001 | 1676 (83.8) | 11.6 | 11.1–12.1 | 1 | - | - | |
| Distant LN metastasis | ||||||||
| Yes | 223 | 187 (83.9) | 8.7 | 6.9–10.5 | 0.017 | 1.175 | 1.008–1.371 | 0.040 |
| No | 1967 | 1652 (84.0) | 11.5 | 11.0–12.0 | 1 | - | - | |
| Pericardial metastasis | ||||||||
| Yes | 45 | 39 (86.7) | 7.6 | 4.3–10.8 | 0.001 | 1.221 | 0.882–1.690 | 0.229 |
| No | 2145 | 1800 (83.9) | 11.5 | 11.0–12.0 | 1 | - | - | |
| Peritoneal metastasis | ||||||||
| Yes | 6 | 6 (100.0) | 3.9 | 0.1–13.2 | 0.122 | - | ||
| No | 2184 | 1833 (83.9) | 11.4 | 10.9–11.9 | ||||
| Tumor Response | ||||||||
| CR/PR | 1461 | 1252 (85.7) | 13.4 | 12.8–14.1 | <0.0001 | - | ||
| SD | 324 | 271 (83.6) | 11.6 | 10.0–13.2 | ||||
| PD/NA | 405 | 316 (88.0) | 1.9 | 1.7–2.1 | ||||
| Prognostic Variables | Hazard Ratio | 95% CI | p-Value | Points Assigned in Nomogram | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Performance score | |||||
| 0 | 1 | - | - | - | 0 |
| 1/2 | 1.274 | 1.120 | 1.449 | <0.001 | 48 |
| 3/4 | 1.655 | 1.351 | 2.027 | <0.001 | 100 |
| Morphology | |||||
| Adenocarcinoma | 1 | - | - | - | 0 |
| Non-adenocarcinoma | 1.610 | 1.129 | 2.294 | 0.008 | 94 |
| Mutation | |||||
| Exon 19 deletion | 1 | - | - | - | 0 |
| L858R | 1.100 | 1.003 | 1.206 | 0.044 | 19 |
| Stage | |||||
| IIIB | 1 | - | - | - | 0 |
| IV | 1.468 | 1.195 | 1.805 | <0.001 | 76 |
| TKI drug | |||||
| Afatinib | 1 | 0 | |||
| Erlotinib | 1.276 | 1.118 | 1.455 | <0.001 | 48 |
| Gefitinib | 1.464 | 1.310 | 1.636 | <0.0001 | 76 |
| Liver metastasis | |||||
| Yes | 1.474 | 1.282 | 1.694 | <0.0001 | 77 |
| No | 1 | - | - | - | 0 |
| Brain metastasis | |||||
| Yes | 1.223 | 1.099 | 1.360 | <0.001 | 40 |
| No | 1 | - | - | - | 0 |
| Bone metastasis | |||||
| Yes | 1.328 | 1.204 | 1.464 | <0.0001 | 56 |
| No | 1 | - | - | - | 0 |
| Pleural metastasis | |||||
| Yes | 1.366 | 1.239 | 1.506 | <0.0001 | 62 |
| No | 1 | - | - | - | 0 |
| Adrenal metastasis | |||||
| Yes | 1.281 | 1.084 | 1.513 | 0.004 | 49 |
| No | 1 | - | - | - | 0 |
| Distant LN metastasis | |||||
| Yes | 1.182 | 1.014 | 1.378 | 0.033 | 33 |
| No | 1 | - | - | - | 0 |
| Nomogram Points | Probability of 6-Month PFS |
| 602 | 0.20 |
| 544 | 0.30 |
| 490 | 0.40 |
| 434 | 0.50 |
| 374 | 0.60 |
| 303 | 0.70 |
| 209 | 0.80 |
| 60 | 0.90 |
| Nomogram Points | Probability of 9-Month PFS |
| 612 | 0.05 |
| 559 | 0.10 |
| 488 | 0.20 |
| 431 | 0.30 |
| 376 | 0.40 |
| 321 | 0.50 |
| 260 | 0.60 |
| 189 | 0.70 |
| 96 | 0.80 |
| Nomogram Points | Probability of 12-Month PFS |
| 613 | 0.01 |
| 527 | 0.05 |
| 475 | 0.10 |
| 404 | 0.20 |
| 348 | 0.30 |
| 292 | 0.40 |
| 237 | 0.50 |
| 176 | 0.60 |
| 105 | 0.70 |
| 12 | 0.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, J.W.-C.; Huang, C.-Y.; Fang, Y.-F.; Chang, C.-F.; Yang, C.-T.; Kuo, C.-H.S.; Hsu, P.-C.; Wu, C.-E. Risk Stratification Using a Novel Nomogram for 2190 EGFR-Mutant NSCLC Patients Receiving the First or Second Generation EGFR-TKI. Cancers 2022, 14, 977. https://doi.org/10.3390/cancers14040977
Chang JW-C, Huang C-Y, Fang Y-F, Chang C-F, Yang C-T, Kuo C-HS, Hsu P-C, Wu C-E. Risk Stratification Using a Novel Nomogram for 2190 EGFR-Mutant NSCLC Patients Receiving the First or Second Generation EGFR-TKI. Cancers. 2022; 14(4):977. https://doi.org/10.3390/cancers14040977
Chicago/Turabian StyleChang, John Wen-Cheng, Chen-Yang Huang, Yueh-Fu Fang, Ching-Fu Chang, Cheng-Ta Yang, Chih-Hsi Scott Kuo, Ping-Chih Hsu, and Chiao-En Wu. 2022. "Risk Stratification Using a Novel Nomogram for 2190 EGFR-Mutant NSCLC Patients Receiving the First or Second Generation EGFR-TKI" Cancers 14, no. 4: 977. https://doi.org/10.3390/cancers14040977