
Tumor-Infiltrating Lymphocytes as Biomarkers of Treatment Response and Long-Term Survival in Patients with Rectal Cancer: A Systematic Review and Meta-Analysis

 , , , and
, , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Data Management and Extraction
2.4. Outcomes and Subgroups
2.5. Data Extraction
2.6. Statistical Analysis
2.7. Risk of Bias of Individual Studies
2.8. Level of Evidence
3. Results
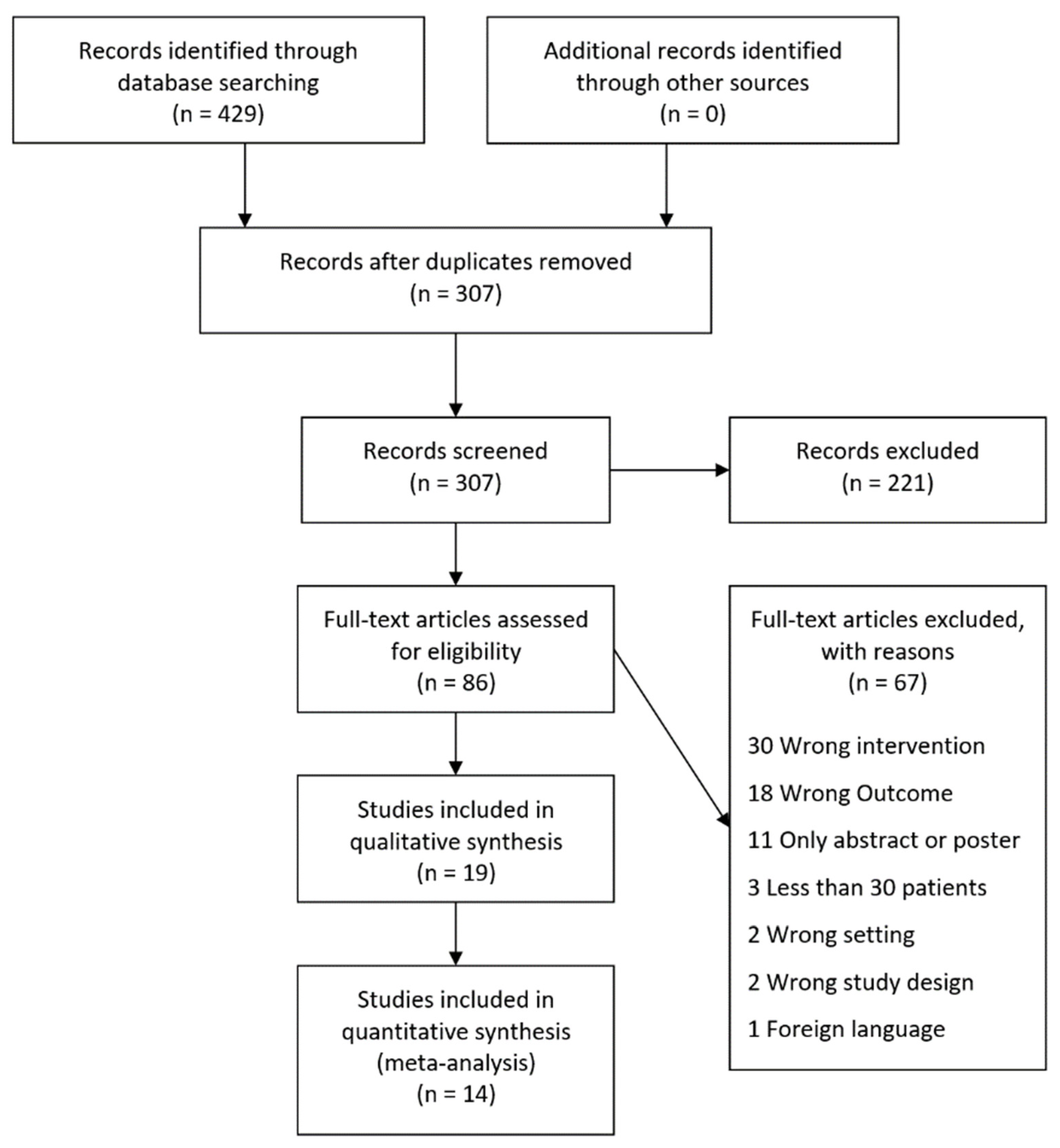
3.1. Search Results
3.2. Study Characteristics
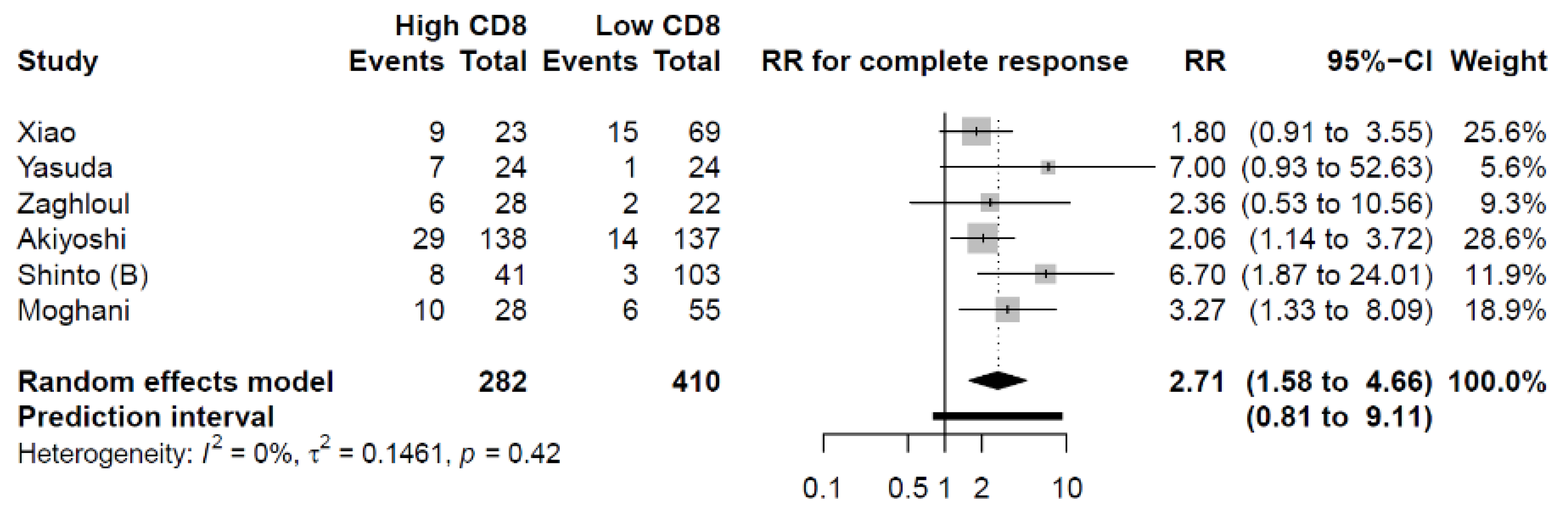
3.3. Pathological Complete Response (pCR)
3.4. Pathological Treatment Response (pTR)
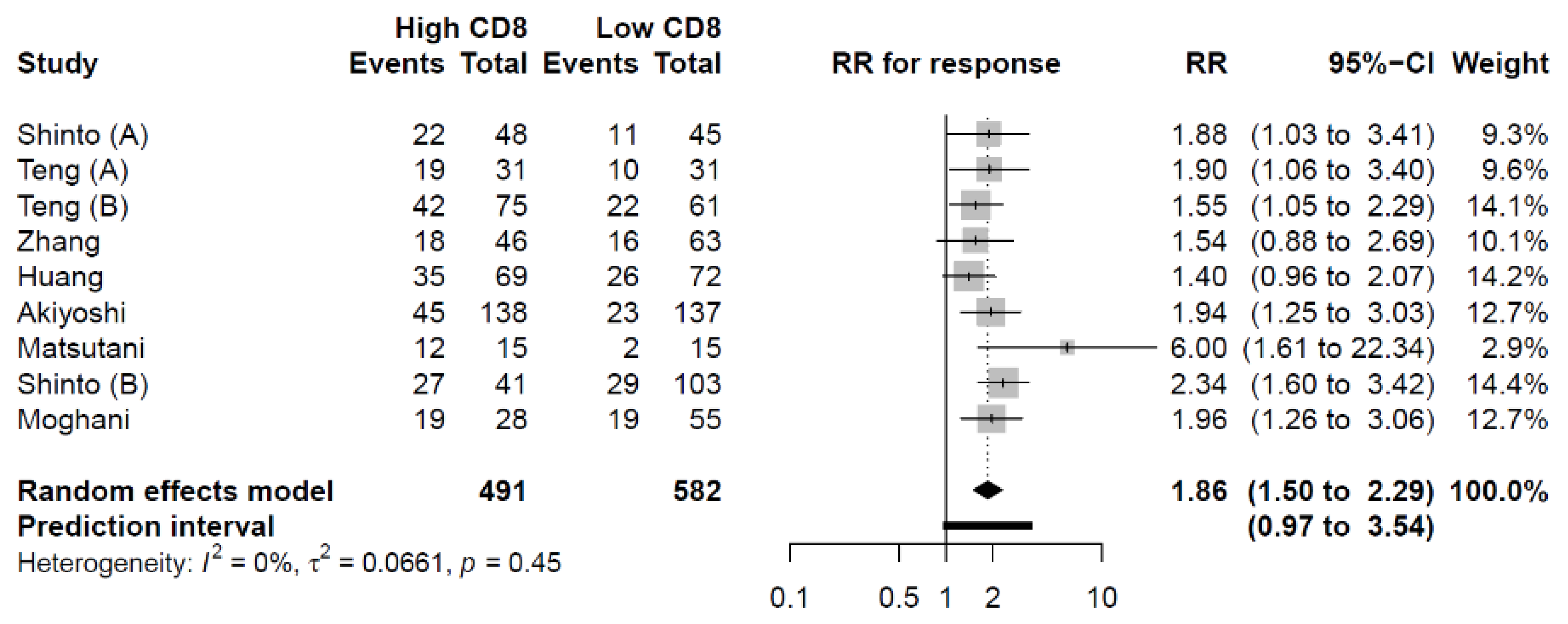
3.4.1. CD8+ TILs
3.4.2. CD3+ TILs
3.4.3. CD4+ TILs
3.4.4. FOXP3+ TILs
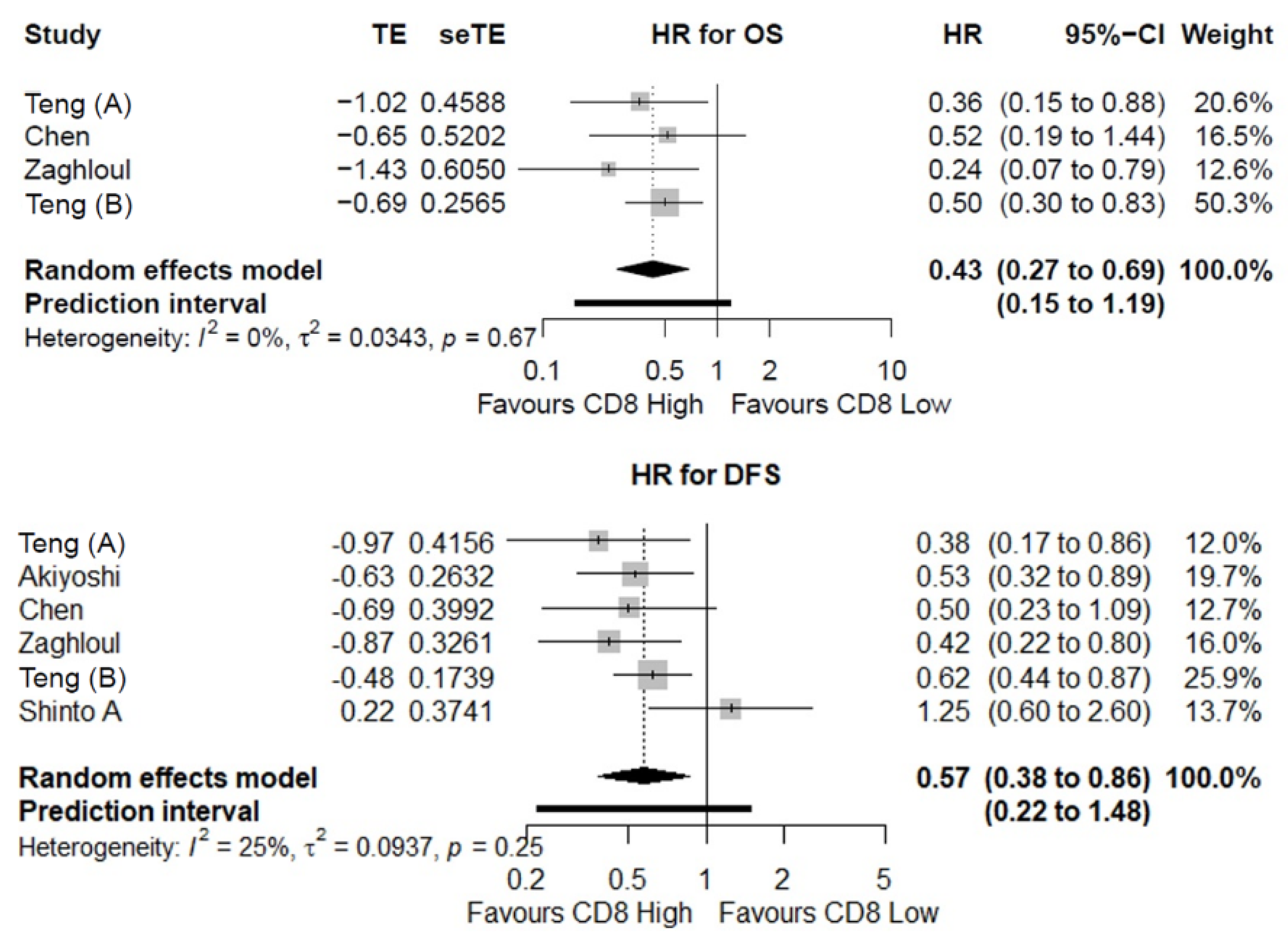
3.5. Overall Survival (OS)
3.6. Disease-Free Survival (DFS)
3.6.1. CD8+ TILs
3.6.2. FOXP3+ TILs
3.7. Risk of Bias of Individual Studies
3.8. Level of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef] [PubMed]
- Fokas, E.; Liersch, T.; Fietkau, R.; Hohenberger, W.; Beissbarth, T.; Hess, C.; Becker, H.; Ghadimi, M.; Mrak, K.; Merkel, S.; et al. Tumor Regression Grading After Preoperative Chemoradiotherapy for Locally Advanced Rectal Carcinoma Revisited: Updated Results of the CAO/ARO/AIO-94 Trial. J. Clin. Oncol. 2014, 32, 1554–1562. [Google Scholar] [CrossRef] [PubMed]
- Valk, M.J.M.; van der Hilling, D.E.; Bastiaannet, E.; Kranenbarg, E.M.-K.; Beets, G.L.; Figueiredo, N.L.; Habr-Gama, A.; Perez, R.O.; Renehan, A.G.; van de Velde, C.J.H.; et al. Long-Term Outcomes of Clinical Complete Responders after Neoadjuvant Treatment for Rectal Cancer in the International Watch & Wait Database (IWWD): An International Multicentre Registry Study. Lancet 2018, 391, 2537–2545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moureau-Zabotto, L.; Farnault, B.; de Chaisemartin, C.; Esterni, B.; Lelong, B.; Viret, F.; Giovannini, M.; Monges, G.; Delpero, J.-R.; Bories, E.; et al. Predictive Factors of Tumor Response After Neoadjuvant Chemoradiation for Locally Advanced Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 483–491. [Google Scholar] [CrossRef]
- Anitei, M.-G.; Zeitoun, G.; Mlecnik, B.; Marliot, F.; Haicheur, N.; Todosi, A.-M.; Kirilovsky, A.; Lagorce, C.; Bindea, G.; Ferariu, D.; et al. Prognostic and Predictive Values of the Immunoscore in Patients with Rectal Cancer. Clin. Cancer Res. 2014, 20, 1891–1899. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, K.; Nirei, T.; Sunami, E.; Nagawa, H.; Kitayama, J. Density of CD4(+) and CD8(+) T Lymphocytes in Biopsy Samples Can Be a Predictor of Pathological Response to Chemoradiotherapy (CRT) for Rectal Cancer. Radiat. Oncol. 2011, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Idos, G.E.; Kwok, J.; Bonthala, N.; Kysh, L.; Gruber, S.B.; Qu, C. The Prognostic Implications of Tumor Infiltrating Lymphocytes in Colorectal Cancer: A Systematic Review and Meta-Analysis. Sci. Rep. 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Gooden, M.J.M.; de Bock, G.H.; Leffers, N.; Daemen, T.; Nijman, H.W. The Prognostic Influence of Tumour-Infiltrating Lymphocytes in Cancer: A Systematic Review with Meta-Analysis. Br. J. Cancer 2011, 105, 93–103. [Google Scholar] [CrossRef] [Green Version]
- Teng, F.; Meng, X.; Kong, L.; Mu, D.; Zhu, H.; Liu, S.; Zhang, J.; Yu, J. Tumor-Infiltrating Lymphocytes, Forkhead Box P3, Programmed Death Ligand-1, and Cytotoxic T Lymphocyte–Associated Antigen-4 Expressions before and after Neoadjuvant Chemoradiation in Rectal Cancer. Transl. Res. 2015, 166, 721–732.e1. [Google Scholar] [CrossRef]
- Teng, F.; Mu, D.; Meng, X.; Kong, L.; Zhu, H.; Liu, S.; Zhang, J.; Yu, J. Tumor Infiltrating Lymphocytes (TILs) before and after Neoadjuvant Chemoradiotherapy and Its Clinical Utility for Rectal Cancer. Am. J. Cancer Res. 2015, 5, 2064. [Google Scholar]
- McCoy, M.J.; Hemmings, C.; Anyaegbu, C.C.; Austin, S.J.; Lee-Pullen, T.F.; Miller, T.J.; Bulsara, M.K.; Zeps, N.; Nowak, A.K.; Lake, R.A.; et al. Tumour-Infiltrating Regulatory T Cell Density before Neoadjuvant Chemoradiotherapy for Rectal Cancer Does Not Predict Treatment Response. Oncotarget 2017, 8, 19803–19813. [Google Scholar] [CrossRef] [Green Version]
- Ding, W.; Xu, X.; Qian, Y.; Xue, W.; Wang, Y.; Du, J.; Jin, L.; Tan, Y. Prognostic Value of Tumor-Infiltrating Lymphocytes in Hepatocellular Carcinoma A Meta-Analysis. Medicine 2018, 97, e13301. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Won, H.S.; Sun, D.S.; Hong, J.H.; Ko, Y.H. Prognostic Role of Tumor-Infiltrating Lymphocytes in Gastric Cancer A Systematic Review and Meta-Analysis. Medicine 2018, 97, e11769. [Google Scholar] [CrossRef] [PubMed]
- Orhan, A.; Vogelsang, R.P.; Andersen, M.B.; Madsen, M.T.; Hölmich, E.R.; Raskov, H.; Gögenur, I. The Prognostic Value of Tumour-Infiltrating Lymphocytes in Pancreatic Cancer: A Systematic Review and Meta-Analysis. Eur. J. Cancer 2020, 132, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Dworak, O.; Keilholz, L.; Hoffmann, A. Pathological Features of Rectal Cancer after Preoperative Radiochemotherapy. Int. J. Colorectal Dis. 1997, 12, 19–23. [Google Scholar] [CrossRef]
- Mandard, A.-M.; Dalibard, F.; Mandard, J.-C.; Marnay, J.; Henry-Amar, M.; Petiot, J.-F.; Roussel, A.; Jacob, J.-H.; Segol, P.; Samama, G.; et al. Pathologic Assessment of Tumor Regression after Preoperative Chemoradiotherapy of Esophageal Carcinoma. Clinicopathologic Correlations. Cancer 1994, 73, 2680–2686. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical Methods for Incorporating Summary Time-to-Event Data into Meta-Analysis. Trials 2007, 8, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. Statistics in Practice How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Möbius, T.W.D. Metagen: Inference in Meta Analysis and Meta Regression. Available online: http://00tau.github.io/metagen/ (accessed on 12 December 2020).
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- IntHout, J.; Ioannidis, J.P.; Borm, G.F. The Hartung-Knapp-Sidik-Jonkman Method for Random Effects Meta-Analysis Is Straightforward and Considerably Outperforms the Standard DerSimonian-Laird Method. BMC Med. Res. Methodol. 2014, 14, 1–12. [Google Scholar] [CrossRef] [Green Version]
- IntHout, J.; Ioannidis, J.P.A.; Rovers, M.M.; Goeman, J.J. Plea for Routinely Presenting Prediction Intervals in Meta-Analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altman, D.G.; Bland, J.M. How to Obtain the Confidence Interval from a P Value. BMJ 2011, 343, d2090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 December 2020).
- Huguet, A.; Hayden, J.A.; Stinson, J.; McGrath, P.J.; Chambers, C.T.; Tougas, M.E.; Wozney, L. Judging the Quality of Evidence in Reviews of Prognostic Factor Research: Adapting the GRADE Framework. Syst. Rev. 2013, 2, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinto, E.; Hase, K.; Hashiguchi, Y.; Sekizawa, A.; Ueno, H.; Shikina, A.; Kajiwara, Y.; Kobayashi, H.; Ishiguro, M.; Yamamoto, J. CD8+ and FOXP3+ Tumor-Infiltrating T Cells Before and After Chemoradiotherapy for Rectal Cancer. Ann. Surg. Oncol. 2014, 21, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Shinto, E.; Omata, J.; Sikina, A.; Sekizawa, A.; Kajiwara, Y.; Hayashi, K.; Hashiguchi, Y.; Hase, K.; Ueno, H. Predictive Immunohistochemical Features for Tumour Response to Chemoradiotherapy in Rectal Cancer. BJS Open 2020, 4, 301–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsutani, S.; Shibutani, M.; Maeda, K.; Nagahara, H.; Fukuoka, T.; Nakao, S.; Hirakawa, K.; Ohira, M. Significance of Tumor-Infiltrating Lymphocytes before and after Neoadjuvant Therapy for Rectal Cancer. Cancer Sci. 2018, 109, 966–979. [Google Scholar] [CrossRef] [Green Version]
- Zaghloul, H.; Abbas, A.; Abdulah, D. Tumor Microenvironment Mediators CD8+- and FOXP3+-Labeled T Lymphocytes Are Prospective Prognosticators in Curatively Treated Rectal Cancer Patients. J. Gastrointest. Cancer 2020, 52, 177–186. [Google Scholar] [CrossRef]
- Zhang, S.; Bai, W.; Tong, X.; Bu, P.; Xu, J.; Xi, Y. Correlation between Tumor Microenvironment-associated Factors and the Efficacy and Prognosis of Neoadjuvant Therapy for Rectal Cancer. Oncol. Lett. 2019, 17, 1062–1070. [Google Scholar] [CrossRef]
- Akiyoshi, T.; Tanaka, N.; Kiyotani, K.; Gotoh, O.; Yamamoto, N.; Oba, K.; Fukunaga, Y.; Ueno, M.; Mori, S. Immunogenomic Profiles Associated with Response to Neoadjuvant Chemoradiotherapy in Patients with Rectal Cancer. Br. J. Surg. 2019, 106, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.-W.; Huang, K.C.-Y.; Chiang, S.-F.; Chen, W.T.-L.; Ke, T.-W.; Chao, K.S.C. Prognostic Relevance of Programmed Cell Death-Ligand 1 Expression and CD8+ TILs in Rectal Cancer Patients before and after Neoadjuvant Chemoradiotherapy. J. Cancer Res. Clin. Oncol. 2019, 145, 1043–1053. [Google Scholar] [CrossRef] [PubMed]
- Malekzadeh Moghani, M.; Alahyari, S.; Moradi, A.; Nasiri, M. Pathological Predictors of Response to Neoadjuvant Treatment in Rectal Carcinoma. J. Gastrointest. Cancer 2020, 52, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Xiao, B.; Peng, J.; Zhang, R.; Xu, J.; Wang, Y.; Fang, Y.; Lin, J.; Pan, Z.; Wu, X. Density of CD8+ Lymphocytes in Biopsy Samples Combined with the Circulating Lymphocyte Ratio Predicts Pathologic Complete Response to Chemoradiotherapy for Rectal Cancer. Cancer Manag. Res. 2017, 9, 701–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Lou, X.; Zhu, Y.; Wang, Y.; Zhang, L.; Liu, H.; Wang, C.; Zhan, H.; Cheng, Z.; Tan, W.; et al. Local Environment in Biopsy Better Predict the Pathological Response to Neoadjuvant Chemoradiotherapy in Rectal Cancer. Biosci. Rep. 2019, 39, 20190003. [Google Scholar] [CrossRef] [Green Version]
- Mirjolet, C.; Charon-Barra, C.; Ladoire, S.; Arbez-Gindre, F.; Bertaut, A.; Ghiringhelli, F.; Leroux, A.; Peiffert, D.; Borg, C.; Bosset, J.F.; et al. Tumor Lymphocyte Immune Response to Preoperative Radiotherapy in Locally Advanced Rectal Cancer: The LYMPHOREC Study. Oncoimmunology 2017, 7, e1396402. [Google Scholar] [CrossRef]
- Huang, A.; Xiao, Y.; Peng, C.; Liu, T.; Lin, Z.; Yang, Q.; Zhang, T.; Liu, J.; Ma, H. 53BP1 Expression and Immunoscore Are Associated with the Efficacy of Neoadjuvant Chemoradiotherapy for Rectal Cancer. Strahlenther. Und Onkol. 2019, 196, 465–473. [Google Scholar] [CrossRef]
- Rudolf, J.; Büttner-Herold, M.; Erlenbach-Wünsch, K.; Posselt, R.; Jessberger, J.; Haderlein, M.; Hecht, M.; Hartmann, A.; Fietkau, R.; Distel, L. Regulatory T Cells and Cytotoxic T Cells Close to the Epithelial–Stromal Interface Are Associated with a Favorable Prognosis. Oncoimmunology 2020, 9, 1746149. [Google Scholar] [CrossRef] [Green Version]
- El Sissy, C.; Kirilovsky, A.; van den Eynde, M.; Muşină, A.-M.; Anitei, M.-G.; Romero, A.; Marliot, F.; Junca, A.; Doyen, J.; Mlecnik, B.; et al. A Diagnostic Biopsy-Adapted Immunoscore Predicts Response to Neoadjuvant Treatment and Selects Patients with Rectal Cancer Eligible for a Watch-and-Wait Strategy. Clin. Cancer Res. 2020, 26, 5198–5207. [Google Scholar] [CrossRef]
- Apetoh, L.; Ghiringhelli, F.; Tesniere, A.; Obeid, M.; Ortiz, C.; Criollo, A.; Mignot, G.; Maiuri, M.C.; Ullrich, E.; Saulnier, P.; et al. Toll-like Receptor 4–Dependent Contribution of the Immune System to Anticancer Chemotherapy and Radiotherapy. Nat. Med. 2007, 13, 1050–1059. [Google Scholar] [CrossRef]
- Lee, Y.; Auh, S.L.; Wang, Y.; Burnette, B.; Wang, Y.; Meng, Y.; Beckett, M.; Sharma, R.; Chin, R.; Tu, T.; et al. Therapeutic Effects of Ablative Radiation on Local Tumor Require CD8+ T Cells: Changing Strategies for Cancer Treatment. Blood 2009, 114, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Vacchelli, E.; Galluzzi, L.; Fridman, W.H.; Galon, J.; Sautès-Fridman, C.; Tartour, E.; Kroemer, G. Trial Watch. OncoImmunology 2012, 1, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frey, B.; Rubner, Y.; Kulzer, L.; Werthmöller, N.; Weiss, E.-M.; Fietkau, R.; Gaipl, U.S. Antitumor Immune Responses Induced by Ionizing Irradiation and Further Immune Stimulation. Cancer Immunol. Immunother. 2013, 63, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Lugade, A.A.; Moran, J.P.; Gerber, S.A.; Rose, R.C.; Frelinger, J.G.; Lord, E.M. Local Radiation Therapy of B16 Melanoma Tumors Increases the Generation of Tumor Antigen-Specific Effector Cells That Traffic to the Tumor. J. Immunol. 2005, 174, 7516–7523. [Google Scholar] [CrossRef] [Green Version]
- Lugade, A.A.; Sorensen, E.W.; Gerber, S.A.; Moran, J.P.; Frelinger, J.G.; Lord, E.M. Radiation-Induced IFN-γ Production within the Tumor Microenvironment Influences Antitumor Immunity. J. Immunol. 2008, 180, 3132–3139. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Taube, J.M.; Pardoll, D.M. Neoadjuvant Checkpoint Blockade for Cancer Immunotherapy. Science 2020, 367, eaax0182. [Google Scholar] [CrossRef]
- Joseph, E.L.M.; Kirilovsky, A.; Lecoester, B.; El Sissy, C.; Boullerot, L.; Rangan, L.; Marguier, A.; Tochet, F.; Dosset, M.; Boustani, J.; et al. Chemoradiation Triggers Antitumor Th1 and Tissue Resident Memory-Polarized Immune Responses to Improve Immune Checkpoint Inhibitors Therapy. J. Immunother. Cancer 2021, 9, e002256. [Google Scholar] [CrossRef]
- Andersson, P.; Ostheimer, C. Editorial: Combinatorial Approaches to Enhance Anti-Tumor Immunity: Focus on Immune Checkpoint Blockade Therapy. Front. Immunol. 2019, 10, 2083. [Google Scholar] [CrossRef]
- Rahma, O.E.; Yothers, G.; Hong, T.S.; Russell, M.M.; You, Y.N.; Parker, W.; Jacobs, S.A.; Colangelo, L.H.; Lucas, P.C.; Gollub, M.J.; et al. Use of Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer: Initial Results From the Pembrolizumab Arm of a Phase 2 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 1225–1230. [Google Scholar] [CrossRef]
- Galon, J.; Bruni, D. Tumor Immunology and Tumor Evolution: Intertwined Histories. Immunity 2020, 52, 55–81. [Google Scholar] [CrossRef]
- Galon, J.; Bruni, D. Approaches to Treat Immune Hot, Altered and Cold Tumours with Combination Immunotherapies. Nat. Rev. Drug Discov. 2019, 18, 197–218. [Google Scholar] [CrossRef] [PubMed]
- Bettoni, F.; Masotti, C.; Habr-Gama, A.; Correa, B.R.; Gama-Rodrigues, J.; Vianna, M.R.; Vailati, B.B.; Julião, G.P.S.; Fernandez, L.M.; Galante, P.A.; et al. Intratumoral Genetic Heterogeneity in Rectal Cancer: Are Single Biopsies Representative of the Entirety of the Tumor? Ann. Surg. 2017, 265, e4–e6. [Google Scholar] [CrossRef] [PubMed]
- van den Eynde, M.; Mlecnik, B.; Bindea, G.; Pagè, F.; Machiels, J.-P. The Link between the Multiverse of Immune Microenvironments in Metastases and the Survival of Colorectal Cancer Patients. Cancer Cell 2018, 34, 1012–1026. [Google Scholar] [CrossRef] [Green Version]
- Mlecnik, B.; Bifulco, C.; Bindea, G.; Marliot, F.; Lugli, A.; Lee, J.J.; Zlobec, I.; Rau, T.T.; Berger, M.D.; Nagtegaal, I.D.; et al. Multicenter International Society for Immunotherapy of Cancer Study of the Consensus Immunoscore for the Prediction of Survival and Response to Chemotherapy in Stage III Colon Cancer. J. Clin. Oncol. 2020, 38, 3638–3651. [Google Scholar] [CrossRef] [PubMed]
- Pagès, F.; Mlecnik, B.; Marliot, F.; Bindea, G.; Ou, F.S.; Bifulco, C.; Lugli, A.; Zlobec, I.; Rau, T.T.; Berger, M.D.; et al. International Validation of the Consensus Immunoscore for the Classification of Colon Cancer: A Prognostic and Accuracy Study. Lancet 2018, 391, 2128–2139. [Google Scholar] [CrossRef]
- Chetty, R.; Gill, P.; Govender, D.; Bateman, A.; Chang, H.J.; Deshpande, V.; Driman, D.; Gomez, M.; Greywoode, G.; Jaynes, E.; et al. International Study Group on Rectal Cancer Regression Grading: Interobserver Variability with Commonly Used Regression Grading Systems. Hum. Pathol. 2012, 43, 1917–1923. [Google Scholar] [CrossRef] [PubMed]
- Westerhoff, M.; Osecky, M.; Langer, R. Varying Practices in Tumor Regression Grading of Gastrointestinal Carcinomas after Neoadjuvant Therapy: Results of an International Survey. Mod. Pathol. 2019, 33, 676–689. [Google Scholar] [CrossRef]
- Loughrey, M.; Quirke, P.; Shepherd, N. Dataset for Histopathological Reporting of Colorectal Cancer; Version 4; The Royal College of Pathologists: London, UK, 2018. [Google Scholar]
- Loughrey, M.B.; Webster, F.; Arends, M.J.; Brown, I.; Burgart, L.J.; Cunningham, C.; Flejou, J.-F.; Kakar, S.; Kirsch, R.; Kojima, M.; et al. Dataset for Pathology Reporting of Colorectal Cancer. Ann. Surg. 2021; Preprint. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | UICC Stage | TILs Density Cut-Off | TRG System | Treatment Response Defined as | Inclusion in Meta-Analysis |
|---|---|---|---|---|---|
| Anitei et al. [5] | II–III | Median | Dworak | TRG 3-4 | CD3 (pTR) |
| Yasuda et al. [6] | II–IV | Unspecified | JCCC | pCR | CD8 (pCR) |
| Teng et al. (A) [9] | II–III | Median | Dworak | TRG 3-4 | CD4 (pTR) FOXP3 (pTR, DFS) CD8 (pTR, OS, DFS) |
| Teng et al. (B) [10] | II–III | Median | Dworak | TRG 3-4 | CD3 (pTR) CD8 (pTR, OS, DFS) |
| McCoy et al. [11] | II–IV | Median | Dworak | TRG 3-4 | none |
| Shinto et al. (A) [28] | II–III | Median | Dworak | TRG 3-4 | FOXP3 (pTR, DFS) CD8 (pTR, DFS) |
| Shinto et al. (B) [29] | II–III | Unspecified | Dworak | pCR, TRG 3-4 | CD8 (pCR, pTR) |
| Matsutani et al. [30] | II–III | Median | JCCC | TRG 1b-3 | CD4 (pTR) FOXP3 (pTR) CD8 (pTR) |
| Zaghloul et al. [31] | II–III | ROC | Unspecified | pCR | FOXP3 (DFS) CD8 (pCR, OS, DFS) |
| Zhang et al. [32] | II–III | Mean | Dworak | TRG 3-4 | CD4 (pTR) FOXP3 (pTR) CD8 (pTR) |
| Akiyoshi et al. [33] | II–III | Median | Dworak | pCR, TRG 3-4 | CD8 (pCR, pTR, DFS) |
| Chen et al. [34] | II–III | Unspecified | Dworak | TRG 3-4 | CD8 (OS, DFS) |
| Moghani et al. [35] | II–III | 11 cells/high power field | AJCC | pCR, TRG 0-1 | CD8 (pCR, pTR) |
| Xiao et al. [36] | II–III | Unspecified | Mandard | pCR | CD8 (pCR) |
| Huang, Y et al. [37] | II–III | Unspecified | AJCC | TRG 0-1 | CD4 (pTR) CD8 (pTR) |
| Mirjolet et al. [38] | II–III | None | Unspecified | Unspecified | none |
| Huang, A et al. [39] | II–III | CD3/CD8 combined | Dworak | TRG 3-4 | none |
| Rudolf et al. [40] | II–IV | Median | Dworak | Unspecified | none |
| Sissy et al. [41] | II–III | CD3/CD8 combined | Dworak | Unspecified | none |
| Outcome | Biomarker | Studies | n | Point Estimate | Lower 95% CI | Higher 95% CI | I2 | GRADE Level of Evidence |
|---|---|---|---|---|---|---|---|---|
| pCR | CD8+ TILs | 6 | 692 | 2.71 | 1.58 | 4.66 | 0% | Moderate |
| pTR | CD3+ TILs | 2 | 191 | 1.63 | 0.35 | 7.69 | 0% | Low |
| CD4+ TILs | 4 | 342 | 1.23 | 0.83 | 1.82 | 0% | Low | |
| CD8+ TILs | 9 | 1073 | 1.86 | 1.50 | 2.29 | 0% | Moderate | |
| FOXP3+ TILs | 4 | 294 | 0.85 | 0.20 | 3.58 | 76% | Very low | |
| DFS | CD8+ TILs | 6 | 716 | 0.57 | 0.38 | 0.86 | 25% | Moderate |
| FOXP3+ TILs | 3 | 193 | 1.66 | 0.17 | 16.32 | 62% | Very low | |
| OS | CD8+ TILs | 4 | 360 | 0.43 | 0.27 | 0.69 | 0% | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orhan, A.; Khesrawi, F.; Tvilling Madsen, M.; Peuliche Vogelsang, R.; Dohrn, N.; Kanstrup Fiehn, A.-M.; Gögenur, I. Tumor-Infiltrating Lymphocytes as Biomarkers of Treatment Response and Long-Term Survival in Patients with Rectal Cancer: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 636. https://doi.org/10.3390/cancers14030636
Orhan A, Khesrawi F, Tvilling Madsen M, Peuliche Vogelsang R, Dohrn N, Kanstrup Fiehn A-M, Gögenur I. Tumor-Infiltrating Lymphocytes as Biomarkers of Treatment Response and Long-Term Survival in Patients with Rectal Cancer: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(3):636. https://doi.org/10.3390/cancers14030636
Chicago/Turabian StyleOrhan, Adile, Faisal Khesrawi, Michael Tvilling Madsen, Rasmus Peuliche Vogelsang, Niclas Dohrn, Anne-Marie Kanstrup Fiehn, and Ismail Gögenur. 2022. "Tumor-Infiltrating Lymphocytes as Biomarkers of Treatment Response and Long-Term Survival in Patients with Rectal Cancer: A Systematic Review and Meta-Analysis" Cancers 14, no. 3: 636. https://doi.org/10.3390/cancers14030636