
Update on Management Recommendations for Advanced Cutaneous Squamous Cell Carcinoma

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Tumour Staging and Prognostic Factors
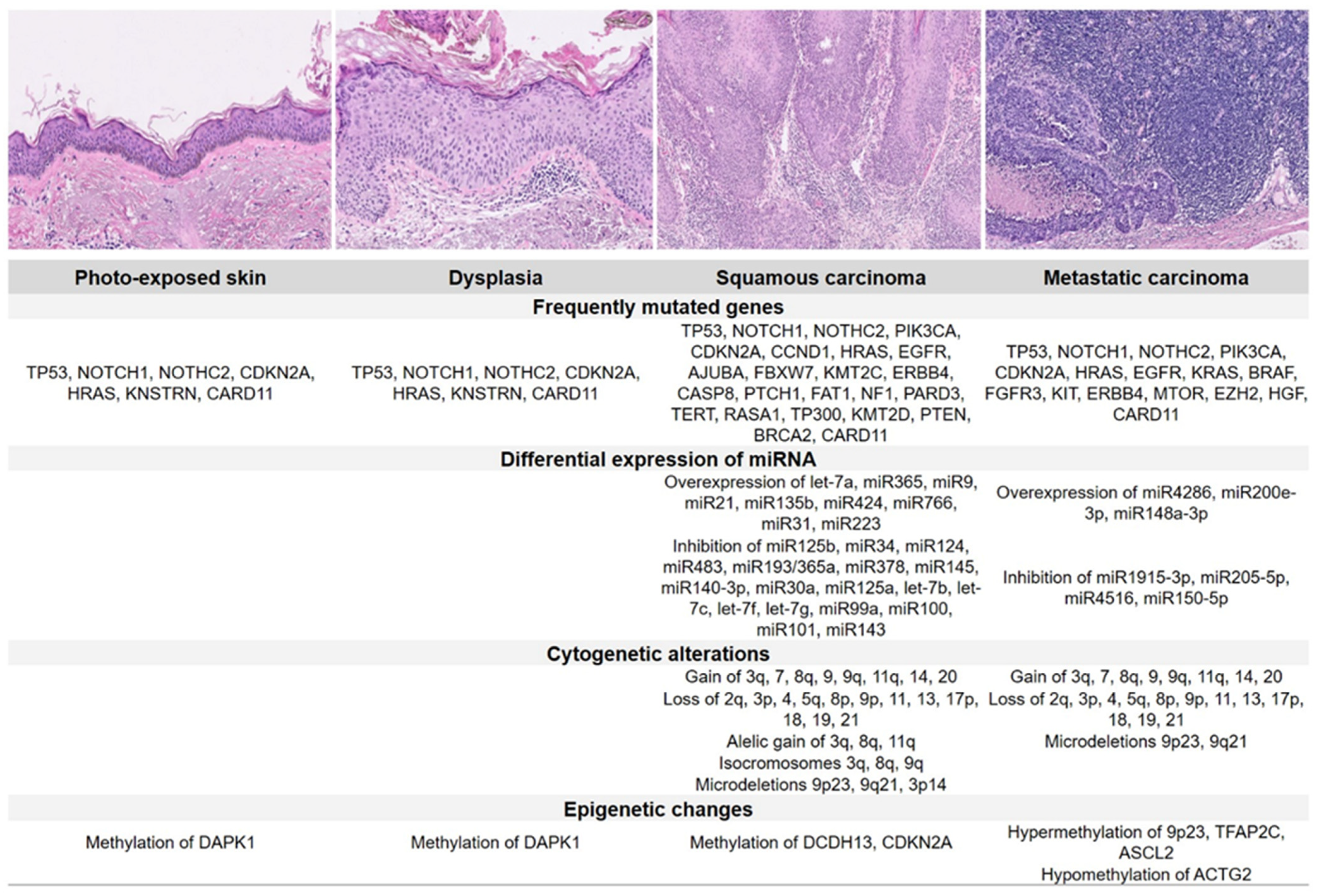
3. Molecular Pathology and Emerging Biomarkers
4. Diagnosis
4.1. Dermatology
4.2. Histopathology
4.3. Medical Imaging
4.4. Assessment of Comorbidities
5. Risk Stratification
6. Treatment
6.1. Role of Surgery in Primary Tumours
6.2. Locoregional Assessment and Sentinel Node Biopsy
6.3. Local Treatment
6.4. Role of Radiotherapy
6.5. Systemic Treatment
6.5.1. Chemotherapy
6.5.2. Targeted Therapy
6.5.3. Immunotherapy
7. Immunosuppressed Patients
8. Follow-Up and Monitoring
9. Summary and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karia, P.S.; Han, J.; Schmults, C.D. Cutaneous squamous cell carcinoma: Estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. J. Am. Acad. Dermatol. 2013, 68, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Flohil, S.C.; van der Leest, R.J.; Arends, L.R.; de Vries, E.; Nijsten, T. Risk of subsequent cutaneous malignancy in patients with prior keratinocyte carcinoma: A systematic review and meta-analysis. Eur. J. Cancer 2013, 49, 2365–2375. [Google Scholar] [CrossRef] [PubMed]
- Tejera-Vaquerizo, A.; Descalzo-Gallego, M.A.; Otero-Rivas, M.M.; Posada-García, C.; Rodríguez-Pazos, L.; Pastushenko, I.; Marcos-Gragera, R.; García-Doval, I. Skin Cancer Incidence and Mortality in Spain: A Systematic Review and Meta-Analysis. Actas Dermosifiliogr. 2016, 107, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.K.; Kricker, A. The epidemiology of UV induced skin cancer. J. Photochem. Photobiol. B 2001, 63, 8–18. [Google Scholar] [CrossRef]
- Stern, R.S. The risk of squamous cell and basal cell cancer associated with psoralen and ultraviolet A therapy: A 30-year prospective study. J. Am. Acad. Dermatol. 2012, 66, 553–562. [Google Scholar] [CrossRef]
- Lindelöf, B.; Sigurgeirsson, B.; Gäbel, H.; Stern, R.S. Incidence of skin cancer in 5356 patients following organ transplantation. Br. J. Dermatol. 2000, 143, 513–519. [Google Scholar]
- National Comprehensive Cancer Center. NCCN Clinical Practice Guidelines in Oncology; Squamous Cell Carcinoma (V2. 2018). Available online: https://oncolife.com.ua/doc/nccn/Squamous_Cell_Skin_Cancer.pdf (accessed on 13 September 2021).
- Stratigos, A.J.; Garbe, C.; Dessinioti, C.; Lebbe, C.; Bataille, V.; Bastholt, L.; Dreno, B.; Concetta Fargnoli, M.; Forsea, A.M.; Frenard, C.; et al. European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: Part 2. Treatment. Eur. J. Cancer 2020, 128, 83–102. [Google Scholar] [CrossRef] [Green Version]
- Combalia, A.; Carrera, C. Squamous Cell Carcinoma: An Update on Diagnosis and Treatment. Dermatol. Pract. Concept 2020, 10, e2020066. [Google Scholar] [CrossRef]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef]
- Norman, G. Likert scales, levels of measurement and the “laws” of statistics. Adv. Health Sci. Educ. Theory Pract. 2010, 15, 625–632. [Google Scholar] [CrossRef]
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D.; Burnanrd, B.; LaCalle, J.R.; Lazaro, P.; van het Loo, M.; McDonell, J.; Vader, J.; Kahan, J.P. The Rand/UCLA Appropriateness Method User’s Manual; RAND Corporation: Santa Monica, CA, USA, 2001; Available online: https://www.rand.org/pubs/monograph_reports/MR1269.html (accessed on 3 March 2021).
- Armin, M.B.; Edge, S.B.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Brantsch, K.D.; Meisner, C.; Schönfisch, B.; Trilling, B.; Wehner-Caroli, J.; Röcken, M.; Breuninger, H. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: A prospective study. Lancet Oncol. 2008, 9, 713–720. [Google Scholar] [CrossRef]
- Karia, P.S.; Jambusaria-Pahlajani, A.; Harrington, D.P.; Murphy, G.F.; Qureshi, A.A.; Schmults, C.D. Evaluation of American JoInt. Committee on Cancer, International Union against Cancer, and Brigham and Women’s Hospital tumor staging for cutaneous squamous cell carcinoma. J. Clin. Oncol. 2014, 32, 327–334. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, E.S.; Karia, P.S.; Besaw, R.; Schmults, C.D. Performance of the American Joint. Committee on Cancer Staging Manual, 8th Edition vs the Brigham and Women’s Hospital Tumor Classification System for Cutaneous Squamous Cell Carcinoma. JAMA Dermatol. 2019, 155, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Blechman, A.B.; Carucci, J.A.; Stevenson, M.L. Stratification of Poor Outcomes for Cutaneous Squamous Cell Carcinoma in Immunosuppressed Patients Using the American JoInt. Committee on Cancer Eighth Edition and Brigham and Women’s Hospital Staging Systems. Dermatol. Surg. 2019, 45, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Tejera-Vaquerizo, A.; Canueto, J.; Llombart, B.; Martorell-Calatayud, A.; Sanmartin, O. Predictive Value of Sentinel Lymph Node Biopsy in Cutaneous Squamous Cell Carcinoma Based on the AJCC-8 and Brigham and Women’s Hospital Staging Criteria. Dermatol. Surg. 2020, 46, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Stratigos, A.J.; Garbe, C.; Dessinioti, C.; Lebbe, C.; Bataille, V.; Bastholt, L.; Dreno, B.; Fargnoli, M.C.; Forsea, A.M.; Frenard, C.; et al. European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: Part 1. epidemiology, diagnostics and prevention. Eur. J. Cancer 2020, 128, 60–82. [Google Scholar] [CrossRef] [Green Version]
- Alam, M.; Armstrong, A.; Baum, C.; Bordeaux, J.S.; Brown, M.; Busam, K.J.; Eisen, D.B.; Iyengar, V.; Lober, C.; Margolis, D.J.; et al. Guidelines of care for the management of cutaneous squamous cell carcinoma. J. Am. Acad. Dermatol. 2018, 78, 560–578. [Google Scholar] [CrossRef] [Green Version]
- Cañueto, J.; Martín-Vallejo, J.; Cardeñoso-Álvarez, E.; Fernández-López, E.; Pérez-Losada, J.; Román-Curto, C. Rapid growth rate is associated with poor prognosis in cutaneous squamous cell carcinoma. Clin. Exp. Dermatol. 2018, 43, 876–882. [Google Scholar] [CrossRef]
- Gonzalez-Guerrero, M.; Martínez-Camblor, P.; Vivanco, B.; Fernández-Vega, I.; Munguía-Calzada, P.; Gonzalez-Gutierrez, M.P.; Rodrigo, J.P.; Galache, C.; Santos-Juanes, J. The adverse prognostic effect of tumor budding on the evolution of cutaneous head and neck squamous cell carcinoma. J. Am. Acad. Dermatol. 2017, 76, 1139–1145. [Google Scholar] [CrossRef]
- Pickering, C.R.; Zhou, J.H.; Lee, J.J.; Drummond, J.A.; Peng, S.A.; Saade, R.E.; Tsai, K.Y.; Curry, J.L.; Tetzlaff, M.T.; Lai, S.Y.; et al. Mutational landscape of aggressive cutaneous squamous cell carcinoma. Clin. Cancer Res. 2014, 20, 6582–6592. [Google Scholar] [CrossRef] [Green Version]
- Hussein, M.R. Ultraviolet radiation and skin cancer: Molecular mechanisms. J. Cutan. Pathol. 2005, 32, 191–205. [Google Scholar] [CrossRef]
- Durinck, S.; Ho, C.; Wang, N.J.; Liao, W.; Jakkula, L.R.; Collisson, E.A.; Pons, J.; Chan, S.W.; Lam, E.T.; Chu, C.; et al. Temporal dissection of tumorigenesis in primary cancers. Cancer Discov. 2011, 1, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Botti, E.; Spallone, G.; Moretti, F.; Marinari, B.; Pinetti, V.; Galanti, S.; De Meo, P.D.; De Nicola, F.; Ganci, F.; Castrignanò, T.; et al. Developmental factor IRF6 exhibits tumor suppressor activity in squamous cell carcinomas. Proc. Natl. Acad. Sci. USA 2011, 108, 13710–13715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriyama, M.; Durham, A.D.; Moriyama, H.; Hasegawa, K.; Nishikawa, S.; Radtke, F.; Osawa, M. Multiple roles of Notch signaling in the regulation of epidermal development. Dev. Cell 2008, 14, 594–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, F.; Viros, A.; Milagre, C.; Trunzer, K.; Bollag, G.; Spleiss, O.; Reis-Filho, J.S.; Kong, X.; Koya, R.C.; Flaherty, K.T.; et al. RAS Mutations in Cutaneous Squamous-Cell Carcinomas in Patients Treated with BRAF Inhibitors. N. Engl. J. Med. 2012, 366, 207–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Küsters-Vandevelde, H.V.; Van Leeuwen, A.; Verdijk, M.A.; de Koning, M.N.; Quint, W.G.; Melchers, W.J.; Ligtenberg, M.J.; Blokx, W.A. CDKN2A but not TP53 mutations nor HPV presence predict poor outcome in metastatic squamous cell carcinoma of the skin. Int. J. Cancer 2010, 126, 2123–2132. [Google Scholar] [CrossRef]
- Darr, O.A.; Colacino, J.A.; Tang, A.L.; McHugh, J.B.; Bellile, E.L.; Bradford, C.R.; Prince, M.P.; Chepeha, D.B.; Rozek, L.S.; Moyer, J.S. Epigenetic alterations in metastatic cutaneous carcinoma. Head Neck 2015, 37, 994–1001. [Google Scholar] [CrossRef] [Green Version]
- Lui, V.W.; Peyser, N.D.; Ng, P.K.; Hritz, J.; Zeng, Y.; Lu, Y.; Li, H.; Wang, L.; Gilbert, B.R.; General, I.J.; et al. Frequent mutation of receptor protein tyrosine phosphatases provides a mechanism for STAT3 hyperactivation in head and neck cancer. Proc. Natl. Acad. Sci. USA 2014, 111, 1114–1119. [Google Scholar] [CrossRef] [Green Version]
- Commandeur, S.; Ho, S.H.; de Gruijl, F.R.; Willemze, R.; Tensen, C.P.; El Ghalbzouri, A. Functional characterization of cancer-associated fibroblasts of human cutaneous squamous cell carcinoma. Exp. Dermatol. 2011, 20, 737–742. [Google Scholar] [CrossRef]
- Moussai, D.; Mitsui, H.; Pettersen, J.S.; Pierson, K.C.; Shah, K.R.; Suárez-Fariñas, M.; Cardinale, I.R.; Bluth, M.J.; Krueger, J.G.; Carucci, J.A. The human cutaneous squamous cell carcinoma microenvironment is characterized by increased lymphatic density and enhanced expression of macrophage-derived VEGF-C. J. Investig. Dermatol. 2011, 131, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, M.; Stockfleth, E.; Roewert-Huber, J.; Astner, S. Noninvasive diagnostic tools for nonmelanoma skin cancer. Br. J. Dermatol. 2007, 157, 56–58. [Google Scholar] [CrossRef]
- Warszawik-Hendzel, O.; Olszewska, M.; Maj, M.; Rakowska, A.; Czuwara, J.; Rudnicka, L. Non-invasive diagnostic techniques in the diagnosis of squamous cell carcinoma. J. Dermatol. Case Rep. 2015, 9, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Zalaudek, I.; Giacomel, J.; Schmid, K.; Bondino, S.; Rosendahl, C.; Cavicchini, S.; Tourlaki, A.; Gasparini, S.; Bourne, P.; Keir, J.; et al. Dermatoscopy of facial actinic keratosis, intraepidermal carcinoma, and invasive squamous cell carcinoma: A progression model. J. Am. Acad. Dermatol. 2012, 66, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Yanofsky, V.R.; Mercer, S.E.; Phelps, R.G. Histopathological variants of cutaneous squamous cell carcinoma: A review. J. Skin Cancer 2011, 2011, 210813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, A.K.; Kelley, B.F.; Prokop, L.J.; Murad, M.H.; Baum, C.L. Risk Factors for Cutaneous Squamous Cell Carcinoma Recurrence, Metastasis, and Disease-Specific Death: A Systematic Review and Meta-analysis. JAMA Dermatol. 2016, 152, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Liao, L.J.; Lo, W.C.; Hsu, W.L.; Wang, C.T.; Lai, M.S. Detection of cervical lymph node metastasis in head and neck cancer patients with clinically N0 neck-a meta-analysis comparing different imaging modalities. BMC Cancer 2012, 12, 236. [Google Scholar] [CrossRef]
- Jennings, L.; Schmults, C.D. Management of high-risk cutaneous squamous cell carcinoma. J. Clin. Aesthetic Dermatol. 2010, 3, 39–48. [Google Scholar]
- Connolly, K.L.; Jeong, J.M.; Barker, C.A.; Hernandez, M.; Lee, E.H. A systematic review of comorbidity indices used in the nonmelanoma skin cancer population. J. Am. Acad. Dermatol. 2017, 76, 344–346.e2. [Google Scholar] [CrossRef] [Green Version]
- Dhiwakar, M.; Khan, N.A.; McClymont, L.G. Surgery for head and neck skin tumors in the elderly. Head Neck 2007, 29, 851–856. [Google Scholar] [CrossRef]
- Charles, A.J., Jr.; Otley, C.C.; Pond, G.R. Prognostic factors for life expectancy in nonagenarians with nonmelanoma skin cancer: Implications for selecting surgical candidates. J. Am. Acad. Dermatol. 2002, 47, 419–422. [Google Scholar] [CrossRef]
- Delaney, A.; Shimizu, I.; Goldberg, L.H.; MacFarlane, D.F. Life expectancy after Mohs micrographic surgery in patients aged 90 years and older. J. Am. Acad. Dermatol. 2013, 68, 296–300. [Google Scholar] [CrossRef]
- Reid, B.C.; Alberg, A.J.; Klassen, A.C.; Koch, W.M.; Samet, J.M. The American Society of Anesthesiologists’ class as a comorbidity index in a cohort of head and neck cancer surgical patients. Head Neck 2001, 23, 985–994. [Google Scholar] [CrossRef]
- Lee, E.H.; Nijhawan, R.I.; Nehal, K.S.; Dusza, S.W.; Levine, A.; Hill, A.; Barker, C.A. Comorbidity Assessment in Skin Cancer Patients: A Pilot Study Comparing Medical Interview with a Patient-Reported Questionnaire. J. Skin Cancer 2015, 2015, 953479. [Google Scholar] [CrossRef] [PubMed]
- Porceddu, S.V.; Bressel, M.; Poulsen, M.G.; Stoneley, A.; Veness, M.J.; Kenny, L.M.; Wratten, C.; Corry, J.; Cooper, S.; Fogarty, G.B.; et al. Postoperative Concurrent Chemoradiotherapy Versus Postoperative Radiotherapy in High-Risk Cutaneous Squamous Cell Carcinoma of the Head and Neck: The Randomized Phase III TROG 05.01 Trial. J. Clin. Oncol. 2018, 36, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.B.; Johnson, M.M.; Chua, T.L.; Karia, P.S.; Schmults, C.D. Outcomes of Primary Cutaneous Squamous Cell Carcinoma with Perineural Invasion: An 11-Year Cohort Study. JAMA Dermatol. 2013, 149, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karia, P.S.; Morgan, F.C.; Ruiz, E.S.; Schmults, C.D. Clinical and Incidental Perineural Invasion of Cutaneous Squamous Cell Carcinoma: A Systematic Review and Pooled Analysis of Outcomes Data. JAMA Dermatol. 2017, 153, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Navarrete-Dechent, C.; Veness, M.J.; Droppelmann, N.; Uribe, P. High-risk cutaneous squamous cell carcinoma and the emerging role of sentinel lymph node biopsy: A literature review. J. Am. Acad. Dermatol. 2015, 73, 127–137. [Google Scholar] [CrossRef]
- Tejera-Vaquerizo, A.; García-Doval, I.; Llombart, B.; Cañueto, J.; Martorell-Calatayud, A.; Descalzo-Gallego, M.A.; Sanmartín, O. Systematic review of the prevalence of nodal metastases and the prognostic utility of sentinel lymph node biopsy in cutaneous squamous cell carcinoma. J. Dermatol. 2018, 45, 781–790. [Google Scholar] [CrossRef]
- Schmitt, A.R.; Brewer, J.D.; Bordeaux, J.S.; Baum, C.L. Staging for Cutaneous Squamous Cell Carcinoma as a Predictor of Sentinel Lymph Node Biopsy Results: Meta-analysis of American JoInt. Committee on Cancer Criteria and a Proposed Alternative System. JAMA Dermatol. 2014, 150, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Samsanavicius, D.; Kaikaris, V.; Cepas, A.; Ulrich, J.; Makstiene, J.; Rimdeika, R. Importance of sentinel lymphatic node biopsy in detection of early micrometastases in patients with cutaneous squamous cell carcinoma. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 597–603. [Google Scholar] [CrossRef]
- Samsanavičius, D.; Kaikaris, V.; Norvydas, S.J.; Liubauskas, R.; Valiukevičienė, S.; Makštienė, J.; Maslauskas, K.; Rimdeika, R. Sentinel lymph node biopsy for high-risk cutaneous squamous cell carcinoma: Analysis of recurrence-free survival. Medicina 2016, 52, 276–282. [Google Scholar] [CrossRef]
- Lee, C.T.; Lehrer, E.J.; Aphale, A.; Lango, M.; Galloway, T.J.; Zaorsky, N.G. Surgical excision, Mohs micrographic surgery, external-beam radiotherapy, or brachytherapy for indolent skin cancer: An international meta-analysis of 58 studies with 21,000 patients. Cancer 2019, 125, 3582–3594. [Google Scholar] [CrossRef]
- Martin, T.; Moutrie, Z.; Tighe, D.; Haady, H.; Fogarty, G. Volumetric modulated arc therapy (VMAT) for skin field cancerisation of the nose—A technique and case report. Int. J. Radiol. Radiat. Ther. 2018, 5, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Likhacheva, A.; Awan, M.; Barker, C.A.; Bhatnagar, A.; Bradfield, L.; Brady, M.S.; Buzurovic, I.; Geiger, J.L.; Parvathaneni, U.; Zaky, S.; et al. Definitive and Postoperative Radiation Therapy for Basal and Squamous Cell Cancers of the Skin: Executive Summary of an American Society for Radiation Oncology Clinical Practice Guideline. Pract. Radiat. Oncol. 2020, 10, 8–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunaratne, D.A.; Veness, M.J. Efficacy of hypofractionated radiotherapy in patients with non-melanoma skin cancer: Results of a systematic review. J. Med. Imaging Radiat. Oncol. 2018, 62, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Zaorsky, N.G.; Lee, C.T.; Zhang, E.; Keith, S.W.; Galloway, T.J. Hypofractionated radiation therapy for basal and squamous cell skin cancer: A meta-analysis. Radiother. Oncol. 2017, 125, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Okuyama, R.; Saida, T.; Uhara, H. Platinum and anthracycline therapy for advanced cutaneous squamous cell carcinoma. Int. J. Clin. Oncol. 2013, 18, 506–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, H.W.; Weinstock, M.A.; Feldman, S.R.; Coldiron, B.M. Incidence Estimate of Nonmelanoma Skin Cancer (Keratinocyte Carcinomas) in the U.S. Population, 2012. JAMA Dermatol. 2015, 151, 1081–1086. [Google Scholar] [CrossRef]
- Shin, D.M.; Glisson, B.S.; Khuri, F.R.; Clifford, J.L.; Clayman, G.; Benner, S.E.; Forastiere, A.A.; Ginsberg, L.; Liu, D.; Lee, J.J.; et al. Phase II and biologic study of interferon alfa, retinoic acid, and cisplatin in advanced squamous skin cancer. J. Clin. Oncol. 2002, 20, 364–370. [Google Scholar] [CrossRef]
- Cañueto, J.; Cardeñoso, E.; García, J.L.; Santos-Briz, Á.; Castellanos-Martín, A.; Fernández-López, E.; Blanco Gómez, A.; Pérez-Losada, J.; Román-Curto, C. Epidermal growth factor receptor expression is associated with poor outcome in cutaneous squamous cell carcinoma. Br. J. Dermatol. 2017, 176, 1279–1287. [Google Scholar] [CrossRef]
- Gold, K.A.; Kies, M.S.; William, W.N., Jr.; Johnson, F.M.; Lee, J.J.; Glisson, B.S. Erlotinib in the treatment of recurrent or metastatic cutaneous squamous cell carcinoma: A single-arm phase 2 clinical trial. Cancer 2018, 124, 2169–2173. [Google Scholar] [CrossRef]
- William, W.N., Jr.; Feng, L.; Ferrarotto, R.; Ginsberg, L.; Kies, M.; Lippman, S.; Glisson, B.; Kim, E.S. Gefitinib for patients with incurable cutaneous squamous cell carcinoma: A single-arm phase II clinical trial. J. Am. Acad. Dermatol. 2017, 77, 1110–1113.e2. [Google Scholar] [CrossRef]
- Maubec, E.; Petrow, P.; Scheer-Senyarich, I.; Duvillard, P.; Lacroix, L.; Gelly, J.; Certain, A.; Duval, X.; Crickx, B.; Buffard, V.; et al. Phase II study of cetuximab as first-line single-drug therapy in patients with unresectable squamous cell carcinoma of the skin. J. Clin. Oncol. 2011, 29, 3419–3426. [Google Scholar] [CrossRef] [PubMed]
- Foote, M.C.; McGrath, M.; Guminski, A.; Hughes, B.G.; Meakin, J.; Thomson, D.; Zarate, D.; Simpson, F.; Porceddu, S.V. Phase II study of single-agent panitumumab in patients with incurable cutaneous squamous cell carcinoma. Ann. Oncol. 2014, 25, 2047–2052. [Google Scholar] [CrossRef] [PubMed]
- Montaudié, H.; Viotti, J.; Combemale, P.; Dutriaux, C.; Dupin, N.; Robert, C.; Mortier, L.; Kaphan, R.; Duval-Modeste, A.B.; Dalle, S.; et al. Cetuximab is efficient and safe in patients with advanced cutaneous squamous cell carcinoma: A retrospective, multicentre study. Oncotarget 2020, 11, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Vermorken, J.B.; Mesia, R.; Rivera, F.; Remenar, E.; Kawecki, A.; Rottey, S.; Erfan, J.; Zabolotnyy, D.; Kienzer, H.-R.; Cupissol, D.; et al. Platinum-Based Chemotherapy plus Cetuximab in Head and Neck Cancer. N. Engl. J. Med. 2008, 359, 1116–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermorken, J.B.; Trigo, J.; Hitt, R.; Koralewski, P.; Diaz-Rubio, E.; Rolland, F.; Knecht, R.; Amellal, N.; Schueler, A.; Baselga, J. Open-label, uncontrolled, multicenter phase II study to evaluate the efficacy and toxicity of cetuximab as a single agent in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck who failed to respond to platinum-based therapy. J. Clin. Oncol. 2007, 25, 2171–2177. [Google Scholar] [CrossRef]
- Galbiati, D.; Cavalieri, S.; Alfieri, S.; Resteghini, C.; Bergamini, C.; Orlandi, E.; Platini, F.; Locati, L.; Giacomelli, L.; Licitra, L.; et al. Activity of platinum and cetuximab in cutaneous squamous cell cancer not amenable to curative treatment. Drugs Context 2019, 8, 212611. [Google Scholar] [CrossRef]
- Sahni, S.; Valecha, G.; Sahni, A. Role of Anti-PD-1 Antibodies in Advanced Melanoma: The Era of Immunotherapy. Cureus 2018, 10, e3700. [Google Scholar] [CrossRef] [Green Version]
- Goodman, A.M.; Kato, S.; Bazhenova, L.; Patel, S.P.; Frampton, G.M.; Miller, V.; Stephens, P.J.; Daniels, G.A.; Kurzrock, R. Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers. Mol. Cancer Ther. 2017, 16, 2598–2608. [Google Scholar] [CrossRef] [Green Version]
- European Medicines Agency. Libtayo: EPAR—Product Information. Available online: https://www.ema.europa.eu/en/documents/productinformation/libtayo-epar-product-information_en.pdf (accessed on 4 October 2021).
- Regeneron Pharmaceuticals, Inc. LIBTAYO® [Cemiplimab-Rwlc] Injection Full US Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761097s000lbl.pdf (accessed on 14 September 2021).
- Burova, E.; Hermann, A.; Waite, J.; Potocky, T.; Lai, V.; Hong, S.; Liu, M.; Allbritton, O.; Woodruff, A.; Wu, Q.; et al. Characterization of the Anti-PD-1 Antibody REGN2810 and Its Antitumor Activity in Human PD-1 Knock-In Mice. Mol. Cancer Ther. 2017, 16, 861–870. [Google Scholar] [CrossRef] [Green Version]
- Migden, M.R.; Rischin, D.; Schmults, C.D.; Guminski, A.; Hauschild, A.; Lewis, K.D.; Chung, C.H.; Hernandez-Aya, L.; Lim, A.M.; Chang, A.L.S.; et al. PD-1 Blockade with Cemiplimab in Advanced Cutaneous Squamous-Cell Carcinoma. N. Engl. J. Med. 2018, 379, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Rischin, D.; Khushalani, N.I.; Schmults, C.D.; Guminski, A.D.; Chang, A.L.S.; Lewis, K.D.; Lim, A.M.L.; Hernandez-Aya, L.F.; Hughes, B.G.M.; Schadendorf, D.; et al. Integrated analysis of a phase 2 study of cemiplimab in advanced cutaneous squamous cell carcinoma: Extended follow-up of outcomes and quality of life analysis. J. Immunother. Cancer 2021, 9, e002757. [Google Scholar] [CrossRef] [PubMed]
- Migden, M.R.; Khushalani, N.I.; Chang, A.L.S.; Lewis, K.D.; Schmults, C.D.; Hernandez-Aya, L.; Meier, F.; Schadendorf, D.; Guminski, A.; Hauschild, A.; et al. Cemiplimab in locally advanced cutaneous squamous cell carcinoma: Results from an open-label, phase 2, single-arm trial. Lancet Oncol. 2020, 21, 294–305. [Google Scholar] [CrossRef]
- Migden, M.R.; Rischin, D.; Sasane, M.; Mastey, V.; Pavlick, A.; Schmults, C.D.; Chen, Z.; Guminski, A.D.; Hauschild, A.; Bury, D.; et al. Health-related quality of life (HRQL) in patients with advanced cutaneous squamous cell carcinoma (CSCC) treated with cemiplimab: Post hoc exploratory analyses of a phase II clinical trial. J. Clin. Oncol. 2020, 38, 10033. [Google Scholar] [CrossRef]
- Hober, C.; Fredeau, L.; Ledard, A.P.; Boubaya, M.; Herms, F.; Aubin, F.; Benetton, N.; Dinulescu, M.; Jannic, A.; Cesaire, L.; et al. 1086P Cemiplimab for advanced cutaneous squamous cell carcinoma: Real life experience. Ann. Oncol. 2020, 31, S737. [Google Scholar] [CrossRef]
- Grob, J.-J.; Gonzalez, R.; Basset-Seguin, N.; Vornicova, O.; Schachter, J.; Joshi, A.; Meyer, N.; Grange, F.; Piulats, J.M.; Bauman, J.R.; et al. Pembrolizumab Monotherapy for Recurrent or Metastatic Cutaneous Squamous Cell Carcinoma: A Single-Arm Phase II Trial (KEYNOTE-629). J. Clin. Oncol. 2020, 38, 2916–2925. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Cheng, J.; Colegio, O.R. Cutaneous squamous cell carcinomas in solid organ transplant recipients: Emerging strategies for surveillance, staging, and treatment. Semin Oncol. 2016, 43, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Lanz, J.; Bouwes Bavinck, J.N.; Westhuis, M.; Quint, K.D.; Harwood, C.A.; Nasir, S.; Van-de-Velde, V.; Proby, C.M.; Ferrándiz, C.; Genders, R.E.; et al. Aggressive Squamous Cell Carcinoma in Organ Transplant Recipients. JAMA Dermatol. 2019, 155, 66–71. [Google Scholar] [CrossRef]
- Nuño-González, A.; Vicente-Martín, F.J.; Pinedo-Moraleda, F.; López-Estebaranz, J.L. High-risk cutaneous squamous cell carcinoma. Actas Dermosifiliogr. 2012, 103, 567–578. [Google Scholar] [CrossRef]
- Manyam, B.V.; Garsa, A.A.; Chin, R.I.; Reddy, C.A.; Gastman, B.; Thorstad, W.; Yom, S.S.; Nussenbaum, B.; Wang, S.J.; Vidimos, A.T.; et al. A multi-institutional comparison of outcomes of immunosuppressed and immunocompetent patients treated with surgery and radiation therapy for cutaneous squamous cell carcinoma of the head and neck. Cancer 2017, 123, 2054–2060. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.Y.; Li, F.Y.; Ko, C.J.; Colegio, O.R. Cutaneous Squamous Cell Carcinomas in Solid Organ Transplant Recipients Compared with Immunocompetent Patients. JAMA Dermatol. 2018, 154, 60–66. [Google Scholar] [CrossRef]
- Rizvi, S.M.H.; Aagnes, B.; Holdaas, H.; Gude, E.; Boberg, K.M.; Bjørtuft, Ø.; Helsing, P.; Leivestad, T.; Møller, B.; Gjersvik, P. Long-term Change in the Risk of Skin Cancer After Organ Transplantation: A Population-Based Nationwide Cohort Study. JAMA Dermatol. 2017, 153, 1270–1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| AJCC-8 Classification | BWH Classification | ||
|---|---|---|---|
| Primary tumour (T) | |||
| T1 | Tumour < 2 cm in greatest dimension | T1 | 0 high-risk factors b |
| T2 | Tumour ≥ 2 cm and <4 cm in greatest dimension | T2a | 1 high-risk factor |
| T3 | Tumour ≥ 4 cm in greatest dimension or minor bone erosion or PNI or deep invasion a | T2b | 2–3 high-risk factors |
| T4a | Tumour with gross cortical bone/marrow invasion | T3 | 4 high-risk factors or bone invasion |
| T4b | Tumour with axial skeleton invasion including foraminal involvement and vertebral foramen involvement to the epidural space | ||
| Regional lymph nodes (N) | |||
| Nx | Regional lymph nodes cannot be assessed | ||
| N1 | Metastasis in a single ipsilateral lymph node ≤3 cm in greatest dimension and ENE (−) | ||
| N2a | Metastasis in a single ipsilateral lymph node >3 cm and ≤6 cm in greatest dimension and ENE (−) | ||
| N2b | Metastasis in multiple ipsilateral nodes all ≤6 cm in greatest dimension and ENE (−) | ||
| N2c | Metastasis in bilateral or contralateral lymph node(s), all ≤6 cm in greatest dimension and ENE (−) | ||
| N3a | Metastasis in a lymph node >6 cm in greatest dimension and ENE (−) | ||
| N3b | Metastasis in any lymph node(s) and ENE (+) | ||
| Distant metastasis (M) | |||
| M0 | No distant metastasis | ||
| M1 | Distant metastasis | ||
| T | N | M | Stage |
|---|---|---|---|
| T1 | N0 | M0 | Stage I |
| T2 | N0 | M0 | Stage II |
| T3 | N0, N1 | M0 | Stage III |
| T1 | N1 | M0 | Stage III |
| T2 | N1 | M0 | Stage III |
| T1–3 | N2 | M0 | Stage IV |
| T1–4 | N3 | M0 | Stage IV |
| T4 | N0–3 | M0 | Stage IV |
| T1–4 | N0–3 | M1 | Stage IV |
| Imaging Modality | Optimal Use in cSCC | Advantages | Disadvantages | Sensitivity/Specificity for H&N Nodal Disease a |
|---|---|---|---|---|
| CT | Bone or lymph node disease | Less expensive, more widely available, and faster image acquisition than MRI | Exposure to contrast dye and ionizing radiation | 52%/93% |
| MRI | Perineural, CNS, deep soft tissue, BM, or lymph node disease | No exposure to ionizing radiation | Less widely available, longer acquisition time, more expensive than CT | 65%/81% |
| US | Superficial lymph node disease and image-guided FNA | Least expensive, no exposure to contrast dye or ionizing radiation, rapid image acquisition, global accessibility | Operator and technique-dependent, limited visualization of deep structures | 66%/78% |
| PET/CT | Distant metastases | Functional and anatomic information, distinguishes postoperative scar tissue from recurrence | Most expensive, lesions less than 10 mm are below resolution for FDG-PET | 66%/87% |
| Low-Risk cSCC | High-Risk cSCC | |
|---|---|---|
| Clinical history and parameters | ||
| Area L < 20 mm Area M < 10 mm | Area L ≥ 20 mm Area M ≥ 10 mm Area H |
| Well-defined | Poorly defined |
| Primary | Recurrent |
| - | + |
| - | + |
| - | + |
| - | + |
| Pathology | ||
| Well or moderately defined | Poorly defined |
| ||
| - | + |
| ≤6 mm, no invasion beyond subcutaneous fat | >6 mm or invasion of subcutaneous fat |
| - | + |
| Type RT | Observations | Dose (Gy) | Sessions (n) | Times/wk | Fractionation |
|---|---|---|---|---|---|
| Definitive | Standard, GPS, size > 2 cm | 64–66 | 32–33 | 5 | conventional |
| Neck, no surgery | 70 | 35 | 5 | conventional | |
| Size < 2 cm | 50 | 20 | 5 | hypofractionation | |
| Frail patients + inconvenience | 50 | 15 | 5 | hypofractionation | |
| Frail patients | 36,75 | 7 | 5 | hypofractionation | |
| Frail patients | 35 | 5 | 3–5 | hypofractionation | |
| Adjuvant | Positive margins | 66 | 33 | 5 | conventional |
| Negative margins | 60 | 30 | 5 | conventional | |
| 50 | 20 | 5 | hypofractionation | ||
| Elective | 50–54 | 25–27 | 5 | conventional |
| Drug | Phase (N) | Patient Characteristics | RR | DC | mDoR | mPFS | mOS | Ref. |
|---|---|---|---|---|---|---|---|---|
| Erlotinib | II (39) | PS 0–2 Median age 68 y | 10% (no CR) | 72% | 7.2 mo | 4.7 mo | 13 mo | [64] |
| Gefitinib | II (40) | PS 0–2 Median age 67 y | 16% (no CR) | 51% | 31.4 mo | 3.8 mo | 12.9 mo | [65] |
| Cetuximab | II (36) | PS 0–2 Strong/moderate EGFR expression Median age 79 y | 28% (6% CR) | 68% | 6.8 mo | 4.1 mo | NR | [66] |
| Panitumumab | II (16) | PS 0–2 Median age 68 y | 31% (12% CR) | 69% | 6 mo | 8 mo | 11 mo | [67] |
| Immunotherapy | Treatment | Patients | NCT Code |
|---|---|---|---|
| Cemiplimab | Alone, pre-operative therapy, intralesional | Recurrent cSCC | NCT03889912 |
| Adjuvant therapy, after surgery and radiotherapy | High-risk cSCC | NCT03969004 | |
| Alone or in combination with RP1 | Advanced or metastatic cSCC | NCT04050436 | |
| Alone | Unresectable locally recurrent and/or metastatic cSCC | NCT04242173 | |
| Alone, neoadjuvant therapy | Stage II to IV cSCC | NCT04154943 | |
| Pembrolizumab | Alone | Recurrent/metastatic or locally advanced unresectable cSCC | NCT03284424 |
| Alone | Locally advanced or metastatic cSCC | NCT02964559 | |
| Adjuvant therapy, after surgery and radiotherapy | High risk locally advanced cSCC | NCT03833167 | |
| Combination with cetuximab | Recurrent/metastatic cSCC | NCT03082534 | |
| Nivolumab | Alone | Locally advanced/metastatic cSCC | NCT04204837 |
| Alone | Advanced cSCC | NCT03834233 | |
| Alone or in combination with ipilimumab | Metastatic cSCC in immunosuppressed patients | NCT03816332 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Foncillas, J.; Tejera-Vaquerizo, A.; Sanmartín, O.; Rojo, F.; Mestre, J.; Martín, S.; Azinovic, I.; Mesía, R. Update on Management Recommendations for Advanced Cutaneous Squamous Cell Carcinoma. Cancers 2022, 14, 629. https://doi.org/10.3390/cancers14030629
García-Foncillas J, Tejera-Vaquerizo A, Sanmartín O, Rojo F, Mestre J, Martín S, Azinovic I, Mesía R. Update on Management Recommendations for Advanced Cutaneous Squamous Cell Carcinoma. Cancers. 2022; 14(3):629. https://doi.org/10.3390/cancers14030629
Chicago/Turabian StyleGarcía-Foncillas, Jesús, Antonio Tejera-Vaquerizo, Onofre Sanmartín, Federico Rojo, Javier Mestre, Salvador Martín, Ignacio Azinovic, and Ricard Mesía. 2022. "Update on Management Recommendations for Advanced Cutaneous Squamous Cell Carcinoma" Cancers 14, no. 3: 629. https://doi.org/10.3390/cancers14030629